
Abstract
Introduction:
Breast-feeding practices (BFPs) can be assessed by interviewing the mother about current feeding practices and with a 24-hour recall. It is crucial to establish the accuracy of these methods, which are commonly used by public health decision makers to design health policies aimed at increasing exclusive breast-feeding rates.
Objective:
We aimed to validate 2 self-report BFP instruments using the dose-to-mother deuterium oxide turnover technique (DMDOT) as the reference method.
Methods:
Breast-feeding practices were assessed by interviewing the mother about current feeding practices and with a 24-hour recall in 36 Guatemalan mother–infant pairs. The validity of these instruments was assessed using DMDOT as the reference method.
Results:
Both self-report instruments overestimated exclusively breast-fed (EBF) infants. Infants classified as EBF were 50% by the reported current feeding practice, 61% by the 24-hour recall, and only 36% using DMDOT. Sensitivity to detect EBF infants from the mother’s self-report was 92% (95% CI: 62%-99%) while from the 24-hour recall was 100% (95% CI: 72%-100%, P < .01). However, specificity for both instruments was low, at 74% (95% CI: 51%-89%) for reported current feeding practice and at 61% (95% CI: 39%-79%) for the 24-hour recall (P < .01).
Conclusion:
Both reported current feeding practice and the 24-hour recall instruments overestimated exclusive breast-feeding. Nevertheless, the use of reported current feeding practice provided more accurate data to assess BFPs in a public health setting. Furthermore, population-based surveys should consider the overestimation of exclusive breast-feeding caused when using these BFP instruments.
Introduction
Appropriate infant feeding practices play an important role in ensuring optimum growth, development, and health in the first years of life. The World Health Organization (WHO) recommends exclusive breast-feeding for 6 months, followed by the introduction of appropriate complementary foods, while breast-feeding continues until 2 years of age. 1 In many countries, however, only a small proportion of infants are exclusively breast-fed (EBF) during the first 6 months of life, and there is limited information about the quantities of breast milk consumed. 2 –5 This lack of information is due to difficulties involved in measuring breast milk intake. 6 Currently, WHO recommends the 24-hour recall instrument to assess infant feeding practices in population-based surveys. 7 This instrument is used to establish breast-feeding rates in most countries. In Guatemala, exclusive breast-feeding prevalence reported in 2009 among infants aged from 0 to 5.9 months was 49.6%. 8
Researchers have to rely on retrospective information provided by the mother when asking her to recall details about her previous breast-feeding practices (BFPs) when her children were younger 9 or during the previous 24 hours. The validity of the data on exclusive breast-feeding based on single 24-hour periods and indicators used to monitor breast-feeding particularly exclusive breast-feeding at the population level has been questioned before. 10 –13 Therefore, some researchers have studied the reliability of maternal report data and the validity of the 24-hour recall. 10,14 –16 However, only 2 studies have assessed the validity of these methods using a direct measurement of breast milk intake as the reference method. 2,4 The reference method was the dose-to-mother deuterium-oxide turnover (DMDOT) technique. 3 This method was introduced by Coward et al in 1979, 17 and described more fully in 1982, 18 but did not see widespread application until after the publication of the WHO Global Strategy for Infant and Young Child Feeding in 2001. 1 Briefly, the method involves a lactating mother drinking a known amount of deuterium oxide (water labeled with deuterium, a stable, nonradioactive isotope of hydrogen). The deuterium mixes rapidly with the water in her body, until it is evenly distributed. The baby receives deuterium only through breast-feeding. Saliva samples are collected from the mother and her infant over a 2-week period, and the enrichment of deuterium in saliva is measured. Figure 1 shows the enrichment of deuterium in the saliva of a mother–infant pair. The deuterium gradually disappears from the mother’s body due to water turnover. If the baby is breast-fed, the enrichment of saliva increases to a maximum in 3 to 4 days and then gradually disappears as the deuterium is eliminated from the mother’s body and the milk consumed by the infant becomes less enriched. The amount of human milk consumed by the baby is calculated by fitting the isotope data to a model for water turnover in the mother and infant as described by Haisma et al. 3 The method also provides information on the baby’s intake of water from sources other than human milk and is therefore an objective measure of exclusivity of BFPs. The method was independently validated against test weighing. 19
