
Abstract
Introduction
Childhood obesity is one of the major global public health challenges of the 21st century. In 2016, approximately one in five children aged 5–19 years were overweight and 6.8% were living with obesity (World Health Organization; World Health Organization, 2019). Levels are continuing to rise around the world as demonstrated by a recent global analysis showing the prevalence of obesity rose eightfold among girls and nearly ninefold among boys aged 5–19 years from 1975 to 2016 (Abarca-Gómez et al., 2017). Obesity during childhood poses immediate health risks (Cote et al., 2013; Lloyd et al., 2012; Bacha and Gidding, 2016; Di Bonito et al., 2018), and often persists into adulthood (Gordon-Larsen et al., 2010) where it is associated with increased risk of major non-communicable diseases (NCDs) including coronary heart disease, stroke, type 2 diabetes, and several types of cancer (Guh et al., 2009; Lauby-Secretan et al., 2016). While the drivers of obesity are complex, poor diet is a leading risk factor. In 2017, unhealthy diets were found to be responsible for more deaths globally than any other risk factor (Afshin et al., 2019). Unhealthy diets are generally those low in fibers, fruits, vegetables, legumes, whole grains, nuts and seeds, milk, seafood, calcium, and healthy fats (omega 3 fatty acids and polyunsaturated fatty acids) and high in trans-fatty acids, sodium, red or processed meat, and sugar-sweetened beverages (SSBs) (Afshin et al., 2019).
Spurred by the complex nature of obesity, intersectoral partnerships have been promoted as an important tool for responding to the childhood obesity epidemic (Hendriks et al., 2013; Institute of Medicine, 2015). As the understanding of drivers of childhood obesity has expanded, so too has the need for a diverse range of expertise and skill sets to address the public health problem. Intersectoral partnerships bring together different sectors of society (e.g. healthcare, education, housing, law enforcement, agriculture, transportation etc.) to collaborate on a shared issue. Public–private partnership (PPP) is an umbrella term used to describe the continuum of intersectoral partnering arrangements between governmental and private sector entities for the purpose of supporting governments’ broader service responsibilities (World Bank, 2017; Roehrich et al., 2014). The term rarely appeared in the literature prior to the 1990s, but has grown exponentially due to (i) skepticism of private sector-led solutions, (ii) a growing pattern of collaboration with national governments, and (iii) investments by high-net-worth individuals (Roehrich et al., 2014; Barr, 2007). Today, PPPs are promoted as a critical component of the Sustainable Development Agenda 2030 through Goal 17 (United Nations Sustainable Development Goals, 2015), which aims to “Encourage and promote effective public, public-private and civil society partnerships, building on the experience and resourcing strategies of partnerships” (p. 1).
Proponents of addressing childhood obesity through PPPs argue the issue is too complex to be addressed by governments alone (Institute of Medicine, 2012), that PPPs play a vital role in modifying the food supply (Institute of Medicine, 2012; Fanzo et al., 2021), are important for promoting health in all policies (Hendriks et al., 2013), contribute important shared resources and expertise (Institute of Medicine, 2012), and can be instrumental for driving research agendas (Perry et al., 2015). Critics of PPPs have focused largely on the conflicts of interest introduced when public organizations partner with businesses motivated by commercial interests (Institute of Medicine, 2012; Fanzo et al., 2021; Ralston et al., 2020). Conflicts of interest may be irreconcilable depending on the initiative and partners involved. For example, in addressing childhood obesity, it would be unlikely for a health promotion organization to maintain credibility while also partnering with an organization known to use aggressive and predatory marketing tactics toward young children (Institute of Medicine, 2012). However, other risks entailed with PPPs includ information sharing outside the partnership, poor participation in the partnership, concerns pertaining to endorsement perceptions, and undue influence over the scientific process (Institute of Medicine, 2012).
To the author's knowledge, no previous reviews of the PPP literature pertaining to childhood obesity have been undertaken. The purpose of this review was to describe the effects of interventions carried out through PPPs on diet-related obesity risk factors among school-aged children.
