
Abstract
Public–private partnerships (PPPs) have been recognized as central for addressing the childhood obesity epidemic. However, very few real-world examples have been published documenting the workings of effective PPPs. The objective of this article is to identify the factors that enabled the successful implementation of school-based PPPs focusing mainly on nutrition and physical activity in 7 countries located in Asia (China and India), Africa (South Africa), Europe (Germany, United Kingdom), and Latin America (Brazil and Mexico). We triaged qualitative data from (1) proceedings from 2 school-based healthy lifestyles program evaluation workshops in October 2013 and in May 2016; (2) Mondelēz International Foundation (MIF) annual country reports and MIF project reports; and (3) interviews with key program leaders from each program. Extracted data were mapped into each of the 11 guiding principles for effective PPPs recently developed by a multisectoral public–private group of stakeholders in the United States. Three of the 7 countries met all, and the remaining 4 met between 4 and 7 of the guiding principles. Therefore, it is not surprising that there is strong evidence that all programs are having a positive impact on healthy lifestyles knowledge and practices in the target populations. This MIF-led initiative provides important lessons as to how to establish effective PPPs designed to tackle the childhood obesity epidemic globally.
Keywords
Introduction
Childhood obesity is determined by a constellation of factors ranging from macro-social, economic, and health policies all the way down to private sector, community, household, and individual choices across the life course. 1 –4 Therefore, public–private partnerships (PPPs) have been recognized as central for addressing the childhood obesity epidemic. 5 In spite of this, there are very few real-world examples that have been published documenting how effective PPPs work in the area of childhood obesity. 2,5 A key challenge behind the establishment of PPPs is the lack of trust among potential partners, especially due to conflict of interest concerns. Therefore, it is important to analyze ongoing PPPs that have apparently been able to overcome such challenges. Over the past 6 years, the Mondelēz International Foundation (MIF) has been partnering with private and public organizations across world regions supporting the delivery and evaluation of school-based healthy lifestyles programs focusing mainly in fostering healthy dietary and physical activity behaviors. 6 –13
The objective of this article is to identify the key factors that have enabled the successful implementation of MIF-supported school-based PPPs in 7 countries located in Asia (China and India), Africa (South Africa), Europe (Germany, United Kingdom), and Latin America (Brazil and Mexico). Findings are likely to help understand how future PPPs seeking to curb the obesity epidemic can be successfully established across world regions.
Conceptual Framework
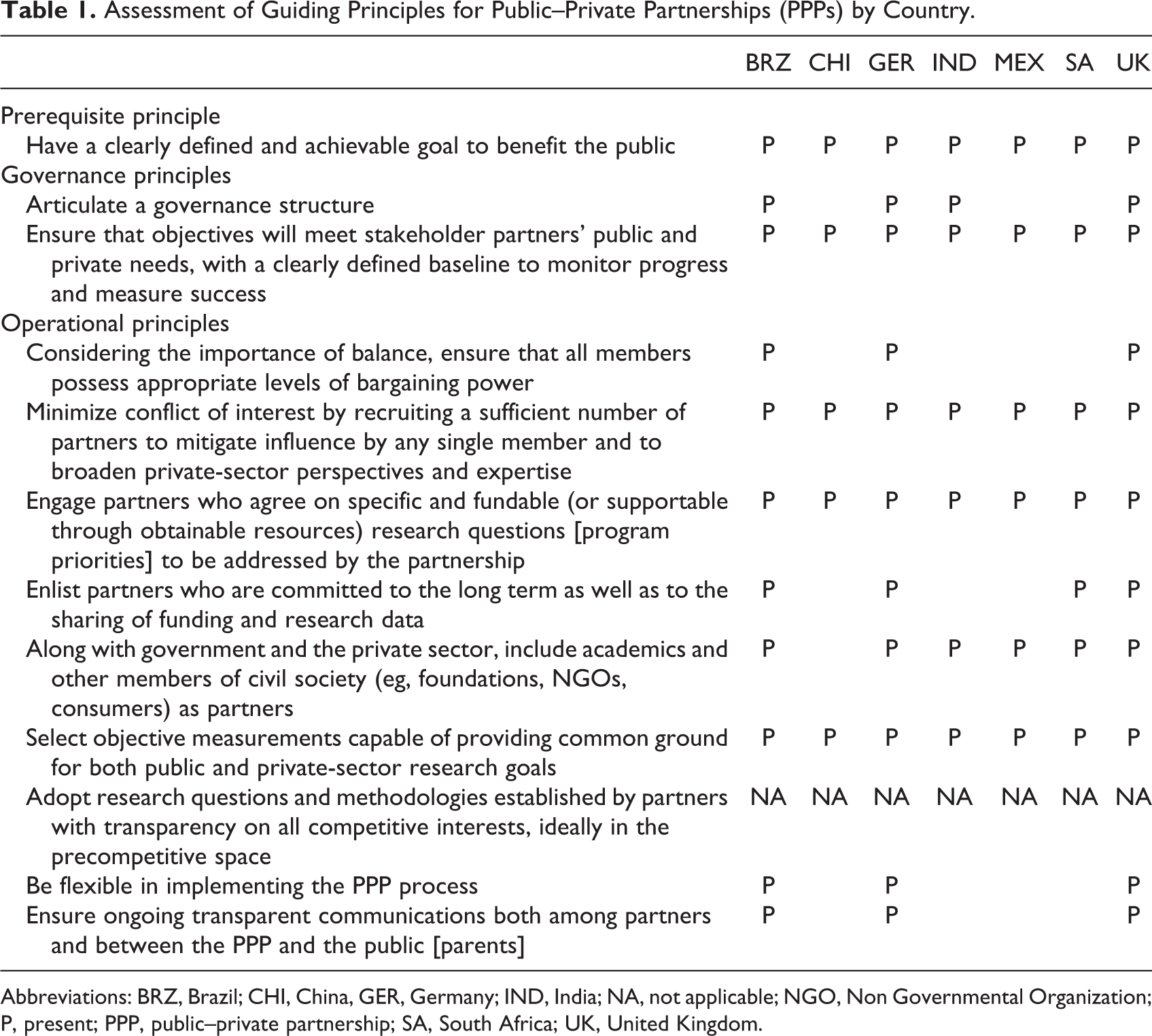
Based on a consensus deliberation process, a United States multisectoral team with representation from food and nutrition scientific societies, government agencies, and the National Institutes of Health recently identified 12 guiding principles to maximize the effectiveness of PPPs in nutrition research. 14 In the analyses presented in this article, we are extending the application of these principles to the delivery of programs based on sound PPP practices. As recommended by Alexander et al, 14 the guiding principles were categorized into the following 3 “consensus principles”: (1) prerequisite principle, (2) governance principles, and (3) operational principles (Table 1).
