
Abstract
Background:
Intake of micronutrient-rich foods among children aged 6 to 23 months in Nairobi is low.
Objective:
This study aimed to assess existing coverage and utilization of micronutrient powders (MNPs), fortified staples, and iodized salt among children aged 6 to 23 months prior to implementation of an MNP program.
Methods:
A cross-sectional survey among caregivers of children aged 6 to 23 months (n = 618) was implemented in 7 neighborhoods within Nairobi County, representing the implementation area of the new MNP program.
Results:
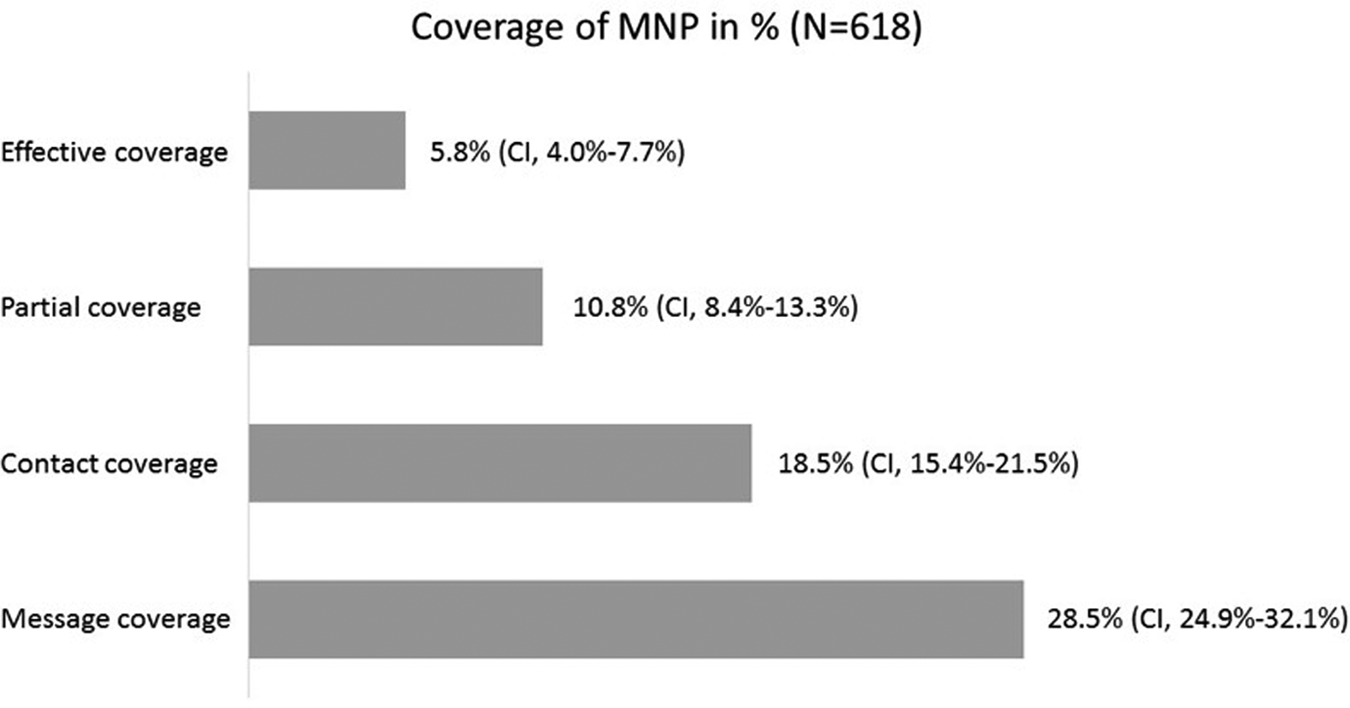
Results for MNP coverage and utilization showed 28.5% of all caregivers were aware of MNP, 18.5% had ever received MNP for their child, and 10.8% had fed MNP to their child in the previous 7 days. Effective coverage (ie, the child had been given the MNP at least 3 times in the previous 7 days) was 5.8%. Effective coverage of infants and young children with poor feeding practices was significantly lower as compared to those with non-poor feeding practices (coverage ratio, 0.34; confidence interval, 0.12-0.70). Most households purchased iodized salt (96.9%), fortified oil (61.0%), and fortified maize flour (93.9%). An estimated 23.9% of vitamin A requirements of children (6-23 months) were provided from fortified oil and 50.7% of iron from fortified maize flour. Most households consumed processed milk (81%).
