
Abstract
Background:
Population exposed to chronic undernutrition in early life seems to be more susceptible to obesity in adulthood due to the development of mechanisms that improve the efficiency of energy use. Therefore, these individuals have relatively reduced energy requirements (thrifty phenotype).
Objective:
To investigate, among women living on severe socioeconomic vulnerability, whether short stature, a marker for undernutrition in early life, is associated with excess body weight but not with a high energy intake.
Methods:
This cross-sectional study, carried out between July and November 2008, evaluated 1308 women from all (N = 39) Quilombola communities of Alagoas. Adequacy of energy intake was estimated by the ratio between energetic ingestion and the estimated energy requirement (EER).
Results:
The prevalence of short stature (≤ 154.8 cm) was 43.0% and 52.4% had excess body weight (body mass index ≥ 25 kg/m2), being that 33.1% were overweight and 19.3% obese. Excess body weight was higher among women with short stature (56.6% vs 49.2%; P = .008), even after adjusting for age, energy intake, and per capita income (prevalence ratio = 1.16; 95% confidence interval = 1.04; 1.28). The ratio of energy intake/EER was independent of women’s stature.
Conclusion:
Excess body weight among Quilombola women represents a serious health problem. Short stature was significantly associated with excess body weight but not with a high energy intake. “Thrifty phenotype” may be one of the plausible explanations for this finding.
Introduction
The relationship between low socioeconomic status and health status has been well established. 1 Brazil, the fifth largest nation in the world, is characterized by a great socioeconomic disparity among its 5 geographic macroregions. The differences between the southern and northeastern regions are especially prominent. The monthly per capita income, for example, in the southern states ranges from R$1241 to R$1434, whereas in the northeast ranges from 509 to 825. 2
In 2014, Facchini et al 3 reported that the prevalence of moderate or severe food insecurity was 22.9% in northeast and 7.5% in southern Brazil. Moderate or severe food insecurity was more commonly observed among families headed by women, black or brown maternal skin color, low maternal education, low family income, and enrolled in the Bolsa Família Program (conditional income transfer).
In 1989, the prevalence of chronic undernutrition in preschool children in Alagoas, which presents the country’s worst social indicators, was more than 7 times higher than that observed in Santa Catarina (36.8% vs 4.9%). 4 As a consequence of the chronic malnutrition, the height of adults in Alagoas is below the median of Brazilian population. 5
Regardless of the region, the inequities are higher among the black population (lower salaries, professional qualification, schooling, access to public policies, and regular jobs), which characterizes a situation of greater social vulnerability. Within the black population, the members of the “Quilombola” communities represent a population contingent that stands out because it presents an even greater social vulnerability. 6
In Brazil, many of the descendants of escaped African slaves (the “Quilombolas”) who, in former times, had hidden in remote rural areas, still live in communities known as “quilombos.” Based on their historical background, specific territorial bonds, and the presumption of black ancestry linked to resistance to past oppression suffered in Brazil, these communities are considered to be a specific ethnic groups when compared to the Brazilian population in general. 7
The continual exposure of Quilombola communities to discrimination and exclusion has imposed socioeconomic conditions that place them at a greater risk of food insecurity. 8,9 Few studies have, however, focused on the nutritional and health status of these populations. 10
Evidence suggests that populations exposed to chronic undernutrition are susceptible to obesity in later life owing to the development of metabolic adaptation mechanisms aimed at increasing the efficiency of energy utilization. 11 -14 Epidemiological studies have shown that short stature that results from undernourishment in childhood is associated with an increased risk of obesity in adulthood. 13,15 -17 Therefore, it is plausible to assume that this obesity would be achieved with a caloric intake level lower than the energy requirements based on the parameters established for individuals not submitted to this “metabolic adjustment.”
The increasing prevalence of obesity in Brazil is a major public health problem, since it affects people of all classes and gender, but is proportionately higher among low-income families and particularly among women. 18 Within this context, investigations relating to the adequacies of food intake and the nutritional status of populations that are both socioeconomically and biologically vulnerable are particularly timely.
The objective of this study was to examine, in a population of Quilombola women subjected to severe socioeconomic vulnerability, whether short stature, a marker for undernutrition in early life, is associated with excess body weight but not with a high energy intake.