Assessment of Guiding Principles for Public–Private Partnerships (PPPs) by Country.
Assessment of Guiding Principles for Public–Private Partnerships (PPPs) by Country.
Abbreviations: BRZ, Brazil; CHI, China, GER, Germany; IND, India; NA, not applicable; NGO, Non Governmental Organization; P, present; PPP, public–private partnership; SA, South Africa; UK, United Kingdom.
Methodology
A qualitative analysis was conducted to identify key enabling factors and map them by each of the 12 principles outlined by Alexander et al for each of the 7 countries included in this article. Key sources of information were (1) MIF school-based Healthy Lifestyles evaluation workshops conducted in Granada in October 2013 6,13 and in Chicago, Illinois, on May 2016; (2) MIF annual reports and MIF program reports (available from author upon request); and (3) interviews with key program leaders from each program. Key program leader(s) were selected based on having extensive knowledge of the history of program, structure of PPP behind program as well as on the key administrative, operative, and evaluation components of program. A total of 19 key program leaders participated in the interviews that were conducted between September 5 and 28, 2016, by a highly trained consultant (Mark Rosati [MR], of Marj Halperin Consulting, Inc). On average, each country interview lasted 60 minutes. Interviews were conducted by phone and Skype. There were many follow-up questions answered via e-mail for each of the countries, extending into the early part of 2017. In preparation for the interviews, MR reviewed MIF progress reports prepared by each of the programs. Program websites were also consulted when available. Interviews were recorded and analyzed by RPE and MR.
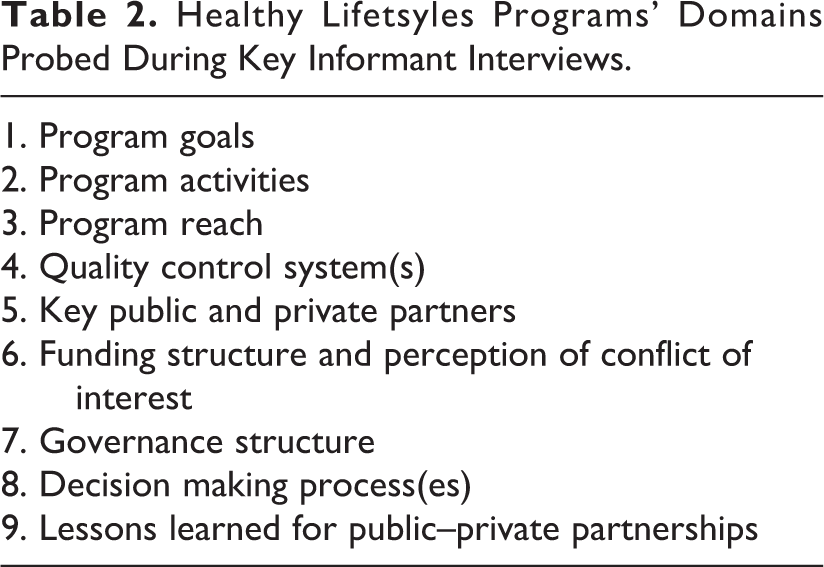
The initial draft of the interview guide was developed specifically for this project by the first author (RPE) and subsequently reviewed by the project’s 4-member steering committee prior to implementation (Table 2). A data extraction form was used to confirm the presence/absence of the implementation of each guiding principle by country. The qualitative data analyses were led by RPE with iterative input from all steering committee members.
Healthy Lifetsyles Programs’ Domains Probed During Key Informant Interviews.
Results
Public–Private Partnerships Descriptions by Country
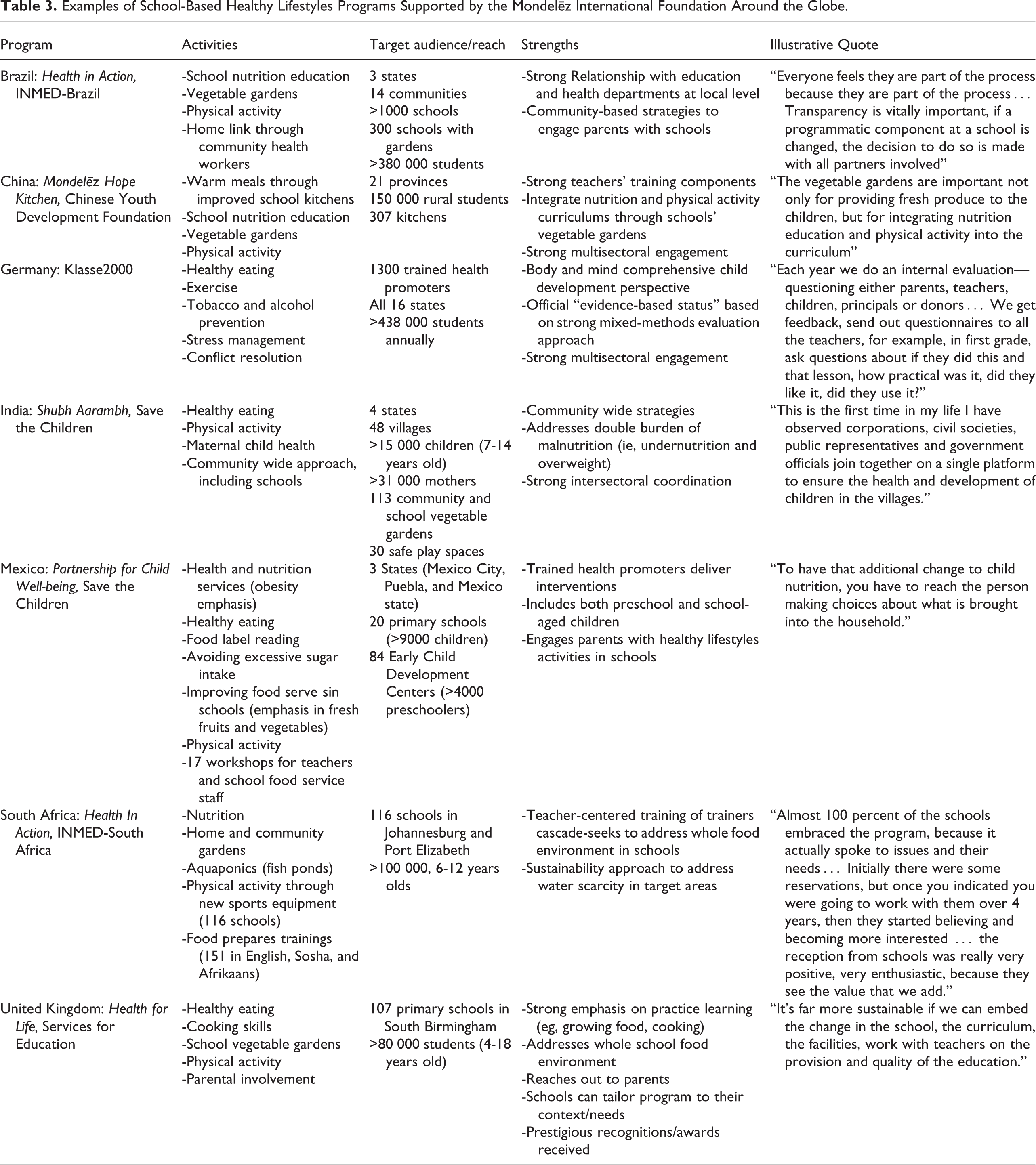
For each country, we describe the following characteristics of its program: (1) PPP structure and governance, (2) program objectives, (3) curriculum content, (4) geographical areas and coverage, (5) process evaluation, and (6) impact. These are summarized in Table 3 and presented in more detail below.