Conclusion:
Coverage of MNPs in the surveyed neighborhoods was low. Coverage of fortified salt, oil, and maize flour was high and provided significant amount of micronutrients to children. Processed milk has potential as a vehicle for food fortification.
Introduction
The prevalence of micronutrient deficiencies is high among children in Kenya. According to the most recent estimates, 26.3% of children aged 6 to 59 months are anemic, 1 9.2% of the children younger than 6 years are vitamin A deficient, 1 21.8% are iron deficient, 1 83.3% are zinc deficient, 1 and 26.3% are stunted. 2 The diets of infants and young children in Kenya are largely plant-based and contain limited animal source foods that are rich in essential micronutrients. 2 Moreover, only a little over a half of children aged 6 to 23 months consume the minimum number of food groups deemed necessary for a nutritionally adequate diet. 2,3 Less than half of the children were reported to have consumed iron-rich foods the day preceding the survey in the 2014 Demographic Health Survey. 2 In many low-resource areas of Kenya, even in urban areas such as Nairobi, access to nutrient-dense complementary foods and intake of micronutrient-rich foods among children aged 6 to 23 months is a challenge. 4,5
As part of national effort to address micronutrient deficiencies, the Kenya Government supports several fortification interventions: Mandatory salt iodization has been in place since 1989 6 and mandatory fortification of wheat flour, maize flour, and vegetable oil has been in place since 2012. 7 Younger children may benefit from staple food fortification; however, due to high nutrient requirements during this age range, additional interventions are often necessary. 8 -10 Ensuring that infant and young child feeding (IYCF) practices are adequate is essential for healthy growth and development. This includes age-appropriate breastfeeding practices and the inclusion of nutrient-dense complementary foods in the diet from 6 months of age and above. In many low-resource areas of Kenya, access to nutrient-dense complementary foods is a particular challenge. One intervention to improve the micronutrient content of infant and young child diets is home fortification with micronutrient powders (MNPs). There is a strong evidence base supporting the efficacy of MNP for reducing anemia, 11-12 and as of 2014, 50 countries have implemented MNP programs. 13
Micronutrient powders were first introduced in Kenya as part of an effectiveness trial that was conducted in a rural region of the Nyanza Province which is located in the western part of the country. 14 This trial showed that the distribution of MNP through a community and market-based approach was effective in reducing the prevalence of iron and vitamin A deficiency as well as anemia among the children aged between 6 and 35 months. 14 Another trial with MNPs has also shown that MNPs improve iron status among children aged 6 to 23 months in Kenya. 15 As a result of this evidence base, the Government of Kenya has included MNP as part of the National Nutrition Action Plan 2012 to 2017. 16
In 2014, Global Alliance of Improved Nutrition, Philips Health Care Services, and Living Goods implemented a market-based (ie, available through sales) program in 7 neighborhoods of the Nairobi Eastlands. The primary objective of the present study was to determine the baseline MNP coverage and utilization mainly from existing free distribution through the government (ie, to determine the coverage of the existing MNP program in the area), especially among subgroups that may be more vulnerable to inadequate nutrient intake as a result of poverty or poor IYCF practices. The second objective was to determine the coverage of fortified oil, flour, and iodized salt. The third objective was to assess the potential of milk fortification.