Theoretical background
Defining PPPs
Despite its popularity, definitions and concepts for PPPs are often contested, and no single definition of a PPP exists in the field of nutrition (Roehrich et al., 2014; Fanzo et al., 2021). In line with an Institute of Medicine (IOM) report, this review embraced a wide range of partnering arrangements (Institute of Medicine, 2012). The IOM emphasized the value of involving all sectors in working together to tackle complex public health problems, such as obesity, including government, academia, industry, and nongovernmental organizations (Institute of Medicine, 2012). Figure 1 shows the conceptual model used to define PPPs in this review. The public sector is comprised of national and subnational governments and governmental services. The private sector is divided into the business sector and the nongovernmental/academia sectors, broadly aligning with the “for-profit” and “nonprofit” delineation (Bajracharya and Hastings, 2015).
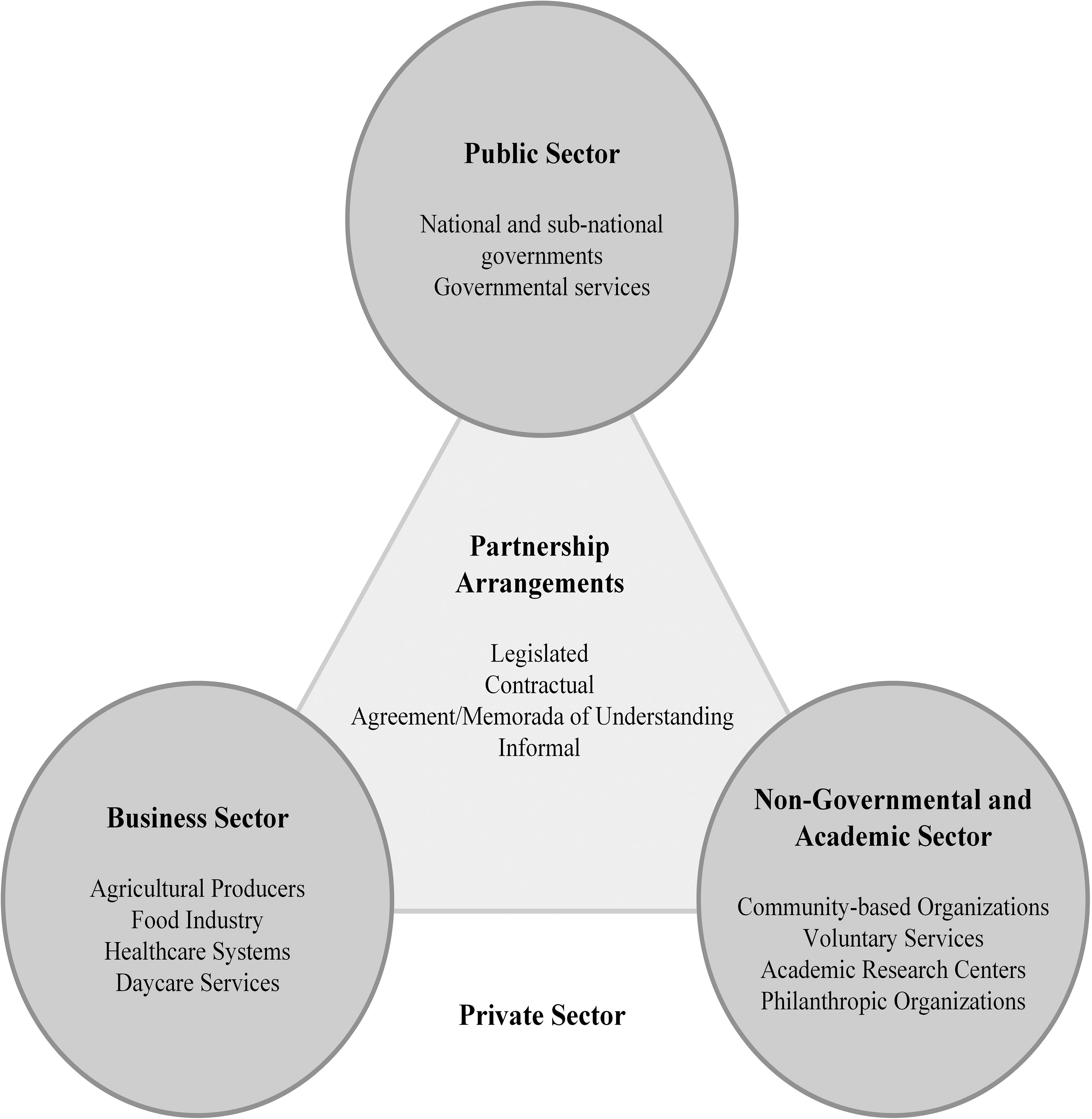
Conceptual model of public–private partnerships (PPP) for childhood obesity prevention and management.
