
Abstract
Background:
Despite improvements in the reduction of child stunting rates over the last decade, poor nutritional status still remains a public health concern in Bangladesh, where young children are the most vulnerable.
Objective:
The objective of this study is to capture the prevalence and determinants of childhood stunting and document its urban–rural disparities in the context of Bangladesh.
Methods:
The study used data from the Bangladesh Demographic and Health Survey of 2014. A bivariate analysis was performed to find out the differentials in prevalence of stunting, and multivariate logistic regression was performed to also assess the association of stunting with potential risk factors.
Results:
The overall prevalence of stunting was 36.3% and was significantly higher in rural (38.1%) areas than urban (31.2%) areas. In all 3 regression models, significantly higher odds were found among children aged 36 to 47 months compared to 6 to 12 months and among the children from the poorest households. In rural areas, male children were significantly more likely to be stunted (odds ratio = 1.31; 95% confidence interval: 1.12-1.53). Other significant risk factors for childhood stunting were maternal education and body mass index, children suffering from diarrhea, initial breast-feeding, and administrative divisions.
Conclusions:
Disparities exist among urban and rural areas regarding stunting among the children younger than 5 in Bangladesh, which need to be reduced. Public health policies and interventions need to consider the risk factors in urban and rural areas separately.
Introduction
Malnutrition is an emerging global public health challenge. One in 3 children is diagnosed as being malnourished in some variant globally, and it is linked with around 45% of all childhood deaths. 1 Furthermore, maternal and child undernutrition are jointly associated as the underlying cause of 3.5 million deaths, with 35% of the disease burden in children younger than 5 years of age and comprising 11% of the total global disability-adjusted life years (DALYs). 2 Globally, 1 (25%) of 4 children experience developmental delays, resulting in 155 million stunted children. 3 The prevalence of stunting is highest in sub-Saharan Africa and Asia, which accounts for 90% of all stunted children, with South Asia being at the epicenter of the global child stunting crisis. 4 The latest data indicated that 38% of South Asia’s under-fives are stunted. This prevalence is greater than sub-Saharan Africa (37%), almost 2 times higher than the Middle East and Northern Africa (18%), and more than 3 times higher than East Asia and the Pacific (12%) or Latin America and the Caribbean children (11%). 5,6 Stunting represents the failure of linear growth, both physically and cognitively, due to poor nutrition and infections both before and after birth. 7 Child stunting is thus a result of long-term chronic insufficiencies, as well as consumption of low-quality diet, in combination with infectious diseases and socioeconomic problems. In developing countries, stunting often starts in utero, and its severity gradually increases until it reaches a plateau at about 2 years of age, a time period called the “1000 days.” 2,8 Furthermore, stunted children are generally more vulnerable to infections, particularly diarrheal and respiratory diseases as well as malaria. Infections enhance malnourishment, creating a vicious cycle leading to growth shortcomings. 2,9 The functional consequences of stunting continue in adulthood including reduced work capacity and, in women, increased risk of mortality during childbirth and adverse birth outcomes. 10,11
The global prevalence of stunting has decreased from nearly 40% to 24%, and most of the progress in the reduction of stunting has been made in the Southeast Asian region. 4 In the line of progress, Bangladesh has achieved an improvement in reducing the child stunting rate in the last decade, but the percentage of stunting still remains at 36% among children younger than 5 years of age, while 12% of them are severely stunted. 12 However, young children and women in the prime reproductive ages are the most vulnerable to nutritional deficits. 12 Nevertheless, the rate of child stunting is still considered to be of a “high prevalence” according to the World Health Organization (WHO). 13 In the past few years, evidence has shown that the rate of stunting had declined by 5%, thus yielding an annual decrease of 1.5% in Bangladesh. 12 However, the prevalence is highly concentrated among the poorer socioeconomic strata, rural areas, and slum settings, although the etiology of stunting is still unclear. 14 Thus, it is crucial to identify the factors associated with childhood stunting, so stakeholders can implement evidence-based policies to improve nutritional status at the population level. In order to tackle the malnutrition burden, international community has set Sustainable Development Goal (SDG-2.2) to end all forms of malnutrition by 2030 and made commitments to reduce childhood stunting by 20 million and to avoid at least 1.7 million childhood deaths through the prevention of stunting. 3,6 Similarly, there are effective interventions in developing countries, such as behavior change interventions, micronutrient and deworming interventions, along with complementary and therapeutic feeding interventions 15,16 In previous studies, it has been reported that a number of factors, including distal factors (mother’s education, wealth quintile, region/division), intermediate factors (environmental factors, such as the number of children in a family, family size, availability of safe water supply and hygienic toilet, and maternal factors, including mother’s age at delivery, preceding birth interval, mother’s body mass index [BMI]), and proximal factors (birth order, childhood diarrhea, and immediate breast-feeding) are associated with child stunting. 17 Evidence from a multicounty analysis revealed that a considerable urban–rural difference exists in determinants and average child health outcomes throughout the developing world. 