Materials and Methods
Study Design, Setting, Participants, and Sampling
A cross-sectional survey was conducted among caregivers of children aged between 6 and 23 months living in 7 selected neighborhoods of Nairobi County (ie, Dandora, Umoja, Kayole, Mathare, Ruaraka, Bahati, and Njiru). A minimum sample size of 618 was calculated to measure the differences between the baseline survey presented here and subsequent coverage surveys to be completed after implementation of the program assuming an increase of 10% in MNP coverage (from 20% to 30%), a precision of 5%, a design effect of 2, and a non-response rate of 5%. Stratified sampling methods were used, where first the number of households selected per strata (ie, neighborhood) was proportionate to the population size estimated from the 2009 Kenya census. Second, households were randomly selected in each neighborhood using the modified Expanded Programme on Immunization (EPI) method. 17 Community health workers helped identify the boundaries of the neighborhoods and households with children aged between 6 and 23 months. If there was more than one child in the household in the target age range, the youngest child was selected.
Ethical Considerations
Research approvals were obtained from relevant authorities including the Ministry of Health (Reference: DNUT/ADMIN/12/1 of 4 November 2014) and the Nairobi County Government Research committee (Reference: CMO/NRB/OPR/Vol 1-2/106 of 17 November 2014). Written informed consent was sought from the respondents on arrival at the household.
Data Collection
A structured questionnaire, adapted from a standardized tool, 18 was administered to the main caregiver of the selected child by trained survey enumerators. Information was collected on demographic and socioeconomic status; water, sanitation, and hygiene practices; IYCF practices; hunger; and awareness, access, and utilization of MNP. Moreover, the questionnaire collected information on household consumption and purchase habits of oil and main flour consumed, as well as purchase habits of salt and milk products. Mid-upper arm circumference (MUAC) measurement was used to assess severe acute malnutrition. Children with an MUAC below 115 mm and/or edema were defined as acutely malnourished and were provided with nutrition counseling and written referral to the nearest health facility for further management.
Data Entry and Analysis
An adaptation of the Multidimensional Poverty Index (MPI) was used to classify households as poor or nonpoor. 19 The MPI is an indicator that takes a value between 0 and 1 and which consists of a weighted sum of 3 dimensions, each contributing one-third of the sum: health, education, and living standards. The health dimension is composed of 4 indicators each worth one-twelfth of the sum: household hunger, child and caregiver malnutrition (MUAC as proxy), infant and young child recent mortality, and coverage of preventative services (ie, vitamin A supplementation and vaccine against tuberculosis). The education dimension consists of 2 indicators each worth one-sixth of the sum: education of caregiver and school attendance of school-age children. The living standards dimension consists of 5 indicators each worth one-eighteenth of the sum: electricity in the household, type of flooring in dwelling, type of cooking fuel, number of key assets, safety of drinking water, and type of latrine. Each indicator is given the value 0 when the response corresponds to the characteristics of a nonpoor household; otherwise, the value is one-twelfth, one-sixth, or one-eighteenth of the sum according to the indicator. Households with an MPI score of one-third or more were considered as poor, and the household with an MPI score below one-third as nonpoor. Household hunger was assessed using the Household Hunger Scale (HHS). 20 The HHS is an indicator of household hunger that is focused on the food quantity dimension of food access. The questions ask whether or not a specific condition associated with the experience of food insecurity ever occurred during the previous 4 weeks (30 days). The IYCF practices were analyzed using the Infant and Child Feeding Index (ICFI). 21 The ICFI score combines age-specific scores for breastfeeding, dietary diversity, and meal frequency into an age-appropriate child feeding practices score which ranges between 0 and 6. Children with an ICFI score of 6 were considered as having optimal IYCF practices; children with an ICFI score of less than 6 were considered “at-risk” of having micronutrient deficiencies due to suboptimal IYCF practices. Four MNP coverage processes were constructed as proposed by Tanahashi. 22 These include “message coverage” (ie, the caregiver has ever heard MNP), “contact coverage” (ie, the selected child has ever been given MNP), “partial coverage” (ie, the selected child consumed at least 1 sachet of MNP in the past week), and “effective coverage” (ie, the selected child consumed at least 3 sachets of MNP in the past week). Moreover, 2 summary measures were calculated: “met need” (ie, the proportion of children considered as at-risk of poverty or poor IYCF practices that are covered by MNP) and “coverage ratio” (ie, the ratio of a measure of coverage in children considered as at-risk to that measure of coverage in children considered as not-at-risk). Coverage ratio values (95% confidence interval [CI] that do not include 1) below 1 indicate lower coverage in at-risk group, above 1 indicate higher coverage in at-risk group, and of 1 indicate equal coverage in both groups. The CIs of the coverage ratio indicate whether the differences in coverage between at-risk and not-at-risk are significantly different. For example, if the CI of a coverage ratio below 1 includes a value equal to or above, then the coverage levels are not significantly different between the 2 groups. Correct MNP preparation was defined as follows: not adding to hot food, adding to solid or semisolid foods, adding only the amount of food the child will finish, adding just before feeding the food to the child, using 1 sachet for 1 meal, and using 1 sachet per day.
