
Abstract
Background:
Poor nutrition during childhood impedes physical and mental development of children, which propagate the vicious cycle of intergenerational under nutrition. This paper is aimed at understanding the determinants of stunting among children aged 0 to 59 months in Bangladesh.
Methods:
The study used Bangladesh Demographic and Health Survey 2011 data and a multistage stratified cluster-sampling design. Anthropometric data (for height and weight) were collected and analysis was limited to 7647 children. Multiple binary logistic regression analysis was performed to assess the association of stunting with potential socioeconomic and demographic factors.
Results:
The prevalence of stunting has been found to be about 41% among children aged less than 60 months and higher in rural setting than in urban areas (43% vs 36%). Adjusted model revealed that several factors were influencing stunting. The children living in moderately food-insecure households had higher odds of becoming stunted (odds ratio [OR] = 1.27, 95% confidence interval [CI]: 1.05-1.54, P = .01) compared to the children living in food-secure households. The derived ORs of stunting for children delivered at institutions facilitated particularly by public (OR = 0.80, 95% CI: 0.67-0.96; P = .02) or private (OR = 0.81, 95% CI: 0.67-0.97; P = .02) sectors were less than for children delivered at home. Similarly, wealth index, exposure of mother to the mass media, age of child, size of child at birth, and parents’ education were significantly associated with stunting.
Conclusions:
Moreover, the demographic characteristics and other indicators appeared to have significant influence in the prevalence of stunting. Public health programs are needed to avert the risk factors of stunting among children in Bangladesh.
Introduction
Globally, an estimated 165 million children aged below 5 years had stunting or chronic under nutrition in 2011, among whom, 36% were residing in African countries and 27% in Asian countries. 1 The prevalence of stunting in South Asia has been found to be 39%, which is a concerning issue for public health. 2 In Bangladesh (a South Asian country), approximately 41% of children were reported to be stunted in 2011, 3 and in 2004, the figure was higher (51%). 4 This decline occurred due to initiatives and interventions that were implemented by the Government and other public health organizations. Although the country has been reducing the prevalence of stunting with annual average reduction rate of 1.3% during 2004 to 2011, the progress is still quite low compared to the global rate of 2.1% decline during 1990 to 2011. 5 According to the World Health Organization’s (WHO) threshold, 15% refers to an emergency situation; this current prevalence of stunting indicates an alarming situation of chronic undernutrition in Bangladesh. 6 In general, lower mental capacity, low school performance, and reduced level of future productivity are consequences of this form of childhood undernutrition, which is linked with poverty and poor access to health services. 7 It also increases the risk of children’s death, inhibits cognitive development, and affects health status in their future years. Therefore, childhood undernutrition not only impedes the physical and mental development of children but also contributes to hindering the socioeconomic development of a country. 8,9
The underlying causes of undernutrition during childhood are multifactorial, such as poor maternal health and nutrition, lower maternal education, inadequate infant and young child feeding (IYCF) practices, low birth weight and size at birth, and short birth intervals. 10,11 However, these factors relating to food, health, and care differ from country to country, and understanding these differences is critical in delivering appropriate, effective, and sustainable solutions. 8 Previous studies in Bangladesh show that different sociodemographic, health, and feeding-related factors are the common determinants of stunting. 10 –12 Reduction of undernutrition among below five children, particularly stunting and wasting, has received emerging attention by the development partners and has been included in the Sustainable Development Goals (SGD 2: target 2.2). 13 The rate of below five stunting is decreasing steadily in Bangladesh but is still at 41% which exceeds the cutoff for very high prevalence and is of public health significance. 3,14 A study conducted in Dhaka city illustrates that the height of mothers, birth weight of children, education level of fathers, knowledge of mothers on nutrition, and frequency of feeding have been identified as significant factors that have independent and direct influences on the stunting of preschool children. 12 However, the findings from the study were not representative of the whole Bangladesh since this was carried out only in Dhaka city of Bangladesh. Several other studies conducted in Bangladesh aimed to illustrate the relationship between some identified determinates, such as socioeconomic status and household wealth, and stunting among children. 11,12,15 Moreover, previous studies conducted in Bangladesh have identified several factors as determinants of severe and moderate stunting among below five children in Bangladesh. 10 There is a scarcity of recent literature determining the underlying factors of stunting.
