
Abstract
Background
To prevent micronutrient deficiencies and address the double burden of malnutrition, Benin has implemented Infant and Young Child Feeding (IYCF) and food fortification policies for several years. Despite these efforts, significant micronutrient deficiencies persist, posing a public health problem.
Objective
This study aims to identify barriers and facilitators to the implementation of government policies on IYCF and food fortification in Benin.
Methods
We conducted in-depth individual interviews with 23 key national and local stakeholders involved in implementing these policies. The interviews were recorded, transcribed, and analyzed through a deductive and iterative process based on the study's objective.
Results
Stakeholders identified several barriers to policy implementation, including low staff motivation, exacerbated by poor personnel management and lack of recognition. Financial resources are insufficient despite organizational support. Training and awareness among health workers and producers are limited outside UNICEF's intervention areas. Traditional eating habits and cultural resistance impede the adoption of new practices. The monitoring system is complex and ill-equipped, hindering quality control of fortified foods. Facilitators include strong political commitment, partnerships with international nongovernmental organizations, and effective intersectoral collaboration. These partnerships have improved training and community awareness, though gaps remain. The involvement of local producers and professional associations also supports food fortification initiatives.
Conclusion
Nutrition policies in Benin face challenges such as low staff motivation and lack of resources. However, strong political commitment and international partnerships present opportunities to overcome these barriers.
Plain language title
Study of Challenges and Solutions to Improve Food Policies for Babies and Children in Benin
Plain language summary
Benin is implementing policies to improve the nutrition of babies and young children and to fortify foods to prevent vitamin and mineral deficiencies. However, the country continues to suffer from these deficiencies, posing a serious health problem. The study seeks to understand why these policies are not working as well as expected, and to identify what could improve them. The researchers interviewed the key people involved in these policies, recording, and analyzing their responses to identify the main problems and positive points. The interviews revealed several problems, notably that health workers are demotivated due to poor management and lack of recognition. Financial resources are insufficient, even with the help of international organizations. Training and awareness-raising are limited, especially outside UNICEF-supported areas. In addition, traditional eating habits and cultural resistance make the adoption of new practices difficult. However, some positive elements have been identified, including: strong political support, effective partnerships with international nongovernmental organizations, successful collaboration between different sectors and the involvement of local producers and professional associations. At the end of this study, we can conclude that nutrition policies in Benin face difficulties such as the lack of motivation of agents and the lack of resources. But, with strong political support and international partnerships, there is a good chance of overcoming these challenges.
Keywords
Introduction
Micronutrient deficiencies have a devastating impact on children's survival, growth, and development. Deficiencies in vitamin A, iron, folic acid, zinc, and iodine significantly increase the risk of mortality, morbidity, blindness, hearing loss, and anemia. These deficiencies hamper linear growth, cognitive development, learning abilities and school performance, reducing productivity, and earnings in adulthood. 1 Indeed, these deficiencies can be present throughout life, and may be associated, at older ages, with obesity and chronic disease. 2
Micronutrient deficiencies affect more than 2 billion people worldwide, with women of childbearing age, children, and the elderly being the hardest hit. 3 They account for around 7.3% of the global disease burden, and iron and vitamin A deficiencies are among the top 15 causes of the global disease burden, contributing to the increase in child mortality. 4 The World Health Organization (WHO) estimates that 42% of children under 5% and 40% of pregnant women worldwide are deficient in iron and vitamin A. 5 Pregnant women with severe anemia are twice as likely to die during or shortly after pregnancy than those without anemia. What's more, micronutrient deficiency during pregnancy can lead to low birth weight, as well as cerebral and vertebral malformations in their offspring. 6
In terms of prevention, the WHO and the Food and Agriculture Organization of the United Nations (FAO) have identified 4 main strategies to combat micronutrient malnutrition: nutrition education leading to improved diet quality, food fortification and biofortification, supplementation, and disease control measures. 7 Food fortification programs have been launched in the 15 member states of the Economic Community of West African States (ECOWAS) (Benin, Burkina Faso, Cape Verde, Ivory Coast, Gambia, Ghana, Guinea, Guinea Bissau, Liberia, Mali, Niger, Nigeria, Senegal, Sierra Leone, and Togo). To improve children's diets, WHO and the United Nations Children's Fund (UNICEF) recommend the implementation of an Infant and Young Child Feeding (IYCF) strategy in various countries. Its main objective is to promote optimal breastfeeding and nutrition practices for children from birth to 2 years of age. Currently, 98 countries have integrated various aspects of this strategy into their national policies. The strategy recommends initiation of breastfeeding within 1h of birth, exclusive breastfeeding for the first 6 months (with no other foods or liquids), continued breastfeeding for 2 years or more, and adequate, safe, and appropriate complementary feeding after 6 months. 8
