
Abstract
Background:
Food insecurity (FI) refers to limited or uncertain access to food resulting from financial constraints. Numerous studies have shown association between FI and adverse health outcomes among adults and children around the world, but in Brazil, such information is scarce, especially if referring to nationally representative information.
Objective:
To test for an independent association between FI and health outcomes.
Methods:
Most recent Brazilian Demographic and Health Survey using nationally representative complex probability sampling. Participants were 3923 children <5 years of age, each representing a household. Data from the validated Brazilian Food Insecurity Scale were dichotomized as food secure (food security/mild FI) or food insecure (moderate FI/severe FI). Poisson regression was used to test for associations between FI and various health indicators.
Results:
Models adjusted for socioeconomic and demographic variables showed that children hospitalized for pneumonia or diarrhea were 30% more prevalent in FI households (adjusted prevalence ratio [aPR]: 1.3; 1.1-1.6). Underweight children were 40% more prevalent in FI households (aPR: 1.4; 1.1-1.7). Children who didn’t eat meat and fruits and vegetables every day were 20% and 70% more prevalent in FI households (aPR: 1.2; 1.1-1.4 and aPR: 1.7; 1.3-2.3), respectively.
Conclusion:
Children who grow up in food-insecure households have been shown to have worse health conditions than those in food-secure households. Consequently, their human capital accumulation and work–life productivity are likely to be reduced in the future, leading them into adulthood less capable of generating sufficient income, resulting in a cycle of intergenerational poverty and FI.
Introduction
Food security, when all people at all times have access to sufficient, safe, and nutritious food to maintain a healthy and active life, 1,2 is the ideal environment in which to raise a child. However, this ideal situation can be disrupted by lack of money to acquire sufficient nutritious food, leading families to experience different levels of severity of food insecurity (FI).
To protect their bodies from weakening, people with constrained resources often compromise the quality or variety of food they purchase in order to maintain food quantity at a level perceived by household members as adequate. This condition is defined as mild FI. If deprivation of financial resources continues, people also decrease the quantity of food purchased and consumed, influencing the usual eating patterns among adults. This situation is known as moderate FI. Households with severe FI are characterized by breakdown of usual feeding patterns, compromising quality and reducing the quantity of food in meals of all family members, including children living in the household. 1,2 Under these circumstances, household members may also experience hunger, defined as the uneasy or painful sensation caused by involuntary and recurrent lack of food, when its intake is reduced below normal levels. 3
In Brazil, data from a national survey identified 37.5% of households with some level of FI. 4 Among households with at least 1 child under 5 years of age, the prevalence of FI was 20% higher (45.5%), 5 meaning that proportionally more households with children under 5 were affected by the lack of access to food at home when compared to all Brazilian food-insecure households. It indicates the double burden of representing a group of individuals more susceptible to adverse effects due to their stage of life in addition to living in food-insecure households. 5
Food is important to maintain body systems, especially in children. Lack of nutrients due to the absence of food in adequate quantity and quality to fulfill the basic needs for growth and development will impact health adversely, and consequently, the capacity for human capital accumulation. 6 By adversely impacting the ability to learn, develop skills, and expand knowledge, abilities, and potential, FI can predispose children to failure in preparation for becoming productive members of the workforce and society. 7,8,9
The negative implications of FI for health have been widely described, 10 –18 but little is known about its impact on Brazilian children. 19,20 This research examines the associations between direct measures of health among Brazilian children under 5 and FI, aiming to identify adverse impacts on their well-being.
Methodology
Study Design
The third edition of the National Survey on Demography and Health of Women and Children (PNDS 2006/07) aimed to describe the health and nutrition of reproductive-age women (15-49 years old) and their children under 5 years old. This survey also gathered data on social, economic, and cultural factors, including FI at the household level using the Brazilian Food Insecurity Scale (EBIA). The PNDS 2006/07 used a complex probability sampling design collected in 2 stages: the primary sampling unit was the census area and the secondary sampling unit was the household. The sample included only noninstitutionalized private households. Eligible households were selected at random, considering the number of census areas in each region and whether they were located in urban or rural areas. The research methodology, including sample selection, procedures for data collection, data consistency, weighting and expansion techniques for complex samples, and ethical aspects, is described elsewhere. 21
Ethical Standards
The PNDS data were collected according to the criteria established by the Declaration of Helsinki, and all procedures involving human subjects were approved by the Centre for Reference and Training in HIV/AIDS, Department of Health of the State of São Paulo Ethics Committee. In addition, this study was approved by the ethics xommittee in Research of the Universidade Federal de São Paulo/Hospital São Paulo (protocol no. 2117/11).