The individual consumption of oil and flour was calculated based on the household consumption over a reported period and using the adult male equivalent method. 23 The coverage of fortified oil, flour, and salt was estimated based on the brands of the product mainly consumed by the household and whether this brand was known to be fortified or not. The contribution of fortified oil and flour to vitamin A and iron intakes, respectively, was calculated using individual consumption estimates, recommended nutrient intakes (RNIs) 23 (for iron, bioavailability was considered to be low, ie, 5%), and minimum required fortification level (ie, 10 ppm vitamin A for oil and 15 mg/kg iron for flour). 7
Data were entered using Microsoft Excel (version 2007) and were cleaned and analyzed using SPSS (version 16 and 20) and R (version 3.1.0). Mean (95% CI) was used as the measure of central tendency for normally distributed variables, and median (25%-75%) was used for non-normally distributed variables. Pearson χ2 test of independence and independent samples t test were used to test for significance and comparison of means by MPI. Percentage met need and coverage ratios were calculated using a blocked weighted bootstrap 24 estimation technique, and 400 bootstrap replicates were used. Significance level was set at .05.
Results
Socioeconomic Characteristics of the Survey Population
Six hundred eighteen households with a child aged 6 to 23 months completed the survey. The survey population characteristics are shown in Table 1. Despite selection of the youngest eligible child in the household, the mean age of the surveyed child was 14.1 months. Although only 3.6% of the