Methods
Study design
This review follows the methodological guidelines of a systematic literature review (Tufanaru et al., 2017). Systematic literature reviews seek to provide a comprehensive, unbiased synthesis of studies on a particular topic through a systematic and transparent approach (Tufanaru et al., 2017). Based on the study objective, the following Participants, Intervention, Comparison, and Outcome (PICO) framework (O’Connor et al., 2008) was developed to guide the review:
Inclusion and exclusion criteria
Articles were eligible for inclusion if they met the PICO criteria above. Studies were excluded if they were not available in English, were not published in peer-reviewed journals, and were not primary research studies.
Healthy school-aged children were defined as those with an absence of complex or chronic diseases based on clinical signs and symptoms. However, given the prevalence of overweight and obesity, studies inclusive of children with overweight or obesity in the absence of other complex chronic diseases were included. Studies focused exclusively on children aged less than 5 years were excluded, as the definition of obesity changes for this age group (World Health Organization [WHO]). PPPs were defined as any partnering agreement between a public and private sector entity as described in the study design section. Studies that did not include sufficient description to allow for partners’ identification were excluded. As studies evaluating PPPs were unlikely to have a comparator or control group, none were required for inclusion.
Primary outcomes were changes in F&V consumption, SSB consumption, or energy-dense food consumption, as these are known diet-related risk factors for childhood obesity (Poorolajal et al., 2020) and food consumption behaviors applicable to both high- and low-income countries. Studies measuring changes in access to or acquisition of these food groups were included as these are proxy measures of consumption. Studies examining only non-dietary obesity risk factors (e.g. physical activity, sedentary behavior, sleep duration, etc.) were beyond the scope of this review and therefore excluded. Studies reporting only changes in BMI were included if any of the previous diet-related risk factors were described as being targeted through the PPP intervention, but only BMI measures were reported as outcomes within the study.
Search strategy and study selection
A search for articles between January 1990 and December 2021 was performed on 3 January 2022 using the electronic databases MEDLINE, PsycInfo, and Web of Science. These three databases encompass a wide range of research across natural sciences, health sciences, and social sciences, providing an extensive overview of published literature in the fields of public health, childhood obesity, and behavior change interventions. The start date for the search was based on previous reviews demonstrating PPPs rarely appeared in the literature before this time point (Barr, 2007; Roehrich et al., 2014). The search was undertaken with a uniform set of search terms, along with Boolean logic modified to the select database (Supplementary Table 1).
One reviewer undertook both the abstract and full-text screening. Ten percent of full-text articles were double-screened to ensure intra-rater reliability. The database search resulted in 276 articles. After removing duplicates, 223 studies remained. The initial round of title and abstract screening yielded 67 eligible articles. A further round of full-text screening resulted in eight articles for inclusion in this review (Figure 2). All screening was undertaken using the Covidence systematic review software (Veritas Health Innovation, 2021).
