
Abstract
Background:
The question whether diets composed of local foods can meet recommended nutrient intakes in children aged 6 to 23 months living in low- and middle-income countries is contested.
Objective:
To review evidence of studies evaluating whether (1) macro- and micronutrient requirements of children aged 6 to 23 months from low- and middle-income countries are met by the consumption of locally available foods (“observed intake”) and (2) nutrient requirements can be met when the use of local foods is optimized, using modeling techniques (“modeled intake”).
Methods:
Twenty-three articles were included after conducting a systematic literature search. To allow for comparisons between studies, findings of 15 observed intake studies were compared against their contribution to a standardized recommended nutrient intake from complementary foods. For studies with data on intake distribution, %< estimated average requirements were calculated.
Results:
Data from the observed intake studies indicate that children aged 6 to 23 months meet requirements of protein, while diets are inadequate in calcium, iron, and zinc. Also for energy, vitamin A, thiamin, riboflavin, niacin, folate, and vitamin C, children did not always fulfill their requirements. Very few studies reported on vitamin B6, B12, and magnesium, and no conclusions can be drawn for these nutrients. When diets are optimized using modeling techniques, most of these nutrient requirements can be met, with the exception of iron and zinc and in some settings calcium, folate, and B vitamins.
Conclusion:
Our findings suggest that optimizing the use of local foods in diets of children aged 6 to 23 months can improve nutrient intakes; however, additional cost-effective strategies are needed to ensure adequate intakes of iron and zinc.
Keywords
Introduction
Adequate nutrition during infancy and early childhood is fundamental to the development of each child’s full human potential. It is well recognized that the period from conception to 2 years of age is a “critical window” for the promotion of optimal growth, health, and development. 1 The World Health Organization (WHO) recommends that after the age of 6 months, breast-feeding should continue until 24 months of age and beyond, whereas energy- and nutrient-dense complementary foods should be introduced to all infants with an emphasis on the use of suitable locally available foods. 2
The challenge for 6- to 23-month-old children to obtain all of their nutrient requirements from locally available and typically unfortified foods has been discussed previously. 3 The predominantly cereal-based, monotonous diet in low-income countries, resulting in low dietary diversity, low nutrient density, and poor micronutrient bioavailability, is recognized as a main cause. 3 In addition, children aged 6 to 23 months require high amounts of micronutrients to grow and develop, but due to their smaller stomach capacities, they can only consume relatively small volumes of the family diet. However, others have challenged whether special formulated, complementary foods should be consumed at all, recommending a rapid and direct transition to the family-food diet. 4
We performed a systematic literature search of studies investigating whether locally available foods are currently meeting or have the potential to meet the energy, protein, and micronutrient needs of children aged 6 to 23 months and assessed whether this may differ by age subgroup (ie, 6-8, 9-11, 12-23 months of age). All of the reviewed studies addressed the question whether locally available complementary foods (ie, locally available foods or local foods) can satisfy macro- and/or micronutrient needs of young children. Locally available foods were defined as foods available in the household and/or market and consumed by the child, which may or may not include fortified foods, such as fortified cooking oil or fortified commercial infant foods. Most studies aimed to determine whether current dietary intakes from local complementary foods were adequate (referred to as “observed intakes studies”). Other studies included used modeling techniques to optimize intakes based on available or consumed complementary foods within given certain constraints such as constraints on food amounts or frequency of consumption (referred to as “modeled intake studies”).
Methods
Search Strategy
In October 2015, a systematic literature search in the PubMed, Web of Science, and MEDLINE databases was performed using the following search terms: (micronutrient* OR iron OR zinc OR iodine OR vitamin-a OR macronutrient* OR energy OR protein OR fat OR carbohydrate) AND (complement* OR supplement* OR wean*) AND (intake OR consumption OR needs OR requirement) AND (local* OR agricultur* OR traditional* OR household*) AND (infan* OR child*) AND (food* OR diet*) AND (“developing countries” OR “low income countries” OR africa OR asia OR “latin america” OR “south america”). All papers identified by this search were assessed for relevance. Reference sections of the retrieved articles were used to obtain additional articles that were not found by the formal searches.
Study Selection Criteria
Studies focusing on locally available complementary food consumption by children aged 6 to 23 months in Africa, Asia, or Latin America were included. The following references were excluded: (1) studies referring to case reports, commentaries, and in vitro studies; (2) intervention studies focusing on supplementation/supplementary foods or point-of-use or commercial fortification; (3) studies investigating less than 3 micronutrients; (4) studies from before 1998 or studies that used reference values from before 1998, as new guidelines on complementary feeding were published in 1998 5 ; and (5) studies not published in the English language. Where relevant, published reports by nongovernmental organizations based on primary data, identified by gray literature search, were included, provided that this information was accessible to the public. Other unpublished data were excluded.
Titles and abstracts of articles retrieved were screened independently by 3 authors (B.B., E.K., and L.B.) to determine whether they might meet the inclusion criteria. Full-text articles were screened if their inclusion or exclusion could not be determined easily by their titles and abstracts. Differences of opinion about suitability for inclusion were resolved by consultation with a fourth reviewer (S.O.).
Two types of studies were identified: (1) studies reporting on dietary intakes from locally available complementary foods as determined by dietary assessment methods in cross-sectional, case–control, cohort or intervention studies (observed intake studies) and (2) studies investigating theoretical dietary intakes based on locally available complementary foods using modeling techniques to optimize intakes within given (costs) constraints (modeled intake studies).
In the observed intake studies included in this review, “locally available foods” were defined as foods available in the household and consumed by the child, which may or may not include fortified foods, including fortified commercial infant foods and fortified cooking oil. In the modeled intake studies, locally available foods were defined as foods available in the market and/or household or as foods typically consumed by the child as assessed from (national representative) food consumption surveys.
Data Handling and Analytical Strategy
Considering the methodological differences to determine adequacy of dietary intakes from locally available complementary foods between the observed and modeled intake studies, their data were analyzed separately.
Observed Intake Studies
The studies included used various methods and reference values to assess dietary adequacy from local complementary foods. From all studies included, the most commonly used method was to compare the mean or median nutrient intakes from complementary foods to the recommended nutrient intakes (RNIs). 6 –8 However, it is no longer considered appropriate to assess dietary adequacy by comparing absolute nutrient intakes against the RNI because the prevalence of inadequacy depends on the shape and variation in the usual intake distribution and not on the mean or median intakes. 7 Instead, adequacy of dietary intakes should be evaluated against the estimated average requirements (EARs) by calculating the proportion of the population with intakes below the EAR using the EAR cut-point method. The EAR cut-point method assumes that the proportion of a population with intakes below the EAR for a given nutrient corresponds to the population having an inadequate intake for that nutrient. 9,10
To allow for comparisons between the observed intake studies and in order to standardize the reporting of findings, we aligned the methods used to assess dietary adequacy of the individual studies as follows: first, the proportion of children at risk of inadequate intakes for specific nutrients was estimated using the EAR cut-point method. The EARs 7,10 –16 were corrected for breast-milk intake (EAR-CF) to define the EAR from complementary foods, as follows: the EARs of protein and micronutrients required from complementary foods were estimated by subtracting the amounts provided by human milk from the EAR for each of the age intervals following the method as described by WHO and Dewey and Brown. 5,17 Using the mean and standard deviation (SD) of nutrient intakes (ie, assuming normal distribution), the area under the curve below the EAR-CF was determined, representing the population proportion at risk of inadequate intakes for a given nutrient. 9 Unfortunately, not all studies reported mean and distribution of intakes, and an EAR has not been established for all nutrients and age-groups, particularly not for children aged 6 to 11 months, and it was therefore not possible to calculate the %<EAR-CF for all studies. In order to compare the findings of all observed intake studies, the estimated nutrient requirements from complementary foods as defined by Lutter and Dewey 18 were used as standardized reference dietary intake (RDI) values. All observed dietary intakes as reported were compared to these standardized reference values. The reported observed dietary intakes from local foods were expressed as percentage of the RNI corrected for mean breast-milk intakes and breast-milk nutrient composition as defined by WHO 5 and Dewey and Brown 17 (%RNI-CF). For iron and zinc, RNIs for diets with medium bioavailability were used. Reference intake values used for all comparisons are presented in Table 1. We did not attempt to meta-analyze the observed intake studies because an average estimate would have masked the heterogeneity in terms of age-groups, geography, sampling, and analytical methods. Thus, the results of the observed intake studies are presented individually.
