
Abstract
Background:
The impact of food-based interventions on child and maternal anthropometry and anemia has not been adequately studied.
Objective:
This study tested the effect of an enhanced homestead food production (EHFP) program consisting of home garden, poultry raising, and nutrition education implemented over 2.5 years versus control (no intervention) on anthropometry and anemia among children (12-48 months) and their mothers.
Methods:
An unblinded cluster-randomized controlled trial involving pre- and post-surveys with independent samples was conducted in rural areas of Baitadi District, Nepal. Data (including weight, height/length, and hemoglobin) were obtained from 2106 and 2614 mother–child pairs at baseline and follow-up, respectively. Changes in outcome variables (stunting, underweight, wasting, and anemia among children and underweight and anemia among mothers) were compared between the study groups using mixed-effects logistic regression models.
Results:
At follow-up, anemia was significantly lower among children (odds ratio, OR [95% confidence interval, CI]: 0.76 [0.59-0.98]) and mothers (OR [95% CI]: 0.62 [0.48-0.82]) in the treatment group compared to the control. Underweight was lower among mothers in the treatment group compared to the control (OR [95% CI]: 0.61 [0.46-0.82]). There was no impact on child anthropometry.
Conclusion:
The EHFP intervention improved anemia among children aged 12 to 48 months and their mothers in Baitadi District of Nepal. The intervention also reduced underweight among these women, but had no impact on child growth, in this district.
Introduction
Nepal is among the 34 countries that account for 90% of the global burden of maternal and child malnutrition. 1 Nationally, 18% of reproductive-age women are underweight (body mass index [BMI] < 18.5 kg/m2), while 41% of preschool children are stunted (height/length-for-age Z score [HAZ] <−2), 11% are wasted (weight-for-height Z score [WHZ] <−2), and 29% are underweight (weight-for-age Z score [WAZ] <−2). In addition, 35% of reproductive-age women and 46% of children aged 6 to 59 months are anemic. 2 Among the identified factors associated with child and maternal malnutrition are inadequate quality and quantity of foods consumed, poor feeding practices, frequent infections, low parental education, and inadequate access to and use of public health services. 2,3
There is a growing global interest in examining the impact of food-based interventions on the immediate, underlying and basic determinants of malnutrition. Compelling evidence has indicated that homestead food production programs increase the quantity and variety of foods produced and consumed by families. 4 -7 However, these results are inconclusive as to whether such approaches improve overall dietary quality or simply increase the intake of specific food items. A homestead food production program in Vietnam that supported households to raise gardens to produce carotene-rich fruits and vegetables, and provided nutrition education to mothers of preschool children, found a significant improvement in the intake of both micronutrients (vitamin A and iron) and macronutrients (energy and protein) among women and children in participating families. 8 However, a similar program in South Africa found no impact on macronutrient intake, despite improvements in intakes of vitamin A, riboflavin, vitamin B6, and ascorbic acid among children 2 to 5 years old. 9 Participation in the Vietnam program also reduced the incidence of respiratory infections and diarrhea among children. 8 There is also suggestive but inconclusive evidence that combining home garden interventions with household animal (particularly, poultry and aquaculture) production and consumption can improve child nutritional status. 10 Some of these programs have also demonstrated improvement in nutritional knowledge of women and their involvement in household decision-making. 5,11 -14 Nevertheless, the evidence base for the benefit of homestead food production programs on nutritional status of women and children remains inconsistent. The strongest findings to date are improvements in vitamin A status (either by increased serum retinol or reduction in clinical signs of vitamin A deficiency such as nightblindness) among women and children, resulting from these programs. 11 -13,15,16 Some studies have also shown reduction in anemia among women and children, 13,14 although others found no impact. 17 To our knowledge, no study has reported an association between homestead food production programs and anthropometry of women, and the existing evidence suggest that these programs have no impact on child anthropometry. 11,16 -21 The prevailing consensus is that the lack of consistent association between homestead food production programs and the nutritional status of children and women is largely due to weakness in the program and impact evaluation design, targeting, and implementation, as well as complexity of the pathways by which these programs influence nutritional outcomes. 4 -6
The objectives of this study was to test the impact of an enhanced homestead food production (EHFP) program, consisting of home garden, poultry raising, and nutrition behavior change communication, on the prevalence of stunting, underweight, wasting, and anemia among young children and underweight and anemia among women.
Methods
Study Area and the EHFP Intervention
The study was conducted in Baitadi District, a remote hilly community in the far western region of Nepal. The study area and the EHFP intervention are described briefly by Osei et al. 22 The district comprised 12 Ilakas, or subdistricts, each of which is further divided into village development committees (VDCs) that represent several wards or villages (∼9 per VDC).
The EHFP program was implemented from 2009 to 2012 and was expected to improve nutritional outcomes of mothers and children aged 0 to 23 months through several hypothesized pathways (Figure 1). Before starting the intervention, a detailed project planning process was organized, which brought together all the implementing partners to discuss its design and successful rollout. This included workshops in Kathmandu (the capital city) to garner government support and inputs of other technical experts in refining the methods and tools for the implementation, followed by briefings in all the intervention villages (including meetings with village leaders) to gain their commitment and support. Following this, 1 woman per group of intervention villages (∼5 to 6) was selected and trained by Helen Keller International (HKI) in improved gardening and poultry rearing practices in preparation to host a village model farm (VMF). Under the guidance of HKI, this woman then trained 20 other beneficiary women on how to establish their home gardens and poultry production. Altogether, the project intended to establish 120 VMFs, each of which served as a site for purchasing inputs and ongoing training for all the beneficiary women. For every season (rainy and winter) of the first year, each woman was given a 1-time free supply of seeds, saplings, and locally bred chicks to establish their home gardens and poultry production. Vegetables and fruits promoted in the program included kangkong (Ipomea aquatica), amaranth, carrots, spinach, bitter gourd, bottle gourd, orange-fleshed sweet potato, papaya, and mango. Throughout the period of the intervention, the women met monthly at the VMF to refresh lessons on agriculture techniques and nutrition through social and behavior change communications, such as optimal infant and young child feeding (IYCF) practices, cooking demonstrations on how to use the EHFP produce to enrich family meals, and participation in routine public health services (immunization, growth monitoring, vitamin A supplementation, and deworming) offered in their communities. The intervention activities were jointly monitored through monthly home visits by trained project staff, female community health volunteers, and agriculture extension officers. During each home visit, the project staff and agriculture extension officers observed the home gardens and poultry, including the number of different varieties of crops cultivated, whether the garden was fenced, how many of poultry birds the family had, whether the poultry had started laying eggs, and so on, and provided advice on any garden or poultry issues the family was facing. On these home visits, the project staff and the female community health volunteers also reinforced the educational messages on breastfeeding and complementary feeding to all mothers.