Outcome Variable
The outcome variable for this research is food security status measured by the validated US Household Food Security Survey Module (HFSSM) adapted for the Brazilian population (referred to henceforth as the EBIA). For methodological purposes, the PNDS 2006/07 used a modified EBIA, containing 16 questions, since question number 5 “In the last 3 months, did you or other adults in the household ever cut the size of your meals or skip meals because there wasn’t enough money to buy food” was split into 2 parts “In the last 3 months, did you or other adults in the household ever cut the size of your meals because there wasn’t enough money to buy food.” And “In the last 3 months, did you or other adults in the household ever skip meals because there wasn’t enough money to buy food.” For analysis purposes as indicated by PNDS, these 2 questions were recombined as a negative answer “no” when both parts had negative responses, or “do not know” to 1 part, and “no” to the other part. For any other possibility, the answer was marked positively “yes.”
The number of questions affirmed indicates the level of FI in the household and is the basis for classifying households in one of the 4 food security categories. When the response was “do not know” to questions regarding conditions of access to food (first to fourth question), the interview was interrupted, and the record was eliminated (n = 17, corresponding to 0.35% of sample). The 4 food security categories for households with children under 18 years are as follows: food secure (0 questions affirmed), mild FI (1-5 questions affirmed), moderate FI (6-10 questions affirmed), and severe FI (11-15 questions affirmed). 4 All questions in the EBIA refer to the 3 months preceding the survey, instead of the 12-month reference period used in the HFSSM. Prevalence estimates were generated for the 4 levels of food (in)security. Inferential analyses were conducted using a food security status variable dichotomized as households not considered at risk, including the food security and mild FI categories (food security) or against those at risk, comprising moderate and severe FI categories (FI). The FI composite category represents the greater severity of food scarcity in the household, where adults and children could be experiencing hunger in the last 3 months.
Exposure Variables
Prevalence estimates for macroregion were calculated for 5 administrative geographical regions: north (N), northeast (NE), midwest (MW), southeast (SE), and south (S). For both bivariate and multivariate analyses, variables were dichotomized to contrast Brazilian development areas, with the MW, SE, or S identified as more developed regions. For prevalence estimates and prevalence ratio (PRs) of urban–rural classification, urban or rural household status was considered.
Per capita or household income measures the direct availability of financial resources to purchase food and other goods and services. In Brazil, it is considered an unstable variable varying monthly for families with unstable jobs. Therefore, to represent household’s economic status, the Brazilian Economic Classification Criterion (CCEB) was used as an indicator for families’ purchasing power. The CCEB quantifies 8 household items (color TV, radio, bathroom, car, washing machine, VCR/DVD, refrigerator, and freezer), number of household employees, and the level of education of the household head. Scores vary from 0 to 46 points, and 8 cutoff points are used to indicate the purchasing power of each person or family. From A1, the wealthiest economic class, to D or E, the less affluent economic classes. 22 For prevalence estimates, bivariate, and multivariate analyses, a dichotomized variable was used grouping household economic status into wealthier classes, that is, from A1 to C2, and less wealthy classes, that is, D/E.
The living conditions variable was composed of 5 items: type of water system, sewage system connection, predominant material used on house ceilings, walls, and floor. This variable indicates the housing quality based on whether water is available via indoor plumbing inside the house, the house is connected to a sewer network, the ceiling in house is made of shingle or concrete slab, the walls are bulit of brickwork, and the floors are made of wood, vinyl, ceramic tiles, cement, or carpet.
Cash transfer program (CTP) was labeled “yes” for households receiving any financial aid from at least 1 of Brazil’s social safety-net programs in 2006: Bolsa Família, Bolsa-Escola Municipal, Benefício de Prestação Continuada, Auxílio-gás, Cartão Alimentação, Programa de Erradicação do Trabalho Infantil, and Agente Jovem. For statistical analysis, a dichotomous variable was used to indicate when a resident of the household received any of these forms of governmental financial aid (receive CTP).
Maternal education was dichotomized as ≤8 years or more than 8 years of study. This categorization of education attainment is equivalent to graduation from middle school. Marital status variable followed PNDS criterion: when a woman was formally married or was in a stable union, she was considered having a partner (with partner). If a woman was single, widowed, separated, legally separated, or divorced, she was considered without a partner (without partner—w/o partner). The number of children living in the same household was dichotomized as 1 to 2 children or ≥3 children. Exclusive breast-feeding was obtained retrospectively by asking mothers for how long they fed their children solely breast milk, without providing water, tea, or other foods. This variable was dichotomized as children breast-fed solely on breast milk for more than 6 months or less than 6 months (<180 days/>180 days), or breast-fed children solely on breast milk for exactly 6 months (180 days).
