
Abstract
Background:
The delivery of vitamin A supplements in Ethiopia has been shifting from Child Health Days (campaigns) to routine delivery via the community health services.
Objective:
The objective of this study was to compare the cost and effectiveness of these 2 delivery methods. No previous studies have done this.
Methods:
A mixed method approach was used. Quantitative data on costs were collected from interviews with key staff and coverage data from health facility records. Qualitative data on the 2 modalities were collected from key informants and community members from purposefully sampled communities using the 2 modalities.
Results:
Communities appreciated the provision of vitamin A supplements to their under 5-year-old children. The small drop in coverage that occurred as a result of the change in modality can be attributed to normal changes that occur with any system change. Advantages of campaigns included greater ease of mobilization and better coverage of older children from more remote communities. Advantages of routine delivery included not omitting children who happened to miss the 1 day per round that supplementation occurred and not disrupting the availability of other health services for the 5 to 6 days each campaign requires. The cost of routine delivery is not easy to measure nor is the cost of disruption to normal services entailed by campaigns.
Conclusion:
Cost-effectiveness likely depends more on effectiveness than on cost. Overall, the routine approach can achieve good coverage and is sustainable in the long run, as long as the transition is well planned and implemented.
Introduction
The distribution of vitamin A supplements has been an important strategy in helping to improve child health and make progress toward the Millennium Development Goals. Vitamin A deficiency was well known to be important in reducing morbidity and mortality associated with measles. A meta-analysis of trial results 1 showed that there were benefits for diarrhea and pneumonia. An update 2 found a 24% reduction in all-cause mortality and a 28% reduction in diarrhea mortality. When a large trial in India which did not find an impact is included, there is still an improvement in mortality albeit somewhat lower. 3
Following these studies, there was a large expansion of programs, with international donor support, which was further reinforced by the development of World Health Organization guidelines that children aged 6 to 59 months should receive supplements every 4 to 6 months in countries where deficiency is a public health problem. 4 By 2012, more than 70 countries had national scale supplementation programs, and United Nations Children’s Fund (UNICEF) estimates that by 2015 global 2-dose coverage has reached 69%. 5
A common way of delivering supplements, given the limited capacity of health services in many low- and middle-income countries, has been through campaigns such as Child Health Days. These campaigns deliver a package of services such as deworming and nutritional screening, as well as vitamin A capsules, on specific days during the year. Child Health Days in sub-Saharan Africa have been shown to be both modest cost (per child) and cost-effective. 6 –9
With the shift from the Millennium to the Sustainable Development Goals, there has been a recognition of the importance of moving to a form of delivery that is less reliant on external donor funding, which supports the strengthening of the capacity of the routine health system. Immunization services have already largely moved to routine delivery, and a number of countries are beginning a similar transition for vitamin A distribution, often piloting the shift in a few areas before rolling out the strategy more broadly.
We examine the shift of pilot districts (woredas) in 1 region in Ethiopia starting in 2013 and compare the experience with that of other districts in the same region continuing with campaign distribution. The specific research objectives were to compare the coverage of supplementation in the 2 modalities, to compare costs and effectiveness, to examine the perceptions of stakeholders, and to identify factors contributing to the success of delivery using each method. A mixed methods (quantitative/qualitative) approach was used to provide a richer evidence base.
We first describe the context in Ethiopia, then the research methods used, and the results and finally discuss the implications of the findings for policy purposes and provide brief conclusions. We are not aware of other studies comparing campaign and routine distribution of vitamin A capsules, other than a parallel study initiated at the same time for Senegal, with which we make comparisons (unpublished data).
Background
Ethiopia has 9 administrative regions and 2 city administrations. Each region is divided into districts (woredas) with 1 or more health centers (first-level hospitals) with several trained health personnel. Oversight at the district level is provided by the woreda health officer. Districts are further divided into kebeles (subdistricts: the smallest administrative structure, with an average population of 5000). Woreda Health Offices supervise health centers, which in turn supervise up to 5 satellite health posts. The health posts should have 2 salaried health extension workers (HEWs) supported by community volunteers (such as the Women’s Development Army). Ethiopia has invested in health services, building additional health posts to achieve a ratio of 1 health post per 5000 population (ie, 2500 population per HEW). 10 The goal is to have 1 supervisor per 10 HEWs and for each HEW to be supported by 10 to 15 volunteers (approximately 1 volunteer per 25-30 households). 10
There has been a gradual evolution in primary health and nutrition interventions for children in Ethiopia, accompanying the investments in the health system. In 2004, the Enhanced Outreach Strategy (EOS) began in 4 drought prone regions. Mobile teams went from kebele to kebele to provide vitamin A supplements, deworming, and nutrition screening during twice-yearly campaigns. Malnourished children and pregnant and lactating women were referred to supplementary feeding programs. By 2006, the whole country was included, although nutrition supplements were restricted to the drought prone regions. Almost 10 million children received vitamin A supplements in 2006. 6 High coverage rates were achieved, with UNICEF supporting two-thirds of the costs and providing organizational support. 6 Health extension workers and their supervisors received outreach allowances for the travel that was entailed.