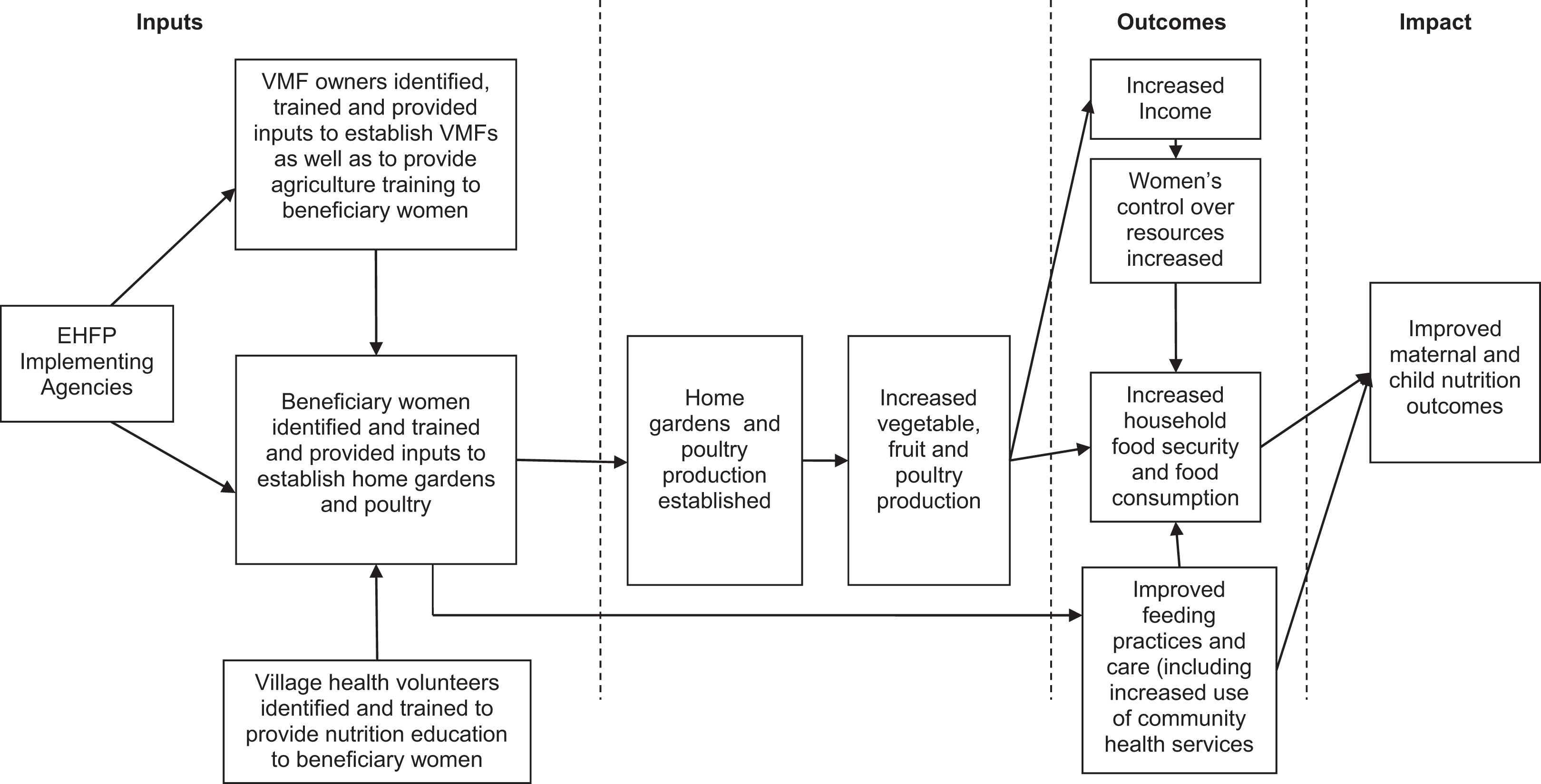
Hypothesized pathways by which the EHFP intervention is expected to improve maternal and child nutritional outcomes. EHFP indicates enhanced homestead food production; VMF, village model farm.
Research Design
This was a prospective, nonblinded, multistage cluster-randomized controlled study. Families with children aged 0 to 23 months in 1 group of communities received the EHFP intervention (treatment group) and those in another group did not (control group). Approval for the study was granted by the National Health Research Council in Nepal.
To minimize spillover of the intervention activities into control communities, we assigned Ilakas (instead of villages or households) into each of the 2 study groups. Ilakas were paired on several key socioeconomic indicators, and 4 of the generated 6 pairs of Ilakas were selected for inclusion in the study using a simple random sampling procedure. 22 The same procedure was followed to assign 1 Ilaka in each pair as the treatment group and the other as the control. Overall, there were 21 and 20 VDCs in the treatment and control Ilakas, respectively (Figure 2).
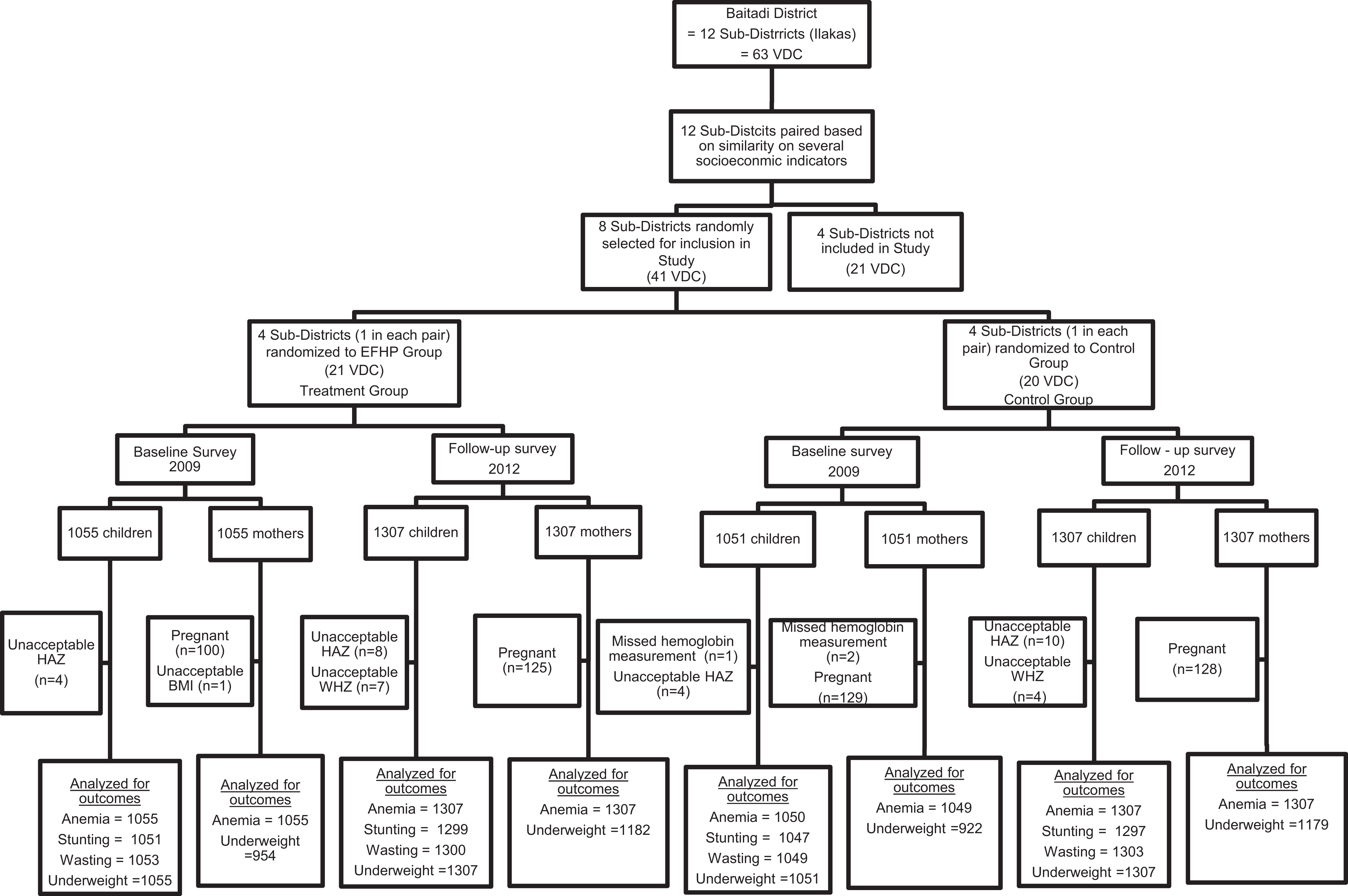
Trial profile. BMI indicates body mass index; EHFP, enhanced homestead food production; HAZ, height/length-for-age Z score; VDCs, village development committees; WHZ, weight-for-height Z score.
We conducted pre- and postsurveys with independent samples in the treatment and control communities during the rainy season (June to September/October), which is also the lean season in the district. The baseline survey was conducted in August 2009 and involved 2106 families with children aged 12 to 48 months (treatment = 1055 and control = 1051), and the follow-up survey was conducted in August/September 2012 among 2614 of such families (treatment = 1307 and control = 1307). Although the EHFP intervention aimed to influence the nutritional and health outcomes of children aged 0 to 23 months, the evaluation sampled children aged 12 to 48 months on the basis that by the end of 4 years, the children in our follow-up survey sample would have consumed the produce from the home garden and poultry for at least 6 months (from 6 months of age when complementary feeding begins to 12 months of age).
