
Abstract
Background:
Despite the nationwide micronutrient powder (MNP) supplementation, the Philippines only saw limited success in reducing the prevalence of anemia—a condition that has remained a public health concern among young children.
Objective:
To assess and explore the acceptability and compliance to MNP and Bigas-Mongo (BigMo) complementary food blend among mothers/caregivers of children aged 6 to 23 months and the promotion of these products by community health workers (CHWs).
Methods:
This study was part of the randomized controlled trial involving 3 methods of data collection: (1) bimonthly visits to mothers and caregivers for 6 months to determine the level of acceptability and compliance of the 4 intervention groups; (2) initial and final interviews with mothers/caregivers (initial = 141; final = 130) to gather their experiences and difficulties in MNP and BigMo preparation and feeding; and (3) focus group discussion (n = 4) among CHWs (n = 13) to understand their perceptions and difficulties in promoting MNP and BigMo.
Results:
The overall compliance to MNP consumption was 74.7%, with some difference between the groups. Analysis of the information received from mothers/caregivers showed that maternal adaptive strategies in preparing and feeding MNP to their children could affect MNP use, while nonreceptiveness of mothers to integrating MNP into the child’s feeding routine, perceived side effects, and perceived unfavorable taste and smell were key factors considered to limit MNP use.
Conclusion:
This study provides insights into MNP and BigMo acceptability and compliance by mothers and their promotion by CHWs, which may be useful in improving MNP program and complementary feeding projects and programs in similar settings.
Keywords
Introduction
Philippines is a country in Southeast Asia with a long-standing problem of anemia and other micronutrient deficiencies affecting most infants and young children. Anemia is most prevalent among infants 6 months to <1 year old (39.4%), followed by 1-year-olds (24.6%) and 2-year-olds (14.0%); cases are remarkably highest in the poorest income group commonly residing in rural areas. 1 Iron deficiency is believed to be the main contributing factor in about half of cases 2,3 with anemia because of limited access to micronutrient-rich foods from animal sources, especially in poor households.
Because micronutrient deficiencies pose many adverse effects on physical growth and mental development of infants and young children, several strategies to address these deficiencies were designed and implemented.
Provision of multiple micronutrients through micronutrient powders (MNPs) has been described as an effective way in combating childhood and infant micronutrient deficiencies based on Cochrane systematic review. 4 The MNP has been considered a “home” or “point-of-use” food fortification using a single-dose sachet, which typically contains iron, zinc, vitamin A, and other micronutrients in powder form, sprinkled over any prepared food.
In 2009, the Philippine government, in partnership with the World Food Program and DSM Nutritional Products, had initiated the MNP supplementation pilot program called “Improving Nutrition-Improving Lives” as an emergency response to the aftermath of typhoons Ketsana and Parma in Central Luzon. 5 This initial MNP experience paved the way for the Department of Health to implement, through Memorandum No. 2011-0303, the home fortification of complementary food using MNP for all children 6 to 23 months old. This MNP home fortification has been a part of the national strategy to prevent anemia and micronutrient deficiency. 6 However, despite this movement since 2011, anemia has remained a serious public health concern, affecting significant number of infants and young children.
Effectiveness of MNP in enriching the complementary foods of young children largely depends on the acceptability and compliance by the target population. 4 A recent systematic review on the adherence and acceptability of MNP reported that 8 studies exhibited an average consumption ranging from 50% to 90% of the recommended number of sachets. 7 Local evidence showed that mean MNP adherence consumed by day-care children was 85% in the municipality of Benguet, Mountain Province. 8 A similar local study conducted in Mindanao showed a median number of 50%, 51%, and 48% consumed MNP sachets per child as recalled by their caregivers, abstracted from compliance cards, and based on counted empty sachets, respectively. 9
Further, given that existing complementary foods of young Filipino children are often low in energy and protein density, and that increasing micronutrient intake through MNP would not necessarily result in adequate energy and protein intake, the combination of MNP with complementary food blend locally known as Bigas-Mongo (BigMo) was hypothesized to be more effective in improving dietary quality and adequacy. This combination, therefore, is deemed to benefit children’s nutritional status better than MNP alone. This study explored how combined nutrition strategies might effectively address undernutrition and micronutrient deficiency.
Qualitatively, this study aimed to explore acceptability and utilization as well as promotion of MNP and BigMo blend among mothers/caregivers and community health workers (CHWs), respectively. Results of this study can provide valuable information needed to improve home fortification intervention programs, which ultimately address micronutrient deficiency.
Methods
This was a substudy performed within the randomized community trial implemented from February to September 2017 among children aged 6 to 23 months in the municipality of Calauan, Laguna, where the effect of 2 different formulations of MNP supplemented with or without BigMo blend on children’s growth and micronutrient status as primary outcomes of randomized community trial was evaluated. This article evaluated the acceptability, compliance of MNP and BigMo use among mothers/caregivers of children, and the promotion of these products by CHWs.
The study protocol (FIERC-2016-008) was approved by the Food and Nutrition Research Institute-Institutional Ethics Review Committee. Mothers who gave informed consent after being informed of the study rationale and procedures by the researchers were included to join the study.
Study Area, Design, and Randomization
The municipality of Calauan was selected because of its high prevalence of children younger than 5 years who are underweight (20.4%). Four barangays were randomly selected, matched based on their characteristics in terms of population and location, and further randomized into 4 intervention groups: (1) VitaMix plus BigMo blend; (2) VitaMix without BigMo blend; (3) micronutrient growth mix (MGM) plus BigMo blend; and (4) MGM without BigMo blend. Since the barangay is the smallest unit in the political structure of the Philippines, where each has its own barangay health center that acts as the main access point for delivering health and nutrition services, this was considered the unit of randomization in the study. The municipality has a reasonably well-functioning health system. The rural health unit consists of 15 barangay health centers serving approximately 14 987 households.
Sample Size and Sampling
With 90% level of confidence, margin of error of 10%, 20.4% postulated proportion of underweight, and a design effect of 1.5 (to adjust for sampling design), the calculated sample size of children was 144. Each intervention group comprised 36 children, selected based on inclusion and exclusion criteria: (1) all apparently healthy children between 6 and 17 months of age at the time of recruitment, without feeding problem/inborn/congenital/severe illness and were not having disease as assessed by the municipal health officer; (2) all children 6 to 17 months old without severe anemia (hemoglobin <7 g/dL) and without severe acute malnutrition (WHZ score <−3 standard deviation); (3) all children who were already consuming semi-solid or solid food in addition to milk or breast-milk before the beginning of the study; (4) permanent residents in the barangay or municipality for the past 6 months; and (5) mothers who were willing to participate in the study with signed informed consent.
Distribution of MNP and BigMo and Nutrient Composition
A total of 141 mothers of children aged 6 to 17 months randomly selected to receive the interventions were invited to join the study. The MNPs were provided freely every month for 6 months to mothers/caregivers of participating children living in the study area. All mothers were advised to add 1 sachet of MNP into the right amount of complementary food blend prepared at home, which ought to be consumed by their children once daily.
Framing within the context of the 2 different MNP formulations, VitaMix and MGM, currently available in the country, the study evaluated their effects in terms of acceptability and compliance among mothers/caregivers. Each sachet of VitaMix contains 15 micronutrients, providing 100% of the recommended nutrient intake (RNI) of each micronutrient for a child 6 to 24 months old. On the other hand, each sachet of MGM has 9 nutrients, providing lower daily RNI for each nutrient, ranging from 12% to 69% of the daily recommended dosage of micronutrients added therein.
Combination of rice, locally known as bigas and mongo (BigMo), is a ready-to-eat processed blend developed by extrusion cooking method, intended for infants and preschoolers. The daily portion size of uncooked BigMo powder blend contains 30 g, providing 120 kcal or approximately 17.8% and 12.5% of the recommended daily caloric intake for children 6 to 11 months and 12 to 23 months old, respectively. The blend also contains 4 g of protein to meet 25.0% and 22.8% of the recommended daily protein intake, respectively, by age-group. Mothers/caregivers from VitaMix+BigMo (group 1) and MGM+BigMo (group 3) were instructed to prepare the powder blend, adding it to the child’s normal diet, mixing 1 sachet or just the amount the child can consume at a time, to 1 cup of previously boiled water.
Data Collection
Qualitative data collection methods were employed through focus group discussion (FGD) and in-depth interview (IDI). Using IDI guide questions, mothers were interviewed at their homes regarding their experiences in preparing and feeding the MNP with BigMo (groups 1 and 3) and without BigMo (groups 2 and 4); perceptions on the effects (positive or negative) of feeding with MNP with or without BigMo blend; willingness to buy MNP and BigMo blend; and their intention to continue feeding the child given the supplements’ availability in the market, among others. Responses were collected during the first (n = 141) and last visits (n = 130), which were within 3 to 7 days after the start and 7 days before the end of MNP supplementation, respectively.