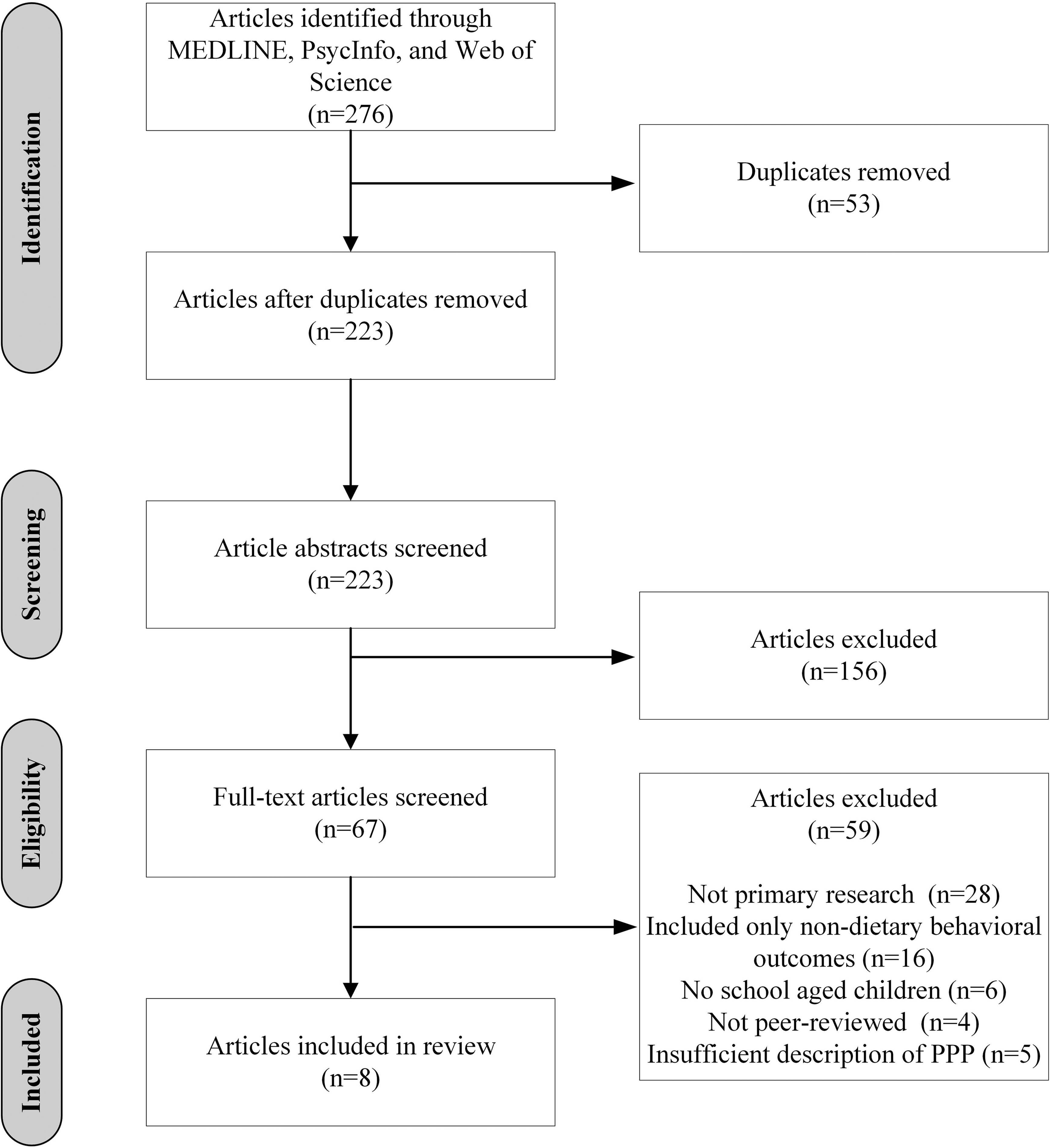
PRISMA diagram.
Data extraction and analysis
Articles included in this review were analyzed and data were extracted for details on the following categories: study characteristics (publication year, country of study, study design, research aims, intervention, study participants, relevant risk factors targeted, and critical appraisal), partners involved (partner names and partner sectors), description of partnerships (partnership objectives and partnering arrangements), and partnership outcomes (effects on diet-related obesity risk factors). All data were collected, stored, and analyzed in Microsoft Excel.
A critical appraisal of study quality was undertaken for each of the included studies using the Quality Assessment Tool for Quantitative Studies from the Effective Public Health Practice Project (EPHPP) (Thomas et al., 2004). Overall study quality was assessed based on eight criteria: selection bias, study design, confounders, blinding, data collection methods, withdrawals and dropouts, intervention integrity, and analyses. Global ratings of strong, moderate, or weak were calculated following EPHPP scoring guidelines.
Given the heterogeneity of study designs related to PPPs and childhood obesity prevention and management, the effect of PPPs on diet-related obesity risk factors was evaluated on a descriptive basis, rather than quantitatively. Following data extraction and critical appraisal, data were organized according to the type of partnership and frequency counts were calculated for specific study attributes.
Results
Characteristics of studies included in the review
This review included 8 primary research studies. All studies took place in the United States and were published between 2010 and 2017. A summary of study characteristics is available in Table 1. Most studies were cohort studies (75%; n = 6), apart from one quasi-experimental study and one case study. Study participants ranged in age from approximately 5–17 years of age, with 50% of studies targeting low-income children. Three studies targeted only children with overweight or obesity.