18 Thus, it is important to generate evidence regarding the determining factors of child health outcomes separately for urban and rural areas in order to design fundamentally different nutrition policies and interventions that will optimize the improvement in the nutritional status of children in the respective settings. Although there are a number of studies available in different corners of the world that address the risk factors associated with child stunting, 19 -23 there are a limited number of studies in Bangladesh that compare the prevalence and risk factors between urban and rural settings that use nationally representative data. In 2 earlier studies, Rah et al and Kamal reported the prevalence and determinants of stunting only among children of rural areas. 21,22 Menon et al showed the socioeconomic differentials in stunting among children from 0 to 36 months old in 11 selected countries. 23 In their study, they reported the prevalence of stunting in a comparison of the urban and rural areas within the selected countries, rather than describing the determinants of stunting. Srinivasan et al performed decomposition analysis to identify the covariate effects, using Bangladesh Demographic and Health Survey (BDHS) 2007 data. Therefore, we aim to contribute to this area by utilizing the latest country representative household-level data set in order to find such disparities. Consequently, the objective of this study is to capture the influence of the determining factors of childhood stunting as well as differentiating the urban and rural areas of Bangladesh.
Methods
Data and Study Design
The study used the cross-sectional data of BDHS, 2014. This is a nationally representative survey that is a part of the long-standing worldwide Demographic and Health Survey (DHS) program. This survey is conducted every 3 years and captures information covering individual and household-level, sociodemographic, and health indicators, and health-care data. A wide range of information, including background characteristics such as age, region of residence, place of residence, education, and household characteristics, was collected through questionnaire-based, face-to-face interviews, where reproductive-age women (15-49 years) were interviewed based on the MEASURE DHS program model. A 2-stage stratified random sampling technique was used in this survey. This survey used the sampling frame provided by the Bangladesh Bureau of Statistics, which was previously used for Population and Housing Census 2011 conducted in Bangladesh. Details about the sampling technique, survey design, survey instruments, measuring system, and quality control have been described elsewhere. 24 This survey was conducted from June 28, 2014, to November 9, 2014, by a trained and experienced data collection team. A total of 18 000 residential households were surveyed and, with the 98% response rate, the total of 17 863 interviews were completed among the 15 to 49 age-group in ever-married women. 12 Details of the DHS methodology are also elaborated in the MEASURE DHS website. 24 All DHS data are publicly accessible and were made available upon request by MEASURE DHS. Furthermore, approval was sought from and given by the MEASURE DHS program office to use this data set. According to the DHS, written informed consent was obtained from all participants enrolled in the survey.
Data Management and Analysis
Dependent variable
Data regarding height/length were obtained for children below 5 years of age. Height-for-age index was calculated according to the WHO Multicentre Growth Reference Study 2006 Child Growth Standards, where it is expressed in standard deviation (SD) units (z-score) from the median of the reference population as recommended by WHO and adopted in the Bangladesh DHS. 12,25 Height-for-age-z-score (HAZ) < −2SD was defined as stunted. Furthermore, HAZ between −2SD and −3SD was considered as moderate stunting and HAZ < −3SD as severe stunting. 13
Independent variables
In this current study, independent variables were selected based on the previous studies, where they identified risk factors associated with childhood stunting. 19,22,26 In the analysis, the child’s age was categorized into 6 groups and maternal age upon delivery into 3 groups. Self-reported maternal educational attainment was used and categorized as “no education,” “primary,” “secondary,” and “higher”. No education refers to not attaining any formal education, primary is defined as completing grade 5, secondary as completing grade 10, and higher is defined as attaining more than grade 10. 12 Birth intervals were categorized as the length of time between 2 consecutive live births. Maternal nutritional status was assessed by BMI, which was defined as a ratio of weight (kg)/[height (m)]2 and coded as follows: below 18.5 kg/m2 = thin; 18.5 kg/m2 to 24.9 kg/m2 = normal; and BMI ≥ 25.0 kg/m2 = overweight. 17 In BDHS, maternal perception of the size of children at birth (larger than average, average, and smaller than average) was obtained, despite the actual birth weight of children. Thus, the mother’s perceived birth size was used as a proxy for the child’s birth weight. Improved drinking water sources included water piped into dwelling, piped to yard/plot, public tap/standpipe, tube-well or borehole, protected well, rainwater, and bottled water. Nonimproved sources included unprotected well, unprotected spring, tanker truck/cart with drum, and surface water. Improved toilet facilities included flush/pour flush to piped sewer system, flush/pour flush to septic tank, flush/pour flush to pit latrine, ventilated improved pit latrine, pit latrine with slab, and nonimproved toilet facilities were flush/pour flush not to sewer/septic tank/pit latrine, pit latrine without slab/open pit, hanging toilet/hanging latrine, and no facility/bush/field. We utilized a predetermined wealth index, which was classified into 5 groups as: “poorest,” “poorer,” “middle,” “rich,” and “richest”, according to the earlier study. 17,19,20,27 Furthermore, mass media access, child birth order, breast-feeding initiation within first hours of birth, and household residing administrative divisions were also included in the analysis.