Methods
This cross-sectional study was part of a comprehensive project entitled “Nutritional and health diagnosis of a Quilombola population in the state of Alagoas,” which was approved by the research ethics committee of the Universidade Federal de Alagoas (process number 014440/2008-51). All participants signed the written informed consent form.
Participants
Women were eligible for the study if they met the following criteria: (1) lived in one of the 39 Quilombola communities existing in Alagoas in 2008 (according to records of the Afro-Quilombola Management Program sponsored by the Alagoas government); (2) aged between 19 and 59 years; and (3) were not pregnant or breastfeeding. As recommended by Willett, 19 women reporting 24-hour energy intake values lower than 500 kcal or greater than 4000 kcal (outliers) were excluded.
We evaluated 1405 women, and 81 women were excluded (65 reported energy intake lower than 500 kcal and 16 greater than 4000 kcal). In addition, 16 women were excluded because of missing information on weight and/or height. Therefore, the final studied population comprised 1308 participants.
Data Collection
Data were collected from July to November 2008. In order to facilitate this process, the study population was assembled in a place chosen by the community leaders, and home visits were carried out for those participants who did not attend the first round of evaluation. This strategy was important to ensure that the entire population was evaluated.
Demographic, health, and socioeconomic data, including family income, economic classification, schooling, occupation, skin color, blood pressure (BP), and number of children, were obtained from the participants.
Those women whose schooling was less than 4 years were considered as functional illiterate. Economic classification was evaluated using the Brazilian Socioeconomic Classification Criteria, 20 which is based on a score that considers achieved schooling of the head of the household, the ownership of household appliances, the presence of bathroom in the household, and housemaid. This score ranges from A (wealthier families) to E (the poorest).
Family income was estimated by adding all financial resources obtained by the family members, including salary, retirement pension, allowance, benefits from government social programs, or any other form of income to the family in the last month. Poverty was defined by a daily income per capita ≤US$1.25. 21 Skin color was self-defined, that is, the participants defined their own color/race.
Weight, height, and waist circumference (WC) were evaluated with the participants barefoot and using light clothes. Body weight was determined using a Marte (model PP180; São Paulo, Brazil) electronic scale with a maximum capacity of 180 kg and a precision of 50 g that was calibrated daily using standard weight. Height was assessed using a portable stadiometer, with the individual in orthostatic position. Waist circumference was measured at the midway between the lowest rib margin and the iliac crest, using a nonextendable tape graduated in 0.1 cm divisions.
Nutritional status was classified according to body mass index (BMI, kg/m2) using the cutoff established by the World Health Organization 22 : underweight: <18.5; normal: 18.5 to 24.9; overweight: 25.0 to 29.9; and obesity: ≥30. We also considered those participants whose BMI was ≥25 kg/m2 as having excess body weight (overweight + obesity).
Central obesity was defined according to 2 indicators: WC >80 cm and waist-to-height ratio (WHtR) > 0.5. 23 Those women whose height was ≤154.8 cm were considered as presenting short stature, which is the 10th percentile in the World Health Organization (WHO) 2007 for females at 19 years of age in the WHO growth charts. 24 A similar approach was used by other authors. 25,26
Blood pressure was assessed using Omron BP monitors (model HEM-7113, Omron Healthcare Co., Ltd., Kyoto, Japan), which were calibrated every week using mercury manometers. Blood pressure was measured twice on the right arm, after 10 minutes of resting, during the interview (in the middle and at the end) and the mean of the 2 readings was used in the data analysis. Hypertension was defined by a systolic BP >140 mm Hg and/or a diastolic BP >90 mm Hg or the intake of antihypertensive medication. 27
Food intake was evaluated with a 24-hour food recall that was completed by participants on a random day of the week. To adjust for the effect of day-to-day variation in intakes, 28 a second 24-hour food recall was applied to a subsample of the population (n = 296; 22.6%) selected randomly. In order to reduce information bias, an album containing pictures of food portions was used. 29 The nutritional composition of the diet was analyzed using Nutwin open-source software (version 1.5). Specific types of foods not included in the data bank were analyzed using tables of food composition published by (in decreasing priority order) Núcleo de Estudos e Pesquisas em Alimentação, 30 Projeto Integrado de Composição de Alimentos, 31 Philippi, 32 and Pacheco. 33
Estimated energy requirement (EER) values were calculated using an equation that predicted the total energy expenditure according to age, weight, height, and physical activity. 34 Levels of physical activity were estimated by considering the type of occupation of the participant. 35
To calculate the EER, the following formula was used 34 :
where physical activity (PA) is: PA = 1.00, when 1.0 ≤ physical activity level (PAL) < 1.4 (sedentary); PA = 1.12, when 1.4 ≤ PAL < 1.6 (low active); PA = 1.27, when 1.6 ≤ PAL < 1.9 (active); PA = 1.45, when 1.9 ≤ PAL < 2.5 (very active).