IYCF is a key area for improving child survival and promoting healthy growth and development. The first 2 years of a child's life are particularly important, as optimal nutrition during this period will have the effect of reducing morbidity and mortality rates, as well as the risk of chronic diseases, and contribute to better overall development. 9
The development of the IYCF strategy was influenced by several events. The key external events that prompted the development of this strategy began in 1978, with the Alma-Ata Declaration on Primary Health Care, which emphasized nutrition as a fundamental right. 10 In 1981, WHO and UNICEF adopted the International Code of Marketing of Breast-milk Substitutes, a regulatory framework to protect breastfeeding. 11 In 1990, the World Conference on Nutrition drew attention to child malnutrition, followed by the Global Strategy for Infant and Young Child Feeding launched by WHO in 1992. 9
Internal events in the implementation of the IYCF strategy began in 2002 with the official launch of the initiative by UNICEF and WHO. In 2003, the World Health Assembly adopted IYCF recommendations, emphasizing the importance of exclusive breastfeeding for the first 6 months and adequate complementary feeding thereafter. 9 In 2004, several countries began to develop specific strategies and policies to implement IYCF in their local contexts. In 2006, the WHO published a “Strategy for Infant and Young Child Nutrition,” setting out concrete measures to be taken to improve infant feeding. 12 In 2012, at the 65th World Health Assembly, resolutions were adopted to reinforce the importance of IYCF in the fight against malnutrition. 13 In 2013, WHO updates its infant feeding recommendations, incorporating guidance on breastfeeding and complementary feeding. 12
In line with international recommendations, Benin has developed and made available to all stakeholders since 2010 a National Strategy for IYCF, including operational tools (training manuals, educational materials, etc). 14 At the end of the first 2010 to 2014 strategy, and in light of the new guidelines contained in the IYCF programming guide (published by UNICEF in 2012) and the framework for action defined at the second International Conference on Nutrition in Rome, Benin drew up its 2nd IYCF national strategy document covering the 2015 to 2019 period. 15 This strategy has since been implemented in all the country's sociohealth structures and nongovernmental organizations (NGOs) working in the field of Food and Nutrition. The overall aim of the strategy was to improve the nutritional status, growth, development, health and survival of infants, young children and mothers, through optimal nutrition, in order to help reduce infant and child mortality. Several years after the implementation of the IYCF strategy in Benin, the results of the Multiple Indicator Cluster Survey (MICS), Benin, 2021 to 2022 reveal that: 1 newborn in 4 is put to the breast within an hour of birth (25%); less than half (45%) of children under 6 months are exclusively breastfed; around 1 child in 4 is not introduced to solid or semisolid foods from 6 to 8 months; 1 child in 5 aged 6 to 23 months benefits from minimum acceptable dietary diversity. 16
Food fortification in Africa began in the early 1980s to address malnutrition and micronutrient deficiencies, particularly in vitamin A, iron, and iodine. 17 Africa was facing high levels of vitamin and mineral deficiencies, notably in vitamin A, iron, and iodine. Initially, the focus was on the iodization of salt, then, in the early 2000s, on the fortification of other staple foods such as flour and oil. 18 The African Food Fortification Initiative was launched at the African Union Summit in 2002, in partnership with the World Food Programme (WFP). 17 Fortification policies intensified and harmonized at regional level in the 2010s, with common regulatory frameworks and increased support from international partners. Indeed, regional economic communities such as ECOWAS are implementing regional fortification strategies, improving compliance and coverage. 18 Several countries are now developing fortification programs targeting rural and urban areas.
Food fortification has been regulated in Benin for several years by interministerial decrees. To prevent deficiencies in iodine, iron, zinc, B vitamins, vitamin A, and folic acid, the government has introduced provisions for the fortification of salt, wheat flour, and edible oils intended for human and animal consumption.19–21 To ensure the fortification of healthy foods and the selection of foods to be fortified, a Beninese Food Fortification Commission was created in 2012 by interministerial decree. 22 Despite all these measures, it is clear that not all targeted foodstuffs comply with stable conditions. What's more Benin still suffers from significant micronutrient deficiencies, which today constitute a public health problem. The 5th Demographic and Health Survey revealed that the prevalence of anemia in children aged 06 to 59 months was 72%, including 3% in its severe form and 41% in its moderate form in 2017 to 2018. This prevalence shows a slight decrease compared with 78% in 2006. 23 In addition, more than half of women of childbearing age are anemic (58%), and anemia has sometimes irreversible consequences on the child's intrauterine development and the mother's state of health. Diets are often poorly varied and fail to cover essential nutritional requirements, in terms of both macronutrients and micronutrients. 23 This situation raises a number of questions. The aim of this study is to establish a better understanding of the barriers and facilitators to the implementation of the National Strategy for IYCF and the national food fortification system in Benin.