Prevalence of stunting and its associated factors have also already been demonstrated in other country contexts, such as in Ethiopia, China, and Indonesia. 16 –19 In addition, these studies were carried out using different methodologies, such as for data collection, analysis, and type and selection of study sites and participants. These studies were based on primary data sources, and most of these were conducted with small sample size. Our study used large data sets as well as large sample sizes that represent the whole country. To our knowledge, this is the first study in Bangladesh that used recent data from Bangladesh Demographic and Health Survey (BDHS) 2011 to identify the most crucial factors of stunting among below five children. Findings from this study may help public health researchers, stakeholders, and policymakers to understand the current situation of stunting and its potential risk factors based on the current scenario, which may help in taking required steps and initiating interventions to improve the condition of chronic undernutrition among children aged 0 to 59 months in Bangladesh.
Materials and Methods
Data for this study came from the nationally representative BDHS 2011. This survey was conducted by the National Institute of Population Research and Training under the authority of the Ministry of Health and Family Welfare, in collaboration with The United States Agency for International Development (USAID). The BDHS report is publicly available and may be accessed upon request (http://dhsprogram.com/data/available-datasets.cfm).
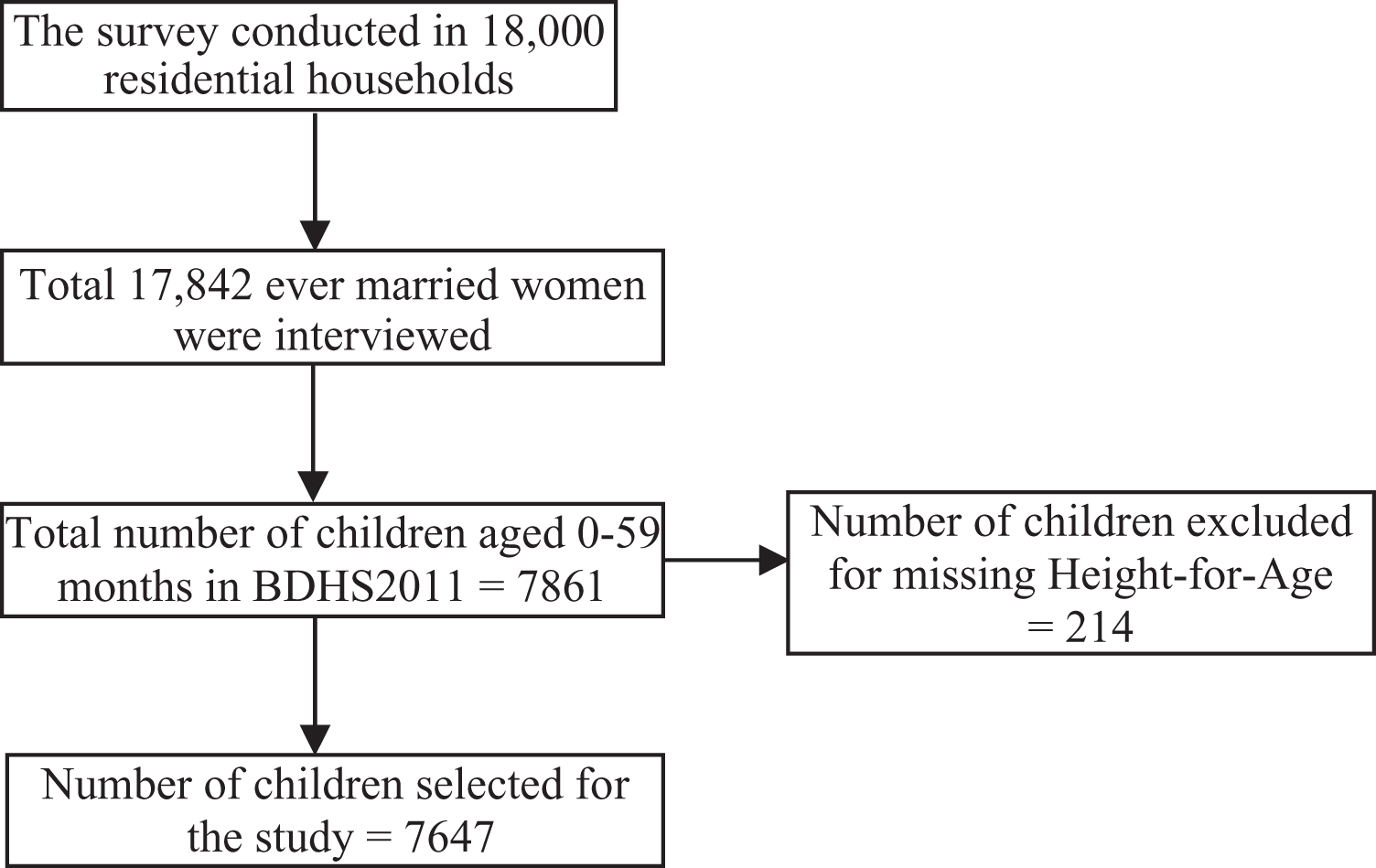
The BDHS 2011 is nationally representative and covers the entire population, using the sampling frame prepared for the 2011 population and housing census, provided by the Bangladesh Bureau of Statistics. The primary sampling unit for the survey is an enumeration area (EA) that was created to have an average of about 120 households. The survey is based on a 2-stage stratified sample of households. In the first stage, 600 EAs were selected with probability proportional to the EA size, with 207 clusters in urban areas and 393 clusters in rural areas. A complete household listing operation was then carried out in all selected EAs to provide a sampling frame for the second stage of selection of households. In the second stage, a systematic sample of 30 households per EA was selected, on average, to provide statistically reliable estimates of key demographic and health variables for the country as a whole, for urban and rural areas separately, and for each of the 7 administrative divisions. The survey was conducted in 18 000 residential households with 6210 and 11 790 in urban and rural areas, respectively. A total of 18 222 ever married women were identified in these households, and 17 842 were interviewed with a response rate of 98% (Figure 1). Interviews were conducted in the same dwelling place of the respondents. Among those households, the survey identified a total of 7861 children aged 0 to 59 months (Figure 1). For this analysis, we first extracted the children’s data set from the BDHS 2011 original file; then, we excluded 214 children whose height-for-age z score (HAZ) values were implausible (−6 > HAZ > 6) or missing, and finally, our final sample size for this analysis was 7647 children (Figure 1). The survey involved well-trained data collectors for conducting interviews with the caregivers of children aged 0 to 59 months and for collecting anthropometric data (for height and weight) using standardized procedures. 20