In 2008, pilot districts in the original 4 regions began to transition the package of nutrition interventions from the EOS to Community Health Days (CHDs), with the aim of gradually integrating the activities into the routine health services. This was phased, with high-performing districts in the agricultural areas in selected regions transitioning first. Health services were less well developed in the pastoralist areas, and the urban system was still in development. 10
Communities were mobilized to attend campaign sites arranged by each health post on specific days (CHDs) every 3 months to receive a package of services. These services included deworming and vitamin A supplementation (every 6 months) and nutrition screening (every 3 months). The quarterly campaigns occurred within a specific month during the 6-month period and were organized at woreda level. Services could also be provided both at outreach sites during the campaigns or (in urban areas) house-to-house. These campaigns were conducted by HEWs with the assistance of volunteers. 10 Health extension workers no longer received outreach allowances, as this work was integrated into their normal workload.
The third step began in 2013, when districts where CHDs were well established transitioned fully from the CHD model to use of routine services and urban districts began to transition from EOS directly to use of routine services. The EOS continued in 3 regions where health system coverage remains limited (regions where pastoralism remains high). The aim was to provide nutrition services during visits to health posts and household visits occurring as part of the routine health services. Health extension workers had flexibility to adopt other methods to maintain coverage, such as “mini-campaigns” within the community to “mop up” those not reached.
Ethiopia has maintained good coverage with supplements throughout these changes. National coverage of vitamin A supplements was at least 80% in each of the 2 annual rounds between 2006 and 2011 inclusive (with 1 exception). 5 Coverage fell to 31% in both rounds in 2012 and then rose back up to between 70% and 80% in the 4 rounds in 2013 and 2014. 5 Data for 2015 were not yet available in the UNICEF database.
The success of transition to routine health services was expected to require strong supervision from the health center level, use of the family folder (ie, health records) to identify those who were unreached, and the support of community mobilizers (Women Development Army, Traditional Birth Attendants, community leaders, and others), among other strategies. 11 An evaluation early after implementation found that 54.2% of community members surveyed accessed the package of services at the health post and 34.3% at outreach sites and identified some of the issues to be solved including supply of materials, additional supervision of HEWs, and additional community mobilization.
Methods
A mixed methods approach was used to provide a richer picture of the 2 vitamin A supplement delivery modalities in Amhara region of Ethiopia. Amhara region has 145 woredas of which 23 have 2 to 3 years of experience of routine service delivery, whereas the rest are still utilizing CHDs for delivery. Data were available by woreda on the level of coverage of Vitamin A supplementation (VAS). From those woredas using routine delivery, one was selected in the second quartile according to coverage levels for the first half of 2015 and one from the third quartile. Similarly, from those woredas using CHDs, one was selected from the second quartile in terms of performance and one from the third quartile, also using some judgment to select woredas with similar characteristics to the routine woredas selected. Criteria used were population density and being predominantly agrarian (as opposed to urban or pastoral).
Coverage of children aged 6 to 59 months across the 23 routine woredas in the first 6 months of 2015 ranged from 29.8% to over 100% with a median of 85.3%. In the routine areas, the high-performing woreda selected for study (Ebinat) had a median coverage of 96.8%, compared to 77.6% for the relatively low-(average) performing woreda (Raya Kobo). Similarly, coverage across the 55 CHD (campaign) woredas for January 3 to 8, 2016 ranged from 49.6% to over 100% with a median of 91.7%. The high-performing woreda (Mecha) selected for study had a median coverage of 97.9%, compared to 87.3% for the relatively low-(average) performing woreda (Bure Zuria). In general, the range of performance was greater for routine service delivery than for campaign, and the median performance was slightly lower for routine than for campaign.
Two different quantitative questionnaires were developed loosely based on one used by Jarco Consulting and Addis Ababa for the baseline survey undertaken soon after the 2013 shift in distribution methods. One questionnaire was used for the HEWs who distribute the supplements at the community or kebele level and 1 for their supervisors, who are based at the health centers. The questionnaires were customized to be appropriate for routine and for campaign service delivery.
