
Abstract
Background:
Severe acute malnutrition (SAM) is a salient health problem in India. Federation of Indian Chamber of Commerce and Industry (FICCI) Research and Analysis Centre, New Delhi, prepared nutreal equivalent to ready-to-use therapeutic food by World Health Organization (WHO) for the management of SAM and defined food like homemade diet.
Objective:
To compare acceptability and efficacy of nutreal over defined food for the management of SAM.
Methods:
One hundred twelve children aged less than 5 years with SAM were enrolled as per the standard of WHO. Children were randomized into 2 groups to receive nutreal (n = 56) and defined food (n = 56) in unlimited amounts for 42 consecutive days and extended by 2 weeks as per demand. Calorie and protein intake, weight, and mid-upper arm circumference (MUAC) were recorded daily.
Results:
Age range was 8 to 45 months. Ninety-three percent of children eagerly accepted nutreal but 7% does not. Whereas in the defined food group, 68% accepted eagerly, 30% did not accept eagerly, and 1.8% accepted poorly (P = .004). At enrollment, mean weight in the nutreal group was 6.44 ± 1.60 kg and in the defined food group was 8.69 ± 1.76 kg, with MUAC in the nutreal group being 11.12 ± 0.47 cm and in the defined food group being 11.54 ± 0.34 cm. Mean weight in the nutreal and defined food groups at eighth week of intervention was 7.97 ± 1.8 kg and 9.71 ± 1.8 kg (P < .001), respectively. Mid-upper arm circumference at eighth week was 12.10 ± 0.29 cm in the nutreal group and 12.49 ± 0.50 cm in the defined group (P < .001).
Conclusion:
Acceptability, mean weight gain, and MUAC in the nutreal group are greater than the defined food.
Keywords
Introduction
Severe acute malnutrition (SAM) occurs primarily due to deficiency of calories and proteins in the diet of young children. Six percent of children have this nutritional problem in India. Severe acute malnutrition is associated with high morbidity and mortality in children younger than 5 years. A large number of children having SAM cannot be managed in hospitals. Uncomplicated SAM in children can be managed with calorie-dense, protein-rich, and vitamin- and mineral-fortified food provided at home under supervision. This can avoid the burden of the hospitals to manage SAM effectively at home. Children with SAM are prone to diarrhea, pneumonia, and other systemic infections. It is estimated that 1.6 million children die of SAM in India annually. A homemade diet is not effective because of preparation of food, storage, and feeding practices under poor hygienic and sanitation conditions. The overfeeding, underfeeding, dilution factors, and infections are the main hindrances in treating SAM. 1,2
The World Health Organization (WHO) recommended ready-to-use therapeutic food (RUTF) for the treatment of SAM. This food is rich in calories, proteins, vitamins, and minerals and comes in properly sterilized packets and can be kept at room temperature and has a shelf life of 2 years. It can be directly fed to the children without reconstitution and addition of water. Ready-to-use therapeutic food has been used to manage SAM children in South Africa and is very effective in relation to other comparative foods used. 3,4 It has been found to be effective when used to manage SAM children in India. 5 There are 132 million children younger than 5 years in India, of which around 8 million children are having SAM. Hence, there is a need of indigenously produced RUTF equivalent to RUTF recommended by WHO. It should be effective, safe, and easily available. 1 –3
Federation of Indian Chamber of Commerce and Industry (FICCI) Research and Analysis Centre, New Delhi, prepared food called nutreal equivalent to RUTF by WHO and defined food equivalent to homemade food prepared under sterile and proper hygienic conditions. The Lok Manya Tilak Municipal Hospital, Mumbai, has prepared RUTF in their own kitchen and trial was done in hospital itself. Presently used RUTF has been produced by FICCI. To prepare nutreal, all precautions have been taken including stabilization at room temperature, microorganism-free, proper airtight package, and having a shelf life of 1 year. The study was done in slums and not in hospital. Nutreal is locally produced, Indianized food rich in calories, proteins, vitamins, and minerals and its nutritive value is equal to RUTF by WHO. Whereas defined food is based on cereals, pulses, and sugar prepared by FICCI similar to a homemade diet. We planned a preliminary study to see the acceptance and efficacy of nutreal and defined food among SAM children in slums of tricity Chandigarh, Panchkula, and Mohali, North India.
Objectives
To study the acceptability and efficacy of Indianized locally produced RUTF, that is, nutreal, in comparison with defined food for the nutritional management of SAM in the community.
Methods
Participants
One hundred twelve children aged less than 5 years with SAM, defined by weight for height (WHZ) <−3 standard deviation (SD), with no evidence of infection or edema, were participated.
Setting
Study was carried out in slums of tricity Chandigarh, Panchkula, and Mohali, North India.
Study Period
This study was conducted from August 01, 2013, to March 30, 2014.