Sample Size and Sampling Procedure
Sample size was calculated to detect an assumed difference in the prevalence of stunting and underweight of 10% as well as a difference in wasting of 5% among children in the treatment compared to the control communities. Using a power of 0.80, a 95% confidence interval (CI; 2 sided), an assumed design effect of 2, and an upward adjustment of 10% to account for loss to follow-up, a total of 1970 children were considered adequate for each of the pre- and posttreatment surveys. The baseline sample was increased to 2106 to allow enough participants for a substudy, which involved providing micronutrient powders to a subsample of children (n = 110) in the intervention communities for a period of 6 months (results published elsewhere). 22 The follow-up sample was also increased to 2614 to allow sufficient participants for disaggregated analysis.
To select families for the pre- and postsurveys, VDCs were stratified by treatment (n = 21) or control group (n = 20), and 14 VDCs were selected from each using a simple random sampling procedure to participate in the surveys. However, all the VDCs in the EHFP program communities received the EHFP intervention, regardless of their participation in the surveys. Within each selected VDC, households were selected using the probability proportional to size technique, and in each selected household, a child aged 12 to 48 months was chosen together with his/her mother for the assessments. If a household had more than 1 eligible child, the youngest child was chosen.
Data Collected
Similar structured precoded questionnaires were used at the pre- and post-treatment surveys to obtain information from the child’s mother or principal caretaker. Data collected included sociodemographic characteristics of the families, their participation in homestead food production activities, infections suffered by the child in the 2 weeks before each survey, immunizations received, vitamin A supplementation and deworming in the 6 months before the interviews, and participation in growth monitoring and promotion (GMP) in their communities. Maternal antenatal visits, iron–folic acid (IFA) supplementation, and deworming during previous pregnancy were also assessed. Information on breastfeeding and complementary feeding practices was obtained from all the mothers with children aged 12 to 23 months in the sample (n = 750 at baseline and n = 943 at follow-up) and computed into composite IYCF indicators in accordance with the World Health Organization (WHO) guidelines, 23 except exclusive breastfeeding, which were obtained only from the mothers who had additional child aged 0 to 6 months (n = 203 at baseline and n = 230 at follow-up).
We created a household wealth index from several socioeconomic status variables using principal component analysis and following similar procedures as Vyas and Kumaranayake. 24 Variables included were the household’s main source of income, source of drinking water, type of toilet facility, presence of electricity, and ownership of durable assets including radio, phone, television, refrigerator, fan, clock/watch, and furniture (bed and cupboard), as well as selected livestock (buffalo, sheep, and goats). The gender of the head of household, type of fuel used in the house, and ownership of land, motorcycle, bicycle/rickshaw, car/truck, pigs, and other livestock were excluded from the wealth index because of their limited variation in the sample. Households were divided into terciles based on the wealth index. Household food insecurity was assessed using the Household Food Insecurity Access Scale developed by the Food and Nutrition Technical Assistance project. 25
Anthropometric and Hemoglobin Measurements
Weight and height/length of all the children (12-48 months old) and their mothers were measured using standardized techniques. 26 WAZ, HAZ, and WHZ of children were calculated using the 2006 WHO growth reference values. 27 Children were classified as stunted (HAZ <−2), underweight (WAZ < −2), and wasted (WHZ < −2). Body mass index of nonpregnant mothers was computed as weight (kg)/(height [m]),2 and they were classified as underweight (BMI < 18.5 kg/m2) or not (BMI ≥ 18.5 kg/m2). 28 Hemoglobin of each child and mother was measured from a finger prick of blood using a HemoCue analyzer (Ängelholm, Sweden). Anemia was defined using altitude-adjusted hemoglobin concentration <110 g/L for children, <120 g/L for nonpregnant, and <110 g/L for pregnant mothers. 29 The altitude of households in the baseline and follow-up samples ranged from 579 to 2302 m, as measured using a handheld global positioning device (model-eTrex, Vista HCx, Garmin).
Data Analysis
Data were entered, cleaned, and analyzed for descriptives using SPSS version 20.0 (IBM, New York). STATA version 11.0 (StataCorp LP, Texas) was used for comparing proportions and for multivariate analysis. All analyses were adjusted for the clustered design by including both VDC and wards as covariates in SPSS or using the svyset command in STATA with VDC as the strata variable. Statistical significance was accepted at P <.05. The impact of the EHFP intervention was assessed in accordance with the hypothesized pathways by which it was expected to influence the outcomes of interest (Figure 1). The primary outcomes of interest were stunting, underweight, wasting, hemoglobin concentration, and anemia among children and hemoglobin concentration, anemia, and underweight among their mothers. First, we assessed household’s engagement in the activities promoted in the intervention, followed by assessing the intervention’s effect on intermediary outcomes including household food insecurity and maternal practices related to breastfeeding, complementary feeding, handwashing, antenatal visits, IFA supplementation and deworming during pregnancy, as well as children’s immunizations, vitamin A supplementation, deworming, and participation in GMP. Besides the impact on maternal breastfeeding and complementary feeding practices that are presented in this article, results on the other intermediary outcomes are presented in Supplemental Tables 1 and 2.
Bivariate comparisons between the treatment and control groups were first made separately for the pre- and posttreatment samples using Rao and Scott χ2 tests for proportions, simple linear regressions for means, and Wilcoxon tests for medians. Multivariate linear and logistic regressions were also used for the bivariate comparisons of the continuous and binary variables between pre- and posttreatment samples within each group, respectively. The difference in these variables between the pre- and post-treatment samples was compared between the groups using multiple linear regressions for means and mixed-effects logistic regressions for proportions, following policy analysis with pooled cross-sectional data as described by Wooldridge. 30
Altitude-adjusted hemoglobin concentration was compared among the groups. Comparison of maternal hemoglobin concentrations was further adjusted for their pregnancy status at the time of the survey. The age of the mother was included in bivariate and multivariate analyses that compared hemoglobin concentration, anemia, BMI, and underweight. The age and sex of children were included in all analyses with child-level variables as outcomes, except for bivariate comparisons of child anthropometric indicators. Multiple regression models comparing the 2 groups on the difference in outcomes between the pre- and postintervention samples included variables that were significantly different between the treatment and control groups at baseline and which were unlikely to have been influenced by the intervention. These included household size, sex and marital status of the household head, caste of families, categorized as “upper” (Brahmin, Chetri, Giri, or Thakuri) or “lower”(Dalit, Janajatis, disadvantaged non-Dalit Terai caste and religious minorities), mother’s education (categorized “no formal education” or “at least primary education”), parity (categorized “<3” or “≥3” children), and pregnancy status at the time of the survey.
Results
Figure 2 shows the trial profile. Of the 2106 mother–child pairs in the baseline sample, 1 child and 2 mothers missed hemoglobin measurements; 8 and 4 children had implausible HAZ and WHZ values, respectively, and 1 mother had implausible BMI (<12.0 kg/m2). These participants were therefore excluded from the analysis involving these outcomes. In addition, 10.9% of the mothers (treatment = 100 and control = 129) were pregnant at baseline and were excluded from maternal BMI and underweight analysis. For the 2614 mother–child pairs assessed at follow-up, 18 and 11 children had implausible HAZ and WHZ values, respectively, and 9.7% mothers (treatment = 125 and control = 128) were pregnant. These participants were excluded from the analysis involving the respective outcome variables.
Sociodemographic Characteristics of the Sample
In both surveys, the treatment and control groups did not differ on several characteristics including sex of children, maternal age, and marital status, as well as ownership of land by households in the sample (Table 1). However, the baseline treatment sample had significantly more pregnant women, lower maternal parity, larger family size, and a lower proportion of male-headed households than the control, although these characteristics did not differ between the groups at follow-up. Whereas the mean ± standard deviation (SD) age of children was similar among the 2 groups at baseline, children in the treatment group were significantly older than those in the control group at follow-up. Other characteristics that were similar among the study groups at baseline but differed significantly at follow-up included the proportion of households with no monthly cash income and those with some financial debts at the time of the surveys. Both surveys showed significantly fewer mothers with no formal education, mothers who worked outside the home, and proportion of families with married household heads, in the upper caste and lower tercile of wealth among the treatment compared to the control group (Table 1).