Description of studies included in the review.
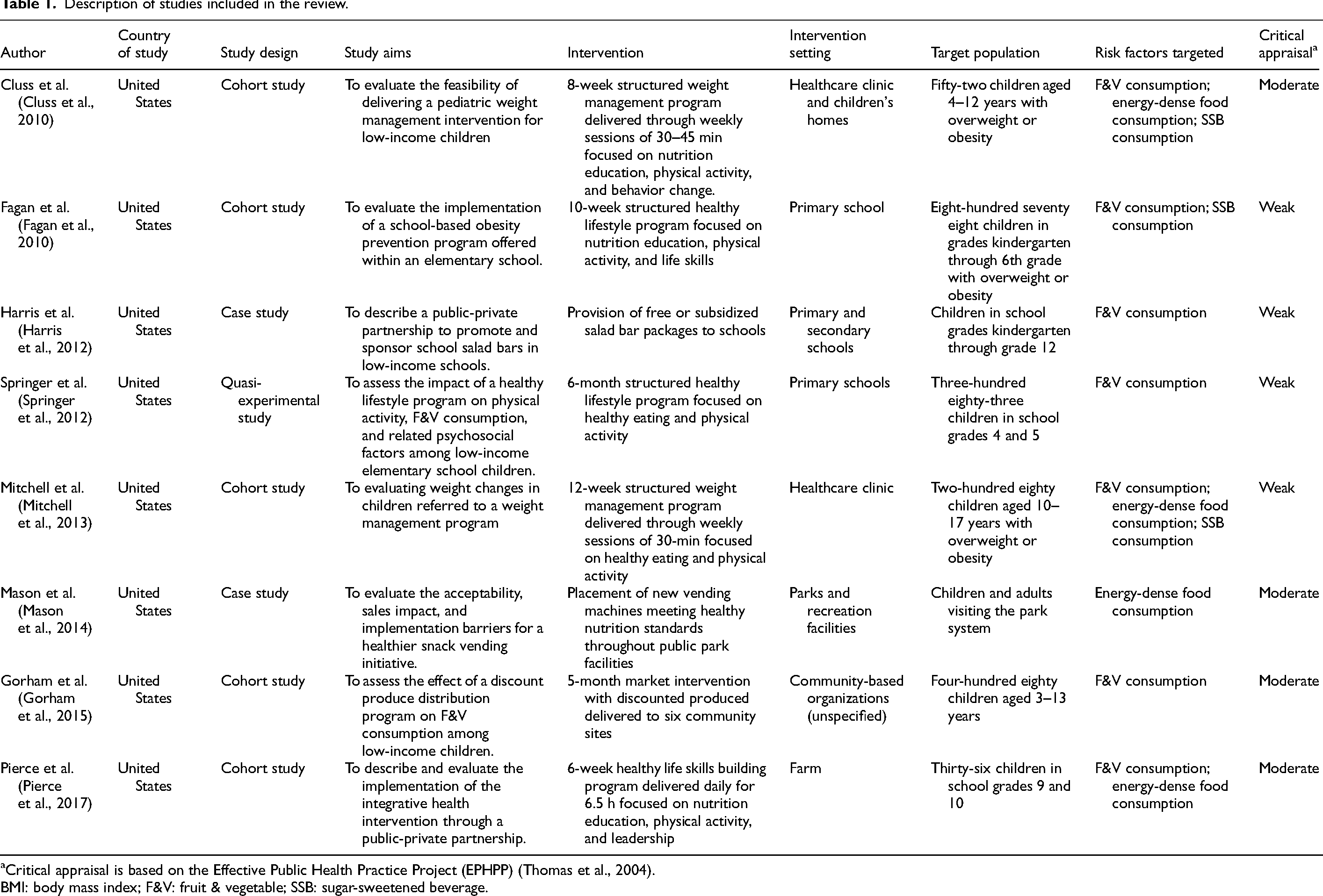
Critical appraisal is based on the Effective Public Health Practice Project (EPHPP) (Thomas et al., 2004).
BMI: body mass index; F&V: fruit & vegetable; SSB: sugar-sweetened beverage.