Staff Recruited
Two nutritionists, 2 anthropometrist, 3 technical assistants, 3 lady health visitors, and 4 other helpers were recruited.
Criteria
Inclusion criteria
Children in the age group of 6 months to 60 months having SAM with WHZ <−3 SD and mid-upper arm circumference (MUAC) <11.5 cm or visible severe wasting.
Exclusion criteria
Children with localized infections, diarrhea, or systemic infections.
Inability to accept oral feed.
Oral lesions and congenital malformations.
Children with pedal edema.
Consent
Informed consent was obtained from parents before enrollment.
Ethical Clearance
As per the ethical principles for medical research involving human participants in accordance with the World Medical Association Declaration of Helsinki, autonomy of the participants was maintained and direct intervention for the therapy of SAM was undertaken with secondary beneficial effects by creating public awareness about nutrition, hygiene, and sanitation for the prevention of SAM. The principle of nonmalfeasance was reflected in this study. Regarding the use of nutreal as a nutrient energy paste for the management of SAM, the ethical clearance was taken from Food Safety and Standards Authority of India (FSSAI) Ministry of Health and Family Welfare, Government of India (product registration number: 15025/783/2012-PA/FSSAI, trial number: FRAC/Nufl/01).
Enrollment
One thousand eight hundred household survey done in slums revealed that 122 children aged less than 5 years were having SAM. Thorough clinical examination of these children was done. None of these children had obvious evidence of infection. They were weighed on the electronic digital weighing scale (Equinox, Mansarovar Garden, New Delhi) with a sensitivity of 10 g. The height or length and MUAC were measured with a tape with a sensitivity of 0.1 cm. The WHO child growth standards were defined by using WHZ z score, and <−3 SD was taken to define SAM.
One hundred twenty-two children were selected to participate in the study. However, there were 10 dropouts: 2 were sick, 5 were migrants, and 3 refused to be the part of this study. The remaining 112 children having uncomplicated SAM were divided into 2 groups of 56 each by simple randomization. The first group was given nutreal and the second group received defined food as the primary food. The scheme of the study is given in Figure 1. Daily weighed nutreal food and defined food were given to the children under the supervision of nutritionists and lady health visitors.
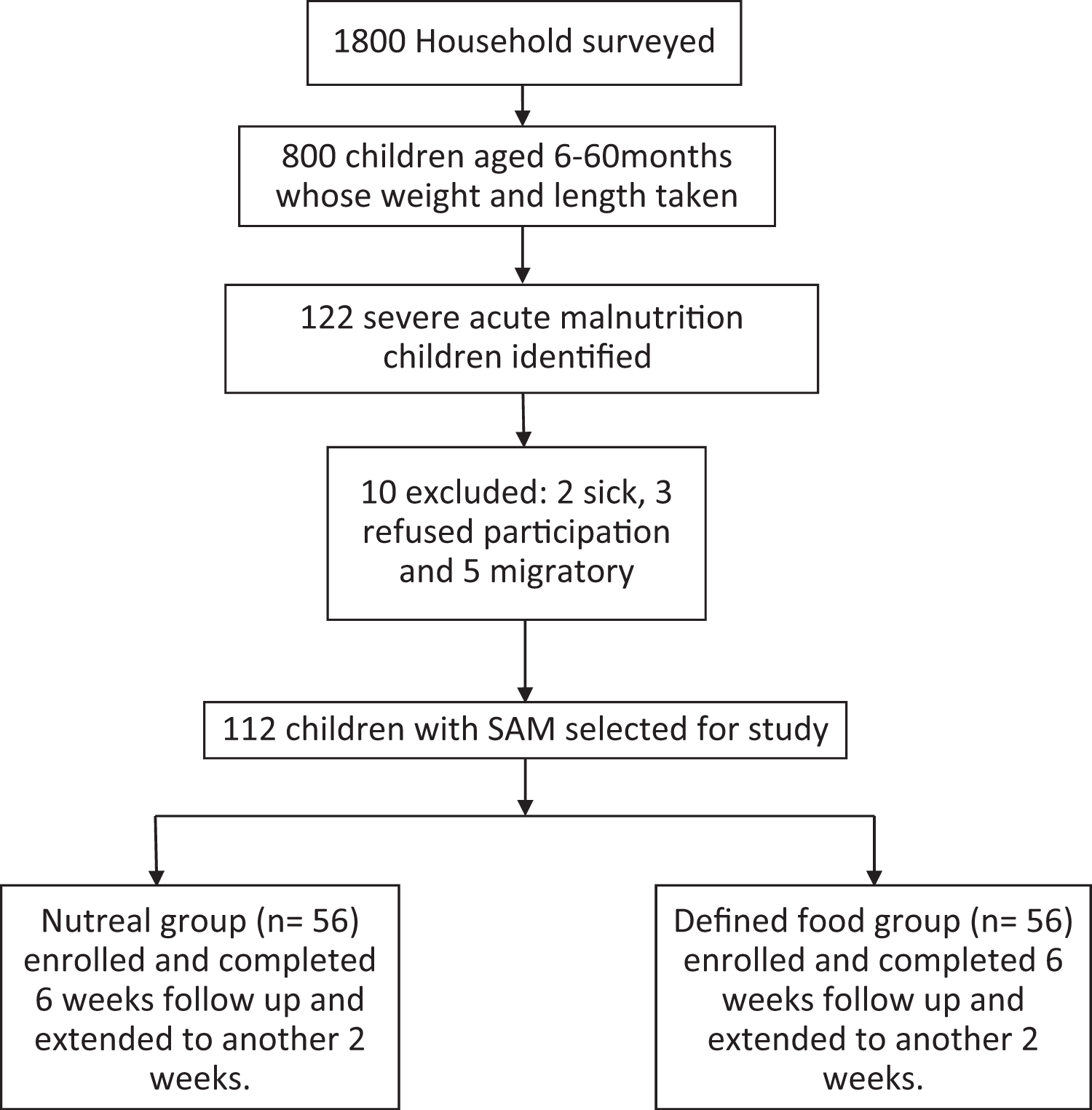
Scheme of the study.