Statistical Analysis
All the outliers and missing observations were excluded from the analysis. Data were excluded if the z-score for a child’s height-for-age was below –6 or above +6. 28 Sampling weight, which was provided within the database, was used for weight data during the analysis. Descriptive bivariate analysis techniques, that is, frequency distribution, and cross-tabulation, were applied for measuring the prevalence of stunting in relation to relevant variables. Bivariate logistic regression analysis was calculated to assess the crude association between dependent and independent variables. Finally, variables that showed a significant association in bivariate logistic regression analysis and other variables of interest, and which were found to be associated in the relevant literature, were added into the multivariate logistic regression model to identify the association of independent predictors on stunting. Three different multivariate logistic regression models were performed for overall (model I), urban (model II), and rural (model III) strata to address the adjusted effects of different predictor variables of stunting in different areas and reported as an odds ratio (OR) with a 95% confidence interval (CI). A P value of <.05 was adopted as the statistically significant level. Diagnostic tests were employed in the analysis. Variance inflation factor test was employed to detect the multicollinearity in the regression model. All the statistical analysis was performed by using the statistical package STATA/SE 13 (Stata Corporation College Station, Texas).
Results
Background Characteristics
The distribution and characteristics of the study participants are described in Table 1. A higher percentage of children were from rural areas (74.2%), and the proportion of male and female children was 52% (95% CI: 50.8-53.3) and 48% (95% CI: 46.8-49.2), respectively. These differences in percentage were statistically significant. Considering maternal education of the study children, 45.8% had secondary education, followed by primary education (28.1%), whereas only 9% had higher educational attainment. According to the BMI scale of mothers, approximately 60% of mothers were normal (BMI Score: 18.5 kg/m2-24.9 kg/m2), while approximately 22% of mothers appeared as thin (BMI: less than 18.5 kg/m2) and 18% were overweight (BMI: more than 25.0 kg/m2). Most of the households consisted of 4 or more members and had access to safe water (97.8%) and improved toilet facilities (70%). Approximately 5.7% of children had diarrheal episodes in the last 2 weeks preceding the survey, 68% were average in size during birth according to their parents, and almost half of the children (53%) were breast-fed within the first hour of birth (Table 1). Table 1 shows percentage distribution of background characteristics of the study participants.
Characteristics of the Study Population.a

Abbreviations: CI, confidence interval, BMI, body mass index.
a n = study sample (differs for few variables due to missing data)
b Child size at birth was obtained by the perception of mothers and used as a proxy of birth weight.
c No education, primary, secondary, and higher education refers to not attaining any formal education, completing grade 5, grade 10, and completing higher than grade 10, respectively.