Household visits were conducted by researchers along with the CHWs bimonthly all throughout 6 months, following a predetermined schedule based on the location of the households. Staggered interviews were necessary to manage the workload of interviewers. Further, mothers or caregivers were instructed to accomplish the MNP and BigMo (groups 1 and 3) and MNP only (groups 2 and 4) compliance form daily to record the feeding schedule, amount consumed by the child, and the perceived side effects of the respective intervention. Compliance to MNP was verified and collected by researchers through counting of empty MNP sachets and unopened sachets during each visit. The same procedure was done by the researchers to verify compliance to BigMo in intervention groups 1 and 3. Data on compliance were also collected to capture the mothers’ behaviors, such as following the recommended preparation and feeding and the children’s willingness to consume the MNP and BigMo. Compliance was defined as the mean percentage consumption of MNP and BigMo blend over the expected number of sachets to be consumed for the entire study duration. In this study, good compliance is achieved when children consumed more than 80% of all MNP sachets provided in all groups and BigMo sachets provided in groups 1 and 3 only (Table 1). 10,11
Number of Interviews and FGDs Conducted per Intervention Group and the Corresponding Number of Respondents.
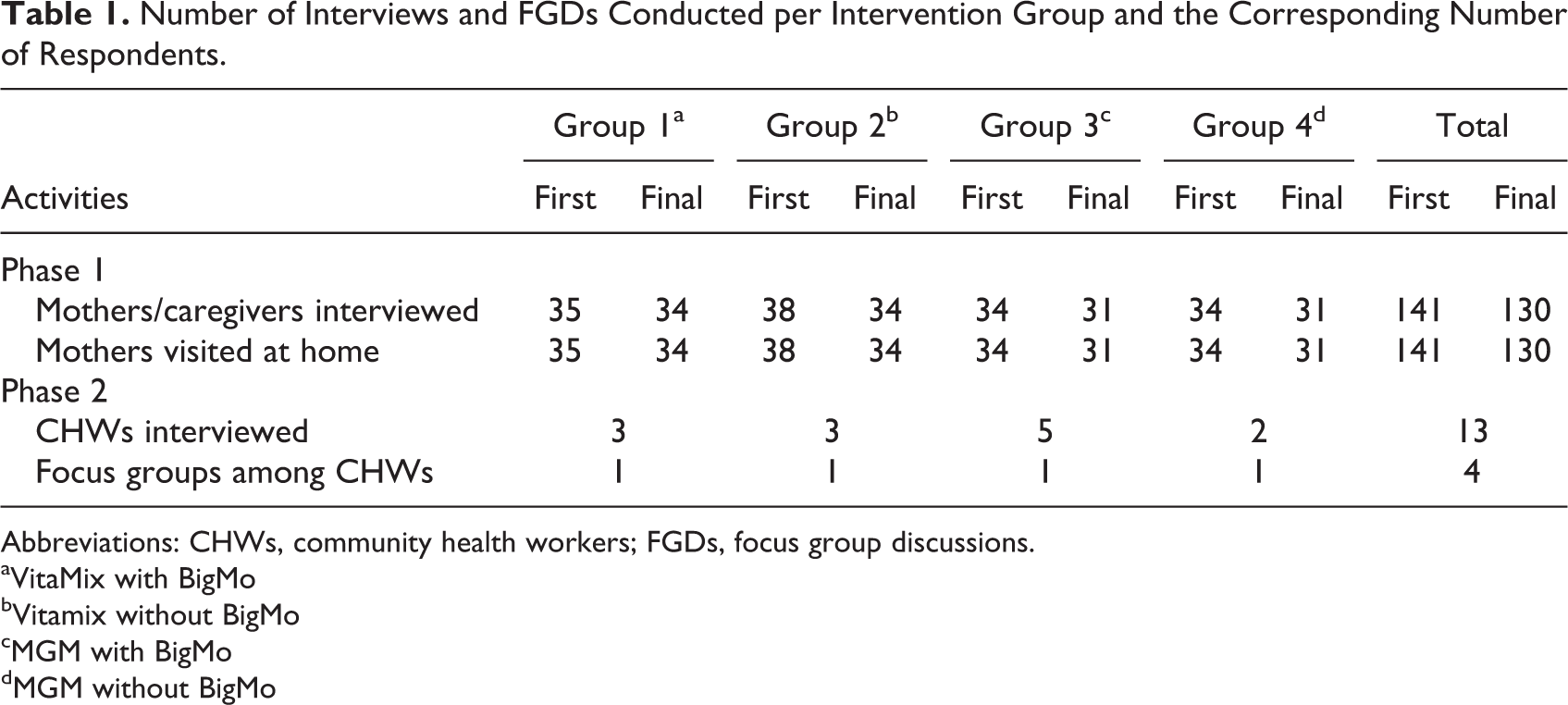
Abbreviations: CHWs, community health workers; FGDs, focus group discussions.
aVitaMix with BigMo
bVitamix without BigMo
cMGM with BigMo
dMGM without BigMo
One FGD was conducted in each barangay, comprising knowledgeable community health and nutrition workers involved in the study. A guide question was developed and pretested for FGD. Topics explored with health workers included the following: (1) knowledge on malnutrition, micronutrient deficiency, MNP and BigMo preparation and use, and optimum infant and young child feeding (IYCF) practices; (2) importance and benefits of MNP; (3) insights and experiences from conducting regular home visits; (4) problems and opportunities encountered in the promotion of MNP in the context of IYCF; and (5) incorporation of MNP supplementation in their daily activities and their attitude toward the program.
A total of 141 mothers/caregivers were included in the initial interview and home visit: 35, 38, 34, and 34 mothers/caregivers were from VitaMix+BigMo, VitaMix only, MGM+BigMo, and MGM only, respectively. Meanwhile, only 130 mothers/caregivers were interviewed poststudy and during visits, since some mothers had opted out. Still, the majority participated in the initial and post-study interviews; 6 mothers were not available to participate in the initial interview, while 18 mothers or caregivers were not interviewed during the post-study because of failure to respond to follow-up or the family relocating to other places outside Calauan, mostly to Metro Manila. Four FGDs were conducted among health workers, and each FGD had 3 to 5 participants.
Data Analyses
The data collected through IDI were summarized by constructing frequency and percentage distributions. Appropriate numerical descriptive measures were also calculated to describe the characteristics of the participating mothers and children. The monthly percentage compliance to MNP and BigMo consumption were recorded and analyzed to come up with the mean percentage compliance for the 6-month follow-up. One-way analysis of variance was performed to compare the mean percentage compliance and acceptability between groups. The FGD contents were transcribed, coded by theme, consolidated, and discussed to extract the main findings.
Results
Characteristics of Participating Mothers
The mean age of mothers was 27.9 years with standard deviation of 7.3 years (Table 2). A majority of mothers (73%) obtained at least a high school education and were full-time or nonworking mothers (79%), which means that most mothers stay at home, usually taking care of their children. Meanwhile, more than half of the mothers (58.2%) were live-in or cohabiting, while more than one-third (37.6%) were married.
Profile of Participating Mothers in In-Depth Interviews.a
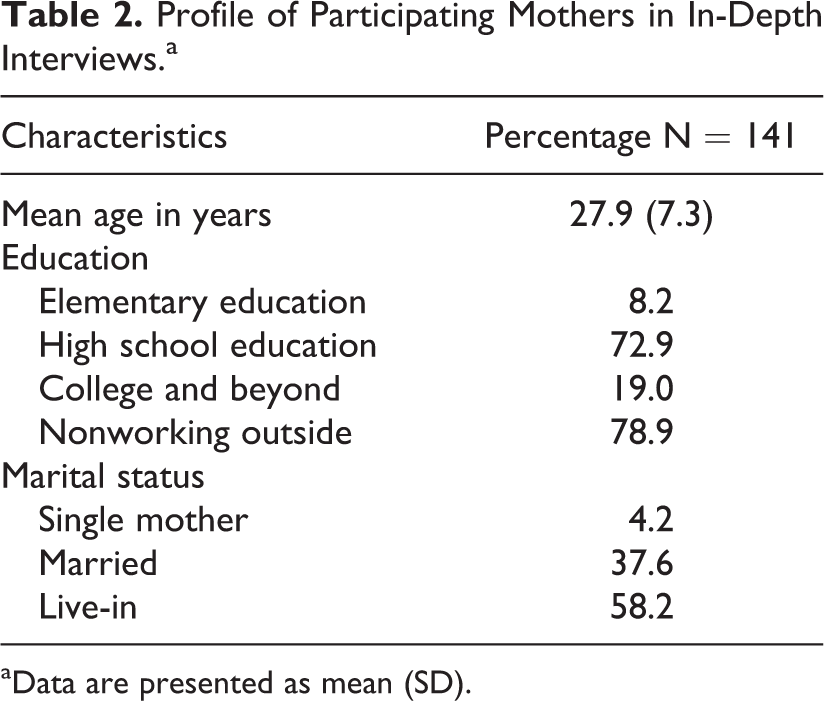
aData are presented as mean (SD).