Methodology
We used qualitative methods to identify the barriers and facilitators to the implementation of the National Strategy for IYCF and the food fortification system in Benin. This study has been reviewed and approved by the Local Ethics Committee for Biomedical Research of the University of Parakou, Benin (Reference number: 0432/CLERB-UP/P/SP/R/SA).
Sampling of Participants
The key Stakeholders involved in implementing these 2 selected policies were identified using a 2-stage purposive sampling technique. The first stage involved researching participants through publicly available secondary data sources (including government websites, scientific publications, NGO publications, and the internet) or through previous projects that had involved contact with policymakers, NGOs, other international organizations or academia. The second stage involved snowball sampling to identify additional relevant participants. This 2-stage sampling was designed to ensure a diversity of representatives within and between the sectors concerned, and sufficient insight into the implementation process of each policy. The selection of participants was carried out in conjunction with the policy. Participants were sought from the Ministry of Agriculture, Livestock and Fisheries, the Ministry of Industry and Trade, the Ministry of Health, the Ministry of Social Affairs and Microfinance, local and international NGOs, and consumer rights organizations. The stakeholders to be interviewed had to have experience in the context of policy development or implementation, or to have played a role in the policy cycle process in the country.
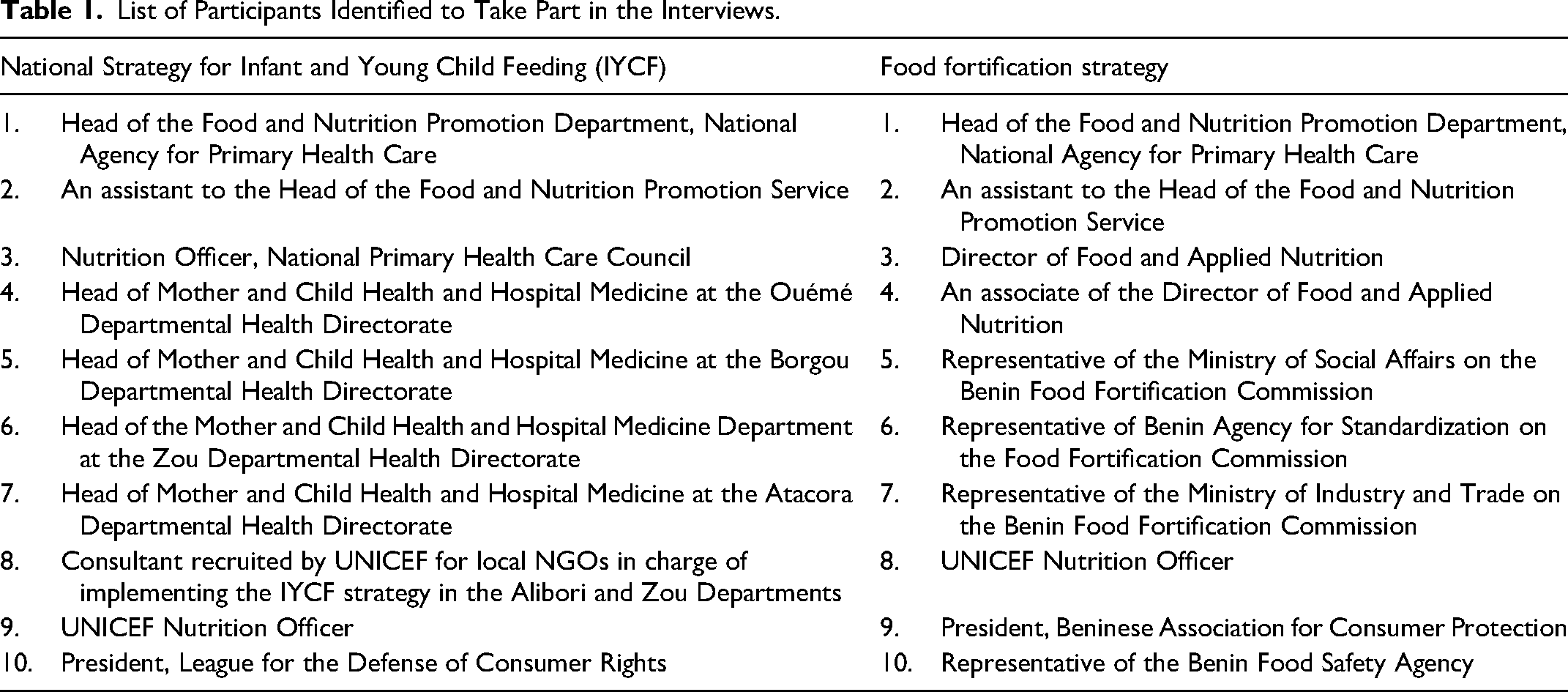
The final number of participants in this study was based on data saturation (the point at which no new themes or information emerge and data begin to become redundant). However, 10 participants were initially recruited into this study for each policy. They were sent a formal letter of invitation, written informed consent, and a general presentation of the project. Table 1 presents the list of the stakeholders who were identified. Stakeholders who agreed to participate were invited to confirm their participation by email. In the absence of any response from stakeholders, a reminder email was sent.