To assess vitamin A and iron levels, blood samples were collected from a single drop spot of blood and deposited on a paper filter. The paper was analyzed by high-performance liquid chromatography at the Laboratory of Nutrition from the Faculty of Medicine of Ribeirão Preto (São Paulo, Brazil). The complete protocols, methodologies, and cutoff points are described elsewhere. 23 Hypovitaminosis A was dichotomized as having hypovitaminosis A at ≤0.70 µmol/L (yes) or not having hypovitaminosis A at >0.70 µmol/L (no). Anemia was dichotomized as having anemia when hemoglobin was ≤11 g/dL (yes) and not having anemia when >11 g/dL (no). Hospitalization was based on mother’s report of whether the child wase hospitalized for diarrhea or pneumonia at least once in the 12 months prior to interview (yes).
The Laboratory of Nutrition Assessments of Populations from the Department of Nutrition (LANPOP-USP), School of Public Health, University of São Paulo was responsible for selecting anthropometric equipment, training and standardization of interviewers, supervision, and quality control of measurements. Techniques used to obtain all measurements followed the standard procedures 24 and were taken in duplicate, considering the average of the 2 measurements as the final result. Children were weighed by trained field-workers using a portable electronic scale with 100 g precision (Dayhome, São Paulo, Brazil). Details are described elsewhere. 25 Weight-for-Age categories, described in Z scores (WAZ), were based on the World Health Organization standards. 26 For analysis purposes, a dichotomous variable named nutritional status was created, considering a child underweight if the WAZ < −2.0 and not underweight if the WAZ ≥ −2.0. These categories were used for prevalence estimates, bivariate, and multivariate analyses.
Dietary intake was obtained using a qualitative food frequency questionnaire (FFQ) composed of 20 typical Brazilian foods. The frequency of children’s consumption of each food was reported by the mother for the 7 days preceding the interview. Response options were “have not eaten in the past 7 days,” “have eaten 1, 2 to 3, or 4 to 6 days in the past 7 days,” “have eaten every day in the past 7 days,” or “do not know.” 27 For the variable meat, 4 types of meat were chosen from the FFQ to reflect its consumption (cow/pig, liver, chicken, and fish). A dichotomous variable, indicating whether children had eaten meat every day in the past 7 days prior to interview, was created. The 2 categories for this variable indicated either a child had eaten meat at least 1 time per day in the past 7 days (at least 1×/day) or a child had eaten meat but not every day in the past 7 days (not every day). To compose the fruits and vegetables variable, 3 food groups were selected from the FFQ. Daily consumption of fruits and vegetables (from the Brazilian questionnaire: frutas, verduras, and legumes) indicates the child consumed at least 3 healthy foods daily, as recommended by the Brazilian Ministry of Health. 28,29 A dichotomous variable, indicating whether children had eaten fruits and vegetables every day in the past 7 days prior to interview, was created. The 2 categories for this variable indicated either a child had eaten fruits and vegetables every day in the past 7 days (every day) or a child had eaten fruits and vegetables but not every day in the past 7 days (not every day). Children under 6 months of age were counted in the analysis by including in the “every day” dichotomous category, children who had not eaten fruits and vegetables on any given day in the past 7 days, implying that breast-feeding, or formula feeding, was the only form of food they had eaten.
Eligibility and Selection Criteria for the Study Sample
For this research, eligible children included those ≤59 months of age, living in the same house as their mothers, and with the EBIA filled correctly (totaling 4800 children). Because the study unit is the household, PNDS replicated EBIA answers for all individuals living in a particular household. Therefore, it was necessary to select 1 child per household to avoid duplication of sample unit representation in the data analysis. Thus, when a woman had more than 1 child younger than 5 years, the younger child/children was/were dropped out of the sample (n = 784). When there were 2 or more children under age 5, and they were children of different mothers residing in the same household, the younger child/children was/were excluded (n = 61). In addition, when there were twins in the household, we maintained in the sample only the twin who was born in better condition, using birthweight as reference. We excluded the twin with the lower birthweight noted on the child’s official Brazilian health record card. If the card was unavailable, birthweight reported by the mother was used. If neither of these were available, the younger child was excluded (n = 35). The younger twin was identified by a variable stating the children’s order of birth. Selection criteria followed a rationale of maintaining in the sample children who had lived longer under determined environmental conditions. After exclusions, 3920 children (1 per household) were available for analysis, representing 11 779 686 households when expanded using sample weights.