Pretesting
To familiarize the nutreal and defined food to mothers and caregivers and children, a pretest was done for 2 days and 6 feeds were given as per WHO recommendations. The children liked the food and had successfully passed the appetite test as per the criteria given by WHO. 2
What is Nutreal?
Nutreal is a nutrient energy homogenous paste prepared by FICCI Research and Analysis Centre, New Delhi. Nutreal is prepared with roasted peanuts, milk powder, vegetable oil, sugar, and adequate minerals and vitamins mixture. It is prepared under strict hygienic and sterile conditions and is stored in sterile packets which can be kept at room temperature. The shelf life of nutreal is 365 days. Cost of nutreal is INR 23 per packet. This is much cheaper than other RUTF products. The composition and its nutrient value are equivalent to RUTF recommended by WHO. The composition and nutritional value of nutreal and RUTF are given in Tables 1 and 2.
Composition of Nutreal and RUTF by WHO.
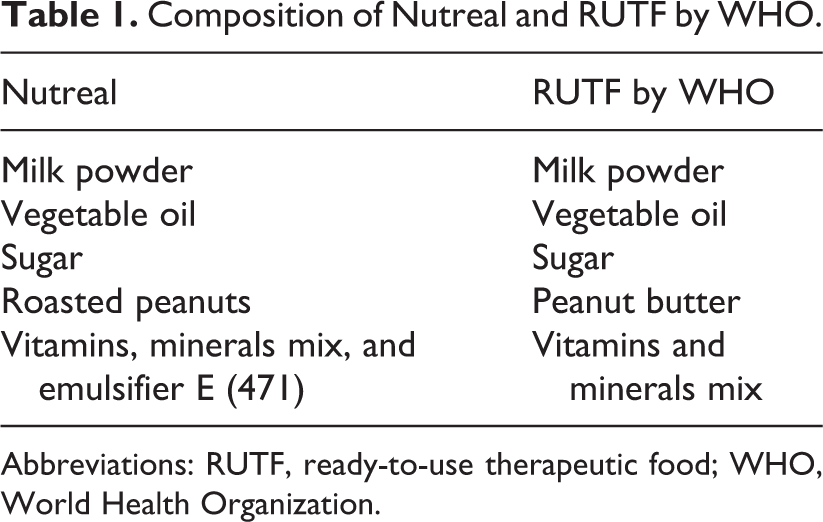
Abbreviations: RUTF, ready-to-use therapeutic food; WHO, World Health Organization.
Nutritional Value of Nutreal and RUTF (WHO) per 100 g.