Standardized Reference Values for Dietary Intake Corrected for Breast-Milk Intake Used for Standardization of Results of the Observed Intake Studies.
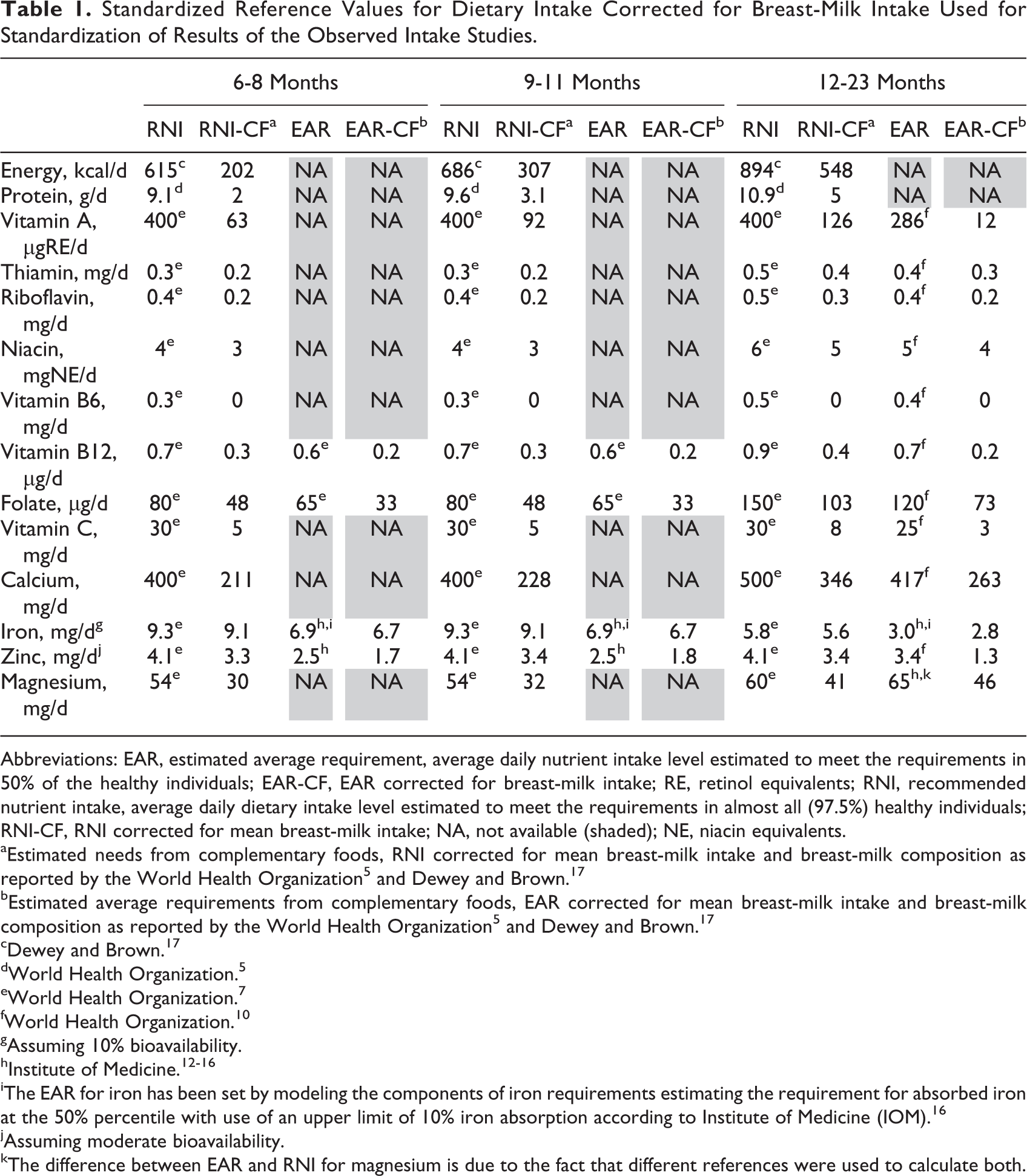
Abbreviations: EAR, estimated average requirement, average daily nutrient intake level estimated to meet the requirements in 50% of the healthy individuals; EAR-CF, EAR corrected for breast-milk intake; RE, retinol equivalents; RNI, recommended nutrient intake, average daily dietary intake level estimated to meet the requirements in almost all (97.5%) healthy individuals; RNI-CF, RNI corrected for mean breast-milk intake; NA, not available (shaded); NE, niacin equivalents.
aEstimated needs from complementary foods, RNI corrected for mean breast-milk intake and breast-milk composition as reported by the World Health Organization 5 and Dewey and Brown. 17
bEstimated average requirements from complementary foods, EAR corrected for mean breast-milk intake and breast-milk composition as reported by the World Health Organization 5 and Dewey and Brown. 17
cDewey and Brown. 17
dWorld Health Organization. 5
eWorld Health Organization. 7
fWorld Health Organization. 10
gAssuming 10% bioavailability.
iThe EAR for iron has been set by modeling the components of iron requirements estimating the requirement for absorbed iron at the 50% percentile with use of an upper limit of 10% iron absorption according to Institute of Medicine (IOM). 16
jAssuming moderate bioavailability.
kThe difference between EAR and RNI for magnesium is due to the fact that different references were used to calculate both.
Modeled Intake Studies
The modeled intake studies modeled theoretical intakes or nutrient densities against recommended intakes or nutrient densities. Six 19 –24 of the modeled intake studies used linear programming, a mathematical tool, that can be used among others to formulate optimized complementary feeding diets, which resemble current dietary practices as closely as possible while at the same time ensuring optimal nutrient intakes. 25 Details of the linear programming process and its challenges have been described before. 26 Santika et al, 20 Skau et al, 19 and Fahmida et al 21 used the linear programming software Optifood 25,26 and reported findings based on best-case scenarios (ie, maximizing nutrient content of the diets selecting high nutrient-dense foods) and worst-case scenarios (ie, optimizing nutrient content, selecting foods with the lowest nutrient density). Optimized scenarios (the nutritionally best model, optimizing all nutrient intakes simultaneously) were reported as well. All models were based on frequently consumed foods and take into account constraints such as diet’s energy content, food consumption frequency patterns, food portion sizes, and costs. Wu et al 22 created nutritious food combinations using the ProPAN tool. Adrianopoli et al 23 used NutriSurvey as linear modeling tool and optimized intakes using different combinations of food amount constraints. Vita and Dewey 24 used Microsoft Excel as linear modeling tool and modeled scenarios with and without constraints on type of foods consumed (ie, minimum quantity from staple foods and/or minimum consumption from 5 food groups).