The majority of studies (62.5%; n = 5) included structured, healthy lifestyle interventions, with varying degrees of intensity and duration. The remaining interventions focused on changes to children's food environment. Schools were the most frequently cited setting for delivering interventions (37.5%; n = 3). Nearly all studies included intervention components aimed at behavior change around F&V consumption (88%; n = 7), followed by energy-dense food consumption (50%, n = 4), and SSB consumption (38%; n = 3). A critical appraisal of study quality found half of the studies were of moderate quality and half were of weak quality based on the EPHPP tool (Thomas et al., 2004).
Partnerships and partnering outcome of studies included in the review
A description of the partnerships undertaken to address diet-related obesity risk factors is listed in Table 2. All studies included both public sector and business sector partners. Most studies included partnerships across all three sectors: public sector, business sector, and nongovernmental/academic sectors (75%; n = 6). Public sector partners were most often state Medicaid programs (25%; n = 2), federal food assistance programs (25%; n = 2), and public schools (25%; n = 2). Other public sector partners included public parks and an elected government office. Business sector partners tended to be food producers (25%; n = 2), food retailers (25%; n = 2), and private healthcare providers (25%; n = 2). Other business sector partners included a private health insurance plan and a commercial weight loss program. Out of the six studies that included nongovernmental/academic sector partners, the most common partners were philanthropic organizations and academic research centers.
Description of partnerships and partnering outcomes included in review.
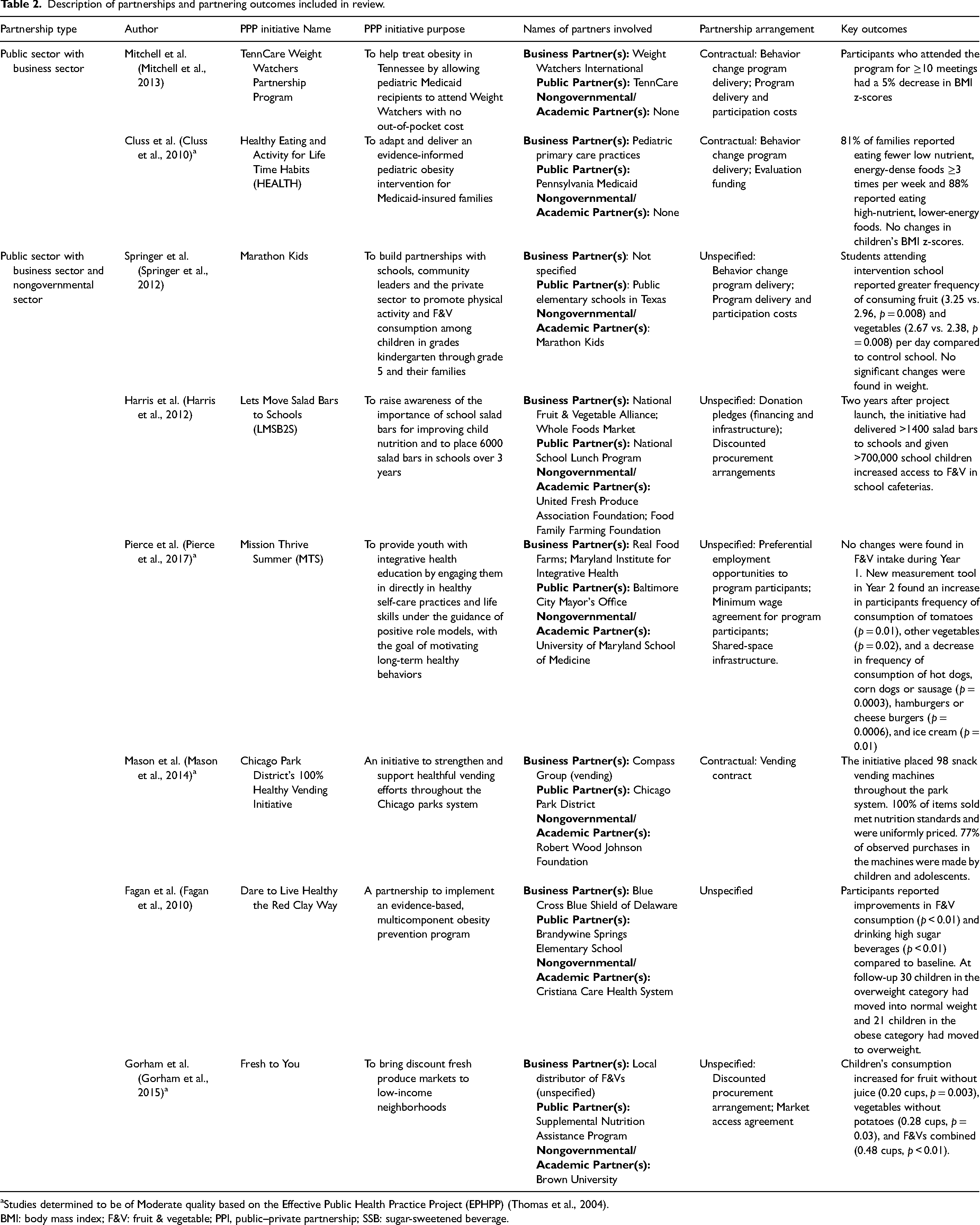
Studies determined to be of Moderate quality based on the Effective Public Health Practice Project (EPHPP) (Thomas et al., 2004).