List of Participants Identified to Take Part in the Interviews.
Data Collection
Data was collected through in-depth individual interviews with key national and local Stakeholders involved in implementing the policies identified. Participants were asked to give their views and reflect on their experience of the process of implementing the 2 policies. They were asked to focus on the factors that might have hindered or facilitated the effective implementation of each policy.
An interview guide containing key themes across multiple contexts and levels of influence was initially developed, based on a literature review of similar interviews in different contexts and countries.15–20 On the basis of this literature review, the interview themes in this study were grouped into 3 categories:
− individual characteristics of policy implementers (eg, individual needs, motivation, values and goals, knowledge, skills, and abilities); − the internal characteristics of implementation bodies (eg, executive leadership, the organization's ability to recognize, assimilate and apply knowledge, dedicated resources, organizational culture, and external collaboration); and − environmental influences (social norms, community involvement, social networks and consumer support/advocacy, politics, governance, external policies, interorganizational networks, communication, and economic context).
Written informed consent was obtained from all participants before the start of each interview. Each interview was conducted in French and recorded by the researchers.
Data Analysis
Each interview was transcribed exhaustively into Microsoft Word® from the audio recordings and analyzed by the researchers using a deductive and iterative process based on the study objective. The aim was to systematically compare individual responses in order to identify emerging themes across all interviewees. Emerging themes were examined and interpreted in the light of participants’ views on facilitators and barriers to the policy implementation process, and suggestions for improving policies in the future. Quotes from the interview transcripts are presented as examples for the themes.
Results
Twenty (20) stakeholders, including 10 for each policy, were initially identified for the interviews. As the final number of participants in this study was based on data saturation, 2 new stakeholders were recruited for IYCF and 1 new actor for food fortification. A total of 23 interviews were conducted and transcribed. The key themes that emerged from the analysis of the interviews were classified into the 3 predefined categories of: individual characteristics of policy implementers, internal characteristics of implementing bodies, and environmental influences. Table 2 presents the contributions of the interview participants from a stakeholder.
Participants’ Contributions to the Stakeholder Viewpoint Interviews.
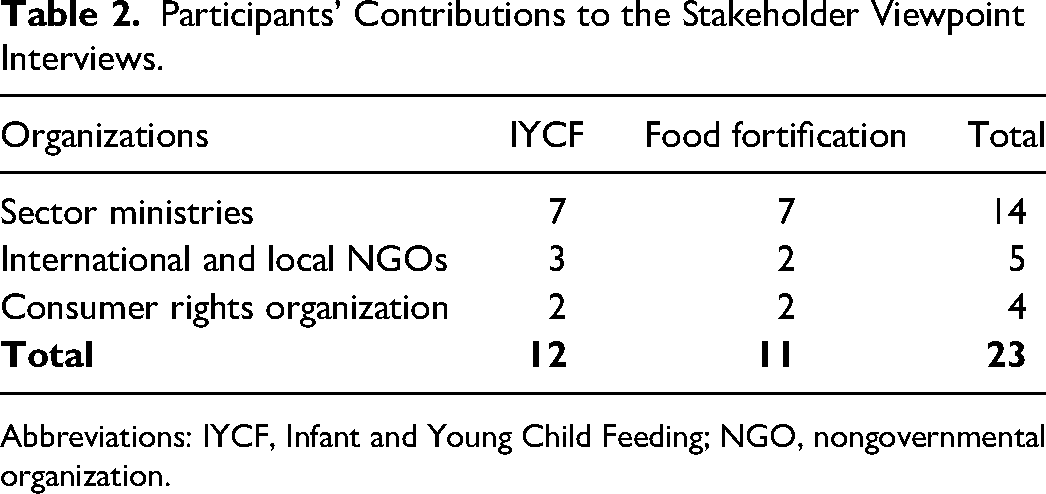
Abbreviations: IYCF, Infant and Young Child Feeding; NGO, nongovernmental organization.