Demographic Characteristics of the Children and Women in the Baseline and Postintervention Samples in the Treatment and Control Communities.a
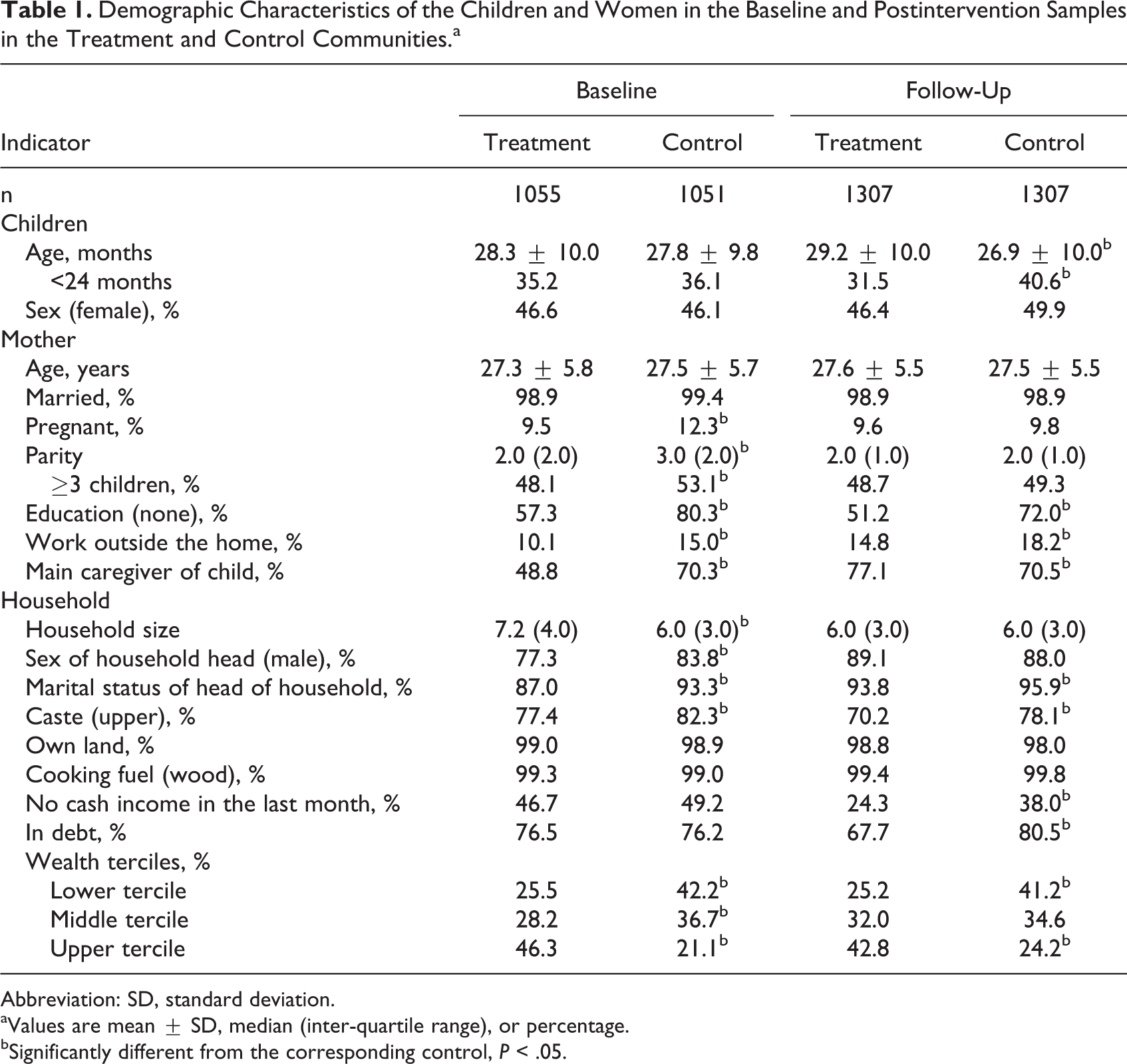
Abbreviation: SD, standard deviation.
aValues are mean ± SD, median (inter-quartile range), or percentage.
bSignificantly different from the corresponding control, P < .05.
Household’s Engagement in Homestead Food Production and Household Food Security Status
Overall, 122 VMFs were established across the treatment district, more than 100% of what the project planned to establish. At baseline, less than half (44.8%) of the treatment households had any homestead food production activity (either home garden, poultry, or both) compared to over half (51.0%) of the control households (P < .05; Table 2). However, at postintervention, a significantly higher proportion of the treatment households (97.6%) were engaged in any such activity compared to the control households (80.2%). Furthermore, the proportion of households that owned both home garden and poultry (the combined intervention promoted in this study) was similar among the 2 groups at baseline but significantly higher in the treatment (29.1%) compared to the control group (16.6%) at follow-up (Table 2).
Households Engaged in Homestead Food Production Activities and Household Food Insecurity Status at Baseline and Postintervention in the Treatment and Control Communities.a
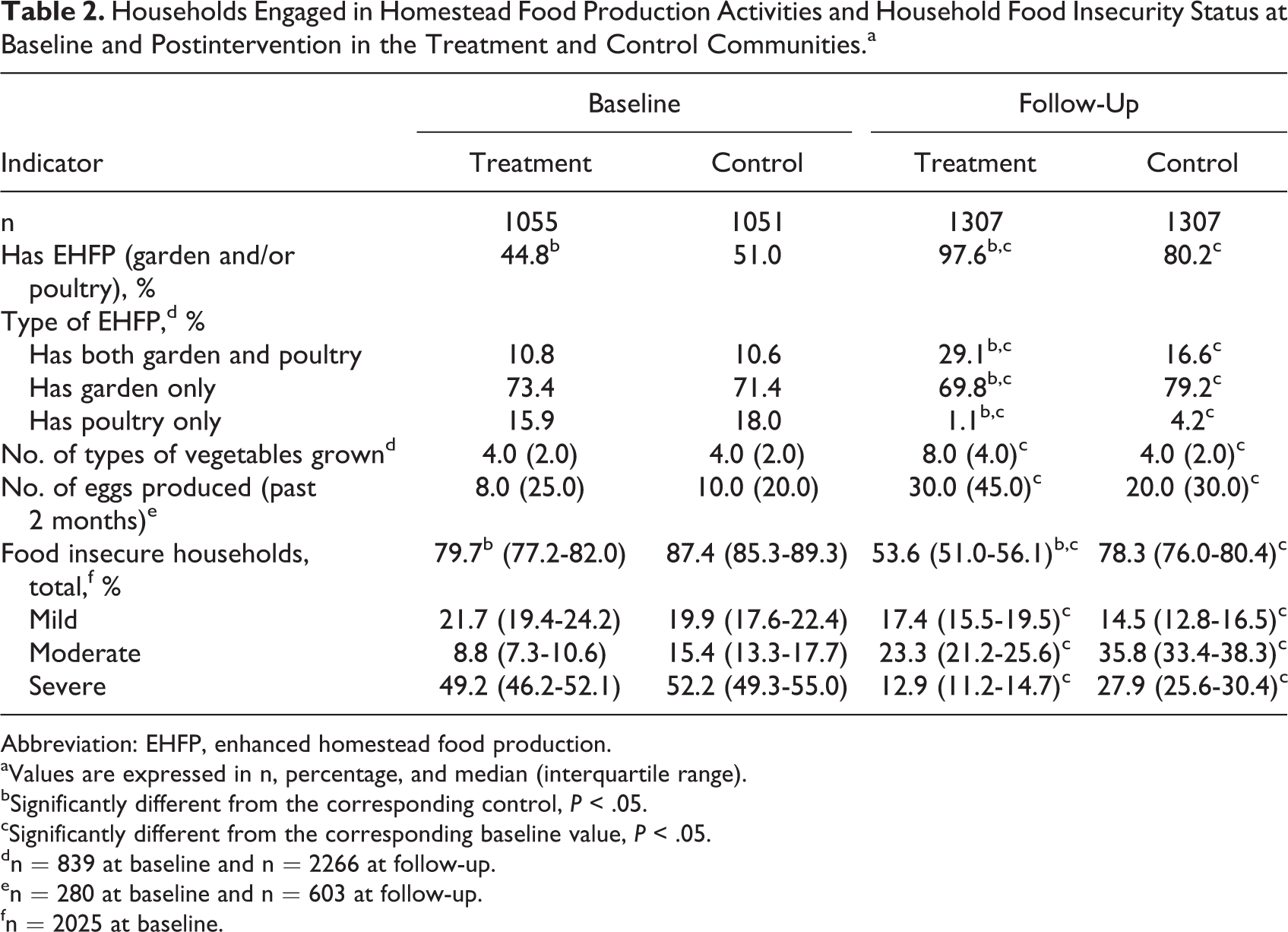
Abbreviation: EHFP, enhanced homestead food production.