Prevalence of Stunting
The overall prevalence of stunting was 36.3%, whereas the prevalence was higher in rural areas (38.1%) than in urban (31.2%). In the overall stratum, the prevalence of stunting was found to be higher among the children aged 36 to 47 months of age (45.3%), and a similar situation was also observed in urban and rural areas. This age-group was also exposed to severe (HAZ < −3 SD) and moderate (HAZ between −2 SD and −3 SD) stunting (15% and 30.3% for severe and moderate stunting, respectively; Figure 1). No significant difference was observed in the prevalence among male and female children (36.5% vs 36.1%). It was also observed that the prevalence of stunting was higher among children whose mothers had no formal education (47%) and were aged more than 35 (44.5%) years at the time of delivery. The maternal BMI was significantly associated with the prevalence of stunting in urban and rural areas. Prevalence of stunting was higher among children from thin mothers (BMI < 18.5 kg/m2) and children from households who did not have access to safe drinking water and improved sanitation facility. This was also the case among the children who were exposed to diarrheal episodes (46.8%) in the last 15 days preceding the survey. According to the administrative divisions, prevalence of stunting was highest in the Sylhet regions (50.2%), followed by Barisal (40.4%). Children from comparatively lower economic groups suffered more from stunting, in terms of prevalence, as it was found that prevalence of stunting was high among children from the poorest household in all urban (47.4%), rural (50.4%), and overall (50.1%) strata. Table 2 shows prevalence of stunting among under-five children by residence in Bangladesh.
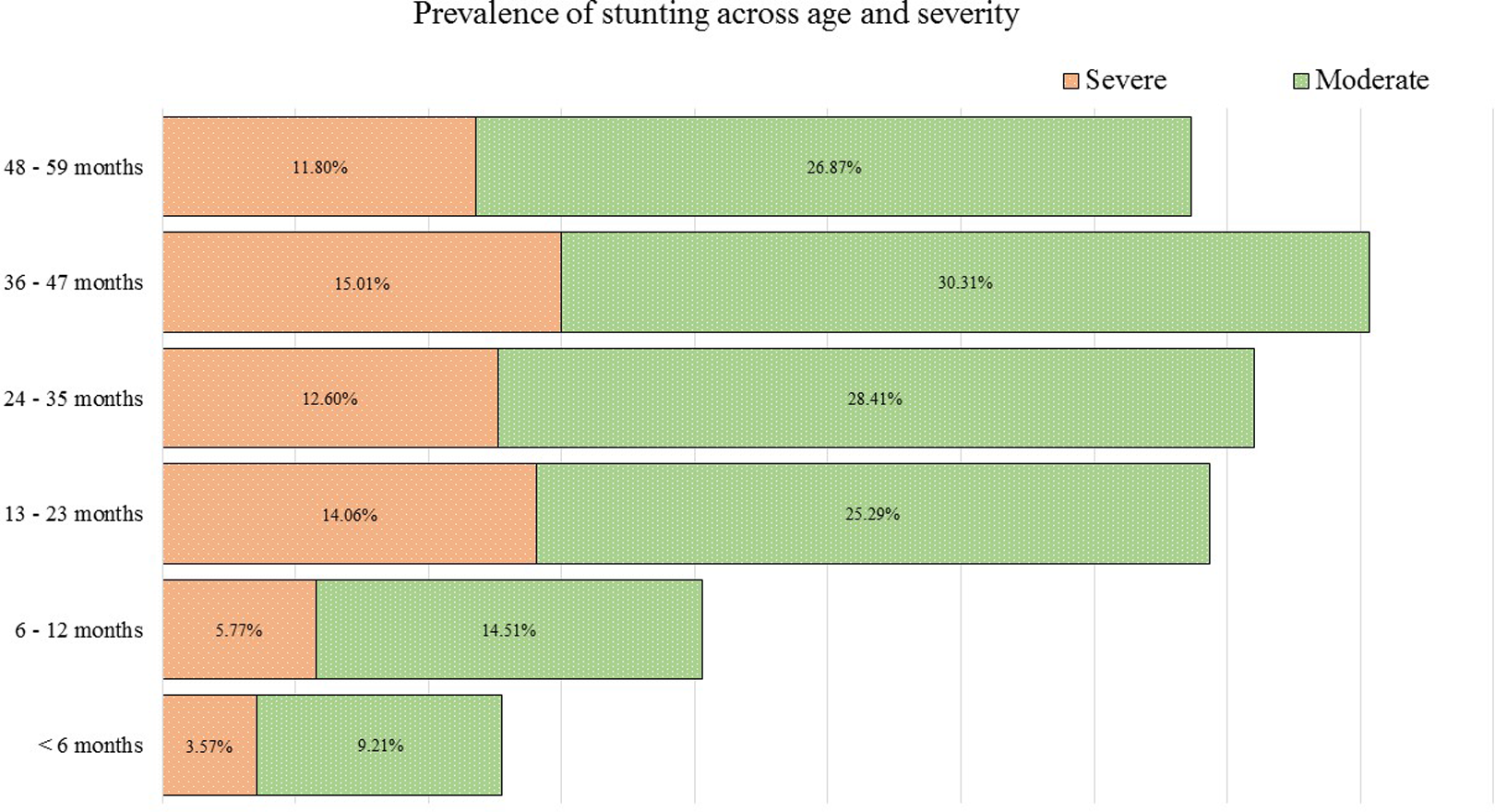
Age-specific severe and moderate stunting.