households were considered as poor by the MPI, 11.8% of households reported experiencing moderate or severe hunger in month preceding the survey and 72.0% did not have an improved toilet facility. About half of all the caregivers interviewed (50.3%) had ever been visited by a community health worker at their home, and among those caregivers, nearly all (98.7%) had been visited in the past month at the time of data collection. The majority of the respondents reported that their households owned a radio and a television (76.5% and 80.3%, respectively) and nearly all respondents (93.9%) owned mobile phones. Most of the children aged between 5 and 14 years were attending school (97.6%).
Survey Population Demographics.a
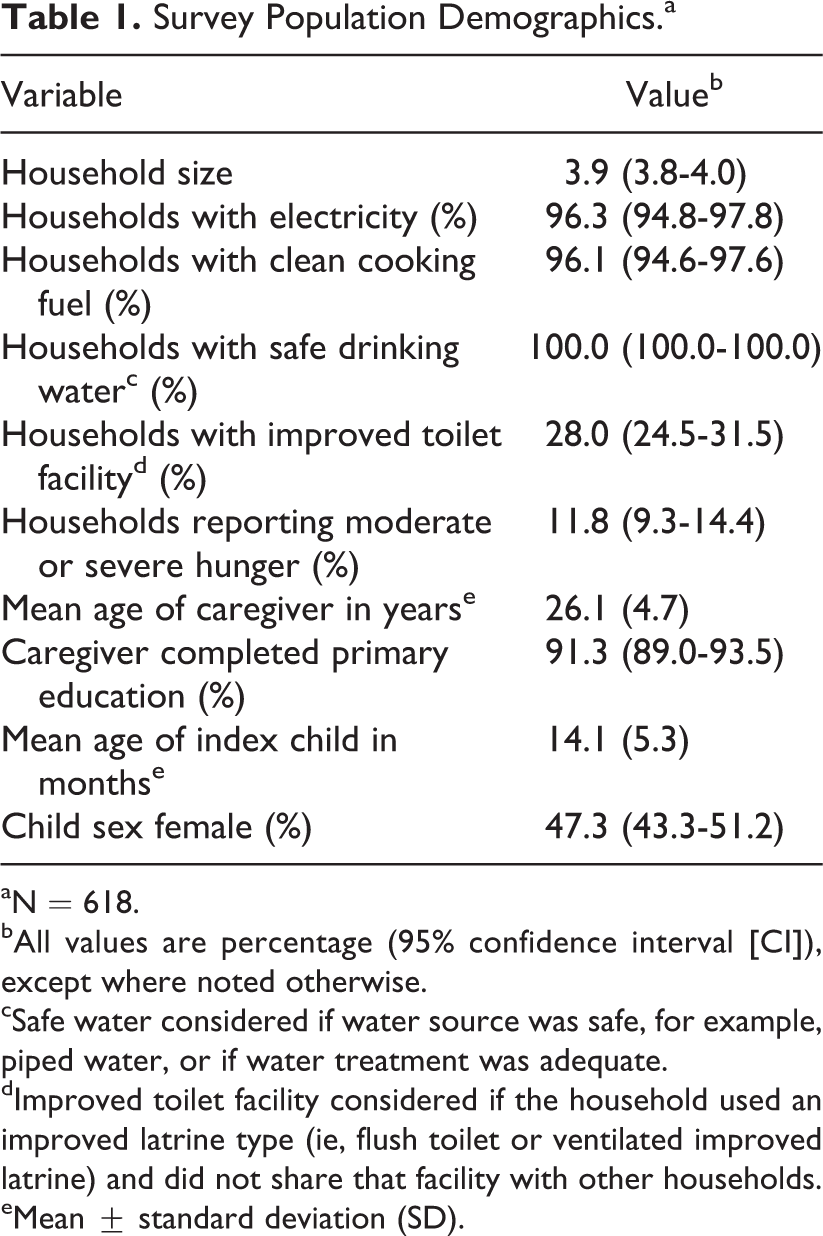
aN = 618.
bAll values are percentage (95% confidence interval [CI]), except where noted otherwise.
cSafe water considered if water source was safe, for example, piped water, or if water treatment was adequate.
dImproved toilet facility considered if the household used an improved latrine type (ie, flush toilet or ventilated improved latrine) and did not share that facility with other households.
eMean ± standard deviation (SD).
The IYCF Practices
The mean ICFI score was 5.4 (CI, 5.3-5.5; Figure 1). Of all the children surveyed, 78.6% were breastfed, 86.1% of them were fed an adequate age-specific dietary diversity, and 84.3% of the children were fed at an adequate age-specific frequency, while only 58.9% of the children were fed at the adequate frequency, with an adequate dietary diversity and breastfed simultaneously. Almost all children (96.9%) had been given a vitamin A supplement in the past 6 months.