Separate, more open-ended, questionnaires were developed for the Head of the Woreda Health Office (both modes of service delivery) and for the Coordinator of the CHDs (only for the CHD modality areas). Guides were developed for focus group discussions with mothers, groups of fathers/local community leaders, and with the Women’s Development Army (the most significant group of unpaid volunteers who support the HEWs by mobilizing the community). Questionnaires and focus group discussions guides were translated into Amharic. Research ethics approval was obtained from Jimma University College of Health Sciences.
Interviews were conducted with 14 key informants at woreda/kebele level to collect qualitative and quantitative data. For qualitative data, interviews were conducted with 4 woreda health officers and 2 CHD coordinators in CHD areas only. Interviews to collect quantitative data were conducted with 4 HEW supervisors and from 4 HEWs at health posts. In addition, 2 interviews to collect qualitative data were conducted with Non-government organization (NGO) partners at national level and 1 interview with the regional nutrition lead for Amhara.
A total of 16 focus group discussions were conducted: 4 with mothers living close to the health post (within about 30-minute walk), 4 with mothers living further from the health post (more than about 1-hour walk), 4 with fathers/male community leaders, and 4 with members of the Women’s Development Army. This was done to assess if there were any differences between VAS coverage and also perceptions of the services between mothers who lived near and those who lived far from the health posts. The focus groups had between 6 and 11 participants each, that is, more than 120 participants in total. The focus groups were timed to occur on community holidays to make it easier for people to participate. Fieldwork was undertaken by 2 teams of 3 individuals over a 2-week period in August 2016, which included 1 day for training and pretesting.
The interviews of the health officials (woreda health officers and CHD coordinators) covered health status of the area, methods of mobilizing the community for VAS, perceptions as to adequacy of coverage of VAS, barriers to and facilitators of coverage, and how the respondent perceived the difference between their current method of supplementation as compared to the other modality. Interviews were also conducted with 2 partner agencies at national level and with the regional nutrition lead for Amhara. Quantitative interviews of HEWs and their supervisors covered time required for administration of supplements and for travel to deliver supplements and to transport supplies, as well as any financial costs of transport required. Questions were also asked about time required and transport costs for supervision and for training.
Participants in the community focus groups were asked about their knowledge of vitamin A and its importance, about the provision of services (how they are provided, barriers and facilitators), and their opinion as to the comparison between the 2 different methods of distribution (campaign vs routine). Interviews and focus groups typically took 1 hour to 1.5 hours, with only 3 of the 30 lasting less than an hour (1 of 30 minutes, 2 of about 45 minutes). Participants in interviews and focus groups gave free and informed verbal consent to digitally record the data which were later translated and transcribed in English by some of the interviewers.
Qualitative data (interviews and focus groups discussions) were analyzed following the principles of qualitative description and thematic content analysis. This involved coding data into major categories of information during open coding. 12 It also included reassembling and grouping data on the basis of patterns and relationships between and among categories. Results were validated using the triangulation method, that is, comparing responses from different sources of information, for example, mothers, fathers, and health officials. Quantitative data that were transferred to an Access database were analyzed using Excel.
Results
Mothers have a generally positive opinion of the package of nutrition interventions they receive from HEWs, although not always being completely clear as to why the interventions are beneficial. It was noted that they often describe the package of nutrition interventions as “vaccination.” One mother commented about vitamin A: …there is lack of information; we just bring our children because we are told to do so. But no one told us about the benefits of VAS. So, the way information is given to us should be modified. It prevents children from illness; it is good. Children will be good in their education. When we hear that “vaccination” is being given, we bring our children so that they will get it. The drug is good. It is good for eyes. It also helps to prevent deafness. Vitamin A frees children from intestinal parasites and prevents them from trachoma.
Activities of Health Extension Workers and Their Supervisors, Campaign, and Routine Areas.