Examples of School-Based Healthy Lifestyles Programs Supported by the Mondelēz International Foundation Around the Globe.
Brazil
The Health in Action (HIA) program is a partnership of INMED Partnerships for Children, INMED Brazil, MIF, and the Instituto Esporte e Educacão (IEE), an organization promoting sports and physical activity in low-income communities. Ação Saudável joins with officials from the Brazilian Ministries of Health, Education, and Agriculture; local governments; principals and teachers; and community leaders for programmatic planning and implementation and performance evaluation. Additionally, INMED has worked closely with the first author of this article (RPE), developing sound program monitoring and quality control procedures.
HIA program seeks to strengthen support infrastructures in community and home settings. Before starting the program in any community’s schools, INMED meets with local mayors and Departments of Education, Health, and Agriculture and signs cooperative agreements. HIA program includes school nutrition education, vegetable gardens, physical activity promotion, and training for community health agents who, working as part of family health teams in each community, make home visits to parents to promote proper diet and hygiene. Training of school staff regarding nutrition and physical activity is a key component of the program. This process includes semiannual, 8-hour training sessions in health, hygiene, sanitation, nutrition, healthy lifestyles, and gardening. Teachers then serve as training multipliers at their local schools. HIA program governance includes regular meetings between INMED project coordinators in all towns and representatives from the education departments and other local government bodies to provide program updates and to plan training and other activities.
The HIA program operates in the Brazilian states of Pernambuco, São Paulo, and Paraná where many vulnerable children live. Phase 1 was launched in 2010 and lasted until 2013. Phase 2 started in 2014 and is still ongoing. HIA program has engaged with more than 1000 schools, and it will reach more than 380 000 students in a total of 14 communities in the 3 states. HIA program reports significant progress across the range of the program’s objectives of improving health, hygiene, and nutrition at school and home (note 1).
Key program leaders attribute HIA’s success to shared goals and close coordination with local officials, school principals, teachers and staff, children, and parents. Local governments are seen as key stakeholders, as governmental support provides a foundation upon which to build strong relationships with schools. After identifying towns with the most need for assistance in nutrition and physical activity education, “we met with all the mayors and education and health and agriculture departments and signed cooperation agreements…This opened the doors of the schools for us. Teachers can participate in our training. It gave us free access to the schools, the teachers, to the students, cafeteria workers” (Key program leader [BRKI]-1). As expected, INMED works closely with education and health departments and schools on the programs: “If each school doesn’t buy in, the program won’t work, so we make sure the principals are aligned with what we are doing.” (BRKI-2).
INMED presents a strategic plan for local governments to approve, thus paving the way for cooperation. Regular meetings are held with government officials to talk about results, upcoming activities, and other important topics. A key program leader reports that parents are generally extremely supportive of the program. “Everyone feels they are part of the process because they are part of the process…Transparency is vitally important, if a programmatic component at a school is changed, the decision to do so is made with all partners involved” (BRKI-1).
In addition to the central leadership team, INMED has at least 2 staff in each community assigned to visit schools and monitor performance. The larger schools also have trained volunteers working with the program. Implementation of the programs starts with a presentation in each of the schools. After the programs are up and running, a local INMED coordinator goes to each school at least once a month to check in, get feedback, and monitor success or other developments. “Our local coordinators with the schools come up with ideas…Last week, in one northeast town, they had an all-day bicycle tour around the town.” (BRKI-2).
HIA program includes 300 schools with full gardens which key program leaders attribute to careful planning, sensitivity to local dietary preferences, and partnership with local agriculture departments. Local coordinators first analyze the availability of water, soil conditions, and other key program leaders. Then, the communities, including the schools, decide what vegetables to plant. Students help run the gardens, providing them with practical training and physical activity.
The formal physical activity component of HIA is done in partnership with IEE in close coordination with the local schools. IEE plays a key role in the program, helping to train teachers and collaborating with INMED and schools to help evaluate students’ performance and document program outcomes in physical activity. As with the gardens, careful planning and coordination with schools is seen as the key to success.
Process and impact evaluations show that HIA is having a positive impact on dietary and physical activity behaviors (note 1). HIA program has also demonstrated that it strengthens social capital in the communities where it operates. For example, when Brazil experienced outbreaks of Zika and dengue viruses, 8 HIA schools in 1 city mobilized to help disseminate prevention information to students, parents, and their communities. This included a march to promote awareness of mosquito control. In another city, the HIA school cleaned its surrounding area, collecting trash and removing standing water where mosquitoes could breed.
China
The Mondelēz Hope Kitchen (MHK) program was established in 2009 initially to address hunger and undernutrition in rural schools, and as a result of the MIF initiative over the years, it now also promotes healthy lifestyles to prevent childhood obesity with strong community engagement. By funding kitchen equipment, as well as teacher and kitchen staff training in health and nutrition knowledge and practice, MHK has enhanced the capability of rural schools to provide warm, cooked meals. This helps students access safe and nutritious food and ultimately, improve their nutritional intake and health.
Mondelēz Hope Kitchen is grounded on a partnership between the Chinese Youth Development Foundation (CYDF), the Chinese Centers for Disease Control and Prevention (CDC), and MIF, engaging students through a 3-pronged strategy involving nutrition education, vegetable gardens, and active play. Mondelēz Hope Kitchen receives inputs from 5 key sectors: the CYDF, grassroots-level community service centers, schools, local governments, and the business sector.