Prevalence of Stunting among Under-Five Children by Residence in Bangladesh.
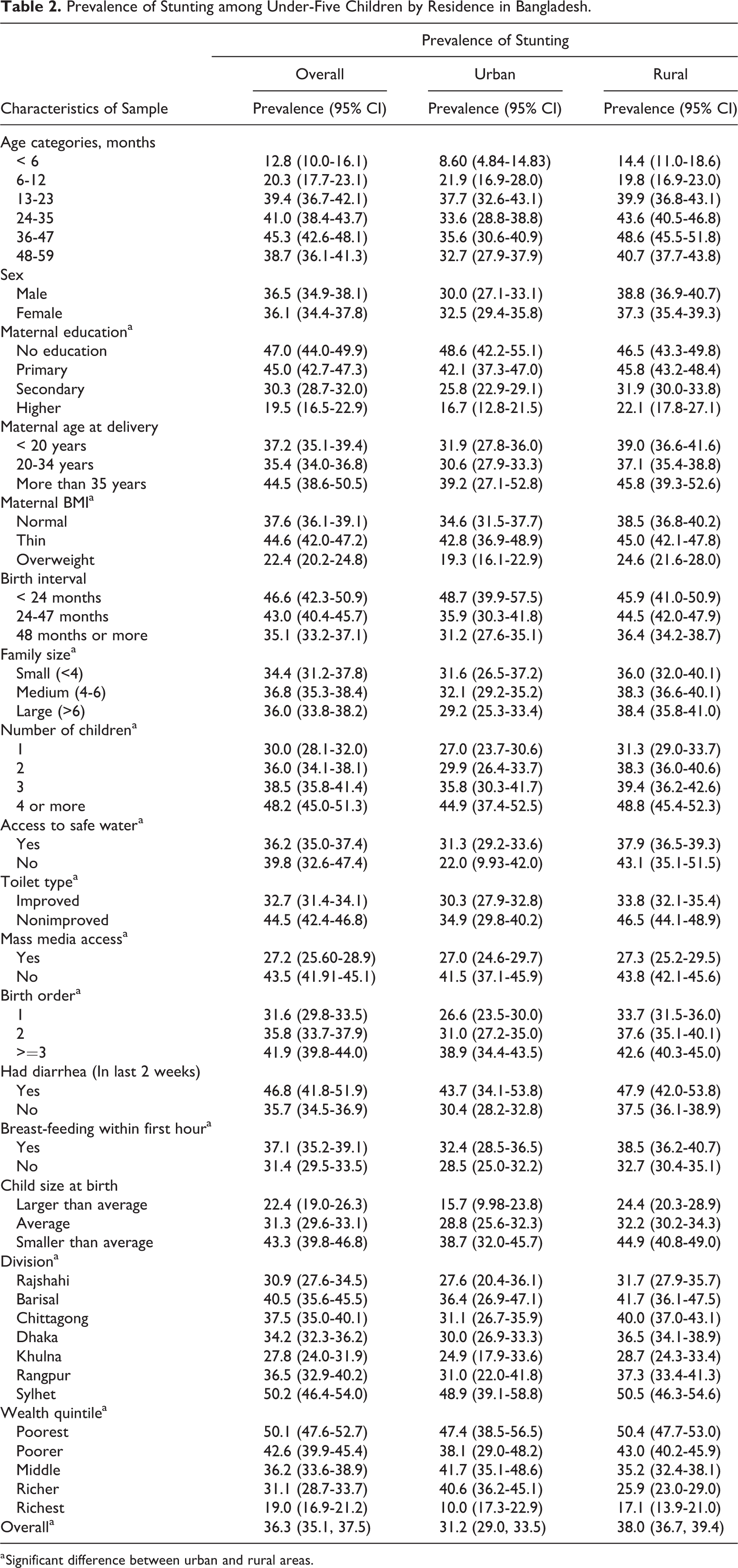
a Significant difference between urban and rural areas.