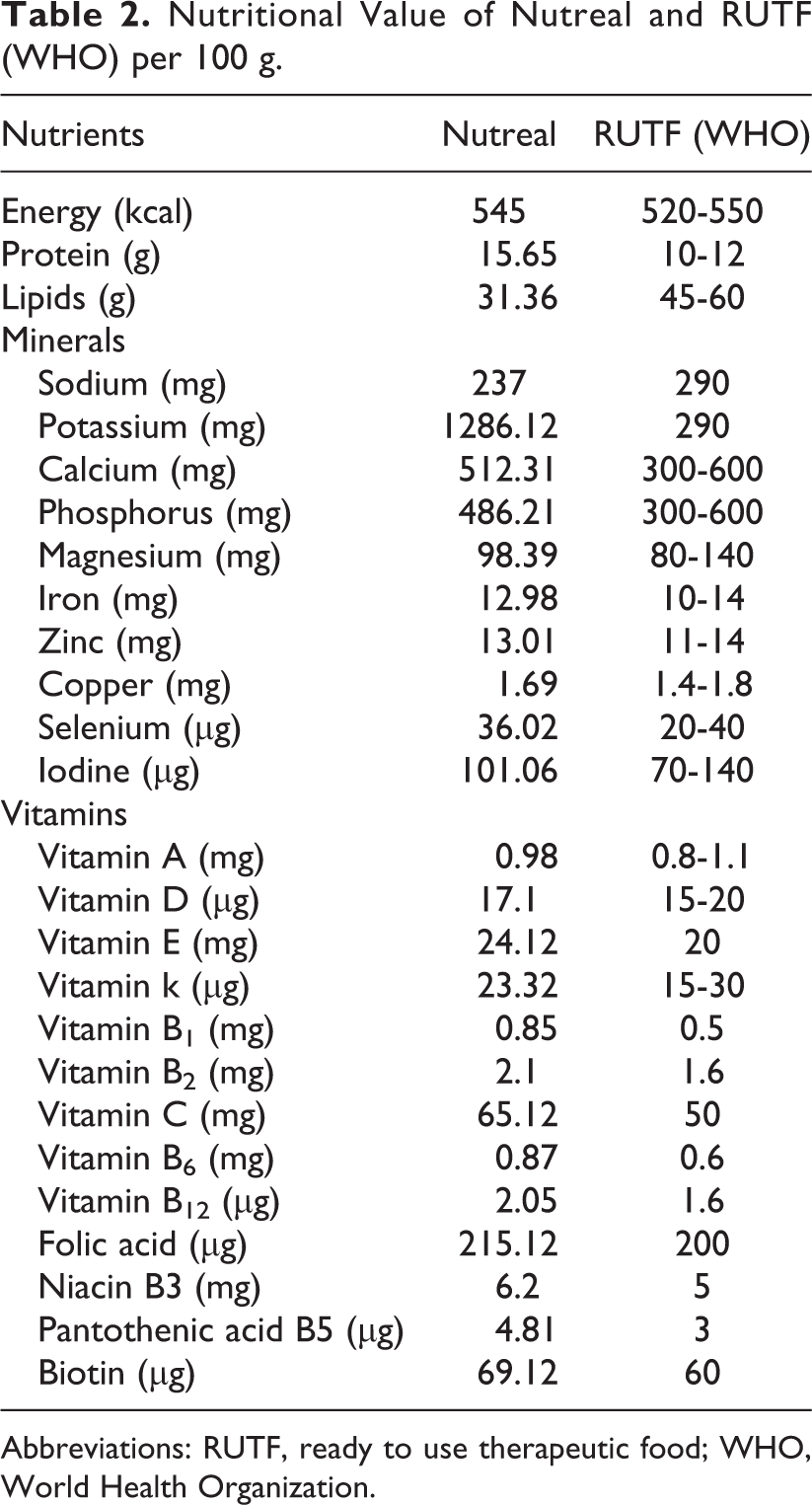
Abbreviations: RUTF, ready to use therapeutic food; WHO, World Health Organization.
What is Defined Food?
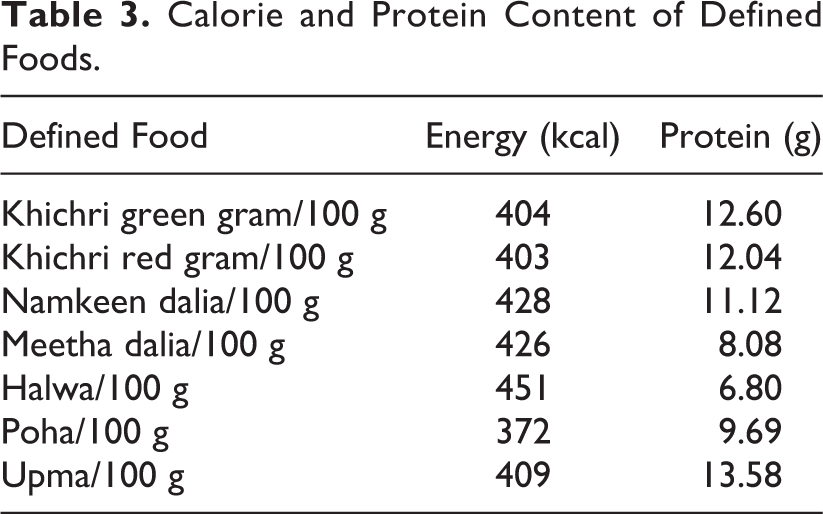
Defined food is again prepared by FICCI and contains cereals, pulses, and oil, and the composition and nutritional values of each food are given in Table 3. The food is precooked and packed in sterile packets. The shelf life of defined food is 3 months from the date of manufacturing. Defined foods used in the present study are precooked foods in the form of khichri (green gram + rice, red gram + rice + vegetable oil + salt), namkeen dalia (broken wheat + soya grits + vegetable oil + salt) and sweet dalia (semolina + soya grits + sugar + vegetable oil), halwa (semolina + soya grits + sugar + vegetable oil), poha (rice flakes + soya grits + groundnuts + dry peas + vegetable oil+ salt) and upma (semolina + soya grits + Bengal gram + vegetable oil + salt).