Adequacy of energy intake was determined by calculating the ratio between energetic ingestion calculated from the 24-hour food recall and EER. Values 10% or more below the EER (<0.9) were considered as low energy intake, whereas values above 1.10 as excessive energy intake. 36
Statistical Analysis
Data were entered independently in duplicate using Epi Info software version 3.5.1 (Centers for Disease Control and Prevention, Atlanta, Georgia) and analyzed using Stata 12.0 software (Stata Corp, College Station, Texas).
The variables of interest were short stature (independent variable) and overweight (dependent variable). All others variables, including energy intake/EER, were used to control possible confounding factors in the association between short stature and obesity.
Differences between proportions were tested using χ2 test. Means were compared using the nonparametric Mann-Whitney test because the variables were not normally distributed (tested with Kolmogorov-Smirnov test).
Poisson regression with robust adjustment of variance was used both in the crude and in the adjusted (multivariable) analysis to estimate the prevalence ratio (PR) and its 95% confidence interval (CI).
Results
Of the 1308 women who were enrolled in the study, 77.5% described themselves as black or brown, 52.7% were functional illiterate, 66.4% had 3 or more children, and 68.0% of the women had an income below the poverty line. None of the families were in the economic classes A and B; the majority (46.9%) belonged to class E, the poorest. More than half of women had excess body weight, 33.1% were