Two of the modeled intake studies 27,28 did not use linear programming but modeled observed nutrient densities of best-case scenario diets (ie, diets meeting nutrient adequacy) to meet nutrient and nutrient density requirements of children aged 6 to 23 months using assumptions for energy, protein, and nutrient requirements. The results of the modeled intake studies are presented individually because of the limited number of studies found.
Results
In total, 536 records were identified by PubMed (n = 279), Web of Science (n = 115), and MEDLINE (n = 143) after conducting the systematic search. Since the records retrieved from MEDLINE were mostly duplicates of the records identified by the other 2 databases, only the first 30 MEDLINE records were screened. Thirty-four references were added for review through scanning secondary references (“own search”). In total, 119 articles were selected as being relevant for further review, of which finally 23 articles were included; 15 studies reported observed dietary intakes, whereas 8 studies described modeled intakes. A flowchart describing the study selection process and reasons for exclusion is presented in Figure 1.
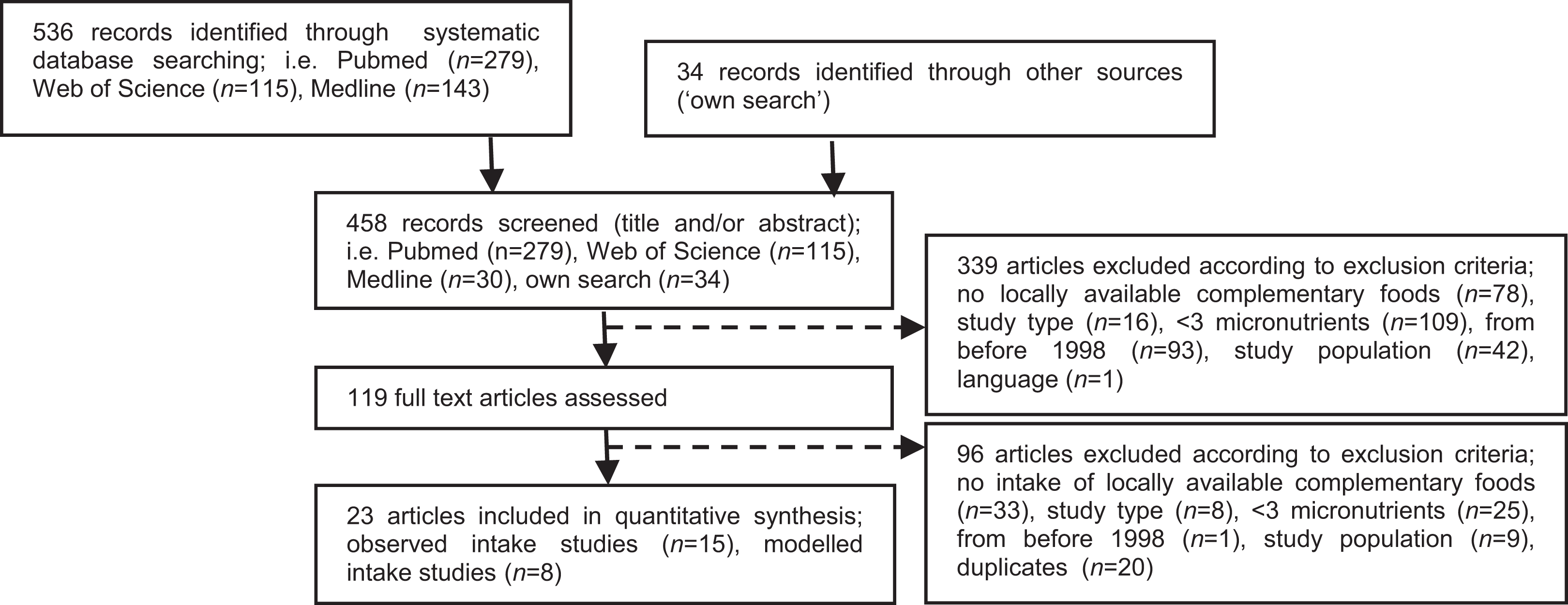
Study selection process.
Fourteen of the 15 observed intake studies reported absolute dietary intakes from complementary foods per day as median and interquartile range (n = 9) or mean and SD (n = 5). One study reported total dietary intake (mean, SD), that is, intake from breast-milk consumption and complementary foods. 23 In 11 of the observed intake studies, 29 –39 all children were (partially) breast-fed, whereas in 3 23,40,41 of the studies, more than 80% of children were breast-fed. For all these studies, nutrient intakes were compared against RNI and EAR corrected for average breast-milk intakes (%RNI-CF and %EAR-CF). In 1 study, 42 41 infants were reported to be partially breast-fed, whereas 210 infants were non–breast-fed. For this study, the RNI and EAR uncorrected for breast-milk intakes were used for the comparisons. The 15 observed intake studies reported findings for at least one of the following age subgroups: 6 to 8 months (n = 10), 9 to 11 months (n = 12), 6 to 12 months (n = 1), and 12 to 23 months (n = 9). Three of the observed intake studies, 2 from Latin America 32,33 and 1 from South Africa, 40 reported the use of fortified (commercial) infant foods in the study population. The other observed intake studies did not mention any consumption of fortified foods. With regard to the 8 modeled intake studies, only 1 study reported dietary intakes from complementary foods together with the intakes as %RDI, 23 4 studies reported nutrient intakes as %RNI, 19,20,23,24 2 studies identified nutrient density gaps, 27,28 and 1 study reported only on problem nutrients defined as <100% RNI in the nutritionally best linear programming model. 21 Table 2 gives an overview of the characteristics of the 23 studies included.
Characteristics of the Included Studies: Observed Intake Studies (n = 15) and Modeled Intake Studies (n = 7).