Acceptability of MNP and BigMo
No significant differences in MNP acceptability were found based on the mean number of times the child disliked MNP taste, reported by mothers between groups (P = .312) as indicated in Table 3. On average, each mother reported her child disliking MNP 2 to 3 times due to its aftertaste and rusty smell.
Acceptability of MNP and BigMo Among Children as Reported by Mothers/Caregivers for 6 Months.
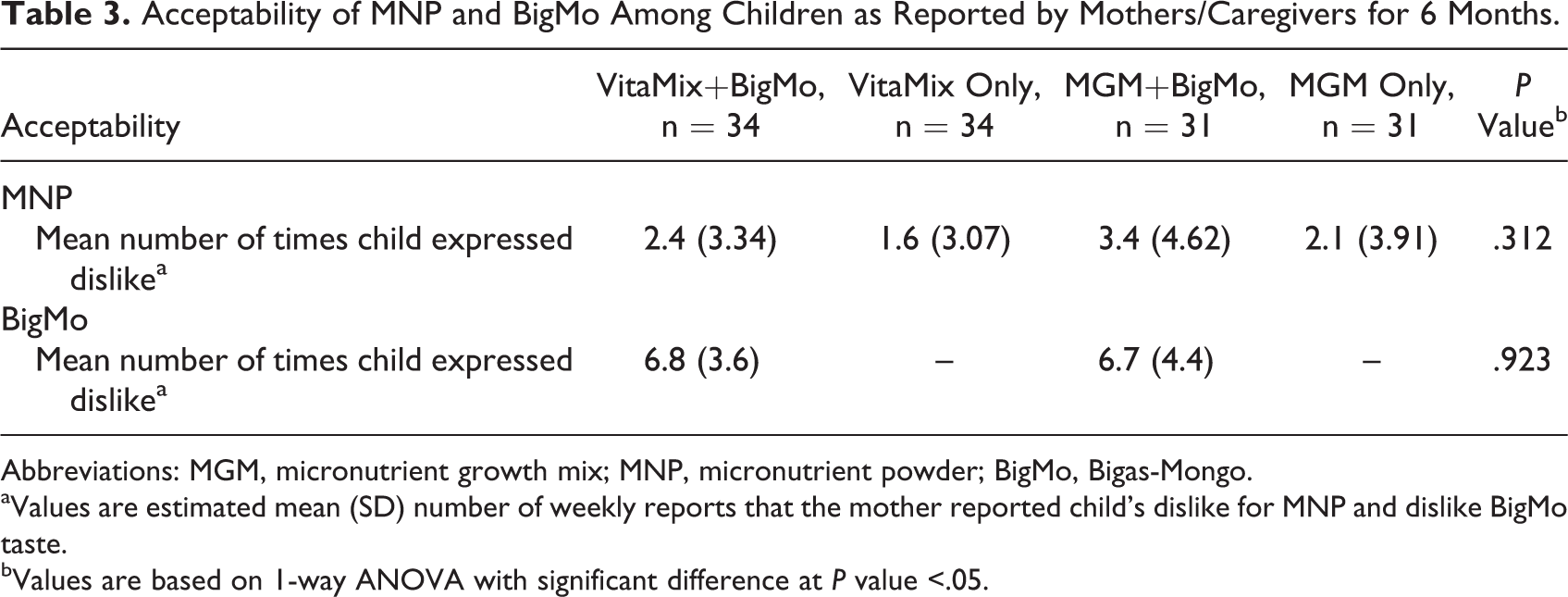
Abbreviations: MGM, micronutrient growth mix; MNP, micronutrient powder; BigMo, Bigas-Mongo.
aValues are estimated mean (SD) number of weekly reports that the mother reported child's dislike for MNP and dislike BigMo taste.
bValues are based on 1-way ANOVA with significant difference at P value <.05.
During the follow-up visits, mothers reported that their children dislike the taste of MNP. One of the mothers even stated that, My child did not want to eat when MNP is added. He spits it out. Similarly, most mothers/caregivers (n = 10) who withdrew from the study justified their decision based on their children’s dislike of the supplement. They grew worried since their children were no longer eating any food, even those without MNP. The children seemed to have associated the taste of MNP with all other food, causing the mothers to fear health consequences for their child if they insist on feeding food mixed with MNP.
No significant difference in acceptability (P = .923) was reported between children who received BigMo in the VitaMix and MGM groups as shown in Table 3. Mothers/caregivers reported that their child disliked BigMo blend at an average of 6 times over the feeding period.
Compliance to MNP and BigMo Blend
As shown in Table 4, the compliance (mean percentage consumption of MNP and BigMo over the expected number of sachets to be consumed) was determined among children who completed the study. The overall mean compliance to MNP consumption by participating children was 74.7%. About two-thirds (63.2%) consumed ≥80% of the expected amount of supplement over the 6-month intervention period. Compliance to the respective MNP supplementation was not significantly different between the VitaMix with and without BigMo (78.8% and 85.1%, respectively; P > .05) and between the MGM with and without BigMo (70.3% and 64.7%, respectively; P > .05). However, children in the VitaMix groups (with and without BigMo) had significantly higher percentage of consumption relative to the expected amount of intake than those in the MGM groups (with and without BigMo). Similarly, significantly more children had consumed ≥80% of the expected amount of supplement in the VitaMix groups (with: 68.8% and without BigMo: 67.6%) than in the MGM groups (with: 57.9% and without BigMo: 58.1%).
Compliance to MNP and BigMo Among Children as Reported by Mothers/Caregivers for 6 Months.
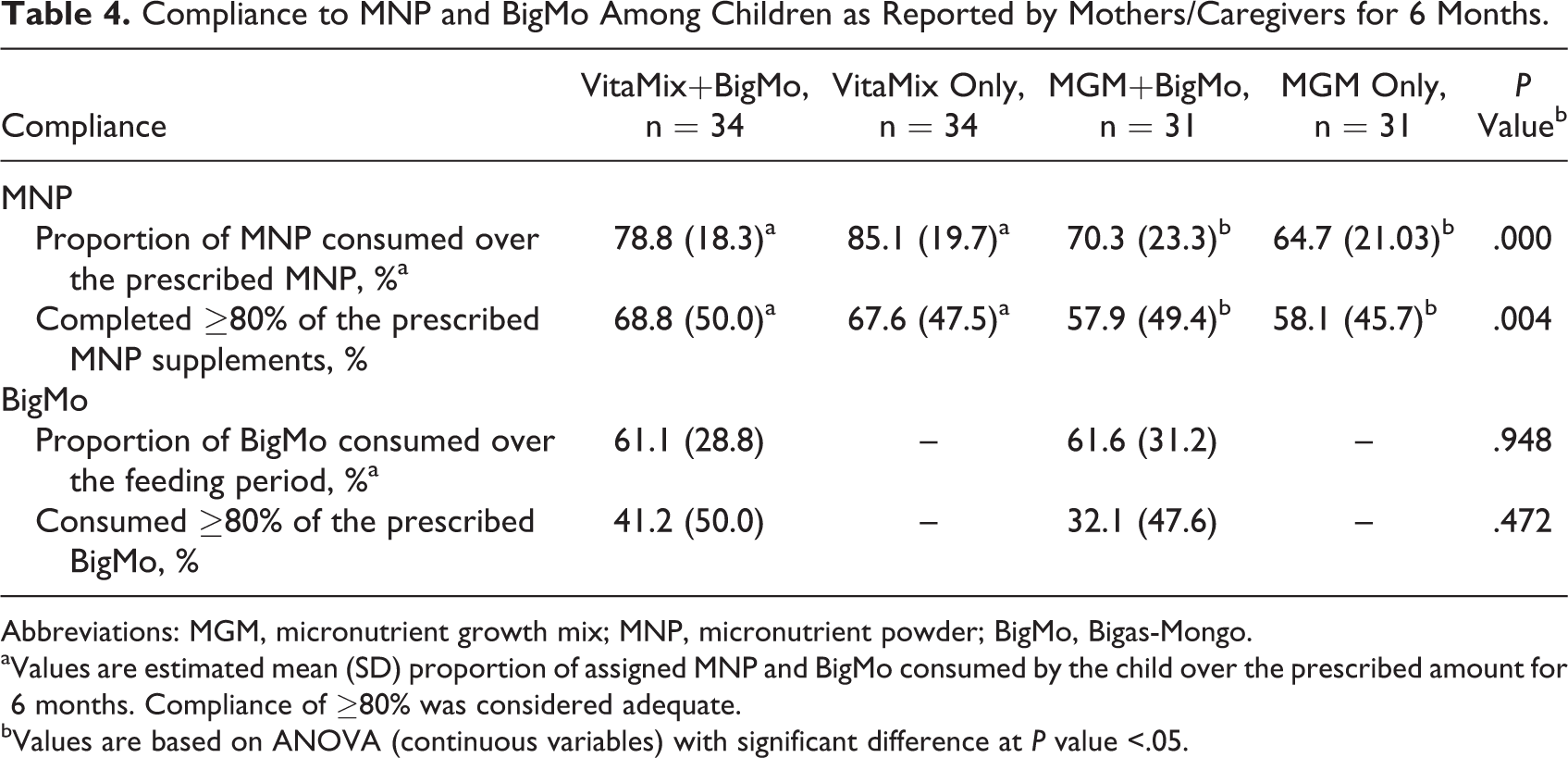
Abbreviations: MGM, micronutrient growth mix; MNP, micronutrient powder; BigMo, Bigas-Mongo.