Potential Barriers to Policy Implementation
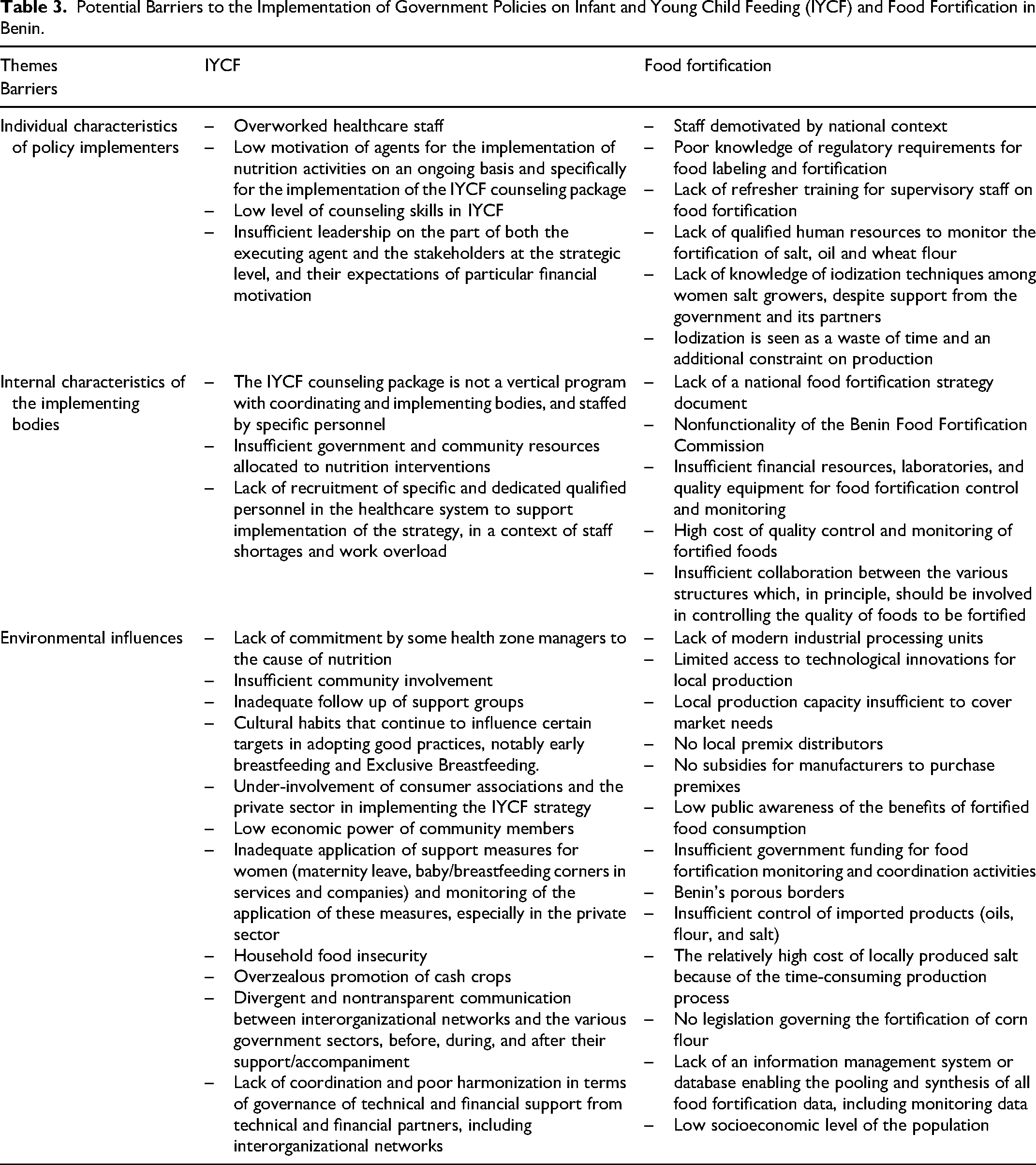
The key themes emerging from the analysis of stakeholder interview data as potential barriers to the policy implementation process are presented in Table 3. Those most frequently mentioned by stakeholders are described as follows:
− − − − −
Potential Barriers to the Implementation of Government Policies on Infant and Young Child Feeding (IYCF) and Food Fortification in Benin.
A representative of a health NGO stated: “The lack of control at all levels of the food chain is worrying. For example, it is common to find oils not fortified with vitamin A on the market, which means that efforts to improve nutrition are not reaching the whole population.”
A food safety inspector from the Ministry of Agriculture also asserted:
“Attempts at corruption are unfortunately common in our work. This hampers our ability to detect and report irregularities, and creates an environment where fortification standards are not consistently met.”