Calorie and Protein Content of Defined Foods.
Intervention
Before the start of the study, all recruited staff members were trained regarding documentation of anthropometry, use of nutreal as sole diet, preparation of a precooked defined food, use of clean water in between the feeds, proper hygiene, number of feeds per day, and observations made by the mothers during the study period. They were also instructed to guide the mothers and caregivers regarding the cooking of defined food, the schedule of feeding, and method of feeding under strict clean and hygienic conditions.
Children were offered intervention foods (nutreal and defined food) 6 times on each day with 2 to 3 hours gap in between meals. A lady helper on each day helped in cooking of preweighed defined food before serving to the children. Defined food was cooked in clean water and no other ingredients were added. Thickness of the food was always kept regarding the age and acceptability by the child. It was also ensured that 2 namkeen (salty) and 1 sweet food were given alternatively. A different type of menu was followed daily to break the monotony in the defined food group. Hygiene was well maintained while preparing the defined food; however, nutreal was given directly from the packet with a clean spoon. Mothers were instructed to feed their children as much as they can eat over half an hour. Clean plain water was also given in between the meals. Mothers were asked not to feed the child any other foods during the interval between the feeds. Nutritionists weighed the amount of food taken daily by the children both in the nutreal and defined food group. Once the meal time was over, the leftover foods were weighed again, and the amount of food consumed daily in grams was estimated and recorded. Prior to commencing meals on the second day, each child was again examined for local and systemic infections. Intake of calories and protein was calculated from the amount of food consumed everyday throughout the study period.
The daily weight of children was measured to the nearest of 10 g by the anthropometrists. Weight was fluctuating during the first week of intervention, and thereafter, steady weight gain was observed. The intervention foods were continued for 6 weeks. Since these were liked by the children, these were extended for 2 weeks more. The taste of nutreal was especially liked by the children. Daily observations regarding untoward effects, weight gain, acceptability, and rejection were recorded on a structured questionnaire by nutritionists.
Statistical Analysis
Mann-Whitney U test, χ2 test, and t test were used for analysis of variables. Data were expressed as mean ± SD. SPSS software was used (version 17). P value less than .05 was considered statistically significant.
Results
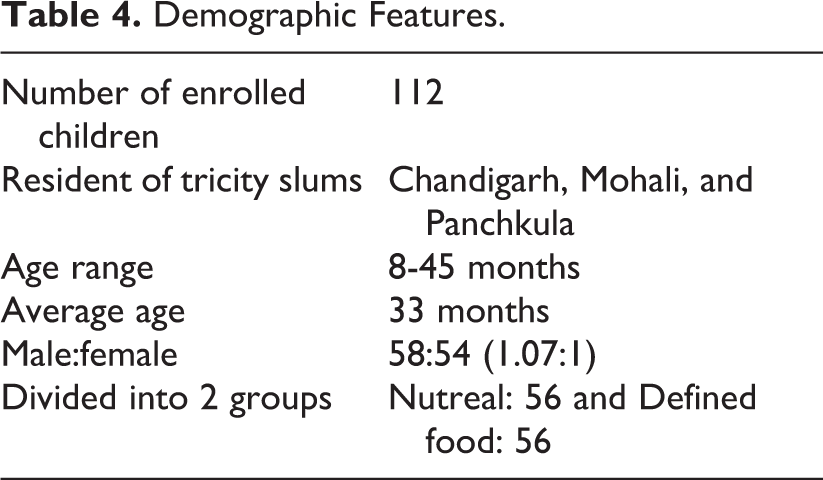
The demographic features are given in Table 4. The age range of children was 8 to 45 months (average: 33 months), and male:female ratio was almost equal in both the groups. The mean age of children in the nutreal food and defined food groups was 25.1 and 32.9 months, respectively.
Demographic Features.
Acceptability of Intervention Foods
The acceptance of intervention food by the children was categorized as below: Eagerly accepted: Children who ate food readily and who did not make a fuss, spit out, vomit out, cry, spillage or grimaced, and smacked the lips during the observed meal. Not eagerly accepted: Children who ate the offered food but made fuss, spit out, or vomit out during the observed meal. Poorly accepted: Children who did not eat food readily and made a fuss, spit out, vomit out, cry, spillage, or grimaced.
The acceptability of intervention foods is given in Table 5. It was better with nutreal as compared to defined food.