aValues are expressed in n, percentage, and median (interquartile range).
bSignificantly different from the corresponding control, P < .05.
cSignificantly different from the corresponding baseline value, P < .05.
dn = 839 at baseline and n = 2266 at follow-up.
en = 280 at baseline and n = 603 at follow-up.
fn = 2025 at baseline.
The prevalence of household food insecurity was lower at follow-up compared to baseline in both the treatment (53.6% vs 79.7%) and control (78.3% vs 87.4%) groups (P < .05). Although the treatment households were less food insecure compared to the control households at baseline, the difference in food insecurity between the pre- and postintervention samples was greater among the treatment group than the control group (Table 2).
Impact on Maternal Breastfeeding and Complementary Feeding Practices
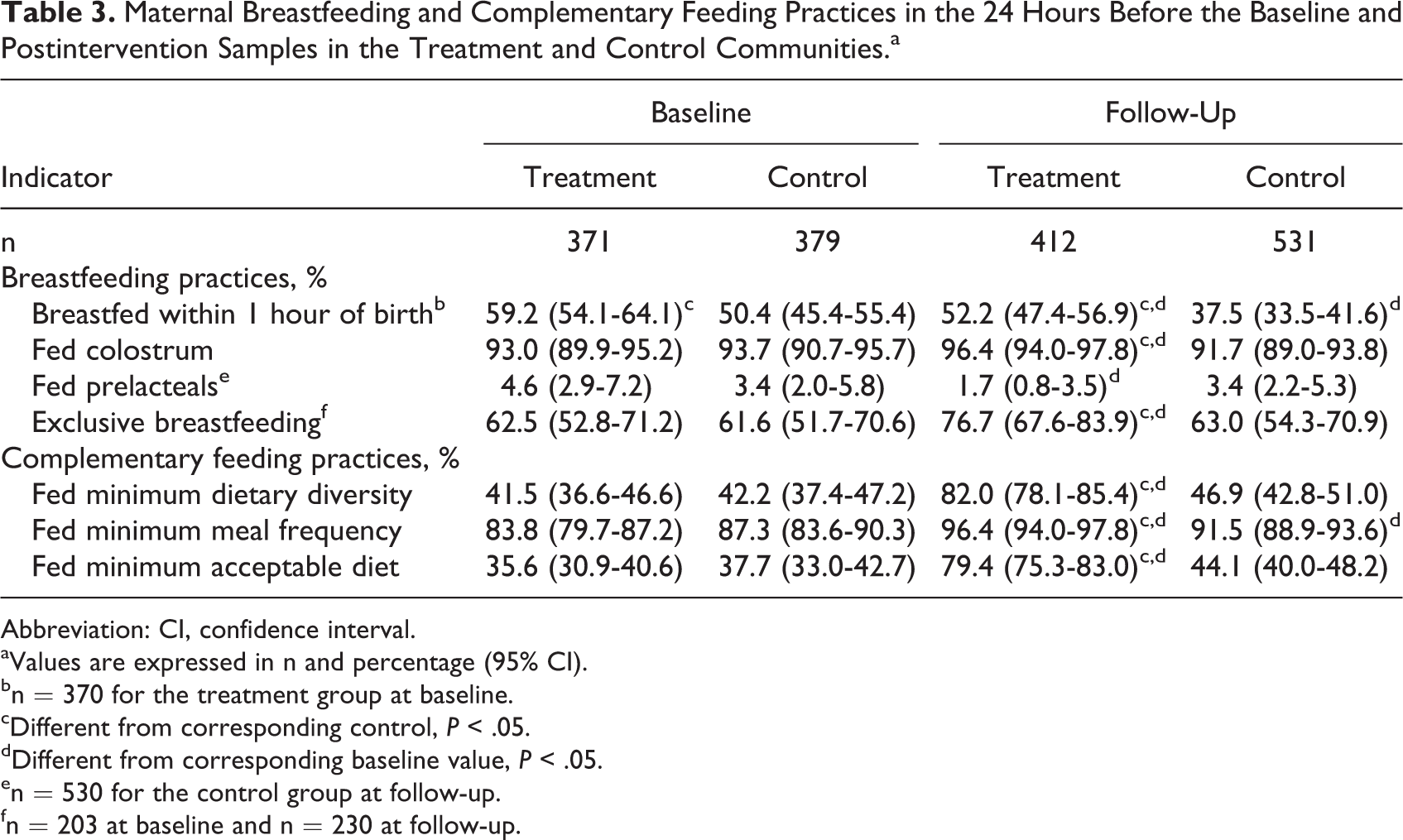
Overall, reported maternal breastfeeding and complementary feeding practices improved in the treatment group relative to the control group (Table 3). The proportion of mothers who initiated breastfeeding within the first hour of life was significantly lower at postintervention (37.5%) compared to baseline (50.4%) in the control group, whereas no significant difference was observed between baseline (59.2%) and postintervention (52.2%) treatment samples. Additionally, fewer of the treatment mothers fed prelacteals and a greater proportion of them fed colostrum and only breast milk during the first 6 months at postintervention compared to baseline (P < .05). However, these practices did not differ among the control mothers sampled at baseline and follow-up. Mother’s complementary feeding practices improved significantly between the baseline and follow-up for the treatment group compared to the control group (Table 3).
Maternal Breastfeeding and Complementary Feeding Practices in the 24 Hours Before the Baseline and Postintervention Samples in the Treatment and Control Communities.a
Abbreviation: CI, confidence interval.
aValues are expressed in n and percentage (95% CI).
bn = 370 for the treatment group at baseline.
cDifferent from corresponding control, P < .05.
dDifferent from corresponding baseline value, P < .05.
en = 530 for the control group at follow-up.
fn = 203 at baseline and n = 230 at follow-up.