There is also a lack of quality laboratories and equipment for controlling and monitoring food fortification. Several players noted this. By way of example, they made the following statements:
“Even when the will to respect fortification standards exists, the lack of appropriate equipment in laboratories prevents rigorous controls from being carried out. This shortcoming slows down efforts to eradicate micronutrient deficiencies.”
“The lack of adequately equipped laboratories complicates our control work. Often, we don't have the necessary tools to carry out accurate analyses of food fortification, which undermines the effectiveness of regulatory measures.”
“The lack of quality equipment in laboratories makes it difficult to monitor product conformity. Without the right devices, it's almost impossible to guarantee that food is properly fortified.”
Potential Facilitators for Policy Implementation
Table 4 shows the potential facilitators for the implementation of government policies on IYCF and food fortification in Benin. The most frequently cited are:
− − − −
Potential Facilitators for the Implementation of Government Policies on Infant and Young Child Feeding (IYCF) and Food Fortification in Benin.
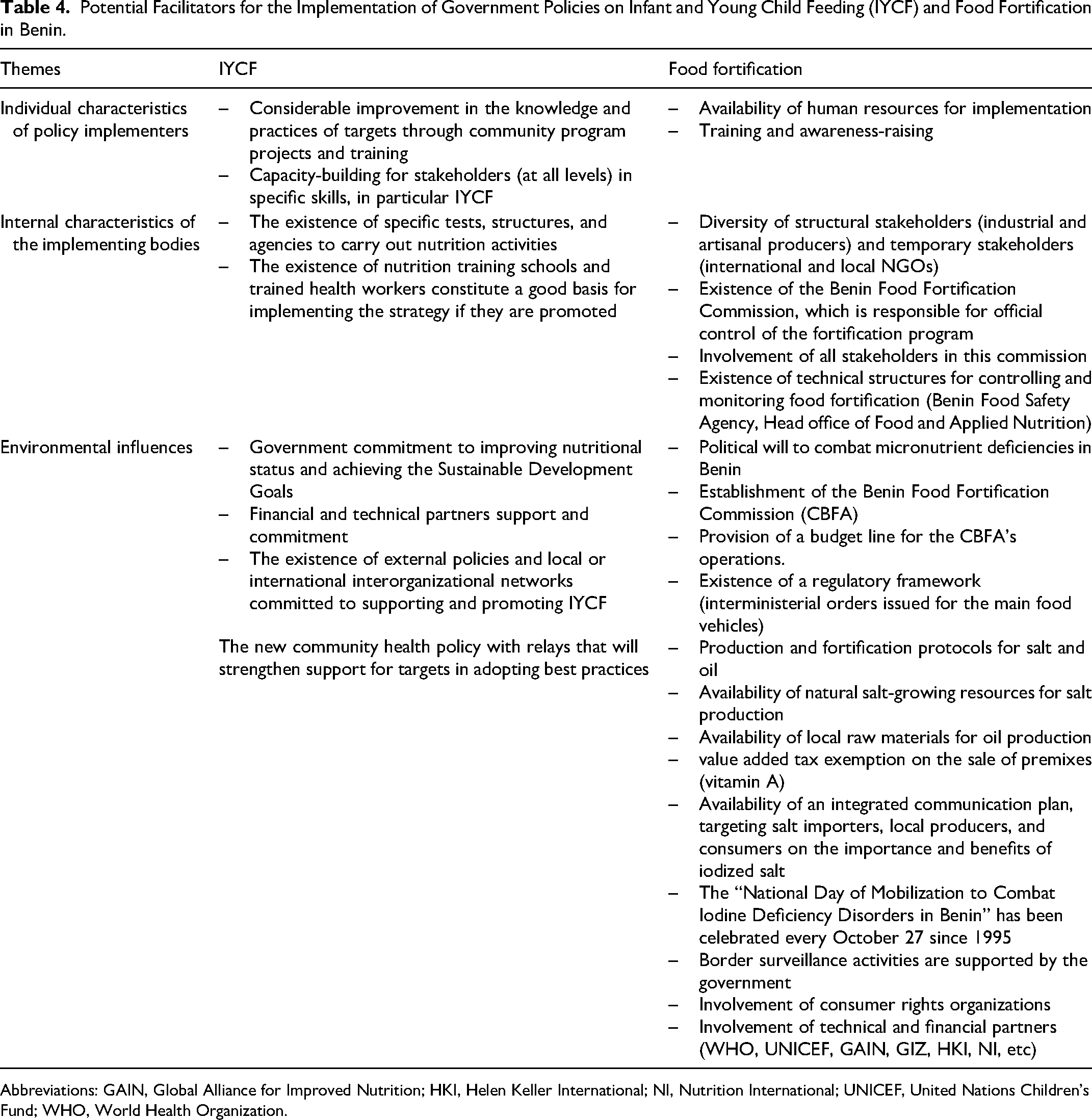
Abbreviations: GAIN, Global Alliance for Improved Nutrition; HKI, Helen Keller International; NI, Nutrition International; UNICEF, United Nations Children's Fund; WHO, World Health Organization.