overweight and 19.3% obese. On the other hand, the prevalence of underweight was 3.0%. Based on the WHtR, 62.3% of women had abdominal obesity. The prevalence of hypertension was 35.4%. Most of the women (64.4%) reported energy intake below their respective estimated needs (Table 1).
Characteristics of the Study Participants: Women of the Quilombolas Communities of Alagoas.
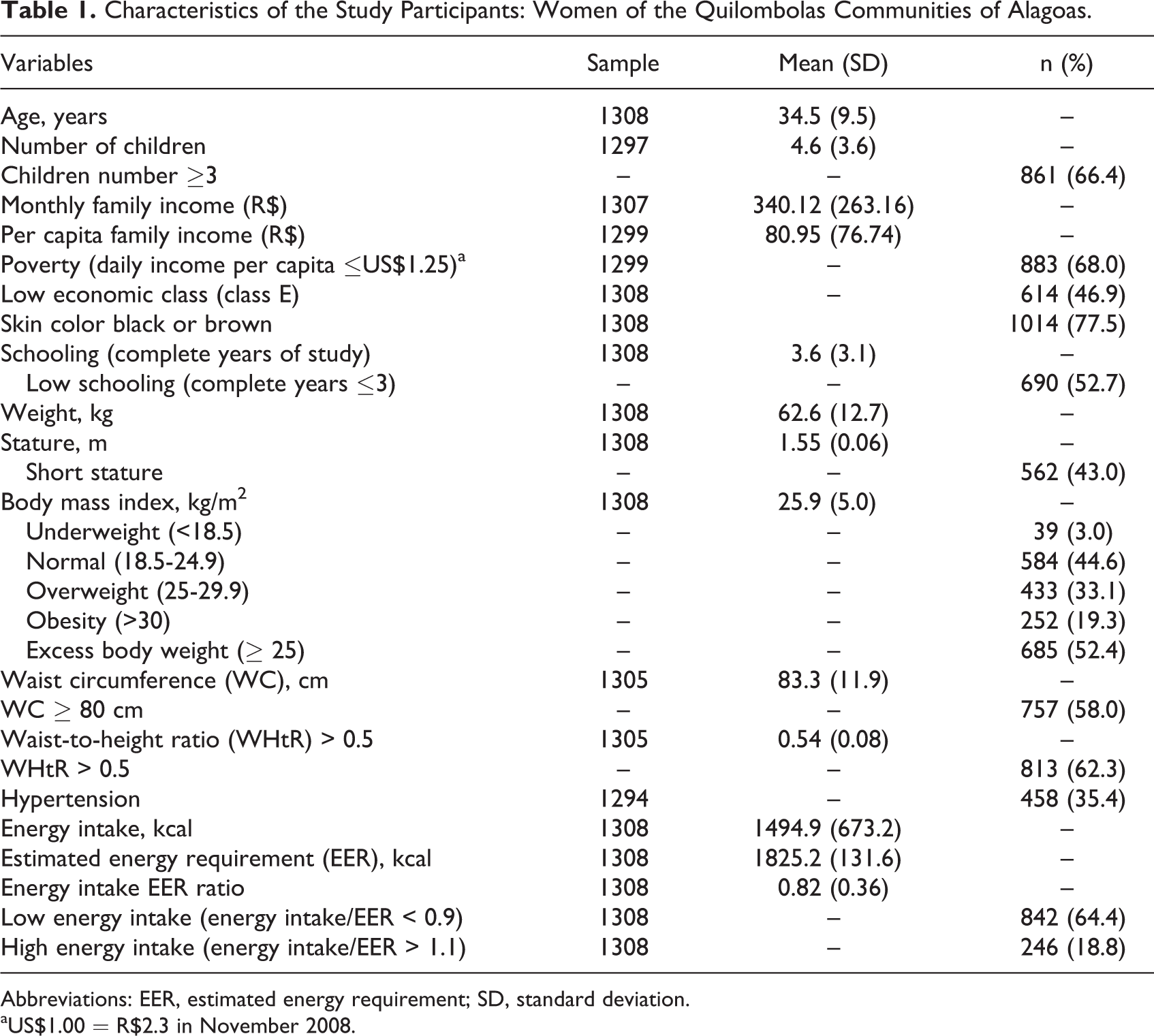
Abbreviations: EER, estimated energy requirement; SD, standard deviation.
aUS$1.00 = R$2.3 in November 2008.
The prevalence of short stature was 43.0% (n = 562). Figure 1 shows that height distribution of Quilombola women was displaced to the left in relation to the WHO 2007 reference. 24
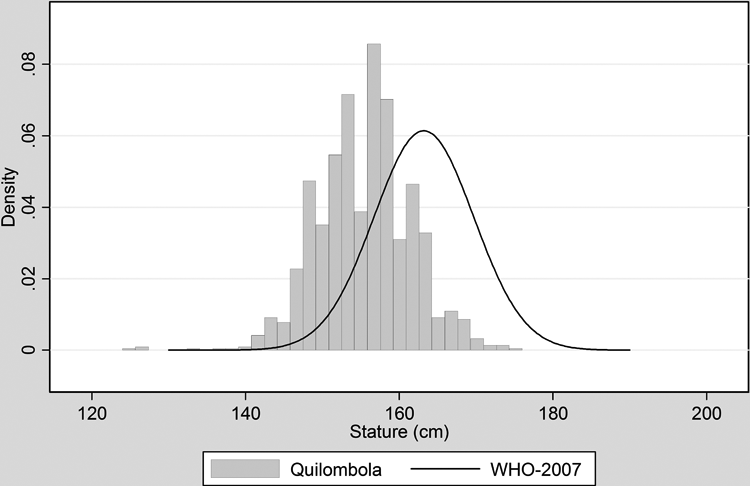
Comparison between the data of stature distribution of the study population (“Quilombola”) and the respective distribution for 19-year women of the World Health Organization (WHO) reference 2007.
Table 2 shows that women with short stature did not significantly differ from those of normal height with respect to age, total and per capita income, and WC. Furthermore, there was no difference with respect to energy intake/EER (0.83 vs 0.81; P = .31). On the other hand, women of short stature showed higher BMI (26.2 vs 25.7 kg/m2; P = .022). Short stature was also associated with a higher number of children (P < .001) and lower attained schooling (P = .0002).
Distribution of Sociodemographic and Health Characteristics (Expressed as Mean and Median) According to Stature of Women From the Quilombolas Communities of Alagoas, Brazil, 2008.