aValues are estimated mean (SD) proportion of assigned MNP and BigMo consumed by the child over the prescribed amount for 6 months. Compliance of ≥80% was considered adequate.
bValues are based on ANOVA (continuous variables) with significant difference at P value <.05.
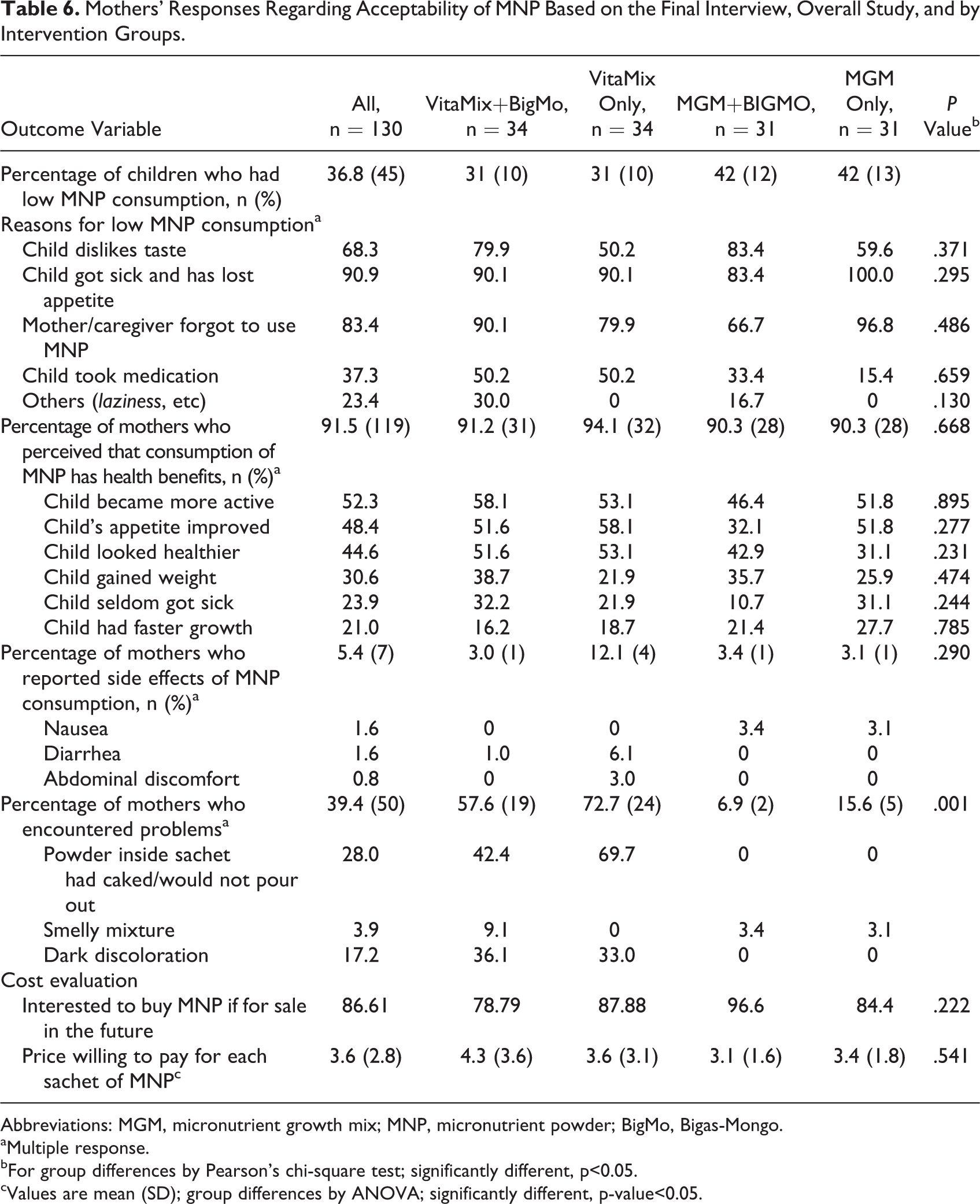
Among mothers of children who had low MNP consumption (n = 45), an in-depth interview was conducted to explore the reasons why their children did not reach at least 80% compliance. Most common reasons for low consumption, as reported by mothers during exit interviews, were the following: child getting sick and losing appetite (90.9%); forgetting MNP use (83.4%); disliking MNP taste (68.3%); stopping MNP supplementation due to other medications (37.3%); and others (23.4%) as shown in Table 6.
The mean BigMo consumption represents 61.34% of the expected intake among those who received the complementary food blend. However, only about 37% of children consumed ≥80% of the recommended BigMo consumption. No significant difference in mean percent consumption of BigMo between groups was noted.
Mother’s Experience in Preparing and Feeding
MNP with BigMo blend given to children
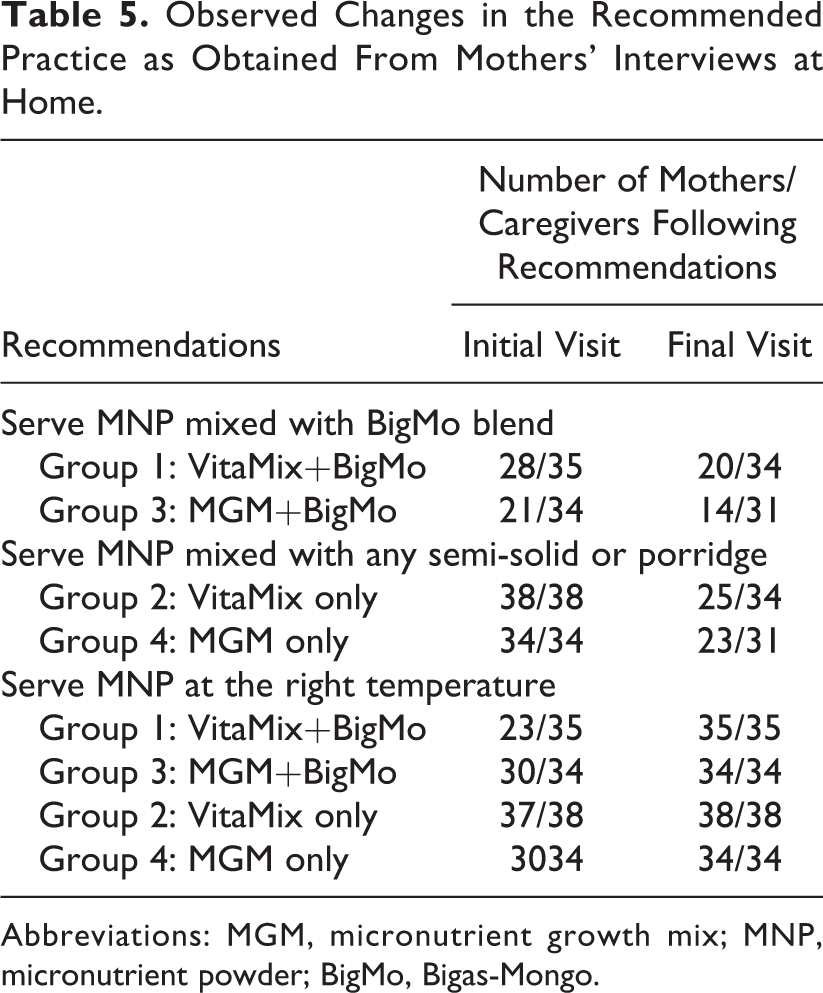
Table 5 summarizes the observed changes in the recommended practice of feeding and preparing MNP, with or without BigMo, gathered during initial and follow-up visits.