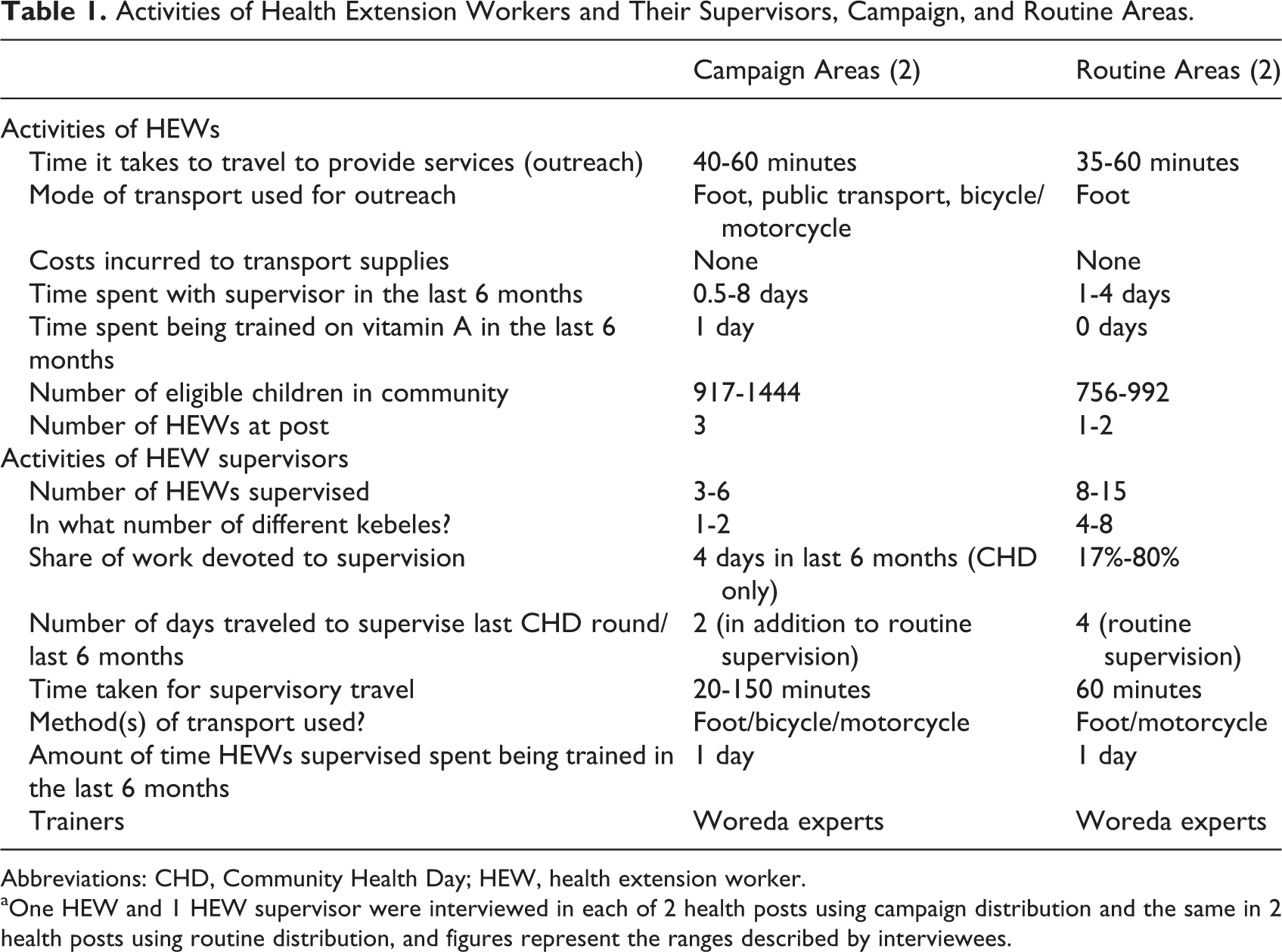
Abbreviations: CHD, Community Health Day; HEW, health extension worker.
aOne HEW and 1 HEW supervisor were interviewed in each of 2 health posts using campaign distribution and the same in 2 health posts using routine distribution, and figures represent the ranges described by interviewees.
In campaign delivery, levels of supervision are higher (additional supervisors are brought in for the campaign week), and refresher training on vitamin A is more frequent (there is typically 1 day of training per campaign). Transport is more readily available through partner support during the campaigns to reach the more remote communities, whereas the HEW in routine mode is expected to arrange for her own travel, which often results in it being on foot or bicycle. Given that the additional training and supervision and transportation for the campaigns require support by partner funds, this can be difficult to sustain in the long run.
However, even in routine areas, somewhat of a hybrid approach is used to boost coverage. To improve coverage, HEWs conduct locally organized mini-campaigns. These involve either mobilizing the community to come to a local fixed point for service on a specific day or house-to-house provision of services or both. Health extension workers still undertake quarterly nutritional surveillance of children and can use this opportunity to remind mothers of the need for regular vitamin A supplements.