Before the program, 70% of students surveyed felt hungry during class, more than 30% reported at least occasional food insufficiency, and schools often lacked the clean, well-equipped cooking facilities regarded as vital to ensuring that students receive 3 nutritious meals a day. As of October 2016, the program had established 307 MHK kitchens benefiting 150 000 rural students, and program managers reported that the percentage of students eating a balanced diet had gone up. By the end of 2016, 50 delicious veggie gardens were operating in 21 provinces and cities across a wide swath of China (note 2).
The leadership team’s approach was methodical. It built upon the foundation that CYDF had established during the previous quarter century by leveraging its network of government officials, community partners, and resources in 29 communities across China. CDC in China is an important partner because it is responsible for evaluating rural students’ nutrition and well-being. Impact findings have documented that the program trainings have enhanced the teachers’ knowledge of nutrition (note 2). As one teacher stated: Previously, I just had limited knowledge about nutrition and sometimes could not fully convince students of my answers on the class. Through systematic learning, I have gained a holistic understanding of nutrition and health and learned how to teach the course. Now, I am fully confident in answering students’ questions and ready to further improve the teaching quality.
The project team runs contests for excellence in teaching plans, for written essays, and for oral presentations from students about the program. These competitions and awards promote the implementation of the program in the schools, organizers say. Homework assignments foster learning outside school and also engage parents to encourage healthy eating habits at home.
As with the gardening and nutrition education initiatives, the active play component of the program began with teaching the teachers. Physical education teachers in rural China are part time; therefore, MHK provides schools with trainings and equipment that can be used by physical education teachers to foster engaging activities, such as jump ropes and ping-pong, to help the children achieve the goal of an hour of exercise per day.
By July 2016, the first phase of the program was completed in 30 schools located in 3 provinces. In the areas where the MHK program was implemented, the percentage of students from grades 2 to 6 showed significant improvements in nutrition and physical activity behaviors (note 2).
Beyond the direct impact on MHK program participants, its success holds promise of inspiring similar work around China. Since its launch in 2009, local education authorities have observed MHK’s success and are urging schools to emulate the program and learn from its best practices. Because both CDC and CYDF are responsible for giving advice to the Chinese government on health and nutrition topics, this MIF-driven experience has strong potential to influence the environment for improved nutrition and physical activity policies throughout China.
Key stakeholders attribute the success of MHK to the strong engagement of partners across sectors including government agencies, communities, schools, teachers, students, and their families.
Germany
From its roots as a 1991 tobacco use prevention program in Bavaria, Klasse2000 has evolved into a multifaceted organization promoting overall health and preventing addiction and violence among young people. It is the largest program for primary school students (grades 1-4, ages 6-10) in the nation, serving more than 1.4 million children since 1991. Klasse2000 operates in all 16 German states; the program served 438 226 students during the 2015 to 2016 school-year. MIF is the largest among almost 7700 active donors.
As a fully national program, Klasse2000 engages with a number of community partners, in addition to German federal and local governmental authorities and MIF. German Lions Clubs are very important supporters, not only because of financial support but because of the members’ advocacy with other partners and donors in their regions.
The program addresses children’s health from a broad perspective, focusing on topics such as healthy eating, exercise, making friends, solving problems without violence, avoiding tobacco and alcohol, and relaxation techniques. The physical activity component is not about competition instead encouraging students to enjoy exercise.
Key program leaders report “a great deal of buy-in” from federal and local stakeholders. Those involved with Klasse2000 “on the ground” are well motivated to see that Germany’s children grow up strong and healthy. As in other countries, keys to the program’s success are cooperation with school officials, monitoring performance, and updating curriculum on a regular basis. As in any complex multistakeholder enterprise, problems or conflicts sometimes arise. “If despite all of our previous agreements a problem occurs, we try to clarify it in personal conversation and try to resolve it…It’s the advice we give to the children.” (GKI-1).
Program delivery relies on 1300 trained external health promoters who go to classes to work 2 to 3 times a year with the students in their schools. All promoters must have a health-related or educational background as well as experience working with children. Students enjoy interacting with the external visitors and the games and materials they bring. Parents are invited to evening activities and receive written materials on health- and nutrition-related topics. Their children’s homework assignments further encourage family discussions.
Klasse2000 sees its impact as resulting in large part from anchor topics addressed over the entire course of grade school, with continual updates. “Each year we do an internal evaluation—questioning either parents, teachers, children, principals or donors…We get feedback, send out questionnaires to all the teachers, for example, in first grade, ask questions about if they did this and that lesson, how practical was it, did they like it, did they use it?” (GKI-1). Every year, Klasse2000 revises the curriculum of 1 grade; so, during every 4-year period, the curriculum for every grade will have been revised.
A randomized controlled study conducted by the University of Bielefeld analyzed data from 2013 to 2015 and documented the program’s effectiveness at protecting healthy nutrition and behaviors in the target children with some evidence that benefits have extended to the whole family (note 3).
15
As reported by a key academic partner: Compared to programs that are offered over a brief period of time and focus on specific topics only, Klasse2000 generates added value by being a key element throughout elementary school, addressing the issue of health promotion from a variety of angles, providing a well thought-out structure that includes school-compatible materials, and cooperating with health promoters…Another gratifying aspect of Klasse2000 is that teachers rate the program positively and appreciate the cooperation with health promoters. The impact of the program is intensified by the fact that parents and teachers observe changes in the children who participate.
A key to the success of the Klasse2000 program is the nature of its PPP. In addition to collaborative programmatic development, implementation, and review with input from multiple stakeholders, Klasse2000 is funded by donations and subsidies from diverse organizations and individuals, mainly in the form of sponsorships for individual classes. To date, the program has been embraced by 7700 sponsors, including corporations, Lions Clubs and other service clubs, schools, parents, associations, foundations, and others.
India
Shubh Aarambh (SHA), a joint program of Save the Children India, Magic Bus, and MIF, serves 48 villages in 4 Indian states. The target population includes about 40 000 children and adolescents and more than 27 000 women, mainly mothers and pregnant women. Goals of SHA are to improve feeding practices, health-seeking behavior and community-based health, nutrition, and childhood development services in 5 locations across 4 states in India. Health and nutrition activities include capacity building of the government’s health and nutrition frontline workers; child, adolescent, and mothers’ community group formation and strengthening; home visits to follow-up on health and nutrition services; and school and community events to raise awareness on nutrition and healthy lifestyles. The main activities involving growing fresh foods include development of kitchen gardens in schools, community spaces, and homes; cooking demonstrations to promote nutritious meals; and linking kitchen garden produce to school and home meals. The main active play activities include community and school-based sessions with children 7 to 14 years of age and development of safe playgrounds.