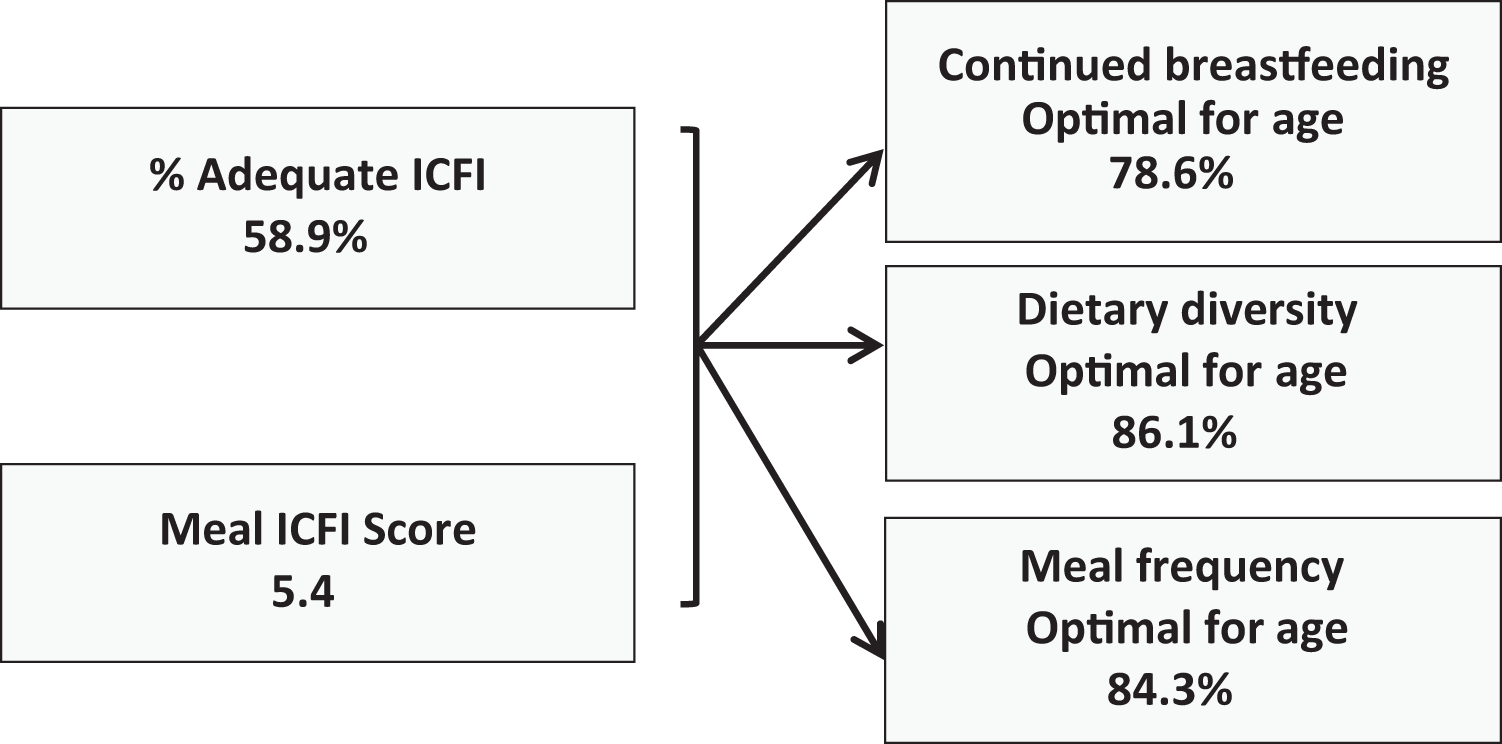
Infant and young child feeding (IYCF) practices according to the Infant and Child Feeding Index (ICFI) score.
Coverage and Utilization of MNP
The different coverage levels of MNP are presented in Figure 2. Among the 28.5% of caregivers who had ever heard about MNP (ie, message coverage, n = 176), the main source of information was government health clinics (84.7% of caregivers who heard of MNP). Other insignificant sources of MNP as reported by those who had heard about MNP were shop/kiosk, relatives/friends, or religious organizations (5.6%).
Micronutrient powder (MNP) coverage in survey area.
The majority of the caregivers (61.4%) who ever gave MNP their children (ie, contact coverage, n = 114) received it at no cost from health facilities. Those who paid for the MNPs paid less than 2 Kenyan shillings (2 CTS USD) per sachet. The mean number of MNP sachets consumed in the past week by the 18.5% of children who had ever been given MNP was 1.3 (CI, 1.1-1.6), and 56.1% of these children were given MNPs that were reportedly prepared correctly. Micronutrient powders were given at all mealtimes of the day but most commonly with the morning snack (41.7%). Only 11.7% of the caregivers of children who had ever been given MNP reported that they liked MNP as it improved the appetite of their child, while 6.6% reported MNP was good for the health of their child. The main potential barriers to optimal coverage that were identified included perception that the MNP do not bring any added benefits (19.4%), incorrect preparation of the MNP (10.4%), and unavailability (3.1%).