Data Analysis
To merge and analyze PNDS 2006/07 data sets, Stata/IC 12 (StataCorp LP, College Station, Texas) was used. To correctly reflect the stratification and clustering effects of the complex sampling design, all analyses were performed using the complex survey command (svy) to represent the Brazilian population. However, to avoid overestimating associations in subgroups, sample weights were only used in descriptive analysis. 30
The χ2 test with a second-order Rao-Scott correction 31 was used in descriptive analysis of socioeconomic, demographic, and biological variables and disaggregated FI. To test the hypothesis that worse health conditions of children under 5 would be associated with living in a moderate or severe food-insecure household, we performed a Poisson regression analysis. 30 Variables with P < .20 in bivariate analyses were considered eligible for inclusion in the multivariate analysis. After adjusting for socioeconomic, demographic, and the following variables: macroregion, urban–rural classification, living conditions, economic status, CTP, maternal education, marital status, number of children, sex, and age, the final model contained only the strongest associated variables, with P < .05, using a backward stepwise elimination technique.
Results
The association of FI and 4 variables (macroregion, urban–rural classification, economic status, and CTP) is addressed in a previous publication. 5 To further clarify the environmental conditions of households with FI, the present research assessed living conditions, economic status, receipt of CTPs, maternal education, marital status, and number of children living under the same roof. The prevalence of moderate and severe FI among the risk categories of sociodemographic variables cited above were found to be between 25.7% and 36.5% against 7.9% and 16.2% among the nonrisk categories (Table 1). Similar prevalence of moderate and severe FI was found among the risk categories of exclusive breast-feeding, hypovitaminosis A, and anemia when compared to each variable’s reference category (P < .05).
Description of Demographic, Socioeconomic, and Biological Variables by Food Insecurity in Households With Children Younger Than 5 Years.
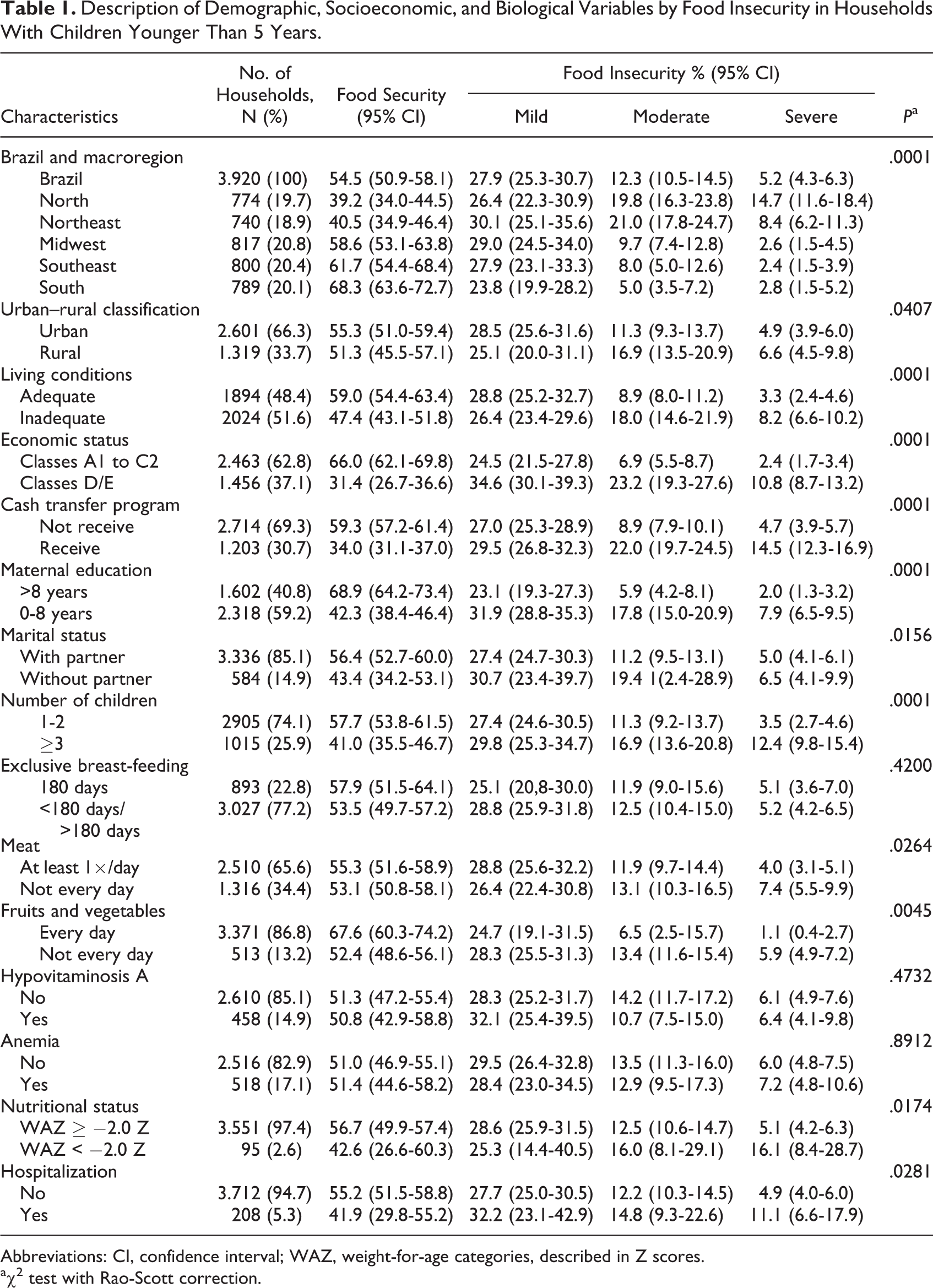
Abbreviations: CI, confidence interval; WAZ, weight-for-age categories, described in Z scores.