Impact on Hemoglobin Concentration and Anemia Among Mothers and Children
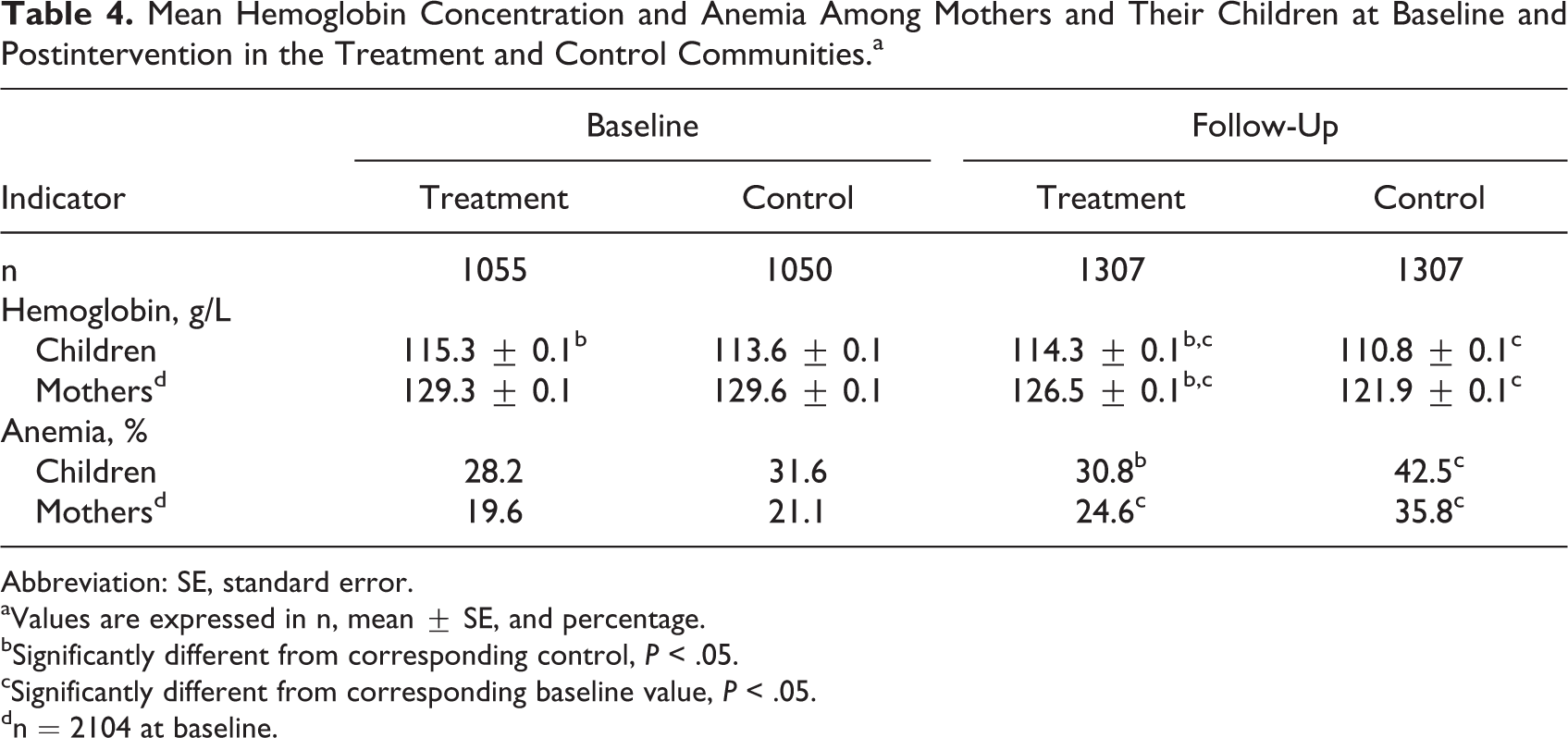
The adjusted mean hemoglobin concentration was significantly lower at postintervention compared to baseline among the children and mothers in both groups (Table 4). The children in the treatment group had higher mean hemoglobin concentration than the control group in both surveys (P < .05). Hemoglobin concentration for mothers was similar among the 2 groups at baseline, but the mothers in the treatment group had significantly higher hemoglobin concentration than the control group at follow-up (Table 4).
Mean Hemoglobin Concentration and Anemia Among Mothers and Their Children at Baseline and Postintervention in the Treatment and Control Communities.a
Abbreviation: SE, standard error.
aValues are expressed in n, mean ± SE, and percentage.
bSignificantly different from corresponding control, P < .05.
cSignificantly different from corresponding baseline value, P < .05.
dn = 2104 at baseline.
Anemia was similar among the children in both groups at baseline but significantly lower at postintervention among the children in the treatment group (30.8%) compared to those in the control group (42.5%). Anemia did not differ between mothers in the 2 groups at either survey and was significantly higher at postintervention compared to baseline in both groups (Table 4).
Each of the multivariate logistic regressions with child and maternal anemia as outcomes showed a significant treatment × time interaction, suggesting that the change in anemia among the children and mothers from baseline to follow-up was significantly different between the treatment and control groups (Table 5). After the intervention, the children in the treatment group were 24% less likely to be anemic compared to those in the control group (odds ratio, OR [95% CI]: 0.76 [0.59-0.98]). Likewise, the mothers in the treatment group were 38% less likely to be anemic compared to those in the control group (OR [95% CI]: 0.62 [0.48-0.82]; Table 5).
Multivariate Logistic Regression of the Impact of the EHFP Intervention on Anemia Among Mothers and Children.a ,b
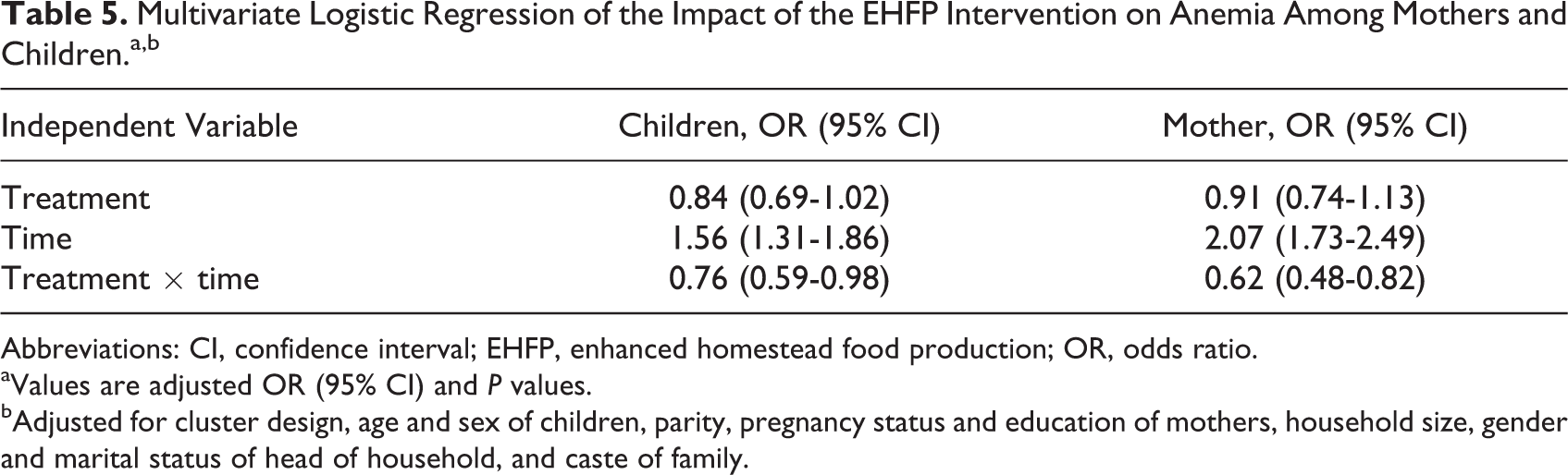
Abbreviations: CI, confidence interval; EHFP, enhanced homestead food production; OR, odds ratio.
aValues are adjusted OR (95% CI) and P values.
bAdjusted for cluster design, age and sex of children, parity, pregnancy status and education of mothers, household size, gender and marital status of head of household, and caste of family.
Impact on Maternal and Child Anthropometry
Table 6 presents the bivariate comparisons of child and maternal anthropometric indicators. Among children, the mean WAZ was significantly higher among the treatment than the control group at baseline but similar among the 2 groups at follow-up. The postintervention mean WAZ was also higher than baseline in both the treatment and control groups. Mean HAZ was significantly higher at postintervention compared to baseline among the treatment but not the control children. Mean WHZ was similar among the 2 groups at baseline but significantly lower among the treatment compared to the control children at postintervention (Table 6). The prevalence of underweight was lower among the treatment (43.4%) than the control (48.0%) children at baseline but similar among the 2 groups at postintervention (41.0% vs 40.6%). Stunting was significantly lower among the treatment than in the control children in both surveys but did not differ significantly between the pre- and postintervention in either the treatment or control group. Wasting was similar among the treatment and control children in both surveys (Table 6).