Observed Changes in the Recommended Practice as Obtained From Mothers’ Interviews at Home.
Abbreviations: MGM, micronutrient growth mix; MNP, micronutrient powder; BigMo, Bigas-Mongo.
During the first visit (within 3-7 days after the start of MNP supplementation), mothers/caregivers were asked regarding their experiences in feeding and preparing MNP at home, with or without BigMo. Of the 69 mothers/caregivers interviewed from groups 1 and 3, 20 (29.0%; 7 in group 1 and 13 in group 3) reported not mixing MNP with BigMo blend as recommended, citing that their children disliked BigMo blend due to its bland flavor, thick consistency, and roasted smell. Several respondents insisted on giving a small amount of BigMo (1 teaspoon) and modifying its taste by adding a small amount of sugar and milk until the child became accustomed to the taste, as was observed during follow-up visits.
Most of the mothers/caregivers from the MNP and BigMo intervention groups 1 and 3 (n = 49) who were able to follow the recommended practice reported to have mixed MNP with BigMo only in small amounts to ensure that children would ingest the full dosage of MNP according to indications. During the follow-up visits, the number of mothers/caregivers who reported giving MNP with BigMo blend went down to only 34 (49.2%; 20 in group 1 and 14 in group 3) from the initial count of 49 (72.0%). Most mothers/caregivers, particularly those who were unable to feed the thick BigMo mixed with MNP, reported to have adjusted or diluted it similar to am, adding a small amount of milk and sugar before mixing the MNP.
While some respondents claimed to have remembered the recommendation, they found it helpful to dilute BigMo so that children would consume MNP according to indications. As one of the respondents from intervention group 1 related, I boiled the BigMo first, let it cool down and fed it to my child just like ‘am’, adding some milk and a small amount of sugar in his feeding bottle. I think this is better because it makes it easier and faster to feed my child, especially if I am in a hurry. It was also good that my child consumes the recommended amount of BigMo and MNP.
Mothers/caregivers under groups 2 and 4 (VitaMix only and MGM only, respectively) reported different experiences with feeding MNP to their children: All mothers in these groups (n = 38 and n = 34, respectively) reported mixing MNP with savory lugaw bought from food establishments, while others mixed it with the family’s regular food during the initial visit. However, the number of mothers able to follow the recommendations went down to 48 (73.8%) during the final visit. Most mothers/caregivers reported that their children disliked regular food added with MNP, particularly food without broth, and thus preferring to mix it with porridge or lugaw for better compliance. In some cases, mothers/caregivers even reported slipping the MNP candidly into the food, since the children refuse to eat once they’ve seen or smelled the MNP in the food.
It is also worth noting that in all intervention groups, most mothers reported mixing MNP at the right temperature to avoid black discoloration on the food as shown in Table 5. In addition, mothers/caregivers added only about 2 to 3 spoonfuls of food so as not to limit the dose their children receive in case the entire serving was not consumed. As one of the respondents put it, I kept in mind that MNP should be added to the food at the right temperature and that to add only to 2-3 spoonfuls of food or more. Afterwards, I only added food if my child asked for more.
Perceived Benefits of MNP Consumption
Of the 130 mothers interviewed during the final visit, 91.5% expressed several benefits of giving MNP to their children (Table 6). Most of them were motivated to use MNP, citing the following reasons rank-wise: increased activity (52.3%), increased appetite (48.4%), weight gain (30.6%), less incidence of sickness (24.0%), and faster growth (21.0%). They were confident in using MNP, since health personnel promoted its use. Some even reported that their children grew accustomed to its taste. Mothers who expressed positive feedback on MNP reported their willingness to recommend it to other mothers based on similar perceived benefits as discussed above.
Mothers’ Responses Regarding Acceptability of MNP Based on the Final Interview, Overall Study, and by Intervention Groups.
Abbreviations: MGM, micronutrient growth mix; MNP, micronutrient powder; BigMo, Bigas-Mongo.
aMultiple response.
bFor group differences by Pearson's chi-square test; significantly different, p<0.05.
cValues are mean (SD); group differences by ANOVA; significantly different, p-value<0.05.
Side Effects of MNP and Problems Encountered
Concerns were raised regarding the observed side effects of MNP to children, namely, abdominal discomfort (n = 16/141) and constipation (n = 5/141) during the initial visit. Mothers (n = 6/11) who withdrew from the study reported that MNP had caused diarrhea or abdominal discomfort to their children. However, CHWs and field researchers reassured the mothers/caregivers that MNP supplements contain only vitamins and minerals that support children’s growth. Of the mothers (n = 7/130) who reported side effects of MNP consumption during the final visit, diarrhea (1.6%), nausea (1.6%), and abdominal discomfort (0.8%) were reported.
Thirty-nine percent (39.4%) of mothers reported to have encountered problem with MNP (Table 6). The most common feedback given during the home visit were the powder turning dark brown, its tendency to form into a compact mass and thus the difficulty in pouring the content (28.0%), and its dark discoloration (17.2%) that eventually disappeared when MNP is mixed with thick mixtures, like BigMo, porridge or lugaw, or mashed banana.
Willingness to Pay MNP