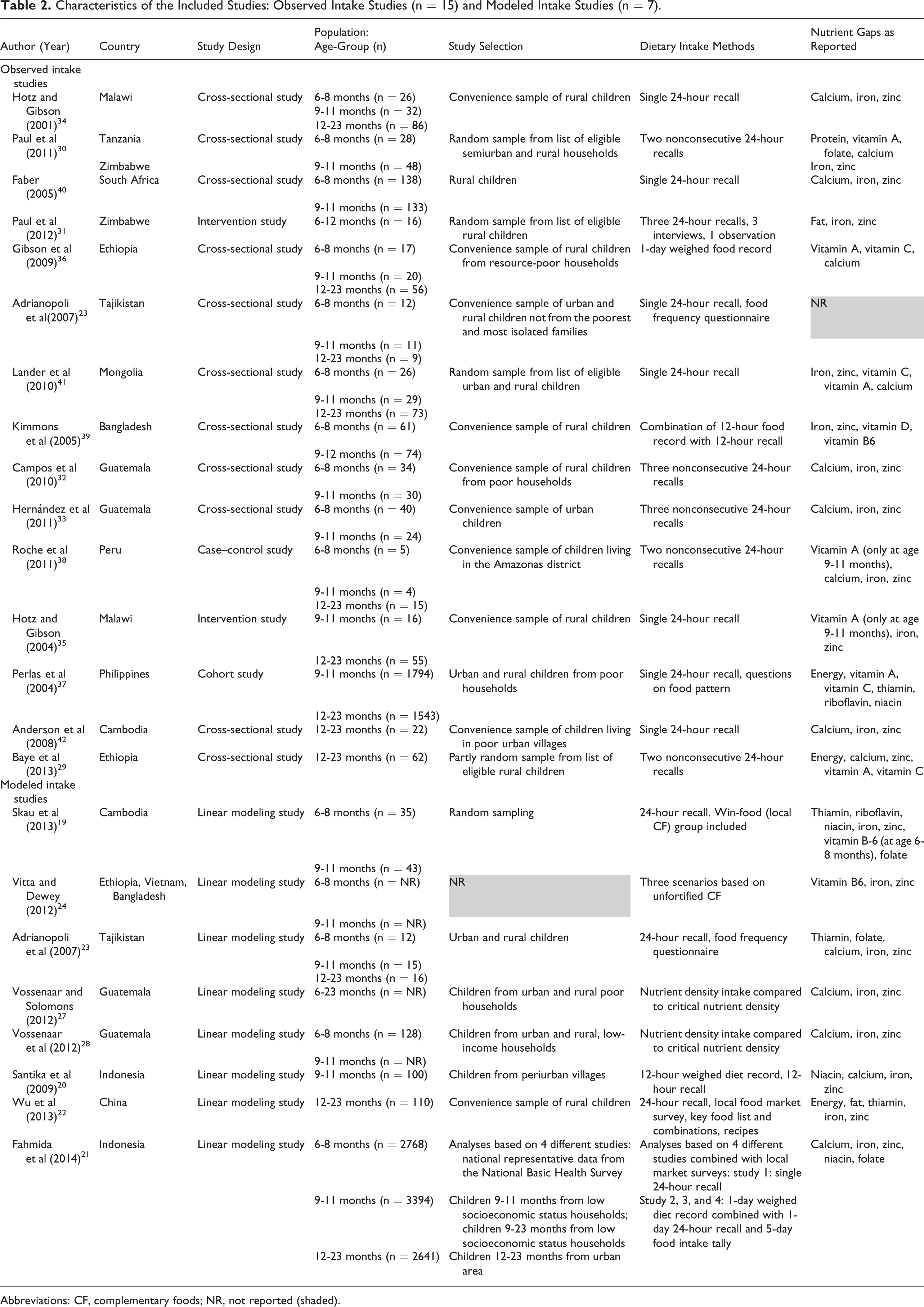
Abbreviations: CF, complementary foods; NR, not reported (shaded).
Observed Dietary Intakes From Locally Available Complementary Foods
An overview of the results as reported in the observed intake studies is presented in Table 3. This table includes intakes as %RNI as reported by the investigators, using various methods and reference values to assess dietary adequacy. The calculated %RNI-CF and %<EAR-CF using standardized reference values as described in Table 1 using data from the 15 observed intake studies are presented by age-group in Table 4.
Reported Findings of Observed Intake Studies on Nutrient Adequacy From Complementary Foods in Breast-Fed Children Aged 6 to 23 Months, Nutrient Density, and Reported Intake as Percentage of Recommended Nutrient Intake by the Studies Included.
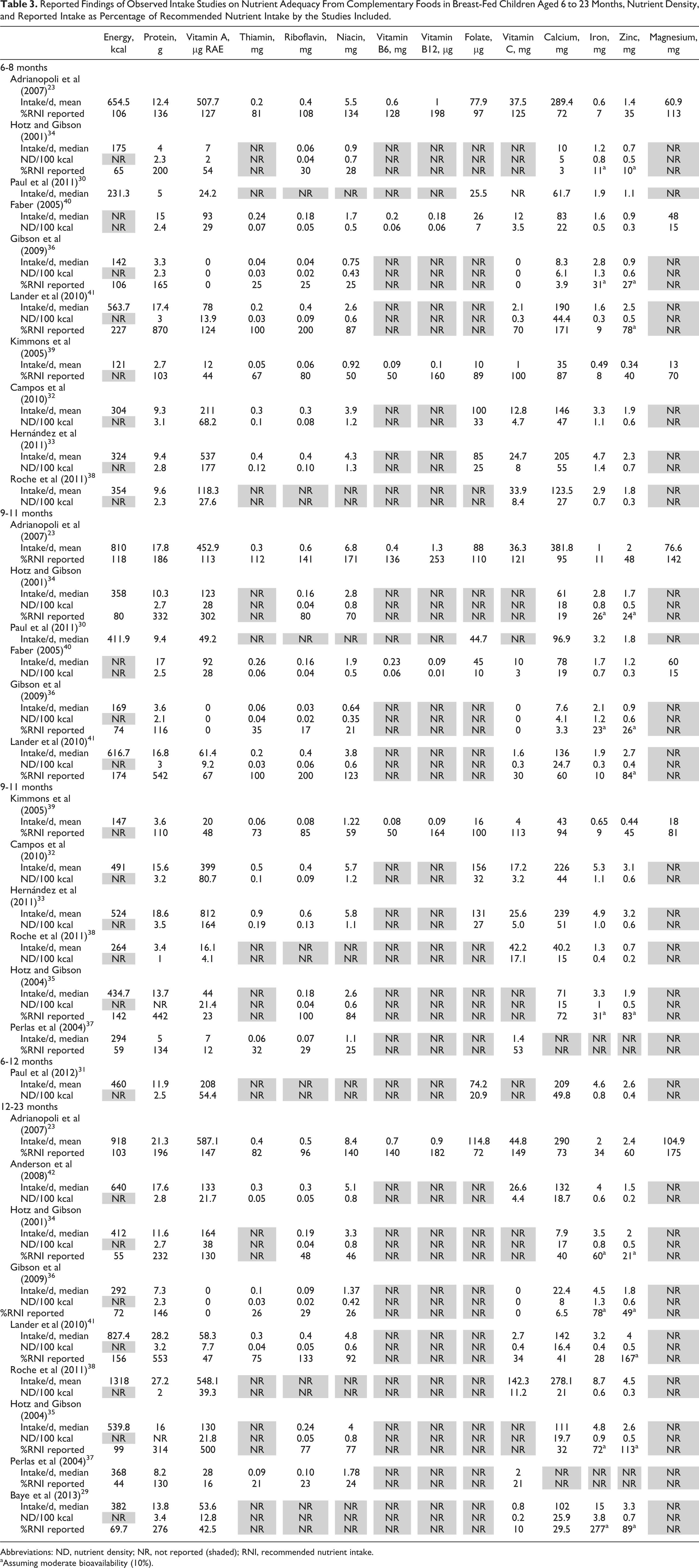
Abbreviations: ND, nutrient density; NR, not reported (shaded); RNI, recommended nutrient intake.
aAssuming moderate bioavailability (10%).
Standardized Estimates of Dietary Adequacy From Local Foods as Percentage of the Estimated Needs and the Percentage at Risk of Inadequate Intakes, by Age-Group—Results of Observed Intake Studies.