Acceptability of Intervention Foods.a
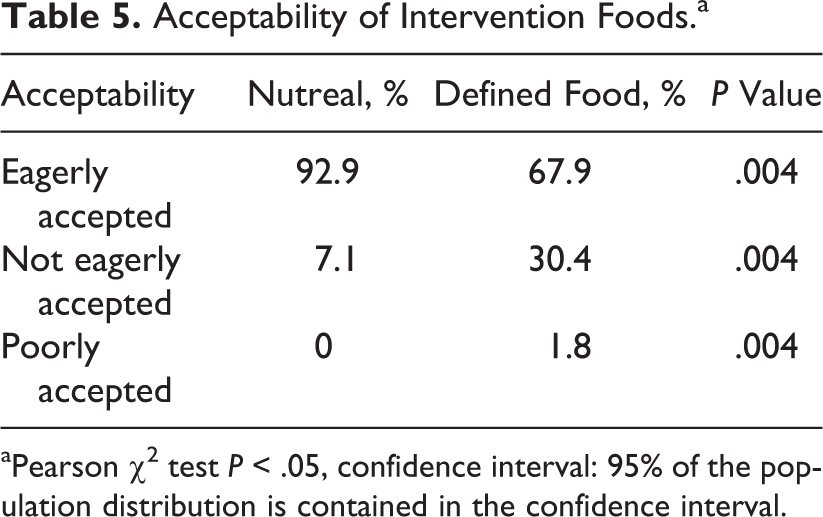
aPearson χ2 test P < .05, confidence interval: 95% of the population distribution is contained in the confidence interval.
Protein and Calorie Intake
Intake of protein and calories from nutreal and defined food per day over 1 week duration is given in Table 6.
Intake of Nutreal and Defined Food per Day Over 1 Week.a
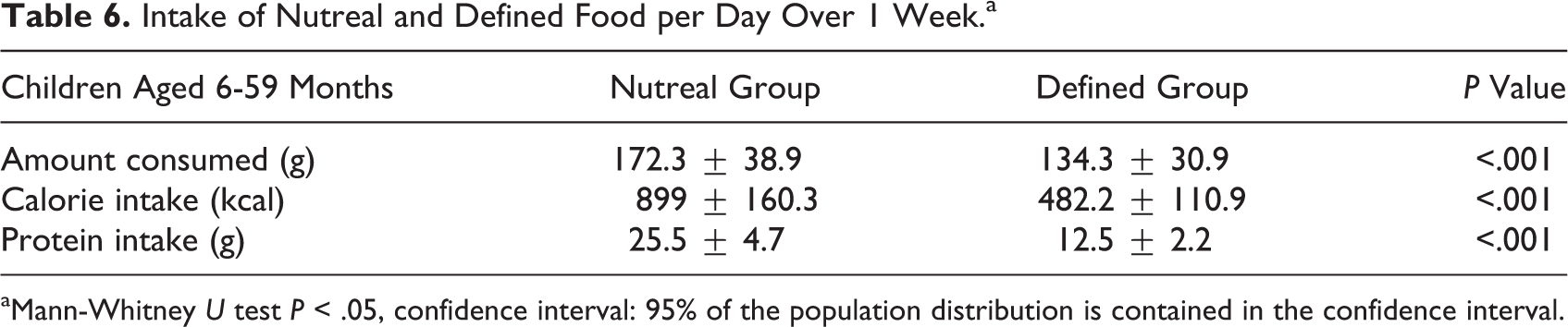
aMann-Whitney U test P < .05, confidence interval: 95% of the population distribution is contained in the confidence interval.
Weight Gain and MUAC
There were fluctuations in weight gain during the first week, but subsequently, steady weight gain was observed and documented. After starting therapeutic food, there may be weight gain or weight loss. Weight gain is usually due to refeeding syndrome, which was not noticed in our study. However, weight loss is expected and this could be the reason for fluctuation in weight during the first week due to loss of extracellular fluid volume.
There was a definite increase in weight in both the groups at second, sixth, and eighth week of intake of intervention foods as given in Table 7, which was more significantly observed in the nutreal group. The MUAC was also found to be more increased in the nutreal group in comparison with the defined food group at sixth and eighth week as given in Table 8.