Factors Associated With Stunting
Risk factors associated with stunting are described in Table 3. In all the 3 regression models, children in each of the categories of age 36 to 47 months had significantly higher odds of being stunted, compared to children 6 to 12 months (OR = 5.53; 95% CI: 3.81-8.02, OR = 4.0; 95% CI: 1.67-9.58, OR = 6.1; 95% CI: 4.01-9.26 for model I, II, and III, respectively). Conversely, children aged <6 months had significantly lower odds of being stunted compared to the children from the reference group. In models I and III (overall and rural area), it was found that male children were significantly more likely to be stunted (OR = 1.21; 95% CI: 1.06-1.39, OR = 1.31; 95% CI: 1.12-1.53 for model I and III, respectively) than females. However, in urban areas, female children were more likely to be stunted, though this was not statistically significant. Maternal education appeared as a protective factor for avoiding childhood stunting. Children of illiterate mothers were found to be 2.12 times (95% CI: 1.49-3.02) more likely to be stunted, compared to higher-educated mothers. Mothers’ BMI was found as a significant factor for the children to be stunted. The findings revealed that children of overweight mothers had a lower risk of stunting than mothers with a normal BMI. Findings from the regression model II revealed that, in urban areas, a second-born child was 1.92 times more likely to be stunted than the first-born child. However, no such associations were found in rural and overall areas. In our study, a significant association was also found between stunted children and childhood diarrheal illnesses (OR= 1.85; 95% CI: 1.41-2.42). In the administrative division-wise distribution of prevalence, it was shown that Sylhet was the highest risk area for stunting, where children of that division were 2.06 times more likely to be stunted than those in the Rajshahi division (95% CI: 1.52-2.79; P < .001). Furthermore, stunting was also significantly associated with the economic status of the households. Children from the poorest group were 2.34 (95% CI: 1.71-3.2) times more likely to be stunted when compared to the richest households.
Multiple Logistic Regression Analysis of Associated Factors for Prevalence of Stunting Among Under-Five Children in Bangladesh.a
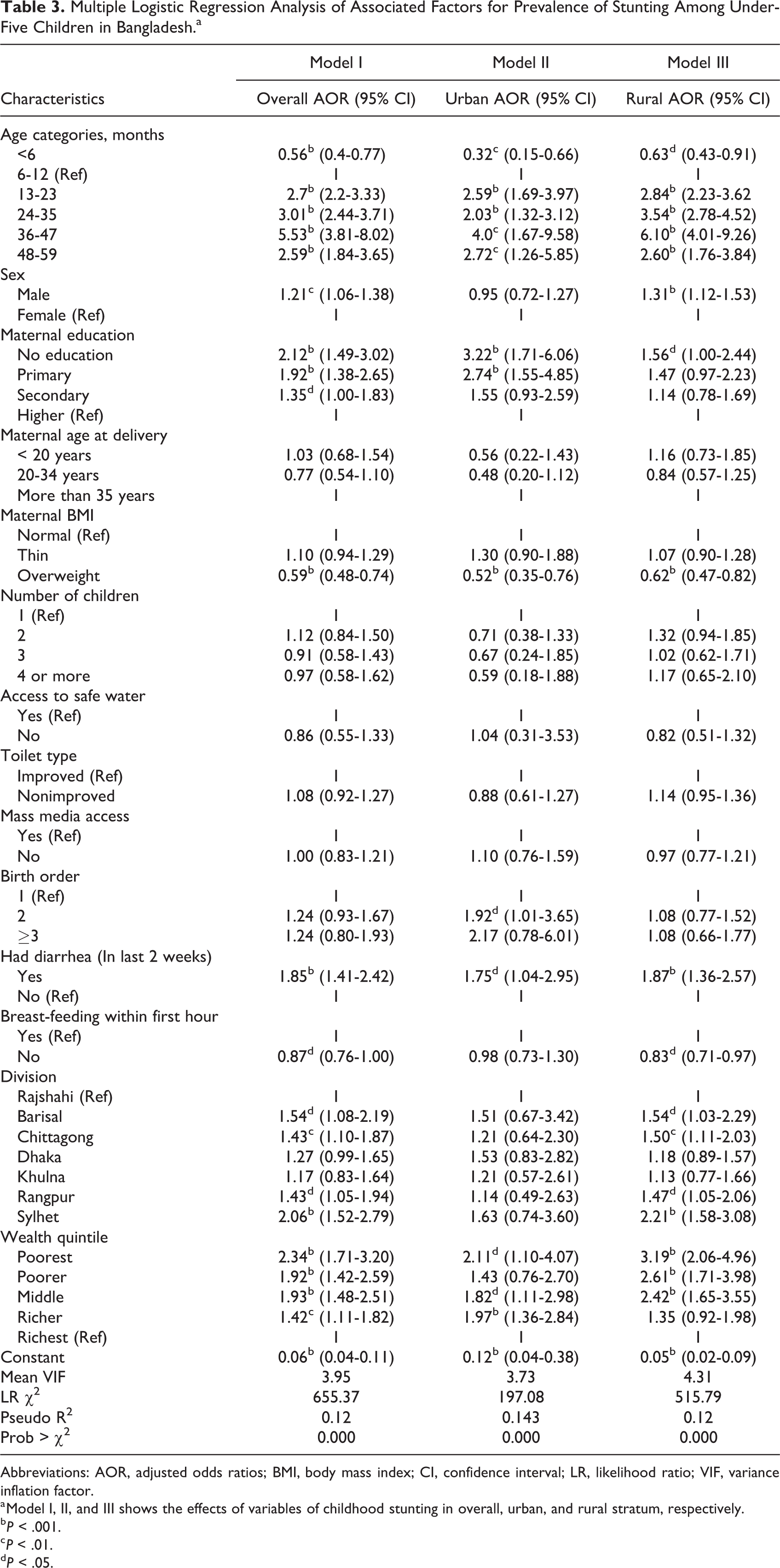
Abbreviations: AOR, adjusted odds ratios; BMI, body mass index; CI, confidence interval; LR, likelihood ratio; VIF, variance inflation factor.
a Model I, II, and III shows the effects of variables of childhood stunting in overall, urban, and rural stratum, respectively.
b P < .001.
c P < .01.
d P < .05.
Urban–Rural Disparities
Two different models (model II and III) as shown in Table 3 showed associations of different factors of childhood stunting for urban and rural areas. Findings revealed that there were significant gender differences in the prevalence of stunting in rural areas, but no such differences were found in urban areas. In rural areas, male children were more likely to be stunted (P < .001). However, in urban areas, female children were found to be at higher risk rather than the male children. Maternal education was found as a protective factor for childhood stunting in both urban and rural areas. Moreover, in urban areas, odds of uneducated mothers were relatively much higher than rural uneducated mothers. A positive association between birth order and prevalence of stunting was found in urban areas, but in rural areas, odd ratios of different birth order were similar. The prevalence of child stunting was higher in both urban and rural areas of the Sylhet division compared to Rajshahi division. This association was found to be significant in rural areas, but no significant associations were found in urban areas. In both the urban and rural areas, the poorest children were more at risk of being stunted. Moreover, the odds of being stunted was comparatively higher for children of poorest household in rural areas (OR = 2.11; 95% CI: 1.10-4.07 vs OR = 3.19; 95% CI: 2.06-4.96). Table 3 shows multiple logistic regression analysis of associated factors for prevalence of stunting among under-five children in Bangladesh.