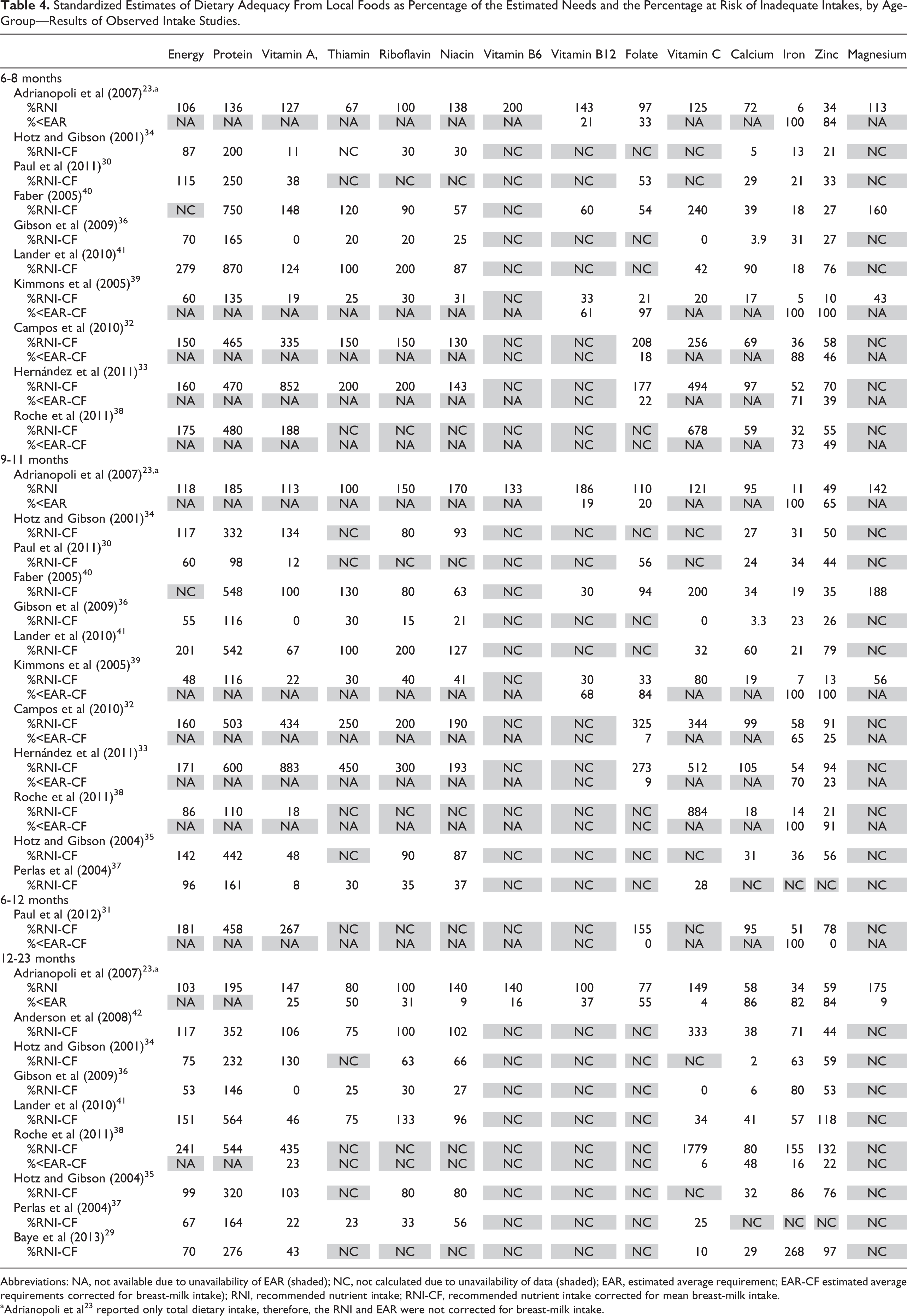
Abbreviations: NA, not available due to unavailability of EAR (shaded); NC, not calculated due to unavailability of data (shaded); EAR, estimated average requirement; EAR-CF estimated average requirements corrected for breast-milk intake); RNI, recommended nutrient intake; RNI-CF, recommended nutrient intake corrected for mean breast-milk intake.
aAdrianopoli et al 23 reported only total dietary intake, therefore, the RNI and EAR were not corrected for breast-milk intake.
Protein requirements were met with local complementary foods, since the standardized %RNI-CF was close to or above 100% in all studies that evaluated protein. An overview of the calculated %RNI-CF per study and age-group for protein is presented in Figure 2A. In contrast, diets based on local foods were generally not adequate in calcium, iron, and zinc. Figure 2B gives an overview of the calculated %RNI-CF per study and age-group for iron as an illustration of a nutrient for which, in general, inadequate intakes were reported. For the other nutrients investigated, that is, energy, vitamin A, thiamin, riboflavin, niacin, folate, and vitamin C, adequate intakes were reported in some studies but not in others. Figure 2C gives an overview of the calculated %RNI-CF per study and age-group for vitamin A, as an illustration of a nutrient for which the findings on dietary adequacy were inconsistent across studies. Very few studies reported vitamin B6 intakes (1 study, for all age-groups 23 ), vitamin B12, and magnesium (1 study for all age-groups, 23 1 study for 2 age-groups 39 ), and no conclusions can be drawn therefore on dietary adequacy for these nutrients based on the observed intake studies.
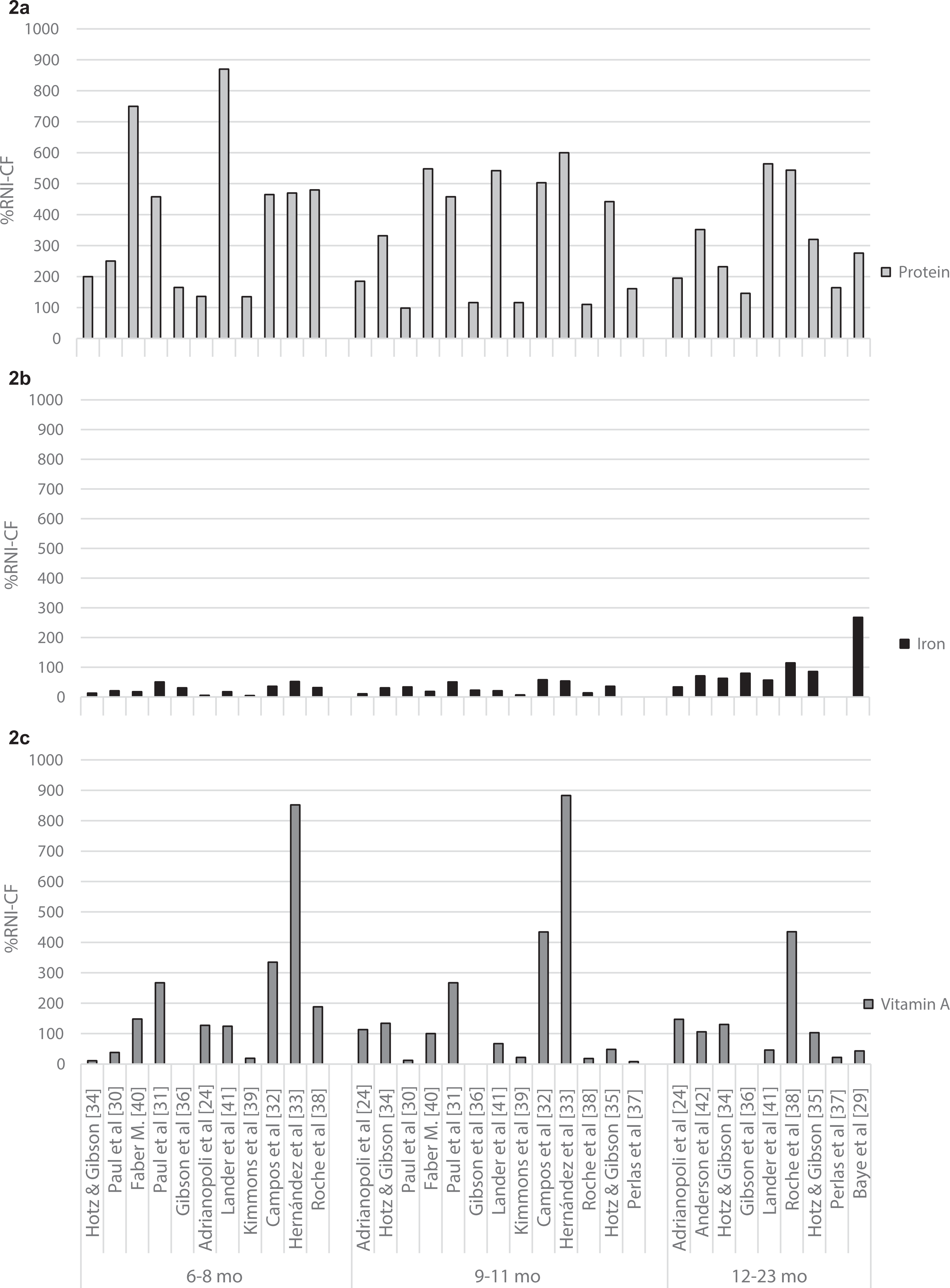
Mean or median protein (2a), iron (2b), and vitamin A (2c) intakes from locally available foods as reported in the observed intake studies, compared to the RNI from complementary foods (%RNI-CF) for children aged 6 to 8, 9 to 11, and 12 to 23 months. Y-axis represent mean intakes as percentage of the RNI-CF; x-axis represent the findings of the included observed intake studies for 3 age subgroups.