SHA arose out of a partnership among MIF, Save the Children, and Magic Bus. The project aligns well with MIF’s goals and its emphasis on allowing programs to adapt themselves to the diverse local contexts in which they operate. Local project leaders worked to identify the areas in India where SHA was needed and would find fertile ground based on the combination of geography, community needs, and partners’ commitment. Because the communities in which the program operates are low income and experience undernutrition, organizers decided to work with children from birth to age 18 as well as with expectant mothers. This comprehensive approach helps ensure that children enter preschool and primary school healthy and ready to learn.
The main partners MIF, Save the Children, and Magic Bus work in full collaboration with a range of government stakeholders, including public education departments (SHA includes children of age 7-14), agriculture departments (to help promote and create more kitchen gardens), and social welfare and health departments (for community health initiatives, including support for pregnant women). Besides trust and transparency, a key to the program’s success has been skill-based training for school personnel, health workers, and child welfare workers. Program leaders hold meetings every 6 months with government officials from the states to review the project status and resolve any issues or concerns.
Respondents report improved fitness and nutrition in key program areas, including awareness of healthy lifestyles (sanitation, hygiene), active play, more householders accessing fresh fruits and vegetables from kitchen gardens, and increased consumption of iron and folic acid, among other indicators. As with other participating countries, the project is succeeding, thanks to consultation with and cooperation among many stakeholders, including government officials, principals, teachers, parents and children, project staff, community leaders, and MIF. Program leaders report great satisfaction with results to date, with very active engagement from children, regular meetings with parents at schools, metrics showing improved nutrition, iron, and folic acid consumption, and 113 operating gardens (note 4).
Program evaluation shows that children, youth, parents, and other community residents have embraced nutrition, health, and physical activity. Evidence includes their large-scale participation in nutrition and active play events and in the sustained presence of kitchen gardens in communities (note 4). By the time the key program leader interviews were conducted, SHA had directly reached 15 465, 7- to14-year-olds (89% of project target) and 31 674 mothers (>100% of project target; note 4). Kitchen gardening has been a very popular activity with children and adults alike, with 113 community and institutional gardens established. Many households have also set up their own individual kitchen gardens. Safe play spaces are another example of visible changes, with 29 of 30 spaces already set up according to program guidelines. These spaces provide children with an easily accessible and safe community playground they can use for daily physical activity, including team sports using volleyball nets and other game items.
It is important to note that the project has started to strengthen and reactivate government programs with a mandate to ensure children’s well-being. These include school management committees, child parliaments, and Village Health and Nutrition Committees. SHA views these structures as critical for the sustainability of school- and community-based nutrition services and education. District and block health and education departments are acknowledging the efforts of SHA to support government services. SHA hosts 665 children’s sports for development groups, 355 adolescent groups, and 1571 mother groups. From January to June 2016, SHA completed 825 school sessions and 3820 community sessions with children, 551 adolescent sessions, and 4531 mother sessions (note 4).
Monthly events and campaigns on nutrition and physical activity engaged entire communities and commemorated special days. Bringing about policy and system change takes time…What we aim for is interventions that can be self-sustaining—inbuilt mechanisms for financing those interventions through government or other partnerships, opportunities for retraining…A large pool team of youth volunteers has been developed, and young people facilitate many of the sessions. They are the change-makers; they can influence younger peers and peers…A lot has been achieved, but there is still a lot more to do. (IKI-1).
Mexico
The purpose of Alianza por el Bienestar de la Niñez (Partnership for Child Well-being [PCW]) is to lay a foundation for healthy lifestyles, ultimately improving the nutrition and physical activity of children aged 2 to 13 years in 20 primary schools (6- to 12-year-olds) in Puebla and Mexico City and 84 early childhood development (ECD) centers (2- to 5-year-olds) in Mexico City and the State of México. The program currently serves 9099 primary-school children and 4126 preschoolers.
PCW is in the initial stage of a 4-year partnership between Save the Children Mexico and MIF to improve children’s nutrition and physical fitness through school and community center-based programming in 3 areas of Mexico. Mexico currently has the highest prevalence of children considered overweight and obese globally, estimated at 33% nationally. In Mexico City, Mexico State, and Puebla, overweight and obesity averages for children 6 to 11 years old range from 35.1% to 22.6%, respectively. 16
The program was designed around 5 key objectives: (1) improving nutrition services, with a focus on detection and referral for prevention and treatment of obesity; (2) improving community knowledge, (3) promoting healthier lifestyles through nutrition education and promotion of physical activity, (4) implementing nutrition gardens through community participation to develop an enabling environment for obesity prevention, and (5) improving the public policy environment to ensure sustainable change on successful measures for childhood obesity prevention.
Save the Children works with school staff and ECD center coordinators to shape nutrition and active play workshops. Save the Children health promoters, most with backgrounds in nutrition, work in the schools and ECD centers implementing the program on a daily basis. Regular meetings are held, both to train the promoters on new workshop materials and to get feedback from the promoters on program performance and ideas for how to improve activities during the year. Save the Children sought additional external expertise to enhance active play methods in schools for both teachers and promoters through a partnership with Sports World, a Mexican company and operator of sports clubs and gymnasiums.
The first full academic year of the program involved 20 primary schools with 9099 children and 84 ECD centers with 4126 children. The nutrition program emphasizes healthy eating choices, showcasing the history and tradition of the Mexican diet; teaching children about the benefits of fruit and vegetable consumption; and eating locally produced and grown foods, including the differences between fresh and processed foods. They also include an experiential component in some workshops so that children can try new foods. Initial metrics show progress in addressing obesity issues and strong engagement with stakeholders, including corporate volunteers (note 5).
In the first academic school-year, the program developed and implemented 12 workshops for more than 13 000 children in the states of Mexico, Puebla, and in Mexico City. Six focused on nutrition, and the other 6 on physical activity. The interactive workshops teach students about specific themes, for example, how to read food labels, how to understand what they are eating, and how to avoid excessive sugar. One highly interactive 60-minute module for fourth and sixth graders is “Hidden Sugar,” in which the students learn to determine how much sugar is in a beverage or serving of packaged food.
Workshops include age-appropriate games and repetition of messages to reinforce learning. In addition, 57 workshops were geared toward parents, 17 for teachers, and 33 for kitchen staff at schools and ECD centers.