aχ2 test with Rao-Scott correction.
The proportions of children who did not eat meat (20.5%) and fruits and vegetables (19.3%) every day, as recommended by the dietary guidelines, were higher than those who ate meat at least once a day (15.9%) and fruits and vegetables every day (7.6%) in households with FI. Nearly one-third (32.1%) of underweight children lived in households with FI when compared with those with weight-for-age ≥ −2.0 Z score (17.6%). Approximately, 1 (25.9%) in every 4 children, who experienced at least 1 hospitalization due to pneumonia or diarrhea in the year prior to interview, lived in a household with FI versus their peers who were not hospitalized (17.1%; Table 1).
In the adjusted models, children who did not eat meat or fruits and vegetables every day in the previous 7 days of interview were significantly more prevalent in households with FI (adjusted PR [aPR]: 1.2, 95% confidence interval [CI]: 1.1-1.4; aPR: 1.7, 95% CI: 1.3-2.3, respectively; Table 2). Underweight children were 40% more prevalent in households with M/SFI (aPR: 1.4; 95% CI: 1.1-1.7). Children who had at least 1 hospitalization for pneumonia or diarrhea in the 12 months prior to interview were 30% more prevalent in households with FI (aPR: 1.3; 95% CI: 1.1-1.6; Table 2).
Association of Demographic, Socioeconomic, and Biological Variables With Food-Insecure Households With Children Younger Than 5 Years.
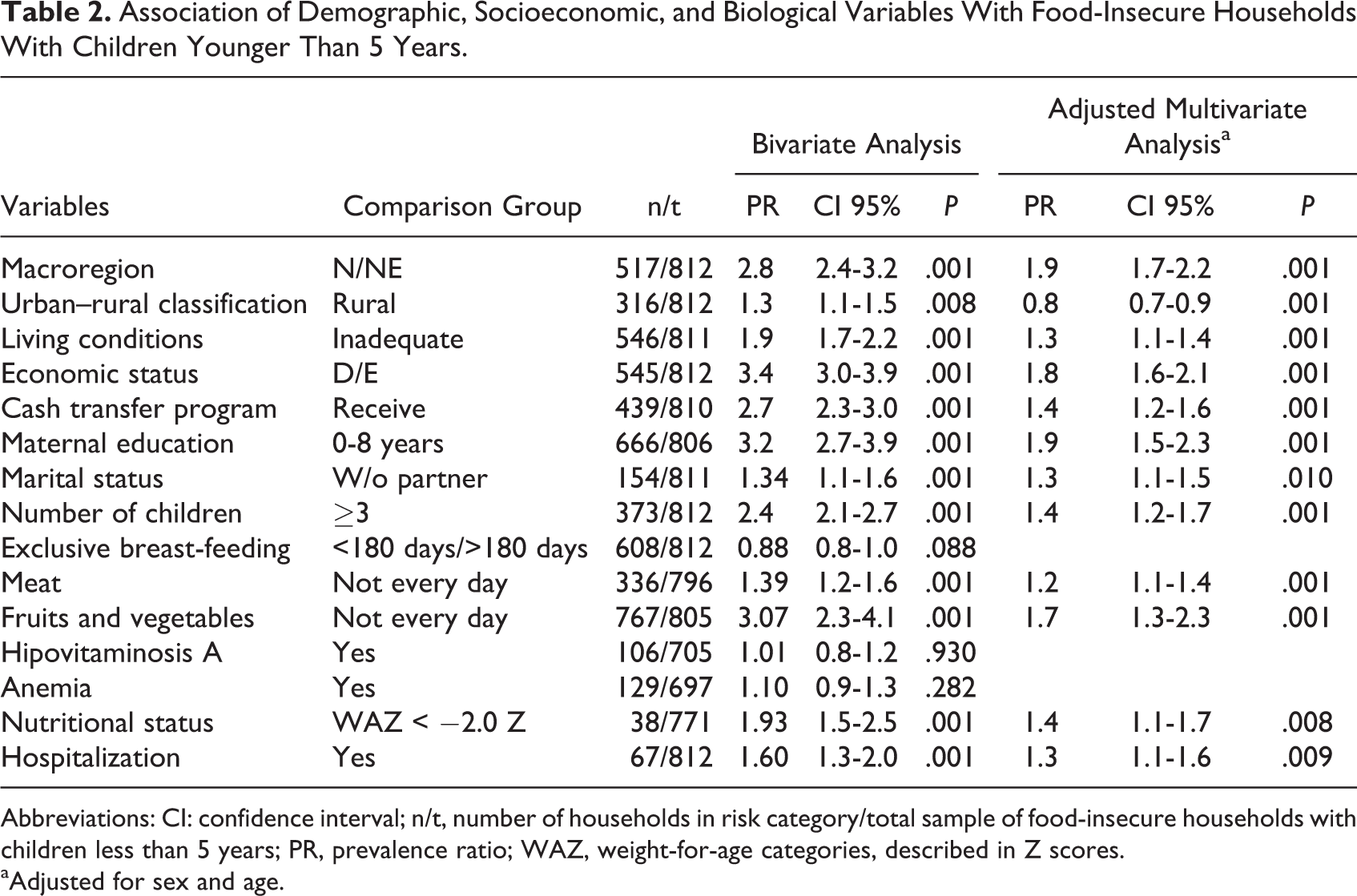
Abbreviations: CI: confidence interval; n/t, number of households in risk category/total sample of food-insecure households with children less than 5 years; PR, prevalence ratio; WAZ, weight-for-age categories, described in Z scores.
aAdjusted for sex and age.
Discussion
The understanding of chronic fluctuation in availability, variety, and nutritional adequacy of food resources in Brazilian households and related nutritional deficiencies in their residents could not be adequately described until the year 2000. Since development of direct measures to assess FI 32 –36 and advances in research on the role of nutrition in health, understanding of the associations between health and household food security is being clarified. Yet, little is known about associations between direct measures of poor health among young children (under 5 years) and FI in Brazil and their possible consequences for the country’s future prosperity.
Children are especially vulnerable to adverse health outcomes related to constrained household resources. 11 Results from this nationally representative cross-sectional study show 3 important health-related factors independently associated with the health of children living in moderately or severely food-insecure households: nutritional status, healthful food consumption, and hospitalizations due to diarrhea or pneumonia.