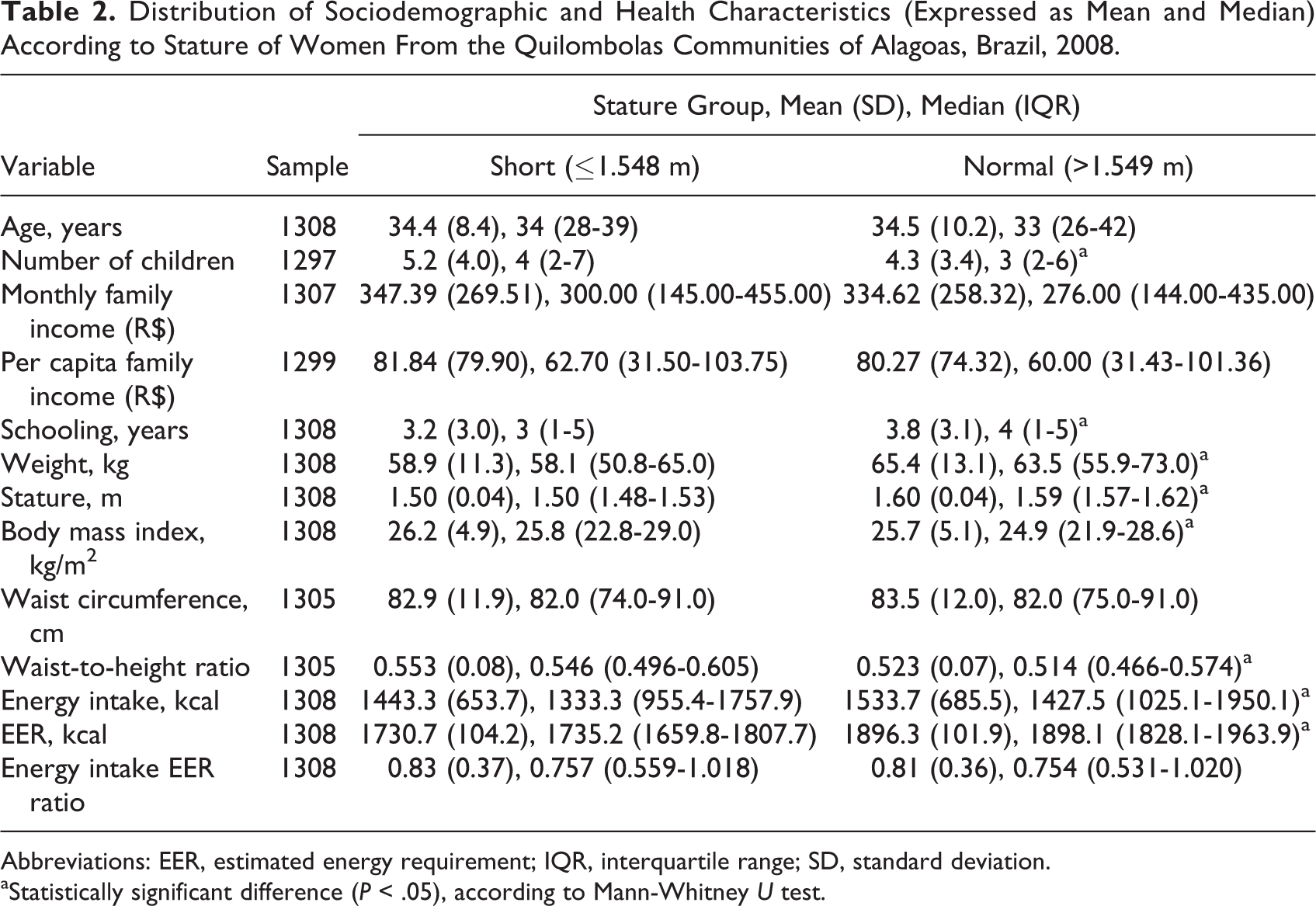
Abbreviations: EER, estimated energy requirement; IQR, interquartile range; SD, standard deviation.
aStatistically significant difference (P < .05), according to Mann-Whitney U test.