Results by Age Subgroups
The findings of the observed intake studies indicated calcium, iron, and zinc as the nutrients of concern for children aged 6 to 11 months. The highest %RNI-CF in children aged 6 to 8 months did not reach 100% for calcium (97%), iron (52%), and zinc (78%), indicating that for these nutrients none of the included studies reported intakes were reaching the estimated needs. The maximum %RNI-CF in children aged 9 to 11 months did not reach 100% for iron (58%) and zinc (94%). Only 1 of the 12 studies found a %RNI-CF slightly above 100% (ie, 105%) for calcium in children aged 9 to 11 months. 33 Six of 8 studies in children aged 12 to 23 months also reported %RNI-CF for iron and zinc below 100%. The fact that 2 studies 38,41 in this age subgroup reported no intake gaps for these 2 nutrients seems to suggest that meeting iron and zinc requirements from local foods can improve with age. The maximum %RNI-CF was equal or smaller than 80% for thiamine (reported by 5 of the 9 studies in this age-group), 77% for folate (reported by only 1 of the 9 studies), and equal or smaller than 80% for calcium (reported by 8 of the 9 studies) in children aged 12 to 23 months, suggesting that the requirements of these nutrients may be difficult to achieve in this age-group.
Children aged 6 to 11 months were meeting the estimated requirements for protein in all studies. Vitamin B6 intakes were adequate in the 1 study 23 reporting on this nutrient for this age-group. Children aged 12 to 23 months were meeting the estimated needs from local complementary foods for protein in all 9 studies that reported data for this age-group. Intakes of vitamin B6, vitamin B12, and magnesium were meeting the estimated requirements in the one study that reported on intakes for these nutrients.
For children aged 6 to 8 months and 9 to 11 months, dietary inadequacy, determined by the %<EAR-CF, could only be calculated for iron, zinc, vitamin B12, and folate, since no EARs have been established for the other nutrients for these age-groups. Dietary inadequacy was generally high for both iron and zinc among all 3 age-groups. For children aged 6 to 8 months, the %<EAR-CF for iron ranged from 71% to 100% and for zinc from 0% to 100%. Moreover, all 6 studies presenting findings for the 2 youngest age-groups (6-8 and 9-11 months) reported a %<EAR-CF higher than 50% for iron. Two of the 6 studies reported a %<EAR-CF higher than 50% for zinc in this age-group. For children aged 9 to 11 months, the %<EAR-CF for iron ranged from 65% to 100% and for zinc from 0% to 100%. Again, all 6 studies reported a %<EAR-CF higher than 50% for iron and 3 of the 6 for zinc in children aged 9 to 11 months. In addition to inadequate iron and zinc intakes, children aged 12 to 23 months were at risk of inadequate calcium intakes, ranging from 48 to 66 %<EAR-CF. Information on dietary adequacy for calcium was not available for the younger children (6-11 months) due to the lack of an established EAR for calcium for these age-groups.
Modeled Dietary Intakes From Locally Available Complementary Foods
The results reported by the 8 studies that investigated modeled dietary intakes from locally available complementary foods are presented in Table 5.
Summary of the Reported Findings by the Included Modeled Intake Studies.a
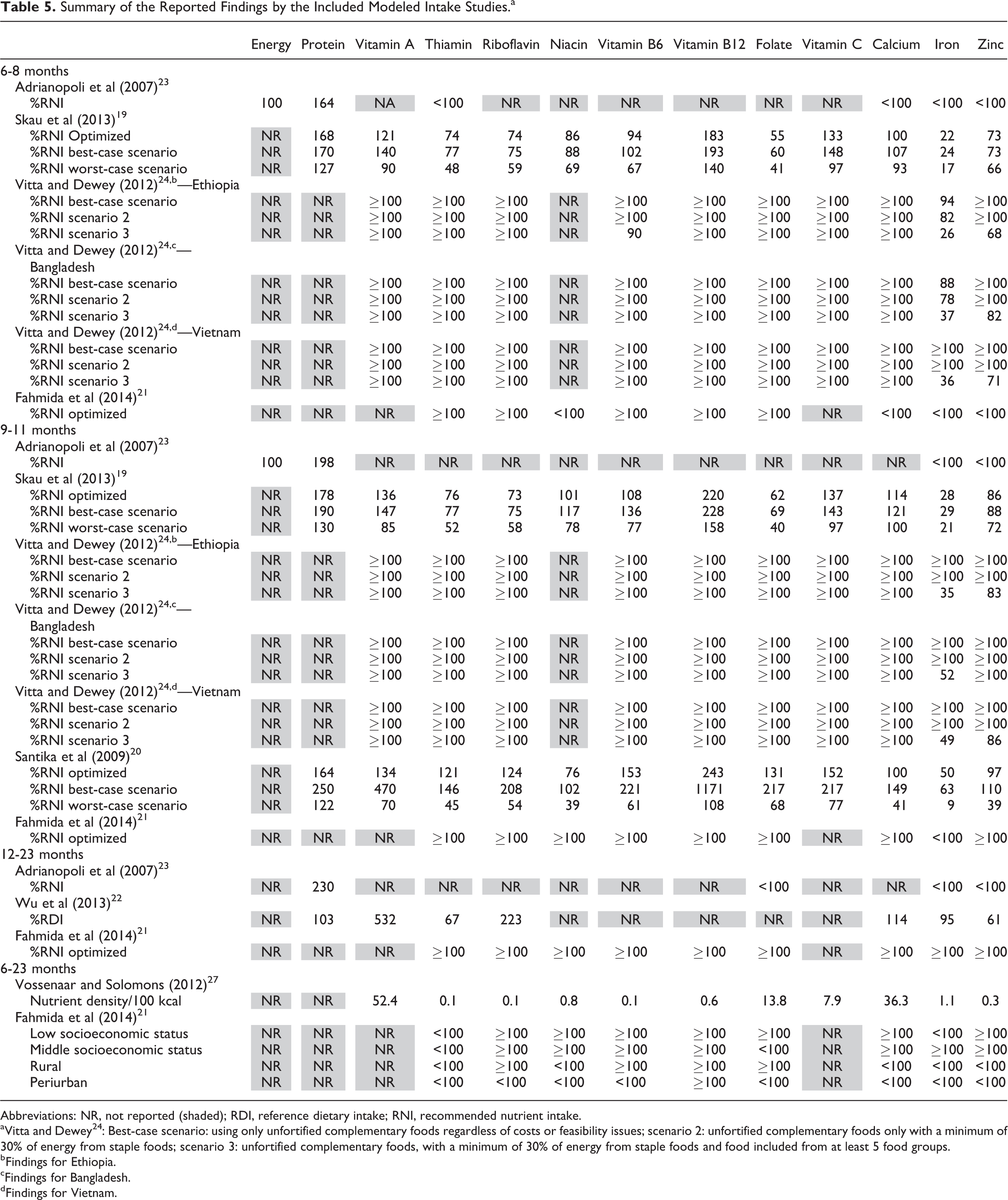
Abbreviations: NR, not reported (shaded); RDI, reference dietary intake; RNI, recommended nutrient intake.