Nutritional Status, Nutrition, and FI
For household food security to exist, food has to be both available and accessible. Healthy food must be in the market, and people must be able to afford it. Additionally, for an active and healthy life, people need to achieve adequate nutritional status, achieving balance in consumption of fats, protein, carbohydrates, and micronutrients.
In 2013, about 17% of children were underweight, the equivalent to 98 million children under 5 years of age in developing countries. Globally, the proportion of children under 5 years old who were underweight declined by 10 percentage points, between 1990 and 2013 (from 25% to 15%). 37 In Brazil, the latest national survey indicated an overall 1.9% of children under five with underweight. 38 Among households where maternal education was less than 3 years or households with economic status classified as “E,” the prevalence of underweight was 2-fold, reaching 4.6% and 4.7%, respectively. Although the prevalence of underweight in Brazil was smaller than that worldwide, the present study found that one-third of underweight children under 5 were living in moderately or severely food-insecure households (32.1%).
About 795 million people are undernourished globally, and the contrast in prevalence of undernourishment between developed countries (<5%) and developing countries (12.9%) is vast. 39 Among Brazilian children under 5, the prevalence of anemia was found to be 20.9% and hypovitaminosis A was 17.4% in the last national survey. 23,38 Although not significantly associated with FI, the present study found comparable prevalence of anemia and hypovitaminosis A among children living in food-insecure households of 20.1% and 17.1%, respectively.
Factors influencing child undernutrition are multifaceted. Immediate (individual), underlying (household/family), and basic (societal) levels, such as food (insufficient access to food, inadequate dietary intake), health (disease, poor water/sanitation), and caring practices (inadequate maternal and childcare practices) are the recognized causes of child undernutrition according to the conceptual framework of United Nations Children’s Fund. 40 Household FI implicitly affects children’s nutritional status by compromising the quality and quantity of dietary intake. In addition, the effects of FI on adults in households with children can adversely affect children in a variety of ways, including decrease in parents’ energy for providing care and developmental stimulation. In other words, children who live in a food-insecure household undergo negative effects, such as undernutrition, through low dietary intake, low sanitation, and parental depression.