BMI: body mass index; F&V: fruit & vegetable; PPI, public–private partnership; SSB: sugar-sweetened beverage.
Most partnering arrangements described in the studies were contractual arrangements (38%; n = 3), with two focusing on the delivery of a structured healthy lifestyle intervention and one on a vending contract. However, the majority of studies (62%; n = 5) did not specify the legal mechanism underpinning their partnership and provided limited descriptions of the products or services provided by different partners. Some of these partnering arrangements included discounted procurement arrangements, shared-space infrastructure, preferential employment opportunities, donation pledges, and market access agreements.
The small sample size and study heterogeneity limits comparisons across studies. Interventions varied by intervention components, duration, delivery settings, and populations targeted. Of the four studies with moderate quality ratings, three found decreases in energy-dense food consumption or the availability of energy-dense foods. One study showed significant increases in F&V consumption between baseline and follow-up of a 5-month healthy lifestyle intervention. Only one moderate quality study measured changes in BMI, and no difference was found in BMI z-score between baseline and follow-up. Of the four studies with weak quality ratings, three found increases in F&V consumption or availability of F&Vs. Three studies included outcome BMI measures, of which two found decreases in BMI at follow-up. The one study that reported on changes in SSB consumption found significant decreases in SSB consumption following a 10-week healthy lifestyle intervention.
Discussion
Childhood obesity is a serious and costly public health problem, driven by multiple and interacting genetic, behavioral, social, and environmental factors. Novel approaches and new structures, including PPPs, are currently promoted as mechanisms to address the complex nature of the challenge (Institute of Medicine, 2015; Institute of Medicine, 2012; Hendriks et al., 2013).
To the author's knowledge, this is the first systematic literature review to describe the effects of interventions carried out through PPPs on diet-related obesity risk factors among school-aged children. The results suggest that certain PPPs may be beneficial mechanisms for addressing diet-related obesity risk factors among school-aged children. However, the small sample size and heterogeneity in study design, target populations, intervention components, settings, and risk factors targeted all limit comparisons. Moreover, few studies described the financial or legal arrangements that governed their partnerships, much less the challenges to implementing interventions within these legal or financial frameworks. While all studies were of moderate to weak quality, those which reported on outcomes relevant to this review found either no changes or beneficial changes in diet-related obesity risk factors.
When it comes to issues of public health, engagement between the public and private sectors, particularly the business sector, is often complex and contentious. Valid concerns exist as to whether commercial interest can be balanced with public health goals or whether the risk to public institutions’ credibility outweighs any potential benefit of partnering (De Pinho Campos et al., 2019). This review found business sector partners participating in PPPs were primarily food producers, food retailers, and private health care providers. No PPPs with food manufacturers (i.e. those responsible for processing raw ingredients into packaged, edible food products) were identified. This may reflect a risk reduction strategy on the part of public sector actors in opting to partner with only certain actors within the food industry. The food industry is not one monolithic group, but encompasses all the actors involved in food production, processing, distribution, consumption, and ultimately disposal. Partnerships with those who produce food (e.g., Fruit and Vegetable Growers’ Association) and those who retail a wide range of food products (e.g., grocery store chains) may carry inherently less risk to public partnerships than those who manufacture highly processed foods and beverages. Policy makers interested in partnering with actors in the food industry may benefit from developing a conflicts of interest policy, using risk-based and due diligence approaches to identify conflicts of interests, and establishing a framework for managing these conflicts. Some guidance tools are readily available through the Scaling Up Nutrition Movement (Scaling Up Nutrition Movement, 2014), the WHO (Ralston et al., 2020), and the Ontario Ministry of Health (Kraak, 2014).