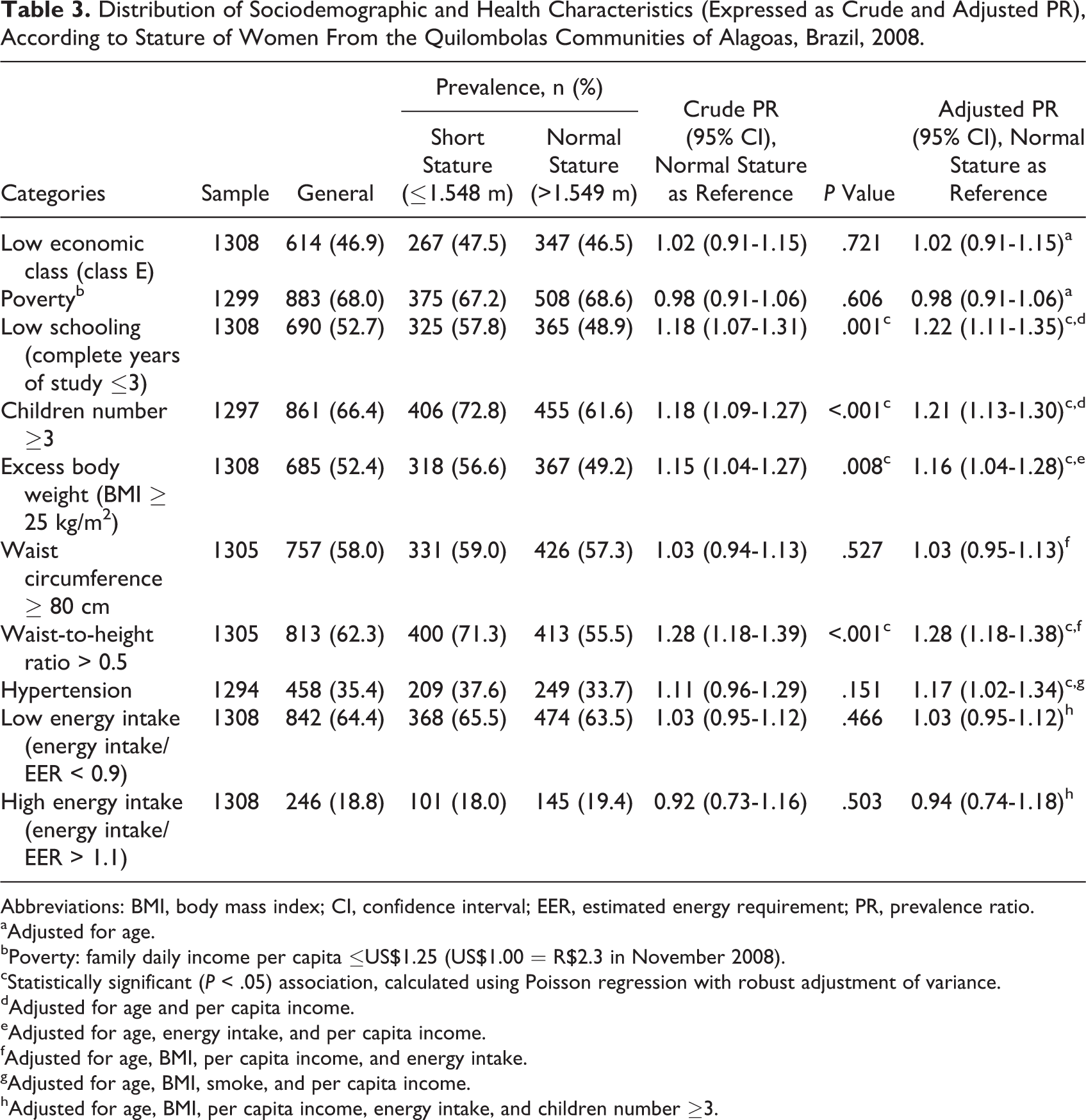
Table 3 shows that even after controlling for confounding variables, women of short stature were more likely to have 3 or less years of schooling, 3 or more children, excess body weight, WHtR >0.5, and hypertension.
Distribution of Sociodemographic and Health Characteristics (Expressed as Crude and Adjusted PR), According to Stature of Women From the Quilombolas Communities of Alagoas, Brazil, 2008.
Abbreviations: BMI, body mass index; CI, confidence interval; EER, estimated energy requirement; PR, prevalence ratio.
aAdjusted for age.
bPoverty: family daily income per capita ≤US$1.25 (US$1.00 = R$2.3 in November 2008).
cStatistically significant (P < .05) association, calculated using Poisson regression with robust adjustment of variance.
dAdjusted for age and per capita income.
eAdjusted for age, energy intake, and per capita income.
fAdjusted for age, BMI, per capita income, and energy intake.
gAdjusted for age, BMI, smoke, and per capita income.
hAdjusted for age, BMI, per capita income, energy intake, and children number ≥3.