Sampling and participants enrollment.
Chronic undernutrition status of children aged 0 to 59 months has been assessed by HAZ. According to the definition of WHO, HAZ explains the height of a child in terms of the number of standard deviations (SD) above or below the median height of healthy children in the same age group. 21 A child was classified as stunted (dependent variable) if he/she had a z score below −2 SD.
Previous studies have shown that different risk factors (independent variables) were associated with stunting in Bangladesh. 9 –11 Based on those studies, we classified the potential risk factors into different groups (such as parental, child, household, and community factors). Mothers’ and fathers’ education (no education, primary, secondary, or higher), fathers’ occupation (unemployed, farm worker, day laborer, semi-skilled worker, and service holder/businessman), mothers’ exposure (yes, no) to the mass media (radio, television, newspapers, and magazines), and birth place of the child (home, public sector facility, private sector facility, and Non-governmental organization [NGO] facility) were included in the parental factors; age of child (0-11, 12-23, 24-35, 36-47, and 48-59 months) and the size of child at birth (average or larger, very small, and small) were considered the child-level factors. Household-level factors included household food insecurity (secure, mildly insecure, moderately insecure, and severely insecure), wealth index (richest, richer, middle, poor (poorer and poorest), and types of toilet facilities (improved, non-improved); the community-level factor included the place of residence (urban, rural).
Statistical Analysis
A description about the sampled participants was revealed using univariate analysis and reported in terms of percentages, along with respective 95% confidence interval (CI). Bivariate analysis was done to see the differentials in the prevalence of stunting over geographical characteristics (administrative division and place of residence). As our dependent variable is dichotomous in nature (stunted or not stunted), we fitted simple and multiple binary logistic regression analysis to see the association of the independent variables with dependent variable (stunting status of children). To explore the factors that influenced stunting, we built multiple regression model adjusted with variables having significant association with dependent variable in simple logistic regression model only to best fit the regression model and predict the outcome variable. A P value less than .05 has been considered for statistical significance. Variations in the errors due to complex survey design were controlled during analysis. The results of logistic regression analyses have been presented in terms of odds ratio (OR), 95% CI, and P value. Data of this study were analyzed using R (version 3.1.0) and STATA (version 12.0).
Ethical Approval
The institutional review board of the Bangladesh Medical Research Council approved the BDHS 2011. Informed consent was obtained from each respondent in the survey before interviewing, and again, separately before taking weight and height measurements. 3 The DHS Program also removed all personal information of the respondents in the database prior to making these available online.