Discussion
Despite greater successes accomplished by Bangladesh in reducing all forms of malnutrition, our study observed that the overall prevalence of stunting was still 36.3%. According to the cutoff values for public health significance by WHO, this prevalence rate lies in the high-prevalence category (30%-39%). 13 We found that the prevalence of stunting was higher among rural children when compared to urban children, a phenomenon that has been frequently observed in other developing countries. 19,23,29 -31 This can be explained by the fact that lower education, poor socioeconomic status, scarcity of potable water supply, prevalence of infectious disease, and poor nutritional knowledge persist more in rural areas than in urban ones. 32 Furthermore, the knowledge on infant and young child feeding practices was also poor among rural mothers. 33 Moreover, the rapid urbanization and high poverty had an effect on malnutrition. 34 The prevalence of stunting in Bangladesh is similar to its neighboring countries: 27.5% in Bhutan, 35 28.4% in Indonesia, 36 35% in Pakistan, 37 and 43% in Nepal. 38 Our study found that a higher prevalence of stunting prevailed among children aged 36 to 47 months, which is commonly observed in different settings. 22,38,39 The high rate of stunting among this age-group (Figure 1) was linked to inappropriate food supplementation that was provided to the child during the complementary feeding period (6 to 24 months). 32 During this time period, breast milk alone is no longer sufficient in meeting the nutritional needs of child, and due to insufficient nutritional intake, malnutrition begins as is reflected at later stages. 40 Our findings demonstrated that the sex of children was a significant factor for childhood stunting. These findings were confirmed by other studies, where they also found that male children were significantly more likely to suffer from stunting. 17,22,41 The reason for this gender divergence is not well established, but it is believed that boys are more influenced by environmental stress than girls. 42 Our study also demonstrated that maternal education was a significant positive factor for controlling childhood stunting, and a child from a higher-educated mother suffers less, and findings are in line with other studies. 19,29,31 Mothers are the primary caregiver of the children, and their education and knowledge are expected to have a stronger effect on protective child-caring behaviors, which would lead to the child’s improved health. 43 Mass media exposure is an important source of knowledge for avoiding malnutrition, as it provides various health awareness–related programs. In our study, access to mass media was found to be associated with childhood stunting in the bivariate analysis. However, no significant association was found in multivariate analysis. Like other studies, we found that the maternal higher BMI displayed a significance in being a protective predictor for childhood stunting. 44,45 We further observed that a child with a higher birth order had a significantly higher risk of stunting. This can be explained by the fact that extra care and food supply are required for larger size of households, which lead to a higher consumption of resources and could thus lead to stunting. 46