aVitta and Dewey 24 : Best-case scenario: using only unfortified complementary foods regardless of costs or feasibility issues; scenario 2: unfortified complementary foods only with a minimum of 30% of energy from staple foods; scenario 3: unfortified complementary foods, with a minimum of 30% of energy from staple foods and food included from at least 5 food groups.
bFindings for Ethiopia.
cFindings for Bangladesh.
dFindings for Vietnam.
Overall, modeled dietary intakes from locally available complementary foods were adequate in all scenarios for protein and vitamin B12. Vitta and Dewey 24 did not identify any nutrient gaps in some best-case scenarios that were based on daily chicken liver consumption, for example, in children aged 9- to 11-months-old. The other 7 studies identified several nutrients gaps, even when dietary intakes were based on a best-case scenario. Among all age subgroups, modeled dietary intakes for iron and zinc were most frequently inadequate when compared to the RNI. Moreover, intake of B vitamins (ie, thiamin, riboflavin, niacin, and folate) and calcium was inadequate in most but not all studies and age-groups. Intakes of vitamin A and vitamin C was mostly adequate based on the best-case and optimized scenarios. However, when intakes of vitamin A and vitamin C were based on a worst-case scenario, they were inadequate (Table 5). Nutrient intake gaps remained for calcium, iron, and zinc (Table 5).
Discussion
It is generally recognized that, in practice, locally available foods do not meet requirements, especially for micronutrients, in most low-income countries and that this contributes to micronutrient deficiencies, growth faltering, and poorer child development during the first 2 years of life, 1 with potential adverse consequences for child health and development and later adult health. 43 The question whether these nutrient gaps can be filled by optimizing the intake of locally available foods has been a topic of debate. Our review provides an up-to-date analysis of the existing, published data, not only of the evidence on observed intakes but also of the potential of local foods to meet all nutrient requirements when diets are optimized through modeling with the use of locally available ingredients.
The findings of the observed intake studies included in this review indicate that diets consisting of locally available complementary foods alone are meeting requirements for protein for children 6 to 23 months of age. The nutrients most commonly inadequate and with the greatest gaps were calcium, iron, and zinc. Also for energy, vitamin A, thiamin, riboflavin, niacin, folate, and vitamin C, children did not always fulfill daily requirements with local foods. Only 2 of the observed intake studies reported on vitamin B6, vitamin B12, and magnesium, and therefore, no conclusions can be drawn on observed intakes for these nutrients based on this review. Optimizing food preparation techniques, for instance, by promotion of soaking techniques to reduce phytate content of a maize diet 35 or by promoting the processing of local foods so that infants could swallow them, 31 improved dietary intakes, but requirements for iron, zinc, and in some cases calcium were still not met. When modeling is used to optimize diets by increasing feeding frequencies or quantities of nutrient-dense foods, most of the nutrient requirements can be met, with the exception of iron and zinc. In some modeled intake studies, adequate intakes for calcium, thiamin, riboflavin, niacin, and folate were also difficult to reach. Our findings are consistent with those of previous reviews 3,5 in which calcium, iron, and zinc were identified as the most critical “problem nutrients” in the diets of children 6 to 23 months of age. In addition, the results of this review suggest that even when use of local ingredients is optimized, and despite the fact that intakes improve when diets are optimized, dietary adequacy for iron and zinc in particular cannot be met across age-groups and across different settings.
While interpreting these findings, several methodological constraints of our review have to be acknowledged. First, the %RNI-CF likely underestimates the actual contribution of complementary foods to the requirements of an individual, since RNIs are defined to cover the nutritional needs of 97.5% of the total population. In addition, our calculated %<EAR-CF was based on reported mean and SD of intakes, assuming that authors would only report SDs when intakes were normally distributed, which may not always have been the case.
In at least 3 of the 15 observed intake studies, diets made of locally available foods included the consumption of (commercial) fortified infant foods or Incaparina. 32,33,40 Faber 40 concluded that infants who consumed fortified infant products and fortified formula milk had significantly higher intakes of nutrients such as vitamin A, calcium, iron, and zinc, compared to infants who did not consume these products. However, even with consumption of fortified infant products, intakes were still inadequate for iron, due to inadequate nutrient densities of fortified infant foods, small quantities consumed and/or infrequent consumption of these products.
In addition to these methodological constraints, the total number of studies found was limited, and not all observed intake studies evaluated all nutrients for all the different age-groups. In particular, intakes of vitamin B6, B12, and magnesium were infrequently reported. For instance, only 2 studies reported on vitamin B6 intakes for 3 age-groups, and thus, no conclusions can be drawn on adequacy of observed intakes for these 3 nutrients.
The restriction to studies published in English language, the small sample size in some of the observed intake studies, 23,31,38,42 and the fact that some studies sampled deliberately children from rural 22,29,31,32,34 –36,39,40 and/or poor communities 27,28,32,37,42 may raise questions on how representative the data from the observed intake studies are for usual dietary intakes of children in that specific country or region. In addition, the quality of some of the observed intake studies can be questioned since dietary assessment methods are generally recognized to be prone to biases. Several of the observed intake studies used single 24-hour recalls 23,34,37,39 –42 and compared to recommended energy intakes from complementary foods as defined by Dewey and Brown, 17 some relatively high energy intakes from complementary foods were reported, for instance 1318 kcal for children aged 12 to 23 months 38 and 565 kcal for children aged 6 to 8 months. 41 The energy intake from complementary food in the latter study may reflect low mean breast-milk energy intake or may be related to overestimation from the single recall. The modeled intake studies typically included data from larger sample sizes and, in some cases, data from national representative dietary intake surveys and are therefore considered to be less prone to selection bias. However, there may have been publication bias toward reporting inadequate intakes for the modeled intake studies. In general, the question whether local complementary foods can in principle meet dietary requirements can best be answered by the modeled intake studies that model optimal diets using local foods. However, we only found 8 of these modeled intake studies.