Results
Among the study children, almost 42% were living in poor (poorer 21%, poorest 21%) households, and about 51% of households had non-improved toilet facilities. About 64% fell in the category of food-secure households and 26% in mildly food-insecure households. About 75% of the children were delivered at home, and the size at birth was average or larger for 83% of the children. Large proportions of the parents (20% mothers and 30% fathers) had no formal education (Table 1). The prevalence of stunting in below five children was higher in the rural regions (43%) compared to the urban regions (36%). Administrative division–wise distribution of prevalence shows that Sylhet was a high-risk area for stunting, where the prevalence was about 50%, and Khulna and Rajshahi division were the low-risk areas for stunting (Figure 2).
Percentage Distribution of Background Characteristics of the Study Participants (Weighted).
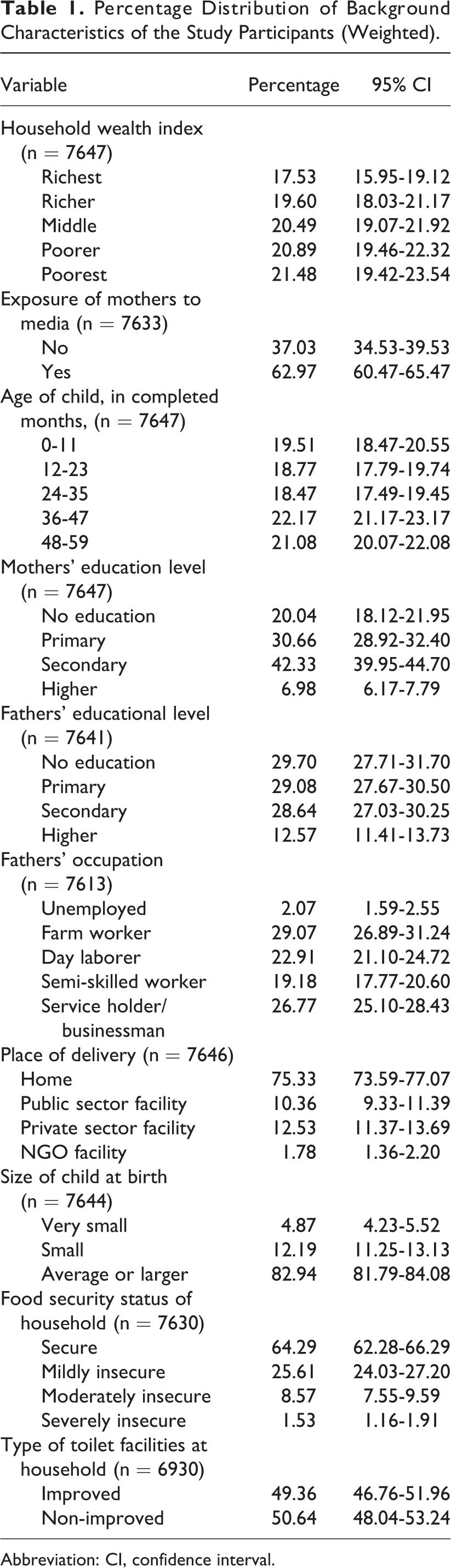
Abbreviation: CI, confidence interval.
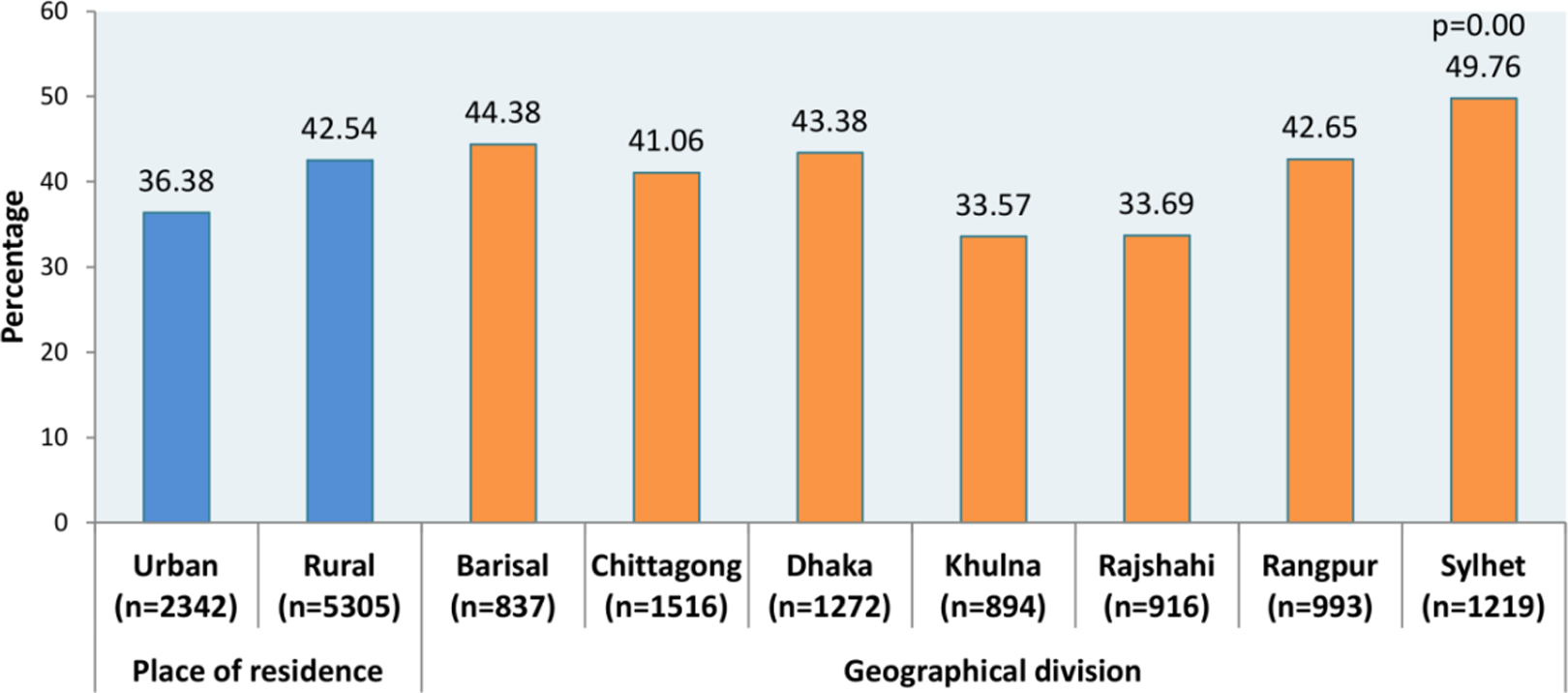
Distribution of stunting across place of residence and geographical divisions.
Table 2 shows the ORs derived from simple and multiple logistic regression analysis for assessing the association between stunting status of children aged 0 to 59 months and sociodemographic characteristics of their households. Results from multiple logistic regression analysis are described here. Child’s age in months was statistically associated with stunting; children aged 12 to 23 months were more likely to be stunted (OR = 3.98, 95% CI: 3.32-4.76; P = .00) than those aged 0 to 11 months. Children living in the poorest households were 2.17 times more likely to be stunted (OR = 2.17, 95% CI: 1.70-2.76; P = .00), and those who lived in poorer households were 1.79 times more likely to be stunted (OR = 1.79, 95% CI: 1.43-2.23; P = .00) compared to those born in the richest households. Exposure of mothers to the mass media seemed to play an important role in the stunting status of children as children of mothers with no media exposure were 1.20 times more likely to be stunted (OR = 1.20, 95% CI: 1.06-1.36; P = .00) compared to children of mothers exposed to the media.
Odds Ratios in Simple and Multiple Logistic Regressions Assessing the Impacts of Selected Variables on Stunting of Children below five in Bangladesh.