While this review sought to describe and characterize the different partners involved in PPPs and their partnering arrangements, this was challenging on several fronts. First, a high level of ambiguity exists in classifying partners as either “public” or “private”. For organizations like healthcare systems and schools, country-specific context often determines whether an entity is “public” or “private”, making classification and comparison across contexts challenging. Philanthropic organizations, largely classified as “nonprofits” and excluded from research on PPPs, can still have questionable ties to commercial interests. For example, the CDC Foundation, and subsequently the WHO Foundation, have both received criticism for being pass-through nonprofits, allowing their namesake organizations to receive industry funding that would otherwise have been prohibited due to conflicts of interest (Lenzer, 2015; Maani et al., 2021). The current review embraced a broad definition of “private” in an attempt to address these nuances by including both for-profit and nonprofit private organizations. Even with a broader definition, a strictly binary classification of “public” versus “private” is likely limiting. Future efforts aimed at developing a comprehensive taxonomy to classify the different partnering mechanisms across sectors would greatly benefit the field of PPP research. Finally, very few studies included in this review provided details on the governance structure, legal, or financial mechanisms underpinning the PPPs. Partnership arrangements span a continuum ranging from highly formalized agreements (e.g., legislated or formal contracts) to informal agreements (Bajracharya and Hastings, 2015). Understanding these arrangements can shed light on power dynamics, resource contributions, accountability mechanisms, etc. Public sector funders can improve the transparency of partnering arrangements by requiring these to be disclosed for all publicly funded grant recipients.
Limitations
This systematic literature review had several limitations. First, the outcomes of interest were narrow and excluded other known diet-related obesity risk factors, such as eating breakfast, family mealtimes, and alcohol consumption (Poorolajal et al., 2020). These risk factors were excluded because they are often culturally specific, while F&V consumption, SSB consumption, and energy-dense food consumption were likely to be applicable across contexts. Second, the literature databases and keyword search string likely limited the search results. Given the complex nature of PPPs, terminology is often inconsistent when describing these relationships. The keywords used may not have been sufficiently broad enough to capture many studies involving both public and private partners. Finally, the studies ultimately included in this review all originated from the United States. This finding may reflect unconscious selection bias on the part of the reviewer or context-specific terminology used in the search string.
Conclusion
Childhood obesity is a serious and complex public health problem, driven by many compounding risk factors, including unhealthy diets. It has been argued that collaboration across all sectors, including the private sector, is needed to address the drivers of obesity in places children live, learn, and play. Nevertheless, little is known about the different types of PPPs undertaken to address diet-related obesity risk factors nor what effect interventions carried out through these partnerships have on school-aged children. This review synthesizes the evidence on PPPs pertaining to diet-related risk factors for childhood obesity. While all studies were of moderate to weak quality, the results reveal either no changes or beneficial changes in children's F&V consumption, SSB consumption, energy-dense food consumption, or BMI. Business sector partners largely represented food producers, food retailers, and private healthcare providers. Few studies described the financial or legal arrangements that governed their partnerships. Given the ambiguity around defining PPPs, future research efforts are needed to develop a taxonomy for better identifying and classifying the different partnering arrangements that can exist between public and private sector partners to improve public health.
Supplemental Material
sj-docx-1-nah-10.1177_02601060221136184 - Supplemental material for Effects of public–private partnership on diet-related obesity risk factors among school-aged children: A systematic literature review
Supplemental material, sj-docx-1-nah-10.1177_02601060221136184 for Effects of public–private partnership on diet-related obesity risk factors among school-aged children: A systematic literature review by Megan R Harrison in Nutrition and Health
Footnotes
Acknowledgments
The author would like to acknowledge Christopher McBrearty for his contribution to the development of search terms.
Author contribution
Megan Harrison was responsible for the entirety of this manuscript, including the conceptualization, methodology, formal analysis, writing, and editing.
Consent for publication
The author approves of publishing this review
Data availability statement
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
As the work was completed as a review article, no ethical approval was needed or sought.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.