The percentage met need and coverage ratios for children with poor IYCF practices are presented in Table 2. The results show that the percentage met need is low (between 3% and 27%). Coverage is lower in children with poor IYCF practices, but only significantly lower for effective coverage (coverage ratio of 0.34). Given the low number of households classified as poor by the MPI and the lack of significant differences between poor and nonpoor groups (P>.05), the results are not presented.
Percentage Met Need and Coverage Ratios for Children With ICFI Score <6 ().a
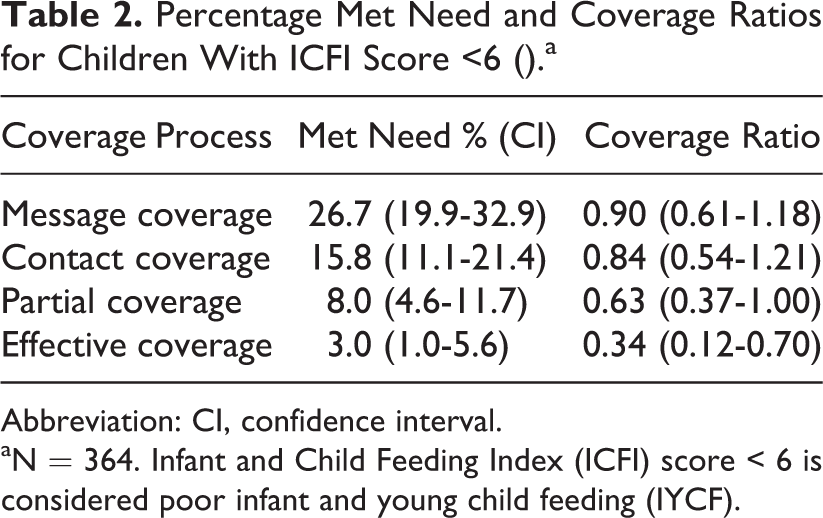
Abbreviation: CI, confidence interval.
aN = 364. Infant and Child Feeding Index (ICFI) score < 6 is considered poor infant and young child feeding (IYCF).
Coverage and Consumption of Fortified Oil
Oil was consumed at the household level by 77.5% (CI, 74.2%-80.8%) of the households, and fortified oil was consumed by 61.0% (CI, 57.2%-64.9%) of the households. On average, 44.6 g/d (CI, 34.5-54.7) of oil was consumed per capita and children aged between 6 and 23 months consumed 12.8 g/d (CI, 9.7-15.8). The amount of oil consumed did not differ between poor and nonpoor households. Fortified oil provided 23.9% (CI, 17.1%-30.7%) of the vitamin A RNI of children aged between 6 and 23 months.
Coverage and Consumption of Fortified Flour
Maize flour was reported as being the main flour consumed at the household level in 98.1% (CI, 97.0%-99.2%) of the households, and 93.9% (CI, 92.0%-95.8%) of the households consumed fortified maize flour.
The mean maize flour consumption was 632.4 g/d (CI, 504.2-760.6) per capita. Children aged between 6 and 23 months consumed 46.8 g/d (CI, 38.0-55.6), which covered 50.7% (CI, 40.1%-61.4%) of their needs in iron. The amount of maize flour consumed was not significantly different between poor and nonpoor households.
Coverage of Iodized Salt
Almost all households (99.5%, CI, 99.0%-100.0%) reported purchasing packaged salt, and 96.9% (CI, 95.6%-98.3%) purchased a salt brand that is iodized.
Household Consumption of Dairy Products
Milk was widely consumed in the population surveyed: About 81.0% of households used fresh processed milk, 5.0% consumed ultraheat temperature pasteurized milk, and 11.5% consumed unprocessed milk. Consumption of other dairy products, such as powdered milk, flavored milk, and yoghurts, was not common (<1.0%). There were no significant differences in dairy product consumption patterns between poor and nonpoor households. Majority of the respondents (81.4%) reported that they would consider using of fortified milk if available.
Discussion
In the surveyed population, the current coverage of MNP was found to be low (5.8% effective coverage) and insufficient to meet the current high level need of children, as showed by the high percentage of children with inadequate IYCF practices (41.1%). The coverage of fortified staple foods, on the other hand, was high and provided a nonnegligible amount of key micronutrients to children.