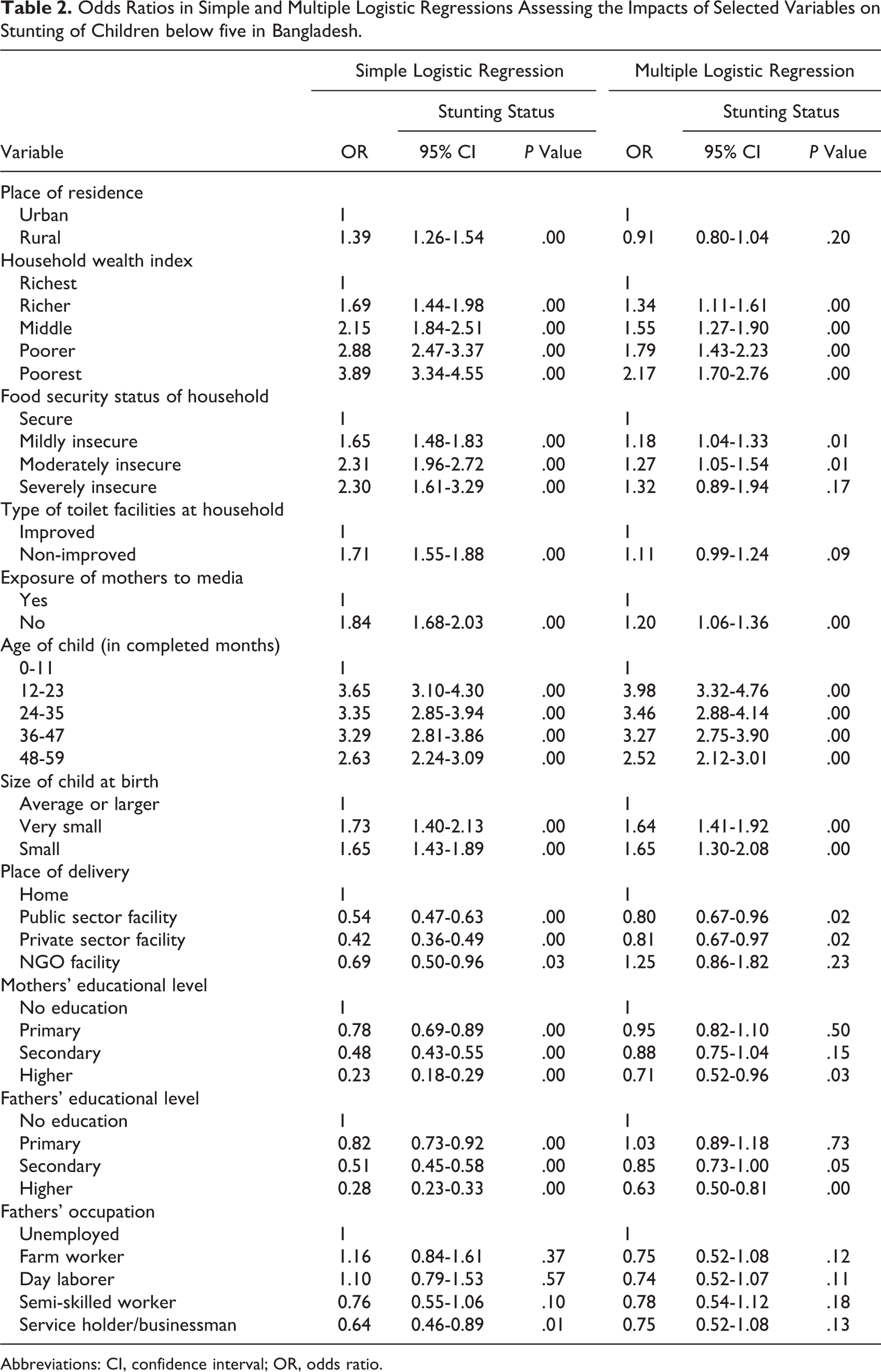
Abbreviations: CI, confidence interval; OR, odds ratio.
The result indicates that children whose parents’ attained secondary educations were less likely to be stunted compared to those whose parents had no formal education. Children who were perceived by their mothers to be small in size (OR = 1.65, 95% CI: 1.30-2.08; P = .00) and those who were perceived to be very small (OR = 1.64, 95% CI: 1.41-1.92; P = .00) at the time of delivery were significantly more likely to be stunted than children who were perceived to be average or larger at the time of delivery (Table 2). Place of delivery and stunting status of children have a significant association as children who were born at health facilities (such as public or private hospital/clinic) were less likely to be stunted compared to children born at home. Our result reveals that households that reported mild and moderate food insecurity were 1.18 (OR = 1.18, 95% CI: 1.04-1.33; P = .01) and 1.27 (OR = 1.27, 95% CI: 1.05-1.54; P = .01), respectively, times more likely to have stunted children than those that reported being food secure (Table 2).
Discussion
Stunting still remains a major public health problem in Bangladesh as in other developing countries. Despite having several interventions in place, the prevalence of stunting in Bangladesh among below five children is 41%. 3 The findings of this study reveal that household wealth, mothers’ exposure to mass media, age of the child, size of the child at birth, place of delivery, parents’ education, food security status of the household, place of residence, and type of toilet facilities are the factors associated with stunting among below five children in Bangladesh. In our analysis, the factors that have been identified to be significantly associated with stunting are household wealth, food insecurity, mass media exposure, age of the child, size of the child at birth, and place of delivery. Our analysis also reveals that, sometimes, these factors are also interrelated. Mass media exposure, age of the child, size of child at birth, and place of delivery are directly dependent on household wealth index as well as on parental education.