Anthropometric Indicators for Children Aged 12 to 48 Months and the Women Surveyed at Baseline and Postintervention in the Treatment and Control Communities.a
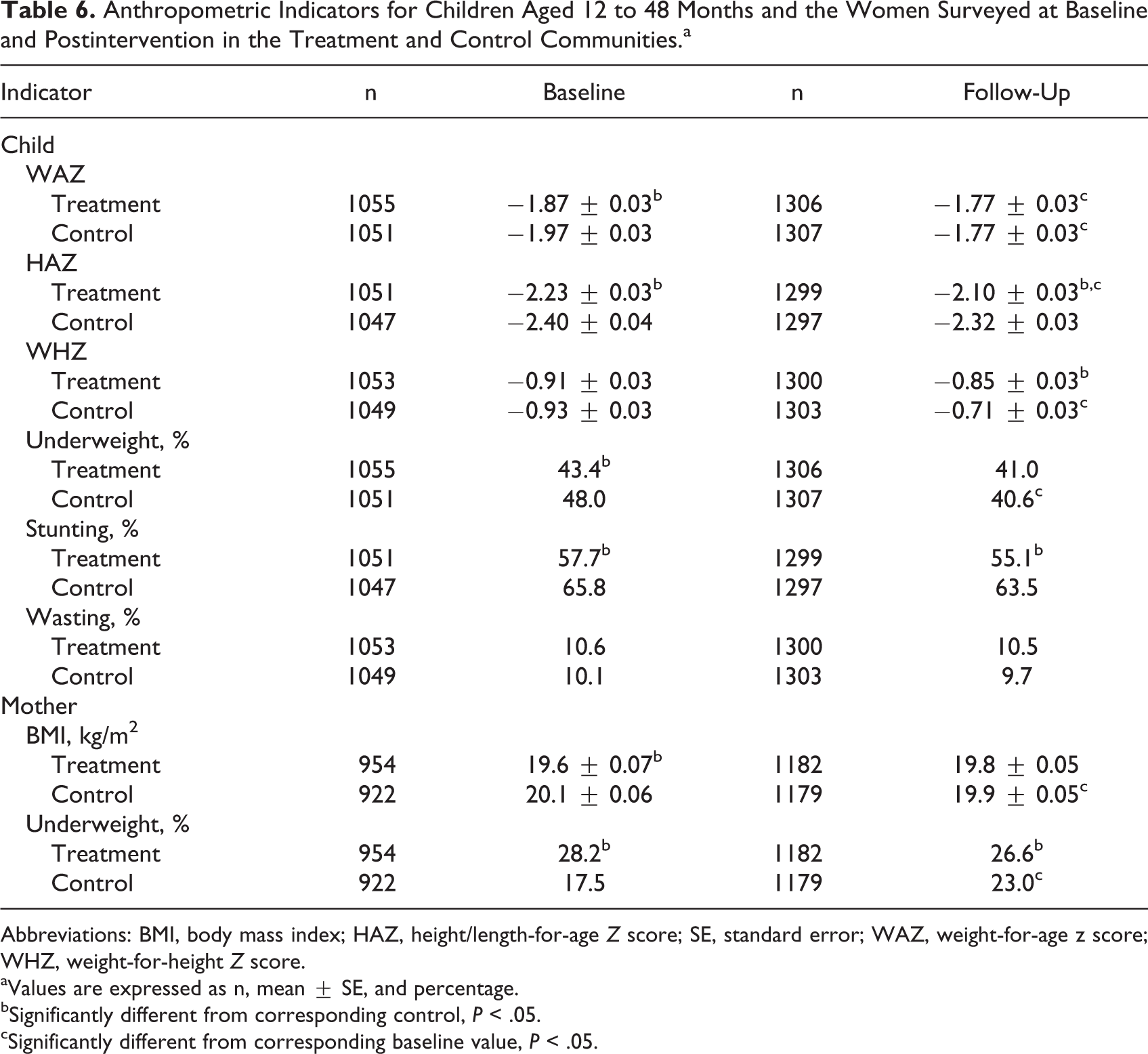
Abbreviations: BMI, body mass index; HAZ, height/length-for-age Z score; SE, standard error; WAZ, weight-for-age z score; WHZ, weight-for-height Z score.
aValues are expressed as n, mean ± SE, and percentage.
bSignificantly different from corresponding control, P < .05.
cSignificantly different from corresponding baseline value, P < .05.
Among mothers, the adjusted mean BMI was significantly lower in the treatment compared to the control group at baseline, although BMI was similar among the 2 groups at follow-up. The postintervention BMI was lower than baseline in the control group, compared to no difference between the 2 surveys in the treatment group (Table 6). Similarly, the prevalence of maternal underweight was significantly higher at postintervention (23.0%) compared to baseline (17.5%) in the control group, whereas it did not vary significantly between the 2 surveys in the treatment group (baseline = 28.2% and postintervention = 26.6%).
None of the multivariate logistic regression models with child anthropometric outcomes showed a significant beneficial effect of the EHFP intervention (Table 7). However, the multivariate logistic regression models with maternal underweight as the outcome indicated that at the end of the intervention, the mothers in the treatment group were 39% less likely to be underweight compared to mothers in the control group (OR [95% CI]: 0.61 [0.46-0.82]; Table 7).
Multivariate Logistic Regression of the Impact of EHFP Intervention on Anthropometry of Mothers and Children.a
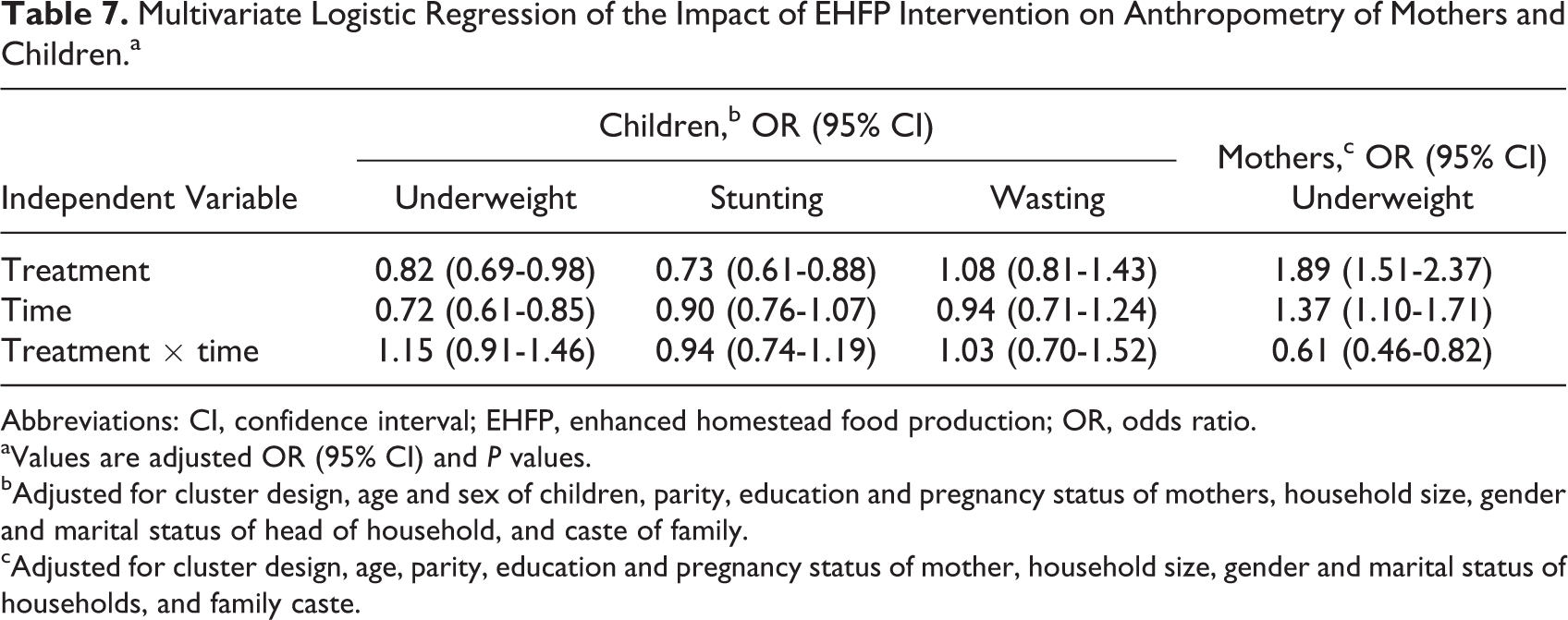
Abbreviations: CI, confidence interval; EHFP, enhanced homestead food production; OR, odds ratio.
aValues are adjusted OR (95% CI) and P values.
bAdjusted for cluster design, age and sex of children, parity, education and pregnancy status of mothers, household size, gender and marital status of head of household, and caste of family.
cAdjusted for cluster design, age, parity, education and pregnancy status of mother, household size, gender and marital status of households, and family caste.