In previous analyses assessing the met need of fortified food products, 25 the MPI was used to identify households at risk of poverty, poverty being a risk factor for poor nutrition outcomes. However, the MPI may not be a suitable indicator of poverty for households living in urban areas in Kenya. In fact, although the majority of the households seemed not at risk of poverty (ie, used clean cooking fuel, had access to electricity, had safe drinking water, had a television, had a radio, and had a mobile phone), a significant proportion experience hunger (11.8%) and did not have an improved toilet facility (72.0%).
Although the mean number of sachets of MNP (ie, 1.3) consumed by children per week was lower than the recommended 3 to 4 sachets per week, 26 it was higher than the 0.9 sachets per week consumed in an effectiveness study conducted in Western Kenya that were shown to be effective in reducing iron and vitamin A deficiency rates. 14 However, approximately half of the caregivers who had an experience giving MNP to their child did not add MNP to complementary foods according to recommendations. The new program will focus on increasing availability of MNP as well as providing caregivers with information on how to feed MNP to their children. In addition to health clinics, possible channels for communication could be mobile phones, television, and radio due to their widespread use (93.9%, 80.3%, and 76.5%, respectively).
The survey results indicate that the consumption of fortified oil and flour is widespread and contributes to significant increases in vitamin A and iron intakes, even among children aged between 6 and 23 months. In fact, an estimated 23.9% of the requirements of children aged between 6 and 23 months in vitamin A were provided from fortified oil and 50.7% of iron from fortified maize flour. In order to better assess the oil and flour fortification situation in Kenya, the results of this survey should be complemented with a market survey assessing the actual fortification levels of these two food vehicles. Similarly, the iodized salt coverage results show nearly all households consumed iodized salt.
Milk could be a promising vehicle for fortification in the Nairobi County. In order to further assess the feasibility of milk fortification in Nairobi County as well as national level, the milk market and industry (eg, degree of consolidation) and supply chain should be assessed, as well as the accessibility and affordability of fortified milk.
The main limitation of this study was that the results were not representative of the country, or of all Nairobi. The neighborhoods included in the survey were selected based on their inclusion in the project area of a new MNP program. Another limitation is that the levels of micronutrients in oil, flour, and salt were assumed based on the minimum required fortification level set by the country. The actual levels of micronutrients in these food vehicles were not measured in this survey and that the proportion of households consuming adequately fortified flour or oil or iodized salt could therefore not be assessed.
Conclusion
The current level of coverage of MNP in the middle-income neighborhoods of Nairobi was low, suggesting the need for additional strategies to improve the availability and accessibility of the MNP. For the existing program, there is the potential to significantly increase coverage by improving the availability and awareness of MNP and thereby reduce the prevalence of micronutrient deficiencies. However, special attention to information and training should be taken to ensure the correct utilization of MNP. The fortification of oil and maize flour should be continued as both provide a significant and complementary amount of nutrients to children aged between 6 and 23 months . In addition, high coverage levels of processed milk indicate that it is potentially an effective vehicle for food fortification.
Footnotes
Acknowledgments
The authors thank the Ministry of Health, Kenya, and the Nairobi County Government for the approval and permission to undertake this study; the Nutrition Information Technical Working Group for their contribution to the study methodology; and the data collection and entry teams, Community Health Volunteers, for their commitment during the data collection and entry period. The authors also thank Maurice Mutisya of African Population and Health Research Center, Nairobi, Kenya, for his support in data analysis and the respondents for their participation in the survey.
Author’s Contributions
A.T., C.M.M., and M.R. conceived the study. A.T., C.M.M., M.R., D.M.D.K., and G.J.A. participated in the development of data collection tools. D.M.D.K. supervised the data collection. D.M.D.K. and M.L. jointly conducted analysis. D.M.D.K., M.L., C.M.M., and A.T. drafted the manuscript. All authors participated in the revision and approval of the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflict of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Bill & Melinda Gates Foundation and the Kingdom of the Netherlands provided funding for this study.