A majority (86.6%) of the mothers were willing to purchase MNP for their children. The average preferred price was computed at Php3.60 (between Php1.00 and Php10.00) per sachet. Based on the ratings, MNP’s perceived health benefits to the children contributed to the mothers’ willingness to buy. Most mothers have anticipated the supplement’s affordability, which would allow them to buy the product. Meanwhile, most mothers/caregivers (anticipating free distribution in the future) were willing to pick up MNP supply from barangay health centers given that it is already provided for free.
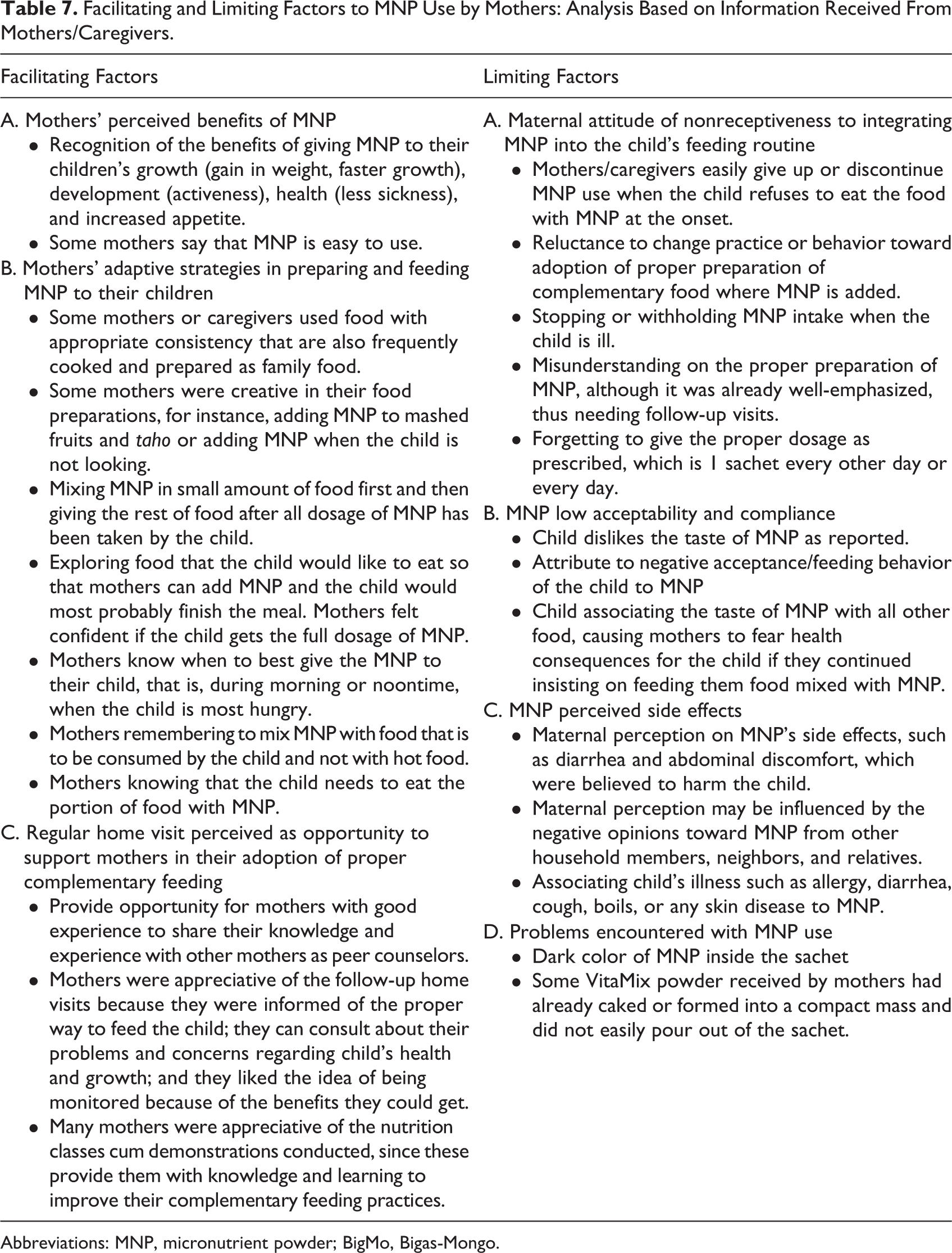
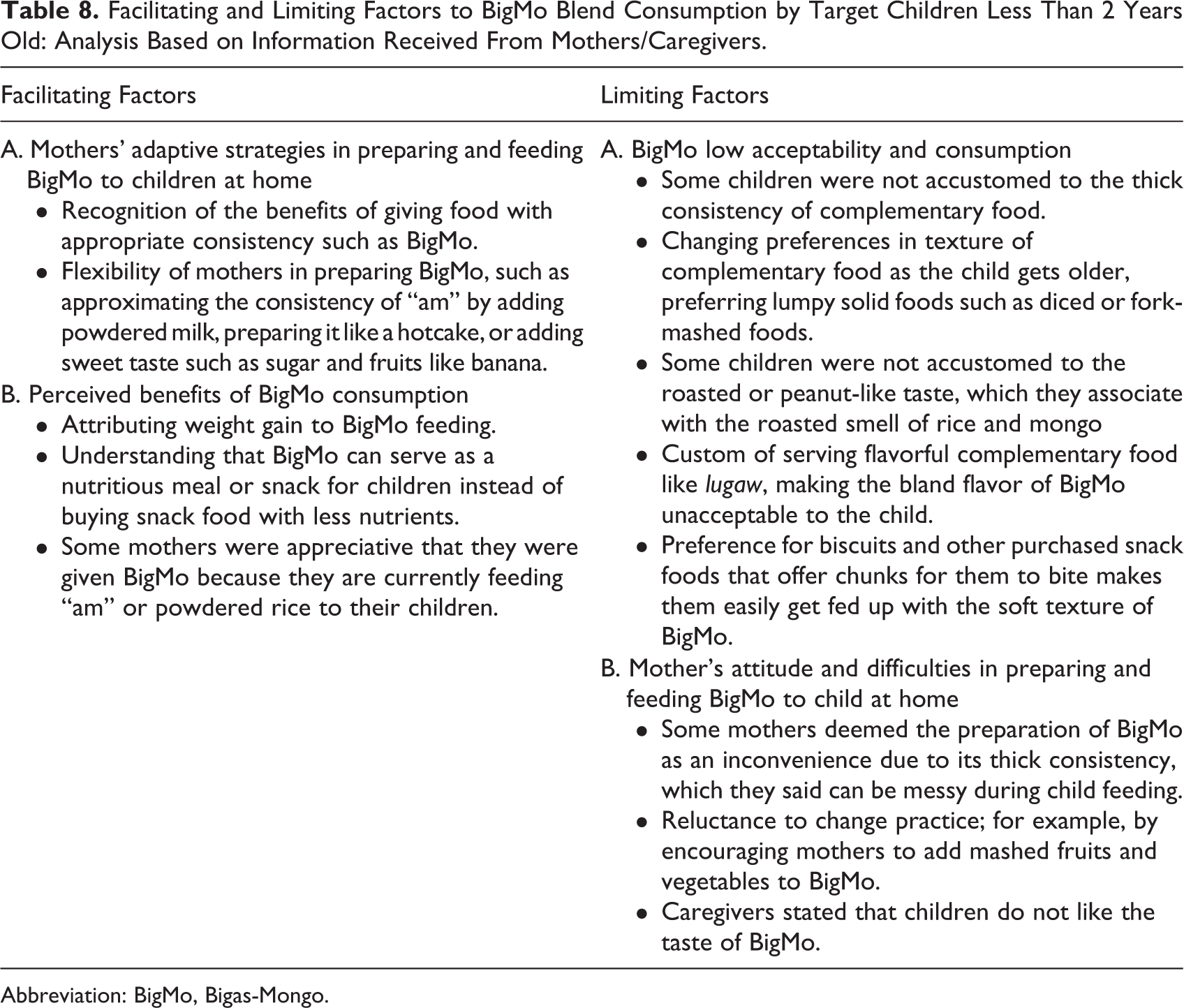
Given the experience of mothers in preparing and feeding MNP with or without BigMo blend at home, including maternal responses regarding acceptability, consumption, and willingness to pay, several facilitating and limiting factors in the use of these products by mothers were identified from this study. Some of these are summarized in Tables 7 and 8.
Facilitating and Limiting Factors to MNP Use by Mothers: Analysis Based on Information Received From Mothers/Caregivers.
Abbreviations: MNP, micronutrient powder; BigMo, Bigas-Mongo.
Facilitating and Limiting Factors to BigMo Blend Consumption by Target Children Less Than 2 Years Old: Analysis Based on Information Received From Mothers/Caregivers.
Abbreviation: BigMo, Bigas-Mongo.
Health Personnel’s Knowledge and Experiences on MNP and BigMo Feeding Distribution and Promotion
Several challenges can facilitate or limit wider promotion of MNP by CHWs and, consequently, the use of MNP and BigMo blend among target groups.
Knowledge on micronutrient deficiencies and feeding practices
Most CHWs had a good understanding of the main causes of malnutrition among young children in their respective areas. Five CHWs cited limited access to food rich in vitamins due to poverty (ie, lack of income and limited purchasing power) as the main reason, while 5 CHWs remarked that mothers/caregivers have poor knowledge and behavioral practices (eg, giving junk food instead of nutritious food) on proper child feeding in terms of type of food, frequency, and amount to be given to their children. One CHW also mentioned that neglecting the importance of exclusive breastfeeding, especially among poor families, is one problem why malnutrition exists among children. Poor hygiene and sanitation also contribute. One CHW also recognized the effect of maternal nutrition before and during pregnancy, citing that “mothers who did not get proper nutrition during pregnancy are at higher risk of giving birth to low birth weight infants.” Most CHWs (11) had adequate knowledge on micronutrient deficiencies: they know that poor vitamin intake causes these deficiencies, and they often notice the common misconception of identifying iron as a vitamin and not a mineral.
The health personnel had adequate knowledge on proper child feeding, citing some recommendations: “starting at 6 months, while continuing breast-feeding, infants should be receiving semi-solid foods, like mashed potato, egg yolk, or fruits that are easily digested and safe to eat by boiling in water”; “introduce a variety of nutritious and balanced food from go, grow and glow”; “avoid giving junk foods”; instead of Cerelac, nutritious food like lugaw, mashed potato, carrots, among others, should be prepared by mothers.”
Knowledge on MNP supplementation
With regard to knowledge on the target age-group for MNP supplementation, 11 of the 14 CHWs correctly identified it as children <2 years; only 3 CHWs answered children 6 months to 6 years old. However, confusion still exists regarding target age-groups for MNP supplementation and its use and preparation, and some inconsistencies and contradictions were observed on MNP use, especially during illness (whether or not to stop supplementation). Nevertheless, most of them recognized the benefits of MNP, which are to improve the child’s appetite (11); provide complete vitamins and minerals as supplement (5); improve growth and development (5); and improve resistance or immunity against diseases (5). One CHW highlighted, “After being provided with MNP, a child who previously looked pale and sickly started to have a healthier complexion.”
Moreover, CHWs were observed to have sufficient knowledge on MNP usage, noting that MNP should be mixed with semi-solid complementary food (eg, lugaw or kanin na masabaw with “broth”) at the right temperature. In turn, promoting MNP use was considered by several CHWs as a great opportunity to focus on appropriate feeding practices for children.
MNP distribution strategy
In terms of the distribution methods, several CHWs (6) deemed that MNP should be distributed during house-to-house visits, since they felt the need to closely monitor actual MNP use as well as remind and clarify with mothers about its proper use. For BigMo distribution, they also reported additional benefits of distributing the products through home visits, because this allows them to encourage the mothers to feed her child BigMo and cultivate a habit of preparing it at a set time. A barangay nutrition scholar explained that Home visits allow us to monitor the use and side effects experienced by children from MNP or BigMo intake. This is corroborated by a testimonial from another barangay health worker who mentioned that It is difficult to convince parents to continue feeding MNP when the child has experienced side effects. The CHWs were concerned about mothers who are unlikely to prepare and feed the MNP and BigMo regularly as prescribed or are less inclined to encourage the child to eat the supplement once the child initially refused, or those who would stop feeding the supplement once perceived that the child became sick from its consumption. These issues were considered barriers to compliance in the absence of CHW’s advice and supervision.