Adults and elderly individuals, but not preschool children, from food-insufficient households have been shown to have a lower nutrient intake than those from food-sufficient households, 41 and fruit and vegetable intake in adults has been shown to decline as FI becomes more severe. 42 The present research found that children under 5 who didn’t eat fruits and vegetables everyday were 70% more prevalent in moderately or severely food-insecure households (aPR: 1.7; 1.3-2.3). In addition, children under 5 who did not eat meat at least once a day were 20% more prevalent in moderate or severe food-insecure households (aPR: 1.2; 1.1-1.4). Usually, adult caretakers living in food-insecure households with children reduce overall quality and variety of their own food intake, sparing children from hunger. This study confirms that in food-insecure households, children are deprived of food in quality and quantity, indicating the urgency of a change in the situation of disrupted eating patterns and reduced food intake. 41,43
The nutritional quality of the diet of food-insecure individuals is less than optimal, in part because fruits and vegetables are more expensive than less nutritious foods. Nutrient-dense foods (fruits, vegetables, whole grains, and lean meats) are more expensive per calorie than energy-dense foods (soft drinks, salty and sugary snacks, and pastries). A study conducted with 456 families in Campinas, Brazil, detected a 68% compromise in household total income just with food, similar to what Josué de Castro found several decades ago in Recife, Brazil. 44 In addition to its cost, families tend to shop in corner stores, which was found to be 150% to 400% more expensive than a supermarket. 45 People living with less than or equal to US$1.00 per person/day, to achieve nutrition recommendations, would have to increase their food expenditure to 58%. 46 Therefore, multivariate analysis is consistent with the outcome measured in which food-insecure families consume less nutrient-dense foods due to lack of financial resources, which may have increased their risk of undernutrition and hospitalizations. 47 Researchers found that an increase in income is to be determinant in rise of meat and fruits and vegetables consumption. 48
It is expected that a less varied diet over time is related to micronutrient deficiency, 49 especially hypovitaminosis A and anemia, which are public health problems in Brazil. The similarity of the food-insecurity profile among children with anemia and without anemia, and also among those with hypovitaminosis A and without it, may be due to factors associated with food-insecurity, such as low birth weight, maternal anemia, and high prevalence of enteric parasites, variables not included in the model or not collected by the survey data. Could also be associated with quality problem of the exams, due to storage and transport and even to the sample lost (21.7% in the vitamin A sample, and 22.6% in the hemoglobin sample).
Hospitalizations and FI
Since respiratory and diarrheal diseases were among the leading causes of morbidity and mortality in children under 5 during many years, an increased focus on reduction of cases has generated interest in more accurate assessment of their prevalence. 50 In 2001, the Child Health Epidemiology Reference Group (CHERG/WHO) reviewed the morbidity and mortality burden of pneumonia among children aged less than 5 years, for the year 2000. The analyses suggested that the incidence of clinical pneumonia in developing countries was close to 0.29 episodes per child-year. This equates to an incidence of 151.8 million cases every year, 8.7% of which were severe enough to require hospitalization. In addition, a further 4 million cases occurred in developed countries. 51 In the United States, a study conducted from 2010 to 2012 estimated that annual pneumonia incidence was 15.7 of 10 000 children during the study period. 52
In Brazil, severe cases of pneumonia among children under 4 requiring hospitalizations were 55065 per 10000 inhabitants in 2005, decreasing almost 11% in 7 years (490.6/10.000 inhabitants in 2012). The last national prevalence of children under 5 hospitalized due to pneumonia was 15.3%. 38 Although there has been a decrease in such hospitalizations, current monthly expenditures for hospitalizations related to pneumonia in children under 4 years range between R$10 000 000 and R$20 000 000. 53
Aiming to estimate mortality from diarrhea, the CHERG/WHO model-based global result was 1.87 million (uncertainty range: 1.56-2.19) diarrhea deaths in the year 2014, corresponding to nearly 19% of the 10 million under 5 deaths that occurred in the world. 54 In Brazil, diarrhea triggered just by rotavirus infections represented 3 525 053 episodes of diarrhea, 655 853 visits to outpatient health-care facilities, 92 453 hospitalizations, and 850 deaths of children ≤ 5 years of age, each year. 55
Pneumonia and diarrhea share environmental risk factors, such as malnutrition, nonexclusive breast-feeding, inadequate sanitation and housing conditions, crowding, mother’s education, and poor nutrition, among others. 51,55 –57 This research used the following 2 variables in composite: at least 1 hospitalization due to diarrhea or pneumonia during the year prior to interview, among children under 5 years. Independent of environmental conditions related to pneumonia and diarrhea, such as macro-region, urban-rural classification, living conditions, economic status, CTP, maternal education, marital status, number of children, sex, age, nutritional status, and nutrition, the multivariate analysis showed that hospitalizations of children under 5 by diarrhea or pneumonia during the year prior to interview were 30% more prevalent in households classified as moderate or severe FI (aPR 1.3; 95% CI 1.1-1.6). This result is consistent with other research 11 finding that children living in food-insecure households were one-third more likely to have a history of hospitalization than their food-secure peers. 11 Food insecurity weakens the immune system, placing children in greater vulnerability to infections. children with FI end up being hospitalized with illnesses that their food-secure peers fight off successfully, either on their own or with basic primary care.