Save the Children also worked directly with parents, coordinators, and cooks in ECD centers to support their efforts to improve the diets of young children. Teacher workbooks and parent flyers promote “conscious eating”—healthy cooking and diets to emphasize the importance of fresh vegetables and fruit consistent with Mexican dietary traditions.
PCW has already run 10-day summer camps in Puebla and Mexico City to reinforce healthy lifestyle basics and initiate contact with parents. The end line survey showed that the percentage of children who knew they should exercise 30 minutes a day tripled, and almost twice the number of children reported eating 3 or more vegetables the previous day (52.3% vs 27.2% at baseline; note 5). During focus group discussions with children in Puebla and Mexico City, program staff discovered that children had learned a lot about how to eat healthier and exercise more. However, some messages around processed foods and fat versus sugar need further reinforcement so that children understand how to make healthier choices. Six new nutrition workshops were developed for the 2016 to 2017 school-year to fill in the knowledge gaps and use new methods of child participation to enhance learning. Additionally, children recognize that more adult involvement (from family and teachers) is necessary so that they can improve their eating habits. Ten gardens were also established, most of them at ECD Centers, with another 10 planned for 2016 to 2017. Students in grades 4 to 6 will help to maintain the school gardens and learn nutrition.
Food grown in the gardens will supplement meals served in the schools. Rain and pollution in Mexico City often inhibit outdoor play workshops, so the Save the Children team is working on how to adapt physical activity sessions for smaller, indoor spaces. A respondent indicated: “We’re making small changes, good changes inside the schools…Kids are learning and realizing that what they’re eating is not as healthy as it should be, but this [change behavior] is not something you can do in a year…Self-awareness is a good start.” (MKI-I).
One challenge, she notes, is that families in poorer communities often have both mother and father working, so getting a parent to take time off to attend a workshop can be difficult. “To have that additional change to child nutrition, you have to reach the person making choices about what is brought into the household.” (MKI-1). As the 2015 to 2016 school-year ended, all participating schools and ECD centers committed to another year of participation. Collaborative relationships have been established between schools and promoters, as teachers and administrators noted a positive change in the habits of their students.
With strong support from MIF, Save the Children worked closely with Mondelēz in Mexico and other private partners, such as Sports World, to establish a program that is contextually and culturally relevant to building healthy lifestyles among Mexican schoolchildren. Workshops for children and direct outreach to parents, teachers, and cooks in schools and in ECD centers are establishing a foundation for sustained improvements in children’s daily diets and physical activity.
South Africa
Health in Action (HIA) South Africa was launched in 2015 in Johannesburg and Port Elizabeth communities. A total of 116 schools in lower income areas with more than 100 000 students aged 6 to 12 are targeted in this phase of the program (note 6).
The partnership between INMED and MIF, upon which South Africa’s HIA is built, is supported by governmental and nongovernmental partners, with the overarching goal of promoting sustainable improvements in children’s health and nutritional status through participatory education and activities on nutrition, physical activity, and healthy lifestyles, including hygiene and sanitation. Selected lead teachers are trained as “multipliers” who, in turn, train their colleagues to improve nutrition and reduce hunger by increasing access to fresh produce through the establishment of school, home, and community gardens and through the installation of a large aquaponic system in each project province to serve as a learning tool and source of abundant fresh produce and nutritious fish protein to supplement meals in targeted schools. “Garden champions” selected by school-governing boards from among local unemployed youth lead cultivation activities and recruit other volunteers to help.
The program also seeks to increase participation in physical activity, both through school-based physical education and leisure time recreation and play, with an emphasis on making activity fun so that it becomes an enjoyable habit. School-governing boards select “break-time buddies” from among local unemployed youth. They encourage children to take an active part in recess time, guiding activities and monitoring safety. The program promotes positive changes in the school food environment, including advocacy for compliance with government feeding program mandates and providing basic food preparation supplies where needed. Training for school food workers includes food hygiene and preparation of nutritious meals that incorporated garden produce. Snack vendors who sell to schoolchildren are encouraged to offer healthier food options. Ultimately, the program is expected to build the foundation for long-term sustainability by actively involving a wide range of partners: parents and community members, local and state governments, academic institutions, other nongovernment and community-based organizations, and private sector entities.
The MIF approach facilitates international collaboration, encouraging and enabling colleagues in different nations to readily draw upon each other’s experiences and best practices. In the case of INMED South Africa, the program was strongly influenced by the success of INMED’s HIA (Ação Saudável) program in Brazil. The first phase of the Health in Action program in Brazil, which preceded expansion of the program to South Africa, was highly successful in terms of healthy lifestyles outcomes…as well as in the range of partnerships developed with local governments—even departments that typically wouldn’t have been involved in a project of this type [such as] school systems, universities and other community groups—and in the level of community mobilization. All…created a strong foundation for the program’s long-term sustainability. The same multi-sectoral approach used in Brazil has also formed the foundation of the [South African] program to ensure sustainability. (SAKI-1) With South Africa sharing a lot of similarities with Brazil—in particular, with the double burden of malnutrition that includes both undernutrition and overweight—it made sense adapting the model to the local context in South Africa through various changes including ensuring that educational content and messaging is aligned to relevant education curricula standards. (SAKI-1) Such learnings and continuous sharing of information is still ongoing between Brazil and South Africa teams through regular technical discussion meetings held mostly over Skype. (SAKI-1).
An important first step in the emergence of the program was meeting with government education and other officials at the national and provincial level to familiarize them with HIA and get approvals. That relationship included not just initial meetings but regular follow-ups and invitations for officials to visit schools and monitor progress. Local buy-in was equally important. Parents, teachers, and students are all key stakeholders, and in launching the new program, it was vital to get a commitment from them to join. At each school, 1 teacher became responsible for the program, serving as a liaison with HIA program staff. Almost 100 percent of the schools embraced the program, because it actually spoke to issues and their needs…Initially there were some reservations, but once you indicated you were going to work with them over four years, then they started believing and becoming more interested…the reception from schools was really very positive, very enthusiastic, because they see the value that we add. (SAKI-2)
By August 2016, the initial training in Johannesburg served a combined total of 151 school food preparers through 3 multilingual sessions (English, Xhosa, and Afrikaans). The training focused on nutritious and balanced meal planning, portion sizes and healthy food preparation, and proper hygiene practices. A cooking demonstration illustrated all the elements discussed during each training session, and attendees enjoyed sampling the food prepared.
The gardening initiative is off to a promising start, thanks in part to existing government policy encouraging all schools to establish food gardens, both to improve access to fresh produce and also for teaching purposes. HIA program first trains the teachers who often do not have an agricultural background and also trains unemployed youth to work maintaining the gardens. With growing interest from parents, training is also being conducted for them. The program also offers resources such as seeds, garden equipment, rainwater harvesting systems, and plans for planting.