Anthropometric Measurements During Second, Sixth, and Eighth Weeks.a
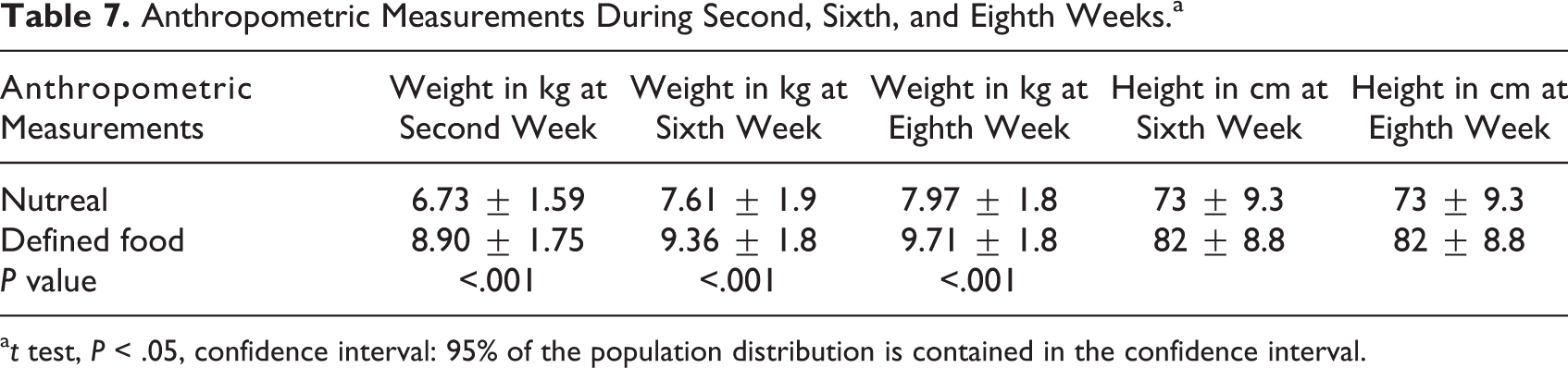
a t test, P < .05, confidence interval: 95% of the population distribution is contained in the confidence interval.
MUAC During Sixth and Eighth Weeks.
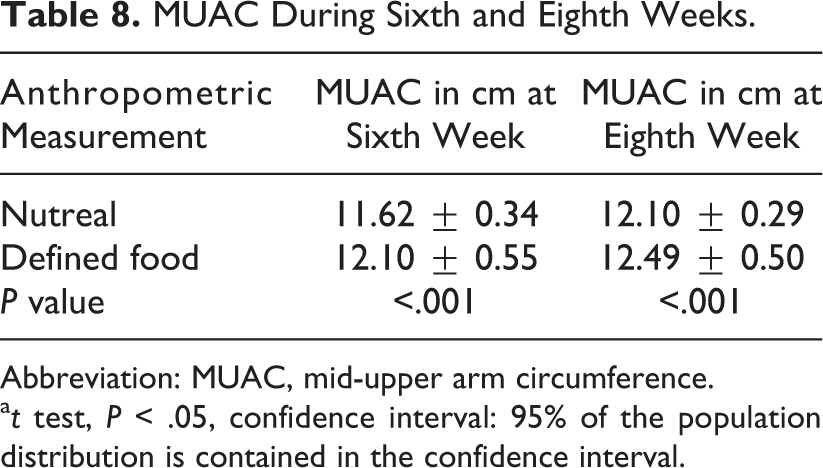
Abbreviation: MUAC, mid-upper arm circumference.
a t test, P < .05, confidence interval: 95% of the population distribution is contained in the confidence interval.
Intervention foods were better tolerated by children. However, nutreal was eagerly accepted by children who ate food readily, did not make a fuss, spit out, vomit or cry, spillage, grimaced, and smacked the lips during the observed meal (92.9%) as compared to acceptance of defined food (67.9%). No adverse effects were documented in the nutreal group, whereas 3 children in the defined food group had acute diarrhea that settled with conventional therapy without administration of antibiotics. Overall, nutreal was well tolerated by the children, and the taste was also more appreciated. Average duration of rehabilitation was 8 weeks, at the end of which all of the children except 4 became moderate acute malnutrition in the nutreal group. However these children were not followed up further.
Observations
Nutreal was liked by the children and parents were also satisfied to feed the children since they were demanding more. There were no untoward effects noted in the nutreal group, whereas in the defined food group, 3 children had diarrhea that settled with conventional treatment, and the defined food was continued. None of the children had refeeding syndrome in the form of edema.
Discussion
Nutreal is an Indianized RUTF and has been used to treat SAM for the first time in India. It is prepared by FICCI and has been used to treat SAM successfully for the first time in Indian slums. This is a first preliminary study when nutreal has been compared with defined food. Nutreal is a therapeutic food and its composition and nutritional values are almost similar to that of RUTF recommended by WHO. Ready-to-use therapeutic food has been used widely to treat SAM at home and has been shown to be very effective to improve the health of uncomplicated SAM children faster than homemade foods. Homemade foods have limitations in terms of composition, ingredients, methods of cooking, and feeding under unhygienic conditions. Moreover, social, cultural, and ethnic factors, poverty, and illiteracy also affect the dietary intake by young children. 1 –3 Defined foods used in the present study are precooked foods composed of cereals, pulses, soya grits, vegetable oil, sugar, and salt as given under Methods. These foods are prepared by FICCI, India, under hygienic and sterile conditions and then semicooked foods are packed in airtight packets and are similar to homemade food for young children in India. Before feeding, the precooked food is cooked properly in clean water under hygienic conditions, keeping in mind the thickness according to the age and acceptability by the child. Nutreal is prepared from roasted peanuts, milk powder, sugar, vegetable oil, vitamins, minerals, and E (471) under sterile conditions (Table 1).