The prevalence of hypertension was higher among women of short stature (PR = 1.17; 95% CI: 1.02-1.34), even after controlling for BMI. Excess weight was also associated with hypertension, and we observed that the prevalence of hypertension was positively associated with the BMI categories (P < .001). Central obesity defined according to WHtR was also associated with short stature (PR = 1.28; 95% CI: 1.18-1.38).
In spite of the association between excess body weight and short stature, the proportion of individuals with energy intakes higher than the energy needs was independent of stature.
Discussion
Among the 1308 women included in the present analyses, 43% had short stature. These women had a significantly higher prevalence of excess weight than women of normal height. There was no difference, however, in the ratio between energy intake and needs, suggesting that the methods of assessing the energy needs overestimate the estimates.
The observation that stunted women had greater probability of overweight/obesity is in accordance with earlier reports that nutritionally induced stunting leads to metabolic alterations, such as reduced energy requirements, increased susceptibility to the effects of fat-rich diet, reduced fat oxidation, and deficient regulation of food intake. Such adaptations would increase the risk of obesity in adulthood. 17,37 It has been hypothesized that the metabolic effects induced by chronic undernutrition during early life can give rise to a so-called “thrifty phenotype,” 11 and the EER would overestimate the energy needs of the population, since the high prevalence of short stature among the Quilombola women suggests that they have been chronically exposed to undernutrition. Therefore, in order to improve the accuracy of EER, it is important to determine the specific energy requirements of populations that have been exposed to chronic undernutrition in early life.
Energy intake and expenditure were estimated using indirect methods, subject to underestimation, as mentioned above. However, previous studies of our group using more precise methods such as direct weighing of food, in case of energy intake, or doubly labeled water, to estimate energy expenditure, found similar results. 13,17 This work differs from previous by being the first to address a population of African ancestry, descendants of slaves, living in specific communities to maintain their cultural traditions and characterized by greater socioeconomic vulnerability. Therefore, the previously obtained conclusions are extended to this particular ethnic group. This is important because it is recognized the possibility that different ethnic groups may differ in body composition and health risks. 38
The historical exposure of Quilombola communities to discrimination and exclusion 8 explains the poor socioeconomic status of the studied population. The majority of women (97.3%) were in economic classes D or E. This proportion was slightly higher than that reported for women living in the semiarid region of Alagoas state 39 (87.3%) and well above the reported for the Brazilian population 40 (26.6%).
Despite the precarious economic circumstances of the Quilombola population, excess body weight (52.4%) was the most prevalent nutritional problem among the studied women. On the other hand, it is important to stress that this prevalence was similar to that reported for women of the country as a whole (48.0%), women in northeastern Brazil 18 (46.0%), and also for women of the semiarid regions of the states of Alagoas 15 (45.2%) and Ceará 41 (48.7%).
Some studies have reported that obesity is higher among women from lower socioeconomic status. 42,43 Aguirré 44 has stated that this association would be related to low quality diet, inadequate access to food, inappropriate choice of dietary constituents, sedentary life style, and an undervalued perception of the body.
The accumulation of fat in the abdominal region is a known cardiovascular risk factor. 27 The higher prevalence of the WHtR seems to explain, at least in part, the higher prevalence of hypertension among stunted women.
However, there was no difference between the groups when abdominal obesity was defined by a WC >80 cm. According to Ashwell et al, 45 based on a systematic review of 31 studies, WHtR was significantly better than WC for detecting hypertension. The authors argue that height has usually been shown to have inverse associations with cardiometabolic morbidity and this is probably because height can also reflect general early life exposures. Then, WC alone is unsatisfactory because people with the same WC but with different statures might have different cardiometabolic risk.
Although the Quilombola community survives under precarious socioeconomic conditions, the prevalence of excess of body weight represents a serious health problem. The “thrifty phenotype” induced by undernutrition during early life may represent a plausible explanation for the fact that women of short stature were more susceptible to overweight/obesity, even after adjusting for energy intake.
Therefore, the association between low stature and overweight/obesity is the main expression of the anthropometric profile of this population, characterized by a significant proportion of women shorter than 155 cm and BMI above 25 kg/m2, a situation that should be considered by public health managers, given the greater susceptibility of these women to chronic diseases in general. 11
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Edital MCT/CNPq 15/2007—Universal (processo 478607/2007-5).