Lack of water is a significant challenge for many schools, and there is a severe drought in South Africa resulting in water restrictions in Johannesburg. Therefore, schools have been encouraged to cultivate plants that require less water such as the orange fleshed sweet potato, which is high in vitamin A.
Another solution—and another educational opportunity for students—is the development of aquaponic systems for producing fresh foods. This is where agriculture and hydroponics meet, a unique feature of South Africa’s HIA.
The physical activity component of the program also includes teacher training and student engagement. The program provided all 116 schools with sports equipment including jump ropes and balls for netball (a basketball-like sport) and soccer. Out-of-school youths are recruited as “break-time buddies” to assist in guiding the younger children in physical activity. Several schools to date have offered “fun days” that include tug-of-war and sack racing. To create an enabling environment for physical activity in schools, some schools are using painted games, including hop-scotch.
A key program leader noted teacher workload is a challenge for schools, where many teachers are under a great deal of stress. Because the program relies heavily on educators to drive in-school initiatives, HIA is also working with Nelson Mandela Metropolitan University’s psychology department to develop a module on teacher wellness and stress management. This is another unique feature of HIA among the MIF-supported programs.
INMED’s extensive work on the front lines of community-based program implementation in South Africa has given the organization experience in dealing with challenges, and HIA has proven no different. For example, a number of food preparers from non-HIA schools attended the initial training, and other schools submitted requests to join. As program funds cannot be used for nonprogram schools, HIA officials agreed to conduct additional trainings for food preparers for nonprogram schools if the Department of Education in Port Elizabeth covers the related expenses. A similar arrangement is being discussed in Johannesburg.
The South African experience in establishing HIA through an effective PPP mirrors that of other participating countries. Shaped by lessons learned from INMED’s experience in Brazil, the South African team started by connecting with government education departments and then went to schools to get local buy-in. Schools are managed by a governing body, and HIA staff met with all stakeholders—parents, teachers, learners—to win support.
The gardening component is well received by schools participating in the program, and benefits from existing government policy encouraging all schools to establish food gardens, not only to improve access to fresh fruits and vegetables but also to teach students how to tend the land.
United Kingdom
Now in its fifth year, Health for Life (HFL) has operated in 107 primary schools in the south Birmingham, UK region, impacting more than 80 000 students. The program serves a diverse socioeconomic range of communities and targets primary schoolchildren 4 to 11 years old and pupils 4 to 18 years old in schools for students with special educational needs. The program is a partnership between MIF and Services for Education (note 7). 12
HFL is designed to make the program a sustainable part of a school’s culture by promoting healthy lifestyles, attitudes, and behavior through healthy eating and cooking skills, growing food, physical activity, and family involvement. HFL works because it seeks to make positive change happen in both the schools and the home. “It’s far more sustainable if we can embed the change in the school, the curriculum, the facilities, work with teachers on the provision and quality of the education.” (UKKI-1). Equally important is bringing the change home after the school day ends because, “you don’t expect schools to do this and then go home and eat unhealthily and just sit down watching the television.” (UKKI-1).
HFL requires schools to sign up for participation over a 15-month period for a range of activities that meet the program’s interrelated objectives. Those identified as most likely to have the greatest impact on children’s healthy lifestyles include developing a sustainable, healthy lifestyle culture throughout the whole school; making a measurable improvement in students’ diet through cooking and healthy eating activities; engaging pupils in growing food to increase their knowledge and understanding of its links with healthy lifestyles; enabling schools to make a measurable improvement in students’ physical activity through improved use of school grounds; and engaging “hard-to-reach” parents/caretakers in the program’s key messages through healthy eating and cooking skills.
HFL participation begins with an initial audit asking key questions about the environment: Does the school have cooking facilities? How much physical activity is incorporated into the curriculum? Then, the school develops an action plan with key performance indicators, which becomes a map for moving forward. Each participating school collected baseline data from students and then repeated the survey of that cohort at the conclusion of the program.
Based upon data collected over the first 5 years, HFL has documented that the program has been very successful in changing the knowledge, attitudes, and behavior of the pupils with regard to healthy eating, cooking skills, growing food, and physical activity (note 7). HFL credits its success to an approach that has clear goals but also enough flexibility to allow the school to tailor the program to its specific needs.
Careful planning has also been central to the program’s success. Developing each school’s action plan can take 10 weeks. Consultations with key stakeholders—teachers, parents, staff, the school’s governing body—“Make the plan really robust…We didn’t want it to be a ‘class project’, we wanted to make schools think about sustainability” (UKKI-1). Another important element is staff training days in practical cooking, healthy eating, growing gardens, physical activity, and safety.
Children are taught different subjects in different years. One year, the program might focus on practical cooking, while the next might center on gardening. Events and competitions—sometimes involving the Lord Mayor of Birmingham—help encourage excellence and make the program fun and engaging for students.
All participating schools have developed gardens with vegetables and fruits (and sometimes chickens) and also cooking initiatives. In some schools, this has involved dedicating an area in the building for cooking and food storage. Physical activity can include active play time, such as games or hula-hooping, or walking or biking to school. Parental involvement is encouraged. Students may bring home a recipe, the family will cook it, and the student will write about it or take a picture. Other strategies to encourage parental involvement include assemblies where parents see their child’s work or work directly on related activities with their children. Schools also organize family bike rides, send home seeds for children to grow and monitor by keeping a diary, and invite parents to cooking sessions.
Surveys of the latest cohort of students have found substantial improvements in dietary intake, physical activity, and cooking behaviors (note 7). A particular focus of the program has been families who, for many reasons, can be characterized as “hard to reach.” For these families, Services for Education developed Family Learning Workshops to support parental engagement and help them encourage their children’s healthy lifestyles. As of February 2016, the program had worked with children and parents chosen by 23 schools.
Surveys show the benefit of the workshop approach. All parents reported that they enjoyed taking part in the workshops. They praised interesting activities for the children, family fun combined with learning, and clear explanations. Over 80% of parents reported they had learned something new. These lessons are central to the program’s goals, including how much sugar is in various foods, the benefits of exercise and healthy eating—especially fruits and vegetables, the amount of fat content in foods, differences between nutritional needs of children and adults, and the importance of sleep. Almost 70% of parents reported they would change/do something differently regarding healthy choices for themselves and their families, such as looking more carefully at labels and changing their child’s lunches and beverages (note 7).