Despite these methodological limitations, the findings on dietary inadequacy of the individual nutrients are remarkably consistent across the individual studies, representing different geographical and socioeconomic settings. This suggests that methodological constraints may have affected the individual estimates of the size of the dietary intake gaps but not the overall conclusion of this review that diets based on locally available complementary foods, even when optimized are not adequate to meet requirements of certain micronutrients and especially not for iron and zinc. The consistency of these findings with previous publications 3,5 provides further support for this conclusion.
The studies included in this review focused on evaluating intakes of energy, protein, and the most commonly reported and often deficient micronutrients. While most observed intake studies reported total daily energy intakes, only 2 of these studies 34,35 provided information on energy densities of the foods consumed. Low-energy density of local complementary foods is a major limitation for young children in low- and middle-income countries to meet daily energy requirements. Minimum energy densities for complementary foods have been recommended taking into account age-appropriate feeding frequencies and gastric capacities of young children. 17 The theoretical intake studies by definition modeled nutrient intakes assuming daily energy intakes equal to the average energy requirement for the age subgroup. 26
None of the studies took protein quality into account, and there were no data available on fat or essential fatty acids intake, despite the growing body of evidence on the importance of essential fatty acids for infant and young child’s growth and development. 44,45 In addition, surprisingly, none of the studies included in this review presented data on iodine intakes perhaps due to methodology issues with reliably estimating iodine intakes from foods and condiments. In Europe, several studies reported lower than recommended iodine intakes or low urinary iodine concentrations in infants receiving home-prepared complementary foods compared to those receiving iodine-fortified commercial infant foods, 46,47 whereas compared to other micronutrient deficiencies, iodine deficiency is common in Europe. 47
In many of the populations evaluated in studies included in this review, children were either moderately malnourished or at risk of becoming so. Dietary reference values used may underestimate the actual requirements for optimal growth and development of malnourished children. The RNIs and EARs for micronutrients are based on requirements of healthy children. 6 –8,12,14 –16 The October 2008 consultation on moderate malnutrition reported that “the nutritional requirements of moderately malnourished children probably fall somewhere between the nutritional requirements for healthy children and those of children with severe acute malnutrition during the catch up growth phase.” 48(pS465) A study of malnourished children aged 3 to 6 years that showed positive impacts on linear growth used between 1.5 and 3 times the RNI for most micronutrients delivered in a fortified spread. 49 A study by Vossenaar and Solomons 27 was the only study included in this review where the authors modeled intakes separately against requirements for a hypothetical moderate malnourished girl (growing at the 15th percentile) and a normal weight boy (growing at the 50th percentile). Due to the larger body size and subsequent larger volumes of breast milk and food intakes, the diet of the normal weight boy had the most adequate intakes, whereas the diet of the underweight girl was inadequate for 8 of 10 nutrients examined. The authors concluded that the diet of the underweight girl was likely to be inadequate in more nutrients compared to the diet of the normal weight boy who could consume larger volumes of breast milk and food due to his larger body size. 27
The findings of the 8 modeled intake studies included in this review suggest that the quality of diets can be substantially improved. Increasing the quantity or feeding frequency of nutrient-dense foods in the diet 19 –24 and introducing new nutrient-rich foods 24 or food supplements 23,24 can partly overcome the nutrient gaps for many micronutrients, particularly in older children and in food secure environments. 42 Vitta and Dewey 24 concluded that diets made of local foods, available on the market, could theoretically meet all of the nutrient requirements, with the exception of iron. However, feasibility to prepare such diets was considered low, since they were about 3 to 8 times more expensive than diets that included micronutrient supplements, or because it would require the daily use of chicken liver, which is not traditionally given to young children in many settings. 24 In contrast, Adrianopoli et al, 23 Wu et al, 22 Skau et al, 19 Santika et al, 20 and Fahmida et al 21 modeled diets based on foods actually being provided and consumed by children and concluded that optimized diets made of these foods, within constraints for feeding frequency and food quantities, could not fulfill requirements for iron and zinc in all cases and, in some settings, for other micronutrients (calcium, folate, B vitamins) as well. Dietary adequacy for these nutrients was only reached when fortified foods or home fortificants such as micronutrient powders (MNPs) or small-quantity lipid-based nutrient supplements (sq-LNS) were added to the model. 19 Analyses using the cost-of-diet tool or a similar programming tool modeling costs in countries including Bangladesh, Kenya, Nigeria, Mozambique, Indonesia, and Nepal confirmed that theoretical optimized diets (ie, those that are able to fill all nutrient requirements) based on local available foods may be too expensive for most households. 50 –54 One of these studies, evaluating the cost of nutritionally adequate diets for an average household size in Mozambique, suggests that multiple micronutrient fortification of maize flour could reduce the cost of the nutritious diet covering the combined nutritional needs of all members of an average household size by 18%. 51 When linear programming was used in Mozambique to formulate a nutritious porridge for children 12 to 24 months of age, with acceptable consistency using local ingredients only, the costs of this porridge were unacceptably high (US$1.85/day) for rural families within a tight budget. In this study, zinc in particular was identified as an economically limiting nutrient, suggesting that it would not be possible to reduce zinc deficiency by dietary changes in this setting without significantly increasing the costs of the foods consumed. 55
The challenge of meeting the nutrient requirements for iron and zinc in the diets of young children has been discussed before 3 and is hypothesized to originate, at least in part, from the introduction of primarily cereal-based diets after the agricultural revolution, 10 000 years ago. Estimates of nutrient intakes before then, based on hypothetical diets of preagricultural humans, suggest that infants had much higher intakes of key nutrients than is true today and would have been able to meet their nutrient needs from the combination of breast milk and premasticated foods provided by their mothers. 3
In summary, the findings of this review indicate that children aged 6 to 23 months are currently not meeting requirements for iron, zinc, and calcium with locally available foods, even in the 3 studies that reported the consumption of fortified infant products as part of the local diet. Optimizing the utilization of local foods by increasing frequency and quantity of nutrient-dense foods will improve intakes of these nutrients but is unlikely to fully cover requirements of iron and zinc. Also for energy, calcium, vitamin A, thiamin, riboflavin, niacin, folate, and vitamin C, children were not always able to fulfill daily requirements with locally available foods.
Our findings show that more effective behavioral change strategies to optimize the use of locally available foods can contribute to improved intakes and better meet the nutrient requirements of young children during this critical period of life. However, even when the use of local ingredients is optimized, in most settings, additional cost-effective strategies are required to ensure adequate intakes of iron and zinc, and in some contexts, this applies to calcium, folate, thiamin, riboflavin, and niacin as well. These cost-effective strategies may include enhancing the local availability of affordable and appropriately fortified infant food products or home fortificants such as MNPs or sq-LNS.
Footnotes
Authors’ Note
S.J.M.O., M.J.v.L., L.M.N., and L.d.R. designed the research. S.J.M.O., B.B., L.B., and E.K. conducted the review and analyzed the data. S.J.M.O. and B.B. wrote the paper. S.J.M.O. had final responsibility of the content. All authors have read, provided input, and approved the final manuscript.
Acknowledgments
The authors would like to thank the following students from the University of Waterloo Masters of Public Health Program for their contribution to this work: Wajma Attayi, Ace Cheung, Gogi Greely, Eugene Jeong, Nina Jetha, and Rebecca Kolstee.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: L.d.R is a full-time staff of The Micronutrient Initiative (MI), an international nongovernment organization that implements complementary feeding programs and research projects in children 6 to 23 months.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research described in this report was supported by the Micronutrient Initiative and the Global Alliance for Improved Nutrition (GAIN).