Younger children are more likely to be brought to the health post, either for routine vaccinations or because they become sick more frequently or because the mother brings the youngest child along when she is seeking care for herself. Older children are less likely to be brought: they become too heavy for the mother to carry, but at the same time, they are not old enough to travel long distances on foot, especially if the community is far from the health post.
Key informants (health officials at regional and woreda levels and NGO partners) provided their opinion as to the advantages and disadvantages of the 2 modes. Routine service delivery will address eligible children exactly at the right time. There will also be no burden over a short period of time. It also will have no extra budget requirement as it is already integrated with other services. It has no pressure on the community to bring all children at a time. So it is better from these perspectives. CHDs [are] effective…to achieve short-term objectives, but it has questionable sustainability…it weakens other activities. CHD is better for us because mothers will not bring their children here for “vaccination.”…mothers are busy with domestic work; they postpone times to bring children and eventually they don’t bring them. We may have two or three children under the age of five. We can’t bring all of them at a time if the service is routinized. As VAS is given for children in the age group six months to five years, a mother may have children of age six months, two years, and five years. She cannot bring all these children to the health post. For this reason, I think CHD is better. Because of the expectation community members have about family planning there is also a saying ‘have you got another baby again?’ in our community. Mothers fear that their relatives and neighbors will say that. As a result, they don’t want to travel to the health post with all their children. They will either totally avoid coming to the health post or bring only some of their children. I think routine is better…if I am not around during those days (CHDs), I can still get my child vaccinated at my convenient time. In CHDs, I can’t get them after the days are over. So, for me the routine one is good.
Discussion
Coverage of vitamin A has dropped slightly in routine delivery compared to campaign delivery. As discussed above, median coverage in the routine districts was 85.3%, compared to 91.7% in the campaign ones, with the range being larger in the routine districts. However, the difference was considerably smaller than in Senegal, where national data for the second half of 2015 showed that mean coverage in the 5 routine regions was 54% compared to 98% in the 9 campaign regions (Mamadou Diouf, Micronutrient Initiative, pers. comm).
It was not possible to estimate costs and cost-effectiveness of supplementation. The sample size (4 woredas) was too small for this purpose, and the questionnaire was not detailed enough even for the campaign style, to capture all cost elements. Insufficient quantitative data were collected at regional and national level where much of the oversight occurs.
It is particularly difficult to calculate costs in routine delivery, since the distribution of vitamin A capsules is so intertwined with the provision of other services. It would require a time and motion study of HEWs and their supervisors over an extended period to truly estimate the proportion of their effort allocated to delivery of vitamin A supplements: we contend that this would not be worthwhile. It is quite likely that cost of routine delivery is lower than campaign delivery, but whether it is more cost-effective depends critically on the levels of coverage achieved.
One previous study found that the Expanded Outreach Strategy package of nutrition interventions was both modest in cost (USD$0.56 per child covered) and very cost-effective (USD$9 per disability-adjusted life-year—averted and USD$228 per death averted: data for 2006). 6 At that time, UNICEF covered 68% of the costs, and concerns were expressed about the long-run sustainability of the program. 6
One factor limiting coverage when using routine delivery is related to record-keeping. In campaign mode, no record is kept of the names of children receiving the supplement, just a tally of numbers of children in the 2 main age groups (6-11 months and 12-59 months). In routine mode, it is necessary to keep track of the child’s name, both in a register at the health post and in the family folder. This is done both to obviate the same child receiving the supplement too frequently and to identify those children who are missed. However, the HEW may have to walk as long as 4 to 5 hours to reach some very remote communities. In these circumstances, she cannot carry a heavy register or pile of family folders with her. Some HEWs simply keep records on pieces of paper as they travel to outreach sites and may not have time to transfer these into the health post records.
Literacy is another limiting factor for mothers who do not necessarily remember to take their older children regularly for supplements. They are busy with agricultural and household work.