Discussion
To our knowledge, this is one of the few studies that have used a randomized controlled design to assess the impact of a homestead food production on the health and nutritional outcomes of women and children. The EHFP intervention promoted in our study significantly improved households’ participation in home garden and poultry rearing activities, perception of household food security, and reported maternal practices in breastfeeding and complementary feeding in the Baitadi District of Nepal. In addition, this intervention improved other maternal practices such as handwashing with soap, antenatal visits, IFA supplementation and deworming during pregnancy, as well as children’s immunization, vitamin A supplementation, deworming, and participation in GMP (Supplemental Tables 1 and 2). Furthermore, at the end of our intervention, the prevalence of anemia was significantly lower among children and mothers and underweight was lower among mothers in the intervention households compared to the control. There was, however, no demonstrated impact of the intervention on child anthropometry.
Comparing our results to that of past studies is quite challenging due to considerable variations in intervention components in the different studies, with some of the past studies promoting only home gardens, others home gardens together with animal husbandry, or these models with or without nutrition education. Nevertheless, the positive effect of the EHFP on anemia among children and mothers in the treatment compared to the control communities of our study is consistent with the findings of other studies in Bangladesh, Philippines, and Nepal, 13 adding to the evidence that food-based interventions can reduce anemia among children and women. Although home gardening and backyard poultry are usual practice in most rural communities in Nepal, our results revealed significant improvement in families participating in the combined home garden and poultry activities (the interventions promoted in our study) and several intermediary outcome variables (by which the EHFP intervention was expected to create an impact), in the treatment compared to the control communities, suggesting that the observed difference in the changes in primary outcomes is due in part to our EHFP intervention. The improvement in the number of different types of vegetables grown, number of eggs produced, household food security, and maternal practices related to breastfeeding and complementary feeding in our study are consistent with that of other studies that concluded that nutrition-sensitive agriculture interventions can improve household food production and consumption 4,5,7,9,12,14,21 and health-related practices of mothers, especially those related to breastfeeding and complementary feeding. 5,6,7,14,21 In the Terai region of Nepal, Jones et al found that participation in a combined intervention of kitchen gardens with nutrition education improved maternal knowledge of nutrition, complementary feeding practices, and increased the variety of vegetables consumed by their families. 31 Studies in Nepal, Bangladesh, Cambodia, and the Philippines have also found that families who participated in homestead food production activities benefited from increased production and consumption of vegetables, fruits, and poultry products. 13 Similar findings were documented for families who participated in an integrated program of home garden, nutrition education, and fish or livestock production in Vietnam. 8
The mitigation of the rise in anemia prevalence realized in our treated communities can be explained by several factors, including significant improvements in maternal practices related to breastfeeding, complementary feeding, and handwashing with soap as well as child and maternal participation in several other preventive public health programs in the treatment group compared to the control group, as well as improvement in food production and consumption by families. A post hoc analysis involving the postintervention sample showed significantly high adjusted mean ± standard error (SE) hemoglobin concentration (128.4 ± 0.3 g/L vs 126.3 ± 0.8 g/L; P < .05) and low anemia prevalence (29.6% vs 36.9%; P < .05) among mothers who took IFA supplement for 5 or more months (n = 2009) than those who took such supplement for less than 5 months (n = 309). That said, the significantly higher prevalence of anemia at postintervention compared to baseline in the treatment mothers was not expected and might be explained by a potential variability in other risk factors that influence anemia among the pre- and postintervention samples, including the extent of deficiencies of iron and other micronutrients (vitamins A, B2, B6, B12, and folate), helminths, and other infections. Unfortunately, none of these factors were assessed in our study. The control communities also experienced significant improvement in households engaged in home gardening and backyard poultry activities as well as several other intermediary outcomes including maternal handwashing practices, childhood immunizations and participation in GMP, and maternal use of antenatal services and intake of IFA supplements, although not to the same extent as the treated communities. Such changes in the control communities might be due to homestead food production being a usual practice in Nepal and the routine public health services provided by the government in all communities in Nepal.
Although disappointing, our findings of no effect of the EHFP on anthropometry of children is not surprising and similar to the results of the majority of previous studies. It is possible for such lack of impact on child growth to be due to inadequate statistical power and the use of independent cross-sectional surveys, instead of assessing the same individuals at baseline and posttreatment to evaluate the impact of the intervention. Masset et al have argued that at least 4000 participants are needed per survey to detect a medium effect of 10% reduction in stunting resulting from nutrition-sensitive agriculture interventions. 5 Furthermore, the families in the treatment group of our study were exposed to the EHFP intervention for only 2.5 years, which may have limited the impact on child growth. Other factors such as infections could also have reduced the potential impact of the intervention on child growth. We only obtained infection data at baseline and follow-up (not shown), which is not sufficient to assess the impact of morbidity on child growth during the period of the intervention. The significant positive changes in proportion of households with gardens and/or poultry and some intermediary outcome variables in the control group also had a potential to have decreased the measured impact of our EHFP intervention. By first randomizing communities to treatment at the subdistrict level, there was minimal likelihood for our EHFP intervention activities to have passed onto the control communities.
On the other hand, the positive effect of the EHFP intervention on maternal underweight is encouraging. As far as we are aware, this is the first study to publish the effect of nutrition sensitive-agriculture intervention on women’s anthropometry. Several factors could potentially explain the positive impact on maternal but not child anthropometry in our study. The EHFP intervention was expected to empower women through their improved nutrition and health knowledge (including understanding the importance of their own nutrition to the growth of their children), as well as increased access to resources. Additionally, cultural practices including age-based preferential allocation of food within the household could have influenced the way mothers and children were fed in the study communities. Past studies in some areas of Nepal suggest postpartum women are thought of being in a “cooling state” and so are preferentially fed chicken and other foods that are considered “heating” foods. 32 The formative research conducted prior to our EHFP intervention in the district revealed cultural preferences to provide more calories and some animal products (such as chicken and eggs) that are believed to increase breast milk production. 33 Considering the EHFP intervention would have increased access of the treatment households to these nutritious foods, it was possible for mothers in these to have had improved consumption of such foods.
The limitations of our study include the use of pre- and post-cross-sectional surveys, which reduced our ability to completely attribute the observed changes in outcomes to the intervention. However, the use of a randomized study design and the inclusion of a control group make it probable that the observed changes in outcomes are due, at least in part, to the EHFP intervention. Other limitations include initial randomization at the subdistrict level, which might have reduced statistical power of the study, and our inability to distinguish the effect of the different intervention components (home garden, poultry, or nutrition education) on the observed improvements in outcomes. Our study was also not able to determine the effect of the intervention on other factors that could influence nutritional status of women and children, including the time allocation of women and the impact of the program inputs on intrahousehold resource allocation or overall household income.
Conclusion
The study showed that an integrated intervention including home gardening, backyard poultry rearing, and nutrition behavior change communication can play an important role in improving household food security, maternal handwashing and child feeding practices, use of certain preventive health services, and maternal and child anemia as well as maternal underweight. However, there was no demonstrated impact on child growth. Further research over a long period is needed to assess the potential impact of homestead food production interventions on child growth.
Footnotes
Authors’ Note
A.K.O., N.H., P.P., J.N., D.S., and V.Q. conceptualized, designed, and conducted the research. A.K.O. and A.P. analyzed the data and wrote the manuscript. P.P., J.N., N.H., D.D., and V.Q. provided comments on the paper. A.K.O. and A.P. had the primary responsibility of final contents. All authors read and approved the final manuscript.
Acknowledgments
The authors thank Rom Shresther and Debendra Adhikari for their inputs in the conception and implementation of this study. The authors also thank Rolf Klemm for his review comments.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support was provided by the United States Agency for International Development (USAID).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.