A bidirectional relationship between diarrhea and malnutrition has been observed in various studies. 38,47 Our study observed that there was a positive association between stunting and childhood diarrhea. 47 However, such relations were not always observed. A study in Nepal found that diarrheal disease occurring in the last 2 weeks was not associated with childhood stunting. 38 In addition, a negative relation was also observed between immediate breast-feeding and childhood stunting. Our result showed that children who were not immediately breast-fed were less likely to be stunted, as exclusive breast-feeding was a factor for child stunting. 29,31 This might be because breast-feeding was considered as a substitute for supplemental feeding up to a certain age of the child, and thus many of the children were not fed other nutritious foods in sufficient amounts, resulting in malnutrition and stunting. 48
Furthermore, regional heterogeneity in the prevalence of child stunting was observed in our study, where more prevalence of stunting was found among children living in the Sylhet division when compared to other regions. The Sylhet division is known as a poor-performing region among most of the health indicators. 49 Although the Sylhet division receives a large flow of foreign currency, people were seen to be investing more in land purchasing and housing rather than in health, education, and the consumption of foods, which might underpin such findings. 49 Children from the poorest households frequently suffered from stunting, and the odds of suffering from childhood stunting declines consistently as the wealth index increases. 17,19,20,31 This might be due to the fact that lower economic people could afford less to receive proper nutrition and might sometimes have to lower calories intake from the minimum daily requirement. On the contrary, higher socioeconomic positions are likely to represent better living conditions with higher affordability, which again contributes to better child care and improved feeding practices. This leads to a decline in the occurrence of different forms of malnutrition. 50
The study had several limitations. First, this study was based on cross-sectional data, which failed to establish a casual relationship. Second, due to the unavailability of data on potential confounders including childcare practices, food taboos, management of illness, and smoking behavior of the parents, these were not included in the analysis. The definition of urban and rural areas in Bangladesh has changed over time with a rapid growth in urbanization. As a result, some areas that were earlier classified as rural in the previous Bangladesh DHSs were considered urban in the more recent BDHSs, which may lead to emerging discrepancies in urban–rural calculations.
Our study revealed that a prevalence of stunting was higher in rural areas and among children aged between 36 and 47 months. A number of factors, such as age, sex, maternal education, mothers’ BMI, administrative divisions, and socioeconomic status, are significantly associated with childhood stunting. This study will help inform the efforts of future and ongoing activities related to nutritional promotion that can serve as a platform to prevent childhood stunting in Bangladesh. However, special focus and care are necessary for rural areas in order to improve the overall performance of the health, nutrition, and population sector. This is particularly so if it is to reach the targets set by SDG 2 of zero hunger and the end of all forms of malnutrition. The policy should focus on nutrition-specific interventions, in particular such as dietary supplementation, optimal feeding practice, exclusive breast-feeding, and childcare awareness related programs, which target the rural and unprivileged population for reducing childhood stunting at the population level. A joint effort involving the government and nongovernmental organizations is also necessary to improve the nutritional status of children.
Footnotes
Acknowledgments
The authors would like to thank health economics and financing research group for their comments on an earlier draft of the manuscript. Icddr,b is also grateful to the Governments of Bangladesh, Canada, Sweden, and the UK for providing core/unrestricted support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.