On the other hand, 4 CHWs preferred centralized monthly MNP distribution, since this allows uniform instruction and discussion, chance to check in with mothers who are interested or willing to join the program and to motivate them to participate in a program that benefits their children. Another reason for this frequency, according to a Barangay Nutrition Scholar, is that Mothers must also learn to take part or assume a role so that the program will last, otherwise they will get used to the system of just receiving without any effort made, when in fact this is for their own children’s welfare. Interestingly, the CHWs who preferred centralized MNP distribution at the Barangay Health Center were working in barangays, where mothers are easily convened during classes and monthly assessments.
Meanwhile, regarding frequency of distribution, 8 CHWs reported preferring monthly MNP distribution and provided the following reasons: Once a month distribution implies less hassle and is more convenient for health workers and This avoids families running out of MNP stock in case health workers could not provide MNP on time due to other activities. Four CHWs preferred once-a-week distribution to facilitate more frequent visits among families, making it easier to closely monitor MNP use and the child’s improvement or changes, as well as to check whether or not mothers are really using MNP. Regardless of their preferred frequency, it is interesting to note that most CHWs preferred conducting home visits among children, recognizing that it is an important strategy in MNP supplementation program.
The CHWs commented that they had received some positive feedback from mothers regarding MNP supplementation during regular home visits: Mothers were thankful for the effect on their child’s health, such as improved appetite and being active; It was useful because one mother reported that MNP replaced the multivitamins syrup she always bought prior to the study; Some mothers reported that their children got accustomed to the taste of MNP; and Some mothers made it a point to remind us or ask us for their next supply.
Feasibility of integrating MNP supplementation with other health services
All CHWs interviewed agreed that it would be feasible to integrate MNP supplementation with other existing programs such as Garantisadong Pambata, Operation Timbang or mass weighing among children 0-71 months of age, growth monitoring, and supplementary feeding programs as long as there is a harmonious relationship and proper coordination among health workers.
Several CHWs deemed MNP distribution and monitoring as easy tasks, since they can integrate these during IYCF nutrition counseling to maximize visiting time of mothers at health-care centers. The MNP supplementation has similar goals and target beneficiaries as other health programs; thus, it would be easier to implement and effort required would be more or less the same. For instance, Garantisadong Pambata, which starts from April to October, targets children 0 to 5 years old, aims to improve the nutritional status of young children and thus can be simultaneously done with MNP distribution. In addition, supplementary feeding was perceived as helpful in facilitating MNP introduction, since food supplementation can be used to demonstrate MNP preparation and use among mothers. Some of the facilitating and limiting factors to MNP promotion by CHWS are presented in Table 9.
Facilitating and Limiting Factors to MNP With or Without BigMo Promotion Based on Information From Community Health Personnel.
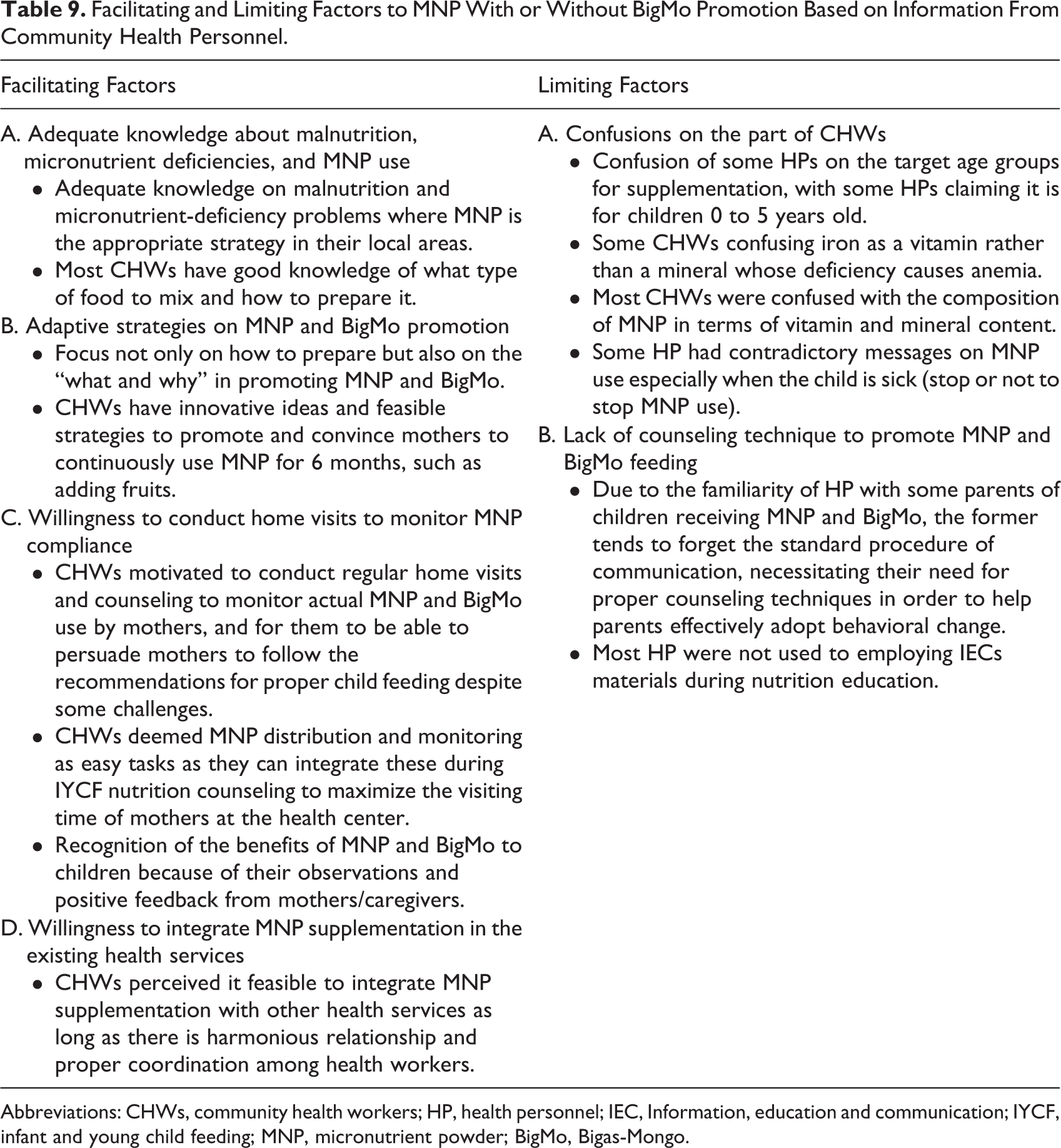
Abbreviations: CHWs, community health workers; HP, health personnel; IEC, Information, education and communication; IYCF, infant and young child feeding; MNP, micronutrient powder; BigMo, Bigas-Mongo.
Discussion
Analysis of the acceptability, compliance, and experience of mothers in preparing and feeding MNP and BigMo to their children was relatively variable and inconsistent. In particular, the VitaMix groups (with and without BigMo) had significantly greater compliance than MGM groups (with and without BigMo). Similarly, significantly more children had consumed ≥80% of the expected amount of supplement in the VitaMix groups than in the MGM groups. The significantly higher mean consumption of the supplements in the VitaMix groups than in the MGM groups might be attributed to the generally less frequent supplementation in the VitaMix groups at only thrice a week compared to the daily supplementation of MNP in the MGM group (with and without BigMo), which explains the lower compliance rate in the daily MNP supplementation. These findings are consistent with the study of Kounnavong et al 11 in Lao PDR, where children under twice-weekly supplementation yielded a higher compliance rate (100%) than those in the daily MNP supplementation (72%). Likewise, highest adherence was observed in trials wherein children received MNP on an intermittent basis. 12 This, according to Ip, 12 may be explained by the perception of mothers or caregivers, wherein intermittent supplementation (eg, 2 to 3 times weekly) is seen as causing less mental pressure and anxiety among mothers or caregivers.
Overall, the perceived health benefits and side effects of MNP shown in this study were similar to other studies. 13 -16 Specifically, the perceived benefits of MNP as viewed by mothers/caregivers, including their interest and adaptive strategies in preparing and feeding MNP to their children, can facilitate greater acceptability and sustainability of local MNP use. However, perceived side effects such as (1) diarrhea and abdominal discomfort as reported by mothers, (2) discontinuation of use when the child refuses to eat the food with MNP at the onset, (3) negative opinions from other household members, neighbors, and relatives on MNP use can influence mothers’ acceptability and compliance, and (4) misunderstanding of its proper preparation were some of the potential barriers to MNP use.