Food insecurity is a broad concept representing an indicator of social vulnerability; but with other variables, it can be used to monitor inequity. 58 It has acquired the status of a public health problem due to its prevalence worldwide and its negative consequences in health. 59
Why Does Food Security Matter for Our Future Prosperity?
Human capital is all the resources embodied and developed in people, including their capacity to learn, develop skills, produce, create, invent, communicate, and expand their knowledge, abilities, and potential. 9 Every child is born with an initial human capital endowment of their own, comprising their genetic material and their parents’ epigenetic transmissions. The first 5 years of a child’s life are critical in determining the potential for human capital formation throughout lifetime. Environment plays an important in shaping it positively or negatively, thereby either increasing the human capital formation or impairing it. 8
Although difficult to establish causality in a cross-sectional study, even with confounding factors controlled, these findings are consistent with the hypothesis that FI is an associated risk factor for the studied problematic outcomes. Underweight, poor feeding, and hospitalizations contribute to the development of children’s brain and body, and they can alter the architecture of developing organs and their functioning, placing severe constraints on future human capital accumulation. 8 If we think of human capital as a stock, and households as producers, parents use their own human capital to enhance their children’s; but when this dynamic is disrupted, caring for an ill child involves missing days of work by caregivers, costs to employers and employees alike, and in worst circumstances, parents losing the job to care for the child, placing the family into a cycle of poverty. 9 Living in a food-insecure household impedes human and socioeconomic development and contributes to the vicious cycle of malnutrition and underdevelopment. Beyond the ethical dimensions of this complex problem, the human, social, and economic costs to the society at large are enormous in terms of lost productivity; health and health-care services; well-being; decreased learning ability; and reduced fulfillment of human potential, and those children are the future of our nations.
Strengths and Limitations
Limitations should be considered when interpreting the study results. The cross-sectional design does not allow one to establish the cause–effect temporal relationships. Although the models were controlled for important confounding variables, other unmeasured confounders may exist. The PNDS questionnaire mainly involves self-reported information, which makes it susceptible to social desirability bias, though this bias would likely occur equally in both food-secure and the food-insecure groups. Since Brazil is a continental country—and most of it is under a tropical climate—the single drop spot of blood used to assess retinol and hemoglobin levels could have suffered alteration in transport and/or storage, leading to overestimation or underestimation. In addition, although the PNDS used a nationally representative sample of Brazil’s children, sample loss may have influenced the representativeness of the sample studied.
Conclusion
Experience-based scales, such as EBIA, correctly identify more vulnerable populations. Therefore, they are instruments used continuously in order to expand the understanding of the complex phenomenon of FI. Results from this 2006/07 population-based cross-sectional nationally representative study indicated 3 key health factors independently associated with children under 5 living in a moderately or severely food-insecure household: hospitalizations for pneumonia or diarrhea, nutritional status, and poor food consumption. If food is important to maintain children’s body systems, and due to the lack of money food becomes poorly available or even unavailable, children’s health will be negatively affected. Children who grow up in moderate or severe food-insecure households have worse health conditions during their childhood, and their human capital accumulation and productivity are likely to be reduced in the future, leading them to become adults less capable of generating sufficient income and avoiding poverty. Thus, the relationship between living conditions and child health, shaped by the environment, may represent an important factor in the transmission of socioeconomic inequality across generations, impacting the future prosperity of a nation. However, since the relationships identified in this study are amenable to social policy solutions, interventions can be implemented to reduce FI, avoid higher public health costs, and prevent the negative impacts on the prosperity of Brazil’s future citizens, whereas more permanent changes in government-supported social infrastructures are consistent with acceptable standards of human dignity.
Footnotes
Authors’ Note
Ana Paula Poblacion was responsible for data set management, interpretation of data, and writing the article. John T. Cook worked on interpretation of data and critically reviewed the article. Ana Maria Segall-Corrêa, Letícia Marín-León, Jonas A.C. Silveira, and Tulio Konstantyner critically reviewed the article. José Augusto A.C. Taddei was responsible for conception and design of the work, interpretation of data, and critical review of the article. All authors approved the final version of the paper to be published.
Acknowledgment
The authors thank for the support from the Brazilian Agency “Coordination for the Improvement of Higher Education Personnel–CAPES” with an international stipend as part of a PhD thesis (process number 15010-13-9). The authors attest that CAPES had no role in the design, analysis, or writing of this article. Special thanks to Children’s HealthWatch for the site support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.