Some Solutions to Improve Implementation of Government Policies on Infant and Young Child Feeding and Food Fortification in Benin
A number of proposals were put forward by the various stakeholders met to improve the implementation of government policies on IYCF and food fortification in Benin. These include
IYCF
Update the strategy to take account of new global recommendations and new health sector reforms in Benin; Redefine monitoring indicators and integrate them into the DHIS2 database for routine monitoring. The need for a higher level of commitment from the state in terms of budget and coordination of actions; Recruit specific nutrition staff to support implementation of the strategy at health zone offices, communal health centers and arrondissements; Integrate modules on IYCF into health worker training curricula; Train the community relays who ensure the implementation of the community health policy on the IYCF strategy; Create a favorable professional environment for the implementation of the strategy for civil servants, especially in the private sector; Address and deconstruct the social and cultural constructs that influence the adoption of good IYCF practices; Develop agricultural policies and support the development of income-generating activities to increase food security and household economic conditions; Comply with the periodic (annual) evaluation of the strengths and weaknesses of policies and programs for the protection, promotion and support of optimal IYCF practices, based on the use of the World Breasfeeding Trends Initiative (WBTi) tool; and Ensure that the recommendations of the WBTi assessment are implemented at all levels, and translated into specific action plans for each level (Central/Strategic, Operational focused on service supply, and Community/Household/Family focused on demand promotion).
Carry out an in-depth diagnosis of the food fortification system in order to identify weaknesses and subsequent corrective actions; Draw up a strategy document on food fortification in Benin, supported by guidelines focusing on the necessary interventions; Identify new food resources that can be fortified; List food factories and production sectors; Revitalize the Benin Food Fortification Commission; and The government should equip inspectors with sampling and analysis tools to enable monitoring and control checks at all points along the iodized salt distribution channel.
Discussion
The results of this study on the barriers and facilitators to the implementation of IYCF and food fortification policies in Benin reveal a series of challenges as well as opportunities for improving these policies.
Barriers to Policy Implementation
The study highlights the low motivation of staff due to the abolition of bonuses and insufficient recognition of their work. This situation is not unique to Benin. For example, a study carried out in Ethiopia by Ejigu et al 24 also showed that demotivated health workers, due to insufficient financial incentives and lack of recognition, constitute a major barrier to the implementation of health programs. Similarly, a study conducted in Rwanda by Ivang et al 25 revealed that health worker motivation is essential for the performance of maternal and neonatal health services, and that nonfinancial incentives, such as recognition and professional development opportunities, can play a crucial role. Karaferis et al, 26 have also identified health staff motivation as a critical factor in the success of child nutrition programs. Recognizing and valuing the work of staff are essential to improving their commitment and performance.
The limited funding of IYCF and food fortification programs is proving to be a significant barrier in Benin. This situation is similar to that observed by Pernechele et al 27 in other African countries, where nutrition programs rely heavily on support from international partners, but this support is often insufficient to guarantee the sustainability of initiatives. Yet Black et al 28 have emphasized that sustainable funding is necessary for effective nutrition interventions.
Inadequate training of health personnel and limited community awareness are major barriers. These findings are similar to those of Bhutta et al, 29 who highlighted the importance of ongoing training and awareness-raising to improve nutritional practices. A study in Bangladesh by Roy et al 30 also showed that training health workers and raising community awareness are essential for the effective implementation of IYCF programs. Watson et al 31 through a systematic review of the literature on interventions to improve maternal and child nutrition in sub-Saharan Africa found that behavior change theory, communication, or counseling led to significant improvements in infant stunting and wasting, household food intake, and maternal psychosocial measures. They therefore recommend incorporating behavior change functions into nutrition interventions to improve outcomes for mother and child.