HFL exemplifies a best-practice PPP. From local Mondelēz International volunteers helping schools to establish gardens, to community workshops for “hard to reach” parents, to student showcases and award ceremonies attended by the Lord Mayor and a member of parliament, the opportunity to instill healthy eating and exercise habits in the city’s schoolchildren has been widely embraced by the city of Birmingham. The corporate sector is also supportive. HFL was recognized with the Building Stronger Communities Award from the West Midlands organization Business in the Community and received a national award from the UK Food and Drink Federation for health and well-being.
Discussion and Conclusions
Although the National Academy of Medicine, American Society for Nutrition, and others have developed sound conceptual frameworks for designing effective PPPs, there is little documentation on how healthy lifestyle school-based PPPs get established and work in the real world. The efforts by MIF and its partners around the world—including metrics for hundreds of thousands of participating students—offers a unique window into how PPPs result in improved nutrition and fitness for children on 5 continents (Box 1).
Mapping of public–private partnerships (PPPs) principles by country
The PPPs analysis showed that the Mondelēz International Foundation (MIF) supported programs overwhelmingly met the suite of recommended best practices principles (Table 1).14
Prerequisite principle
All programs had a clear definition of the primary goals of their programs, and all were in line with the expectation of healthy lifestyles school-based programs.
Governance principles
A clear multisectoral governance structure that included input from teachers and parents was documented in 4 of the 7 countries. Consistent with the inclusion criteria and technical support offered by MIF, all countries had a clear baseline to monitor progress and measure success.
Operational principles
-There was strong objective evidence from 3 programs (Brazil, Germany, United Kingdom) of special efforts to ensure key stakeholders had a “seat at the table” in the decision-making process. There was no evidence of conflict of interest from any of the programs’ private partners. This is consistent, and very likely driven by the MIF “hands-off” approach with regard to the community programs that it supports. For all the programs, there was solid evidence that all key stakeholders had clarity on and were in agreement with the program’s priorities. Five programs demonstrated substantial evidence that the PPP was committed to and had, or was in the process of developing, a strategic plan for program sustainability including funding and evaluation data sharing. Six of the countries provided strong evidence of partners that included academics and other members of civic society (eg, foundations, nongovernmental organization [NGOs], consumers).
-All PPPs had common process and impact indicators in place, undoubtedly a result of the technical capacity-building evaluation support offered by MIF
-Three countries had strong evidence that flexibility regarding program implementation is an intrinsic component of their PPPs. The same 3 countries also engaged families with the school, through program elements that were formally incorporated into their PPP programs
The MIF support of PPPs in the 7 nations highlighted in this article is having a profound impact on hundreds of thousands of students, their families, their schools, and their communities. The evidence-based approach is creating a platform for program sustainability and rippling effects beyond the target schools. And it is all built on MIF’s comprehensive partnership model, ensuring private sector and community organizations join together to provide strategic investment and engaged leadership while empowering local officials, school principals, teachers and staff, students and parents, and other key stakeholders.
The MIF PPP framework is quite flexible and therefore fosters innovative new ways to promote healthy lifestyles for children—from creating gardens out of recycled automobile tires on school rooftops in Birmingham to aquaponics in South Africa. These new approaches and ideas are then shared by partners and can serve as international models for best PPP practices. The linkages between Brazil and South Africa are an excellent example of this kind of ongoing collaboration.
Across all countries and programs, success is built on solid, transparent partnerships involving close consultation with government officials, school principals and teachers, parents, corporations, and other key stakeholders. Regarding conflict of interest perceptions, countries were quite satisfied with the hands-off approach from MIF and the fact that MIF did not request any branding as part of the programs. Each program had total control of their governance and curriculums. What MIF did was to invest in helping the organizations strengthen their program evaluation capacity. Indeed, the programs were strongly empowered to rely on continual monitoring of programmatic quality and effectiveness, transparency, and a curriculum that connects in a meaningful way with primary schoolchildren, their families, and communities. These guiding principles should inform the future development of best practices PPPs seeking to curb the childhood obesity epidemic globally. The MIF PPP experience calls for instilling a culture of formal process and impact evaluation that brings together program leaders to learn from each other. Future work in this area should examine whether PPPs strongly driven by private foundations are having a negative or positive impact on the government’s decisions to take ownership of the scaling up process. On the one hand it can be argued that this model may create strong “donor dependency” but on the other it is also possible that the quality control capacity building will percolate to government structures. This question needs to be answered through future implementation science research to better understand what is the long-term sustainability of PPPs such as the ones examined in this article.
Footnotes
Acknowledgment
The author is very grateful to Mark Rosati for his outstanding work conducting the interviews with and following up with the programs’ leaders and for reviewing the programs’ reports. The programs’ leaders who were interviewed were given the opportunity to review and provide final approval of the program descriptions included in this article. The author deeply thanks the following program leaders who agreed to be interviewed, provided access to documents and responded to many follow-up questions: Brazil: Joyce Capelli, Executive Director and President of INMED Brazil; Marianita Masiero, Program Coordinator; Gabriela Pen, Director. China: Gu Lan, Director, China Youth Development Foundation; Nana Zhao, Assistant Manager, Corporate & Government Affairs for Mondelēz China. Germany: Andrea Dokter, Grant Manager, Klasse2000; Brigitte Horst, Program Manager, Klasse2000. India: Luciana Bonifacio, Senior Director, Global Corporate Partnerships, Save the Children US; Sumita Kirti, Project Manager for Shubh Aarambh; Meena Sriramane, Senior Manager, Corporate Marketing, Save the Children India; Mohini Venkatesh, Technical Advisor on School Health and Nutrition to Shubh Aarambh in India; Dileesh Verghese, Knowledge Management Coordinator for Shubh Aarambh. Mexico: Fatima Andraca, School Health and Nutrition Leader, Save the Children Mexico; Jeanne L. Long, Senior Specialist, School Health and Nutrition, Save the Children USA; Mariana Valdes Riveroll, JD, Director of National Strategic Alliances, Save the Children Mexico. South Africa: Kristin Callahan, MS, Director of International Programs for INMED Partnerships for Children; Sandra Pretorius-Rivalland, PhD, Program Coordinator and specialist in intervention programs for chronic diseases, INMED South Africa; Unathi Sihlahla, MA, Program Director for the Health in Action Program at INMED South Africa; United Kingdom: Sandra Passmore, PhD, Education Advisor, Health Education Services, UK-Life Education
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Rafael Pérez-Escamilla was paid by MIF as a senior evaluation consultant to this project. He maintained his scientific independence throughout the project.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the Mondelēz International Foundation (MIF).