The present study, comparing nutreal and defined foods, was carried out in SAM children in slums of tricity Chandigarh, Mohali, and Panchkula, in North India. One hundred twelve children who had uncomplicated SAM in the age of 8 months to 45 months were chosen for study. These were divided into 2 groups, those taking nutreal and those taking defined foods. The acceptance of nutreal was better than the defined foods. Ninety three percent of children accepted nutreal eagerly as compared to defined foods (68%). The nutreal in the paste form was liked by the children, and weight gain was more (23 g/d) in comparison with defined food (14 g/d) group. Moreover, the nutreal can be fed directly without mixing anything or cooking.
The acceptance and efficacy of nutreal is consistent with the RUTF recommended by WHO. 2,3 In a study by Dube et al, RUTF and Khichri were used in SAM children from New Delhi, India. 5 Severe acute malnutrition children with RUTF showed weight gain, liked its taste, and their results are similar to the present study.
Studies done in a large cohort of Malawian children having SAM where locally produced ready-to-use food was compared with maize/soya food and RUTF with standard therapy. 6 –8 The results were better with locally designed ready-to-use food and RUTF groups as we have seen in the present community-based study with locally produced nutreal as compared to defined food. In a study from Senegal, authors used locally produced ready-to-use food in solid form comparing with F 75 and F 100 foods, and the results were akin to the present study. 9 In Ethiopian SAM, locally made ready-to-use food also showed similar results as we have seen. 10 Weight gain and better acceptability were observed as compared to homemade diet. Authors from Niger have reported the preventive effects of RUTF in the prevention of morbidity and mortality. 11 There are 2 short reports from our country where locally made ready-to-use food on short-term basis was found to be effective to manage SAM. 12,13 The study published recently from India is of a different kind where eeZeePaste prepared by Norwegian company has been used. In that study, the authors have brought in new criteria and also included patients with complications who required hospitalization in stabilization centers. 14
However, in the present study, the nutreal, an RUTF, is used that comes in packets with shelf life of 365 days and can be kept at room temperature, whereas the RUTF by WHO has a shelf life of 730 days and can be kept at room temperature. World Health Organization has recommended that solid RUTF should be ideally used for the treatment of SAM in slum settings where hygiene and sanitation is a big problem.
The observations made by us during the study period were SAM children accepted nutreal eagerly and showed weight gain. As it was liked by children and was demanded more, the study was extended for 2 weeks more. Initially, there were fluctuations in the weight of children over the first week of intervention, but after the first week, steady weight gain was observed, which was superior in the nutreal cohort as compared to the defined food cohort. None of the children in the nutreal group poorly accepted the food. Children were smacking their lips and demanded more so were given liberally to their satisfaction. Mothers and caregivers also liked the nutreal as it did not require cooking and mixing and was fed directly and hence it was easy to feed as compared to defined food. Three children in the defined food group developed self-limiting diarrhea that was attributed to contamination, whereas none had in the nutreal group. There was no evidence of refeeding syndrome in both the groups.
Limitations
The present interventional study was only for 8 weeks and the patients were not followed up. The number of participants was small, and this question warrants a larger prospective study.
Conclusion
To conclude, indigenously produced nutreal equivalent to RUTF recommended by WHO was well accepted. It was easy to feed children directly, and there was weight gain in comparison with defined food, which was in precooked form and before feeding required proper cooking. The calories, protein, vitamin, and mineral content of nutreal are near to that of RUTF by WHO. The shelf life of nutreal is 365 days and can be kept at room temperature. Hence, there is need for large-scale production of nutreal at cheaper rate in our country to take care of the colossal problem of uncomplicated SAM at home. We have 8 million children having SAM and around 1.6 million children die annually in our country. So it is of utmost important to prevent, detect, and treat SAM effectively.
We need to study nutreal further in a large cohort of uncomplicated SAM children in community. Those children who are attending hospitals can also be treated with nutreal on outpatient basis at home under supervision and can regularly be followed in the hospital regarding the acceptability and documentation of weight gain and onset of any infections or other complications like refeeding syndrome. The nutritional management of uncomplicated SAM in children can also prevent further complications and hence curtail morbidity and mortality due to SAM.
Footnotes
Acknowledgments
The authors are grateful to Akshat Khandelwal, Director of Nuflower Foods and Nutrition Private Limited Company, to help us to conduct the study. URL: ![]() . The authors would also like to thank Sunita Shriwal, Ankush Thakur, Hoor Bano, and Neha Thakur for helping in collecting the data and Kusum for analyzing the data.
. The authors would also like to thank Sunita Shriwal, Ankush Thakur, Hoor Bano, and Neha Thakur for helping in collecting the data and Kusum for analyzing the data.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Nuflower Food Private Limited in association with FICCI Research Analysis Centre, New Delhi, India.