Traditional eating habits and cultural resistance represent major challenges to the implementation of IYCF and food fortification programs. Indeed, traditional eating habits are often based on beliefs and practices handed down from generation to generation, such as a preference for certain types of food or preparation methods, which may not include fortified foods or IYCF practices. Cultural resistance, on the other hand, takes the form of reluctance to change established practices, often perceived as identity values. These barriers hinder the adoption of fortification and IYCF programs by reducing the acceptability of fortified products and new nutritional practices. A study carried out in Ethiopia by Endris et al 32 showed that traditional dietary practices and cultural resistance can hinder the adoption of new nutritional interventions. Awareness-raising and educational efforts need to be stepped up to overcome these resistances. Also, the use of influential people and family members in maternal, infant, and young child nutrition activities in communities helps to get the message across and deconstruct certain traditional ideas and eating habits, thus improving the nutritional status of mothers and children.33,34
The complexity of monitoring food fortification regulatory standards is another major barrier. Corrupt attempts and lack of material resources aggravate the situation. These findings are in line with those of Luthringer et al, 35 who identified weak monitoring systems as a significant challenge to the implementation of food fortification programs. A study carried out in Ghana by Abizari et al 36 also highlighted the importance of a robust surveillance system to ensure the success of fortification programs.
Potential Facilitators of Policy Implementation
Strong political commitment is a key facilitator. The Beninese government is showing a willingness to make IYCF and food fortification a national priority. Several studies have shown that political commitment is essential for the success of health and nutrition programs. Indeed, political commitment makes it possible to mobilize the necessary resources and create a favorable environment for policy implementation. These studies show that governments must make a long-term commitment, and that their efforts to strengthen the health system must be sustainable and ongoing.37,38 Political commitment contributes to the sustainability of nutrition programs by integrating them into national development plans and guaranteeing specific budgets for their implementation. 39 A report by the WHO points out that countries with strong political commitment, such as Uganda, have succeeded in improving nutrition thanks to politically well-supported programs. The WHO-supported “Accelerating Nutrition Improvements” (ANI) program in Uganda, showed positive results due to the government's commitment to integrating nutrition into healthcare and actively monitoring progress. 40
In addition, partnerships with international organizations provide crucial support in terms of funding and implementation, particularly in contexts where national resources are limited. These organizations support the training of health workers and facilitate community awareness-raising. They help fill financial and technical gaps, and build local capacity. This was the case for the WHO-supported ANIANI program in Uganda. Several studies have shown that international partnerships play a key role in strengthening local capacities and improving nutritional interventions. Similarly, these studies underline the importance of partnerships for the sustainability and success of nutrition programs. 41
Ongoing training of health workers and community awareness-raising are essential to the success of nutrition programs. 42 Adequate training ensures that health workers have the necessary skills to effectively implement nutrition policies, while community awareness helps improve the adoption of recommended nutritional practices. 43
In addition, collaboration between different ministries and the involvement of stakeholders at all levels facilitate policy implementation. The “health in all policies” (HiAP) approach has been widely advocated as a means of involving multiple government sectors in the fight against health inequalities. 44 Several studies have shown that cross-sector collaboration and stakeholder engagement are crucial to the success of health and nutrition programs.45,46 Studies also emphasize that the involvement of all stakeholders, including local communities, is essential for the success of nutrition interventions. 47 The national IYCF strategy, supported by partnerships with organizations such as UNICEF, has trained many health workers and raised community awareness of the importance of IYCF. Community support programs have been set up, strengthening families’ ability to adopt optimal nutritional practices. Also, thanks to strong political commitment and support from international NGOs, Benin has set up programs to fortify salt with iodine and oil with vitamin A. These initiatives have been supported by training for producers and awareness campaigns for consumers, leading to a significant improvement in food fortification coverage rates.
Study Limitations
As with all research, this study has certain potential limitations. The participants in this study were identified on the basis of their expertise, and we cannot claim that the sample was representative of all the actors involved in or affected by the IYCF and food fortification policies in Benin. It is therefore not possible to make broad generalizations about the views of those interviewed. However, the in-depth nature of the interviews provides key information on the concerns of the actors involved in these policies. Also, the data saturation point could be judged subjective and vary depending on the researcher, which could have influenced the final sample size and depth of data collected. The results of qualitative studies are often contextual and specific to the participants and situations studied. They may not be generalizable to other contexts or populations. Despite these limitations, this study remains a valuable contribution to understanding the obstacles and facilitators to the implementation of IYCF and food fortification policies in Benin.
Conclusion
Analysis of the results reveals that the barriers to implementing IYCF and food fortification policies in Benin are multiple and interconnected, including human, financial, cultural, and structural factors. However, the presence of facilitators such as strong political commitment, effective partnerships, ongoing training and awareness-raising, and cross-sector collaboration shows that there is considerable potential to overcome these barriers. An integrated approach, reinforced by adequate resources and ongoing commitment, is essential to ensure the success of nutrition policies in Benin.
Footnotes
Acknowledgments
The implementation of this research project in Benin is the fruit of collaboration between the Regional Public Health Institute Comlan Alfred Quenum (IRSP-CAQ), the National Council for Food and Nutrition (CAN), various government ministries and local and international NGOs. Many thanks to all those who took part in the interviews.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.