To address these challenges, it is then critical to fully equip the mothers for MNP use, including its potential side effects and accurate and specific instructions on preparation and feeding with BigMo blend prior to and during the intervention period. Such recommendation is agreed upon by mothers and caregivers who found that follow-up visits were indeed very beneficial in helping them incorporate MNP appropriately, providing opportunities to discuss misconceptions, dispensing tactics on how to properly feed the child, and creating an environment where they can freely consult about problems and concerns regarding their child’s health and growth. In short, they liked the idea of being monitored because of the benefits they were experiencing. Home visits led to enhanced understanding and use of MNP, which greatly facilitated its acceptance and use among mothers and caregivers. This activity has also been reported as a helpful component in nutrition programs in Haiti, 17 Nigeria, 14 and Peru. 16 Thus, results of the study suggest that preparation and use of MNP and BigMo blend by mothers at home is optimized when regularly monitored by CHWs.
It is worth noting that the consumption of both MNP and BigMo blend were poor during child illness and recovery period as noted during interviews and observations of mothers and caregivers. The practice of reduced feeding with semi-solid and solid foods during child illness is a recognized challenge for children’s recovery and growth that is commonly observed in many settings. 18 In this study, it was observed that not only MNP and BigMo blend were discontinued when the child is sick; in fact, a child’s typical diet was also reduced by most mothers. Another potential threat to MNP or BigMo blend consumption is when a mother believes that MNP or BigMo blend made her child sick, she may refuse to continue feeding them the supplement even when the child has recovered. Preventing permanent discontinuation of feeding supplements may be avoided through active engagement and monitoring of health workers from the start.
The number of mothers who reported not mixing MNP with BigMo blend decreased between the first and final interviews, suggesting that, with time, most mothers/caregivers find it difficult to sustain feeding the supplement. Some mothers/caregivers reported that their children got fed up with eating BigMo due to its thick consistency or texture, since they already prefer semi-solid food with some little bits to bite as they get older. This is specifically true for children between 12 and 18 months old, already physiologically capable of consuming other solid food frequently served by their mothers/caregivers, 19 suggesting that there is probably a narrower age span when there is a special need for transitional or semi-solid food. Thus, the type of formulation of complementary food should differ between 6 to 11 months and 12 to 23 months of age. Nevertheless, several mothers reported to have insisted on giving a small amount of BigMo blend (1 teaspoon) and, at the same time, modifying the taste by adding small amount of sugar and milk until the child grew accustomed to the taste after several follow-up visits and encouragement. Overall, these findings again highlight the importance of home visits to support and encourage mothers in establishing a feeding routine, especially in the first few weeks of supplementation.
Most of the significant barriers observed to BigMo blend effectiveness in addressing childhood undernutrition point out that its acceptance was associated with the organoleptic properties of the product as discussed earlier. Therefore, careful attention should be given to sensory characteristics, such as taste, flavor, aroma, viscosity, and texture, when developing any kind of complementary food blend to minimize rejection and improve consumption by the target children. Possible ways to improve complementary food blend based on complementary feeding guidelines are available. First, there are specific formulations to possibly reduce the consistency of starchy food while still maintaining high-energy density to make them easier to consume and more acceptable to young children. Second, some viscosity-reducing technologies are available to help balance the energy and nutrient profile of the final complementary food blend and its sensory characteristics to yield higher acceptability and compliance not only for young children but also for mothers/caregivers who would be feeding them. This is an important consideration, especially if the complementary blend is intended to be distributed and prepared at home, as done in this study.
Furthermore, acceptability was also associated with child’s current feeding practices prior to receiving BigMo blend, as evident in the following observations: (1) Typical complementary food in the area is made up of rice and soup from the family cooking pot, oftentimes diluted or has thin-consistency instead of semi-solid food that has the same consistency as BigMo; (2) preference of growing children for eating solids, such as biscuits and other purchased snack foods that offer chunks for them to bite makes them easily get fed up with the soft texture of BigMo. Addition of powdered milk or any other flavors, such as fruits to improve the bland taste of BigMo, was favored. Better compliance was observed among children less than 1 year old, since they were at the age of beginning complementary foods where taste preferences are not yet established, a finding consistent with the study in Bangladesh. 20 However, some mothers were able to improve their practices on BigMo preparation and feeding after cooking demonstrations and regular home visits were conducted by the research team. Cooking demonstrations and home visits are part of the routine functions of CHWs, but to the research team’s knowledge, these activities were not conducted regularly in the study site point out the integration of this enabling component of the IYCF program.
Due to the familiarity of health personnel with some parents of children receiving MNP and BigMo, the former tends to forget the standard procedure of communication, with little attention given to the socioeconomic and cultural background, routines, and practices to help parents stir behavioral change. This may limit the acceptability and use of mothers and caregivers within the context of the MNP and complementary food supplementation program in this setting. As previously reported by Young et al 21 and Creed-Kanashiro et al, 16 there was a greater acceptance and use of MNP by caregivers when CHWs appropriately adapted their interaction, rapport, and counseling with mothers to the local culture, taking time to understand their situation, explaining more about MNP or BigMo as complementary food supplements that could help improve child’s nutritional status, helping them resolve their doubts, and integrating their use into the family and child’s feeding routines.
Such potential limiting factors may be addressed more specifically in the training of CHWs. Improved training will also include proper orientation of CHWs regarding the target group, MNP distribution, distribution schedule, reporting forms, and monitoring system to ensure a well-coordinated program implementation. This is also to ensure the correct understanding of the guidelines, messages/instruments, and proper counseling techniques as well as to avoid confusion in the promotion of MNP by health workers at the local level. Alongside this information, education and communication materials should be developed, made available, and used during interpersonal communication with mothers/caregivers to attain a more lasting psychological impact.
Nevertheless, as reported by CHWs during FGDs, rather than implementing MNP use as an isolated endeavor, it can be seamlessly integrated into existing health programs, gaining value from willingness to distribute the supplements among households of children, conduct monitoring and guidance through home visits, and demonstrate cooking methods. Ultimately, this integration can facilitate and improve MNP model design and complementary food supplementation programs.
However, even if CHWs are willing to integrate MNP supplementation into other health services without additional compensation, they may have difficulty in closely monitoring compliance of target children without any support given to them; thus, providing transportation allowance, increasing the compensation of health workers, or recruiting additional workers may be a more effective means to promote the use and acceptance of MNP locally.
Conclusion and Recommendations
Results highlight specific issues that can facilitate or limit the acceptability and compliance to MNP and BigMo blend with emphasis on the following: (1) maternal perceptions and attitudes toward preparing and feeding such products to the child; (2) CHWs’ attitude and strategies in promoting MNP and BigMo. Based on the results of this study, the recommendations to increase acceptability and compliance to MNP and BigMo use that can be basis for scaling up of the program are as follows: (1) Feeding instructions for MNP and BigMo use should be clear and simple, and if possible, visual aid in the form of brochure, flyers, posters, or reminder cue cards should be provided to mothers/caregivers to ensure consistency of messages; (2) CHWs to visit homes at least once a week during the first month and decreasing frequency thereafter to help mothers/caregivers resolve problems and to ensure sustained use; (3) proper training of CHWs to ensure correct understanding and use of MNP and BigMo; (4) improve formulation of complementary food blend in terms of viscosity, taste, aroma, and texture to yield higher acceptability not only for young children but also for mothers who would be feeding them; and (5) specific formulations of complementary food blend with regard to consistency and texture should be different for infants 6 to 11 and 12 to 23 months of age. The results of this study are expected to provide guidance to MNP program implementers and related programs in the country to help combat micronutrient deficiencies in infants and young children.
Footnotes
Authors’ Note
EA Goyena, CVC Barba, MM Paunlagui, and AC Rola conceived the manuscript. Goyena carried out the fieldwork. Goyena and Talavera drafted and revised the manuscript. NA Tandang analyzed and interpreted the data. All authors read and approved the manuscript.
Acknowledgments
The authors wish to thank all the mothers, children, and community health workers for their willingness to partake in the study, especially for the time they gave and patience they showed in responding to all the questionnaires. They would like to thank the Laguna Provincial, especially Mrs Natividad Vito and the municipal health office headed by Dr Jelidora B. Refrea, and also the Calauan local government led by honorable Buenafrido T. Berris for their valuable participation, coordination, and for facilitating this study. Special thanks to Emely G. Sanson for her hard work in monitoring and interacting day by day with mothers and caregivers during the study implementation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: The study was funded by various organizations: Neys van Hoogstraten Foundation (NHF) of The Hague, The Netherlands; Southeast Asian Regional Center for Graduate Study and Research in Agriculture (SEARCA); and the Department of Science and Technology through the Human Resource Development Program (HRDP) and the Science and Technology Human Resource Development Program (ASTHRDP).