Our study indicates that household wealth is significantly associated with stunting. Children from the poorest households are more likely to be stunted than those from middle, richer, and richest households. These children may become stunted due to their mothers’ lower educational status and lack of sources of knowledge on child nutrition. Moreover, a study in Bangladesh illustrates that the mothers who have more knowledge about child health and nutrition are educated and come from richer households; they also have greater access to media compared to mothers from poorer households. 3 Financial ability of a household is also important for ensuring that the child gets the required amount of nutritious foods. A study in Bangladesh found that mothers from poor households did not have the financial ability to purchase nutritious foods for their children. 22 A study in Nepal revealed that richer households have more financial ability or access to nutritious foods and are more capable of ensuring proper care for the children residing in those households. 7 On the contrary, the children from richer households may also be affected by stunting. The World Bank report suggests that in the richer households stunting may also arise due to inadequate knowledge on food, feeding practices, inappropriate food allocation, and poor hygiene practices. 23 Lack of maternal education, lack of maternal knowledge about child nutrition, and lack of financial ability to purchase appropriate foods are the factors associated with stunting.
One study in Northeastern Peninsular Malaysia showed that food insecurity was associated with stunting and underweight. 24 Another study from Kenya found that stunting was highest among severely food-insecure households ranked in the poorest tertile and lowest among food-secure households in the middle wealth tertile. 25 Similarly, our study found that mildly and moderately food-insecure households were more likely to have stunted children than those reported as being food secure. Similar findings were also obtained from other studies in Bangladesh, Ethiopia, Vietnam, and Colombia. 26,27 In Bangladesh, approximately 25% of the population is food insecure. 28 Approximately 31% of the rural population in Bangladesh suffers from “chronic poverty,” which is characterized by low consumption, lack of access to basic health services, and undernutrition. 29 Another study also illustrated that, in Bangladesh, household food security is significantly associated with child feeding practices. 30
Exposure to mass media is important as sources of knowledge. The mass media provides information that is essential to amplifying people’s knowledge and awareness regarding issues in their day-to-day life. Our study illustrates that the children of mothers who did not listen to the radio, did not watch television, and did not read newspapers or magazines at least once a week had higher risk of becoming stunted compared to the children of those mothers who were exposed to any type of mass media. Moreover, the BDHS 2011 data suggest that almost 49% of women have no access to mass media, and less than 1% women were found to have all the media sources. 3 Mass media advertisements provide information on health, nutrition, proper hygiene practices, proper child feeding practices, and on overall knowledge about health, which may contribute to reduction of the prevalence of stunting among below five children. It is well proven in Bangladesh that mothers who have less access to mass media are less likely to be exposed to appropriate messages and campaigns on heath and vaccines provided by the NGOs or government organizations compared to those who have more access to the mass media. 3 A study conducted among children below the age of 2 years in Bangladesh revealed that mothers of undernourished children were less educated and had less access to the mass media, 31 which indicates that mothers’ education and exposure to the mass media is an important factor for their children’s health and well-being.
Our study revealed that the likelihood of stunting was higher among children who had smaller-than-average size at birth. One study illustrated that stunting passes from one generation to another in an intergenerational cycle; this indicates that the children born to stunted mothers are likely to be stunted themselves. 23 Considering such a reality, size of children at birth plays an important role in the prevalence of stunting. Besides, studies in Nepal, Bangladesh, and Ethiopia have also stated that children born with smaller than average size were more prone to stunting. 7,10,32 Moreover, in Bangladesh, size of child at birth is positively associated with the level of maternal education. A study showed that, in Bangladesh, educated mothers tend to give birth to average or large-sized children; on the other hand, smaller children are born to the mothers who have no education at all. 3 Furthermore, the size of child at birth may also depend on multidimensional factors, including maternal nutrition status, antenatal checkup, and food intake during pregnancy, intrauterine growth, size for gestational age, timely delivery, maternal sociodemographic status, and household economic status. 10 These need to be considered in the prevention of stunting.