Workload of HEWs is another issue which limits coverage in routine delivery. Each HEW is responsible for an average 2500 households, including around 500 eligible children, and for delivering around 16 different packages of services to the households. Health extension workers may be expected to walk for several hours to reach remote households, yet receive relatively low salaries. 10
On the other hand, the well-planned transition to routine delivery in Ethiopia has helped to maintain coverage. Government documents in 2010 provided a blueprint for how the transition would occur. 10 The plan triaged the path for the 3 different areas (pastoral, agrarian, and urban) according to the different conditions, with an explicit ratios of health posts to population, health posts to HEW, supervisor to HEW, and health volunteers to households. While other countries such as Senegal and Uganda use partner funds in campaign delivery for per diems for supervisors and incentive payments for outreach, Ethiopian government policy was that HEWs and supervisors should not receive these bonuses: rather, outreach is an inherent part of the work. Thus, the government is phasing out reliance on partner funding. 11
Transitional funding played an important role, which totaled USD$5.3 million between 2012/2013 and 2015/2016. The Ethiopian government contributed a little over half, with the balance from international partners (mainly Micronutrient Initiative plus UNICEF). These resources funded new behavior change communications materials including mass media (14% of the total), training for HEWs and health managers (22%), meetings for monitoring and evaluations of the new system (48%), printing and distribution of new monitoring tools (6%), and on-the-job mentoring (11%; data from unpublished records of the Micronutrient Initiative).
Another factor was that community mobilization did not disappear. Quarterly mobilization continued to occur for nutritional surveillance. This provided HEWs and opportunity to remind mothers whose children had not received their regular supplement dose of the need to catch up.
There were limitations of the research. We examined only 1 region, and within that region, only 4 woredas, 2 implementing each service modality. The sample is too small to be representative. The woredas selected are themselves not representative: the ones selected to make the transition to routine were ones where the nutrition package was working well. When undertaking fieldwork within a short time frame, those localities which are more accessible were more likely to be chosen over those which involve long travel over difficult terrain. The “low-performing” health posts identified have coverage below the median for the Amhara region but are still in the third quartile of the distribution, compared to others using the same delivery mode in the same region. The worst-performing health posts simply were never up for consideration because they did not provide coverage data. Similarly, individuals who participated in focus groups were selected by the HEW and may not necessarily have felt free to speak openly about concerns.
Conclusions
Our findings suggest that it is more difficult to achieve the same coverage with routine services than with campaigns in a low-income country such as Ethiopia. Ethiopia’s decision to eliminate per diems but build more health posts and hire more community health workers is an approach from which other countries can learn.
The over 100% achievements of campaigns in many areas conceal the fact that mothers may bring older children to participate, whereas some vulnerable children are still missed, since campaigns typically record the number of children who participate but do not track individual children. Our qualitative survey indicated that mothers found both delivery modalities acceptable, and each mode had its advantages.
Our sample was too small to enable us to compare cost of delivering supplements in campaign as compared to routine delivery. Moreover, calculating the cost of routine delivery is very difficult as supplementation is mingled with delivery of many other services. It seems quite likely that routine delivery has lower cost, but whether it is more or less cost-effective than campaign delivery depends on the coverage achieved, which varies a lot by context.
Factors inhibiting coverage include the difficulties of keeping accurate records in a country with dispersed populations with relatively low levels of literacy, workload, limited resources, and limited understanding by families of the benefits of vitamin A. Factors supporting coverage include strong organization and central direction, use of volunteers to mobilize the community, strengthening of the primary health care system, and allowing some latitude to localities in exactly how to maintain coverage, by using a hybrid approach.
Future research can benefit from understanding some of the limitations of our study—the fact that we focused on 1 region, on only 4 woredas, and that we also interviewed too few health workers and supervisors to get robust quantitative data. We did not have access to the full list of woredas in the region surveyed (those missing coverage data were not included); however, given that these may be the worst performers, it is important not to omit them. Future research can also build on the strengths of our study—the use of both quantitative and qualitative data which allowed for triangulation of findings and the decision (in the field) to include interviews with the community mobilizers (the Women’s Development Army): the mobilizers have a key role in linking the communities with the community health workers to make the health workers more effective. Further research on routine delivery will be important, as health services are strengthened and there is a transition away from vertical campaigns, in the path to universal health coverage.
Footnotes
Authors’ Note
Alison Greig conceptualized the study and obtained funding. Susan Horton and Sospeter Gatobu designed the methods, and Sospeter Gatobu led the fieldwork. Yibeltal Kiflie Aleyamehu, Negalign Birhanu, and Gelila Abraham obtained ethics approval, undertook the fieldwork, and prepared both quantitative and qualitative data. Sospeter Gatobu wrote the first draft of the qualitative analysis. Susan Horton wrote the first draft of the quantitative analysis. All authors contributed to development, review, and approval of the final manuscript.
Acknowledgments
The authors would like to thank Getu Molla from the Micronutrient Initiative in Ethiopia for facilitating the study and Girma Guadie and Simeneh Worku from Amhara region for their assistance in undertaking the fieldwork.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this research was provided by Global Affairs Canada.