Our study indicated that children aged 12 to 23 months are mostly at risk of stunting compared to children aged 0 to 11 months and 24 to 59 months. Appropriate complementary feeding practices are essential for mental and physical development of children of these age groups. Studies conducted in rural Bangladesh and in India among children below 2 years of age suggest that the lack of knowledge about time of initiation of complementary feeding, dietary diversity, and nutritional knowledge increases the risk factors of stunting. 31,33 Other studies conducted in rural Uganda, Vietnam, and Ethiopia also reported that mothers and caregivers who have little knowledge or inadequate knowledge about IYCF practice 34 –36 ultimately lead to induce stunting in their children. This means that stunting has a relationship with child feeding practices. So, it can be said that children aged 12 to 23 months are at a risk of stunting because of their inappropriate child feeding practices. Stunting is a cumulative process that can begin in the uterus and continue up to the first 3 years of life. 32 However, after the second year of a child’s life, it seems to steadily reduce again with time. 10,11 The World Bank report illustrates that the lack of care, access to health service, and inappropriate feeding practices also lead to stunting. 23 So, adequate knowledge and appropriate feeding practices are essential for the prevention of stunting.
Place of delivery is found to be another crucial factor for stunting. In Bangladesh, 71% of childbirths still occur in the home while only 29% of births take place in health facilities. 3 Our study indicates that children born in health facilities with the help of health professionals were less likely to be stunted compared to the children born at home with the help of traditional birth attendants (trained or untrained). Similarly, several other studies conducted in Nepal, Bangladesh, and India among below five children also suggest that children born in health facilities were less likely to be stunted compared to children born at home. 7,10,33 There are some factors associated with delivery at health facilities and at home. Studies conducted in Bangladesh and Nepal revealed that educated mothers from richer families go to health facilities for antenatal visits and child delivery. 3,7 Health professionals at hospitals and clinics provide counseling on antenatal care for safe delivery and advise to receive postnatal care. Besides, the counseling is given on IYCF practices to the new mothers helping them to take proper care of their children. However, the assurance of safe delivery and counseling on IYCF practices are not provided in the rural context during home births in Bangladesh. Considering the current situation, below five children are at risk of stunting in Bangladesh.
Knowledge and awareness on child nutrition among parents of below five children are important factors for ensuring adequate and appropriate child feeding practices and child care. In this regard, parental education is important. Our study found that parents’ education was a risk factor for stunting among children aged 6 to 59 months. A study conducted in rural Bangladesh among children below the age of 2 years revealed that educated mothers were more conscious about their children’s health and nutrition, enabling them to take better care, better use of the health services, and also to help ensure better hygiene practice. 31 These findings were also supported by another study conducted in Indonesia. 37 In Bangladesh, mothers and fathers from richer families are more likely to be educated than those from the poorest families. 3 Our analyses derived that there is a negative association between educational status of parents and stunting, which has been observed in all BDHS from 1999 to 2007. 4,38,39 Besides, educated parents might have better income as well as better household access to food, higher proportion of wealth allocated for children’s welfare, and improved standard of living, 10 which would ultimately help to provide better care to the children. So, education is one of the essential needs toward preventing stunting.
One of the limitations of this study is that we depend only on secondary data sources which do not contain detailed information on dietary diversity or dietary practice of the study children. Our study depends on data sources from other studies for clarification or further explanation. This study was unable to present sufficient information on children’s birth weights as well as gestational age from intrauterine growth restriction as a cause for size at birth. Also, these data do not represent the population or the children residing in urban slums, although children of urban slums are more prone to stunting than other children residing in the urban areas. Despite these limitations, the strength of this study is that our results have identified the most vital factors for stunting, which will be important contributions to the available literature on the association of socioeconomic and demographic variables with stunting of below five children.
Our results revealed that stunting is most common among the children aged 12 to 23 months in Bangladesh. The demographic characteristics of the study participants and other indicators, including household socioeconomic status (poorest), place of delivery (home delivery), size at birth (small size), and parents’ education (no formal education) appeared to influence the prevalence of stunting significantly. Several potential educational interventions by the policymakers are needed for developing information that can serve as a platform to prevent stunting among children aged below five years in this country.
Footnotes
Authors’ Note
Jahidur Rahman Khan is currently affiliated with the Center for Bioinformatics Learning Advancement and Systematics Training (cBLAST), University of Dhaka, Bangladesh. This study was conducted by team members of Nutrition Program Evaluation Unit under Nutrition and Clinical Services Division of icddr,b as part of their research activities.
Acknowledgments
The authors acknowledge the contributions of the Bangladesh Demographic and Health Survey 2011 team for their efforts in providing open access to their dataset; icddr,b is grateful to the Government of Bangladesh, Canada, Sweden, and the United Kingdom for providing core/unrestricted support. The authors thank Ms Antara Kabir for support in editing the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Children’s Investment Fund Foundation-UK (CIFF) was the funder for operating research work of this unit. Authors invested their valuable time for this study. So, the study was indirectly funded by CIFF for the time invested by authors.