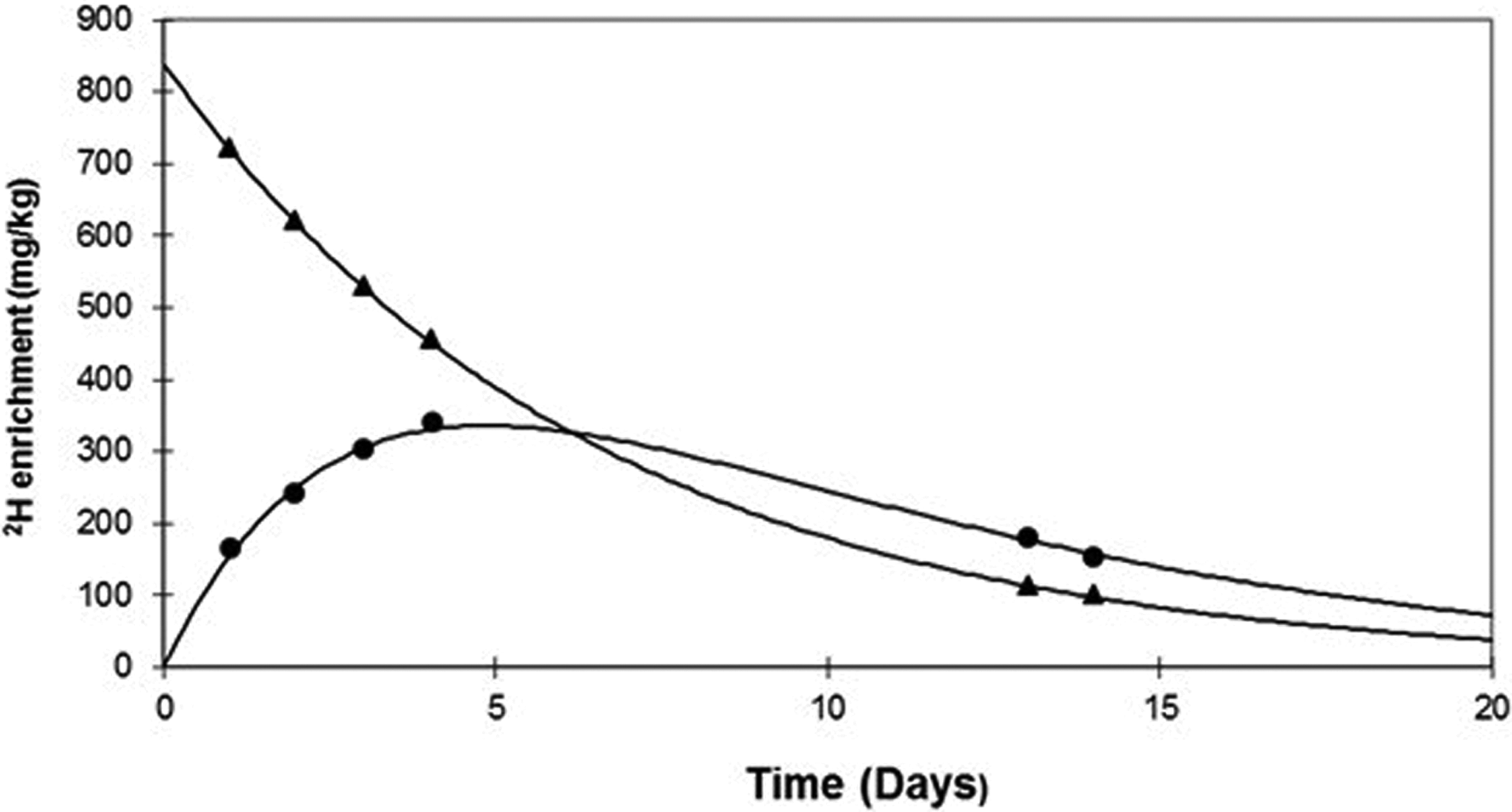
Example of the enrichment of deuterium (2H, mg/kg) in the saliva of the mother (▴) and her exclusively breast-fed infant (•) following a dose of deuterium oxide to the mother.
In this study, we aimed to validate reported infant BFPs in Guatemala using the DMDOT technique. To our knowledge, this is the first study in Latin America that has assessed the validity of self-reported instruments against a reference method, which accurately measures breast milk and nonbreast milk water intakes. The validation study will provide insight into patterns of breast-feeding in Guatemala and will ensure that accurate information is available to public health programs and policy makers.
Methods
Participants
This study was carried out in San Jose La Comunidad, located in Mixco, Guatemala City. The local health center was visited to obtain permission for data collection and invite mothers to participate. The local director of the health center provided a list of mothers who had had a baby in the last 3 months. Each name was assigned a number using a random number generator. Letters of invitation and consent forms (n = 50) were sent, and the purpose of the study and the study procedures were explained to mothers. Eligible infants were healthy infants with adequate length for age and weight for length (between ±2 standard deviations [SDs] according to the WHO growth reference) at 3 months of age who were receiving breast milk. We excluded mothers who were younger than 16 years or older than 40 years, who had more than 3 older children, or who had type 2 diabetes or other chronic diseases. The participants in this validation study were recruited from the Guatemalan cohort of an ongoing multicenter study in the Latin American region in which the main objective was to evaluate breast milk intake and body composition of infants and mothers as indicators of good feeding practices and nutritional status.
Written informed consent was obtained from those eligible to participate after explaining the purpose and the methods of the study. The institutional review board of the Institute of Nutrition of Central America and Panama (INCAP) approved the study protocol.
Anthropometric Measurements
Trained research assistants scheduled appointments at local health center, conducted interviews, and did the anthropometric measurements. Mothers were interviewed to assess sociodemographic data. After the interview, anthropometric measurements from infants and mothers were taken using standardized procedures and calibrated equipment. Height was measured to the nearest 0.1 cm using a portable stadiometer (SECA 214, Medical Measuring Systems and Scales, Chino, CA, USA). The weight of the infant was measured to the nearest 0.02 kg using a digital pediatric scale (Tanita 1584, Tanita Corporation of America, Arlington Heights, IL, USA) on days 0 and 14 of the DMDOT technique. The weight of the mother was measured to the nearest 0.1 kg using a digital scale (Tanita UM-061, Tanita Corporation of America, Arlington Heights, IL, USA). In children, body mass index (BMI) for age, length for age, weight for length, and height for weight were calculated with WHO Anthro, according to the World Health Organization growth reference. Standard deviation between ±2 was defined as adequate. In mothers, BMI was calculated as weight (kg)/height (m2), and overweight was classified as ≥25 kg/m2 and obesity as ≥30 kg/m2.
Breast-Feeding Practices
BFPs were assessed by interviewing the mother about current feeding practices and with a 24-hour recall. The first instrument consisted of asking the mother “Currently, how are you feeding your baby?” with the following options as possible answers: breast milk only; breast milk and additional water, tea, or juice; breast milk and formula; or formula only. Then a questionnaire to collect sociodemographic information was administered, and anthropometric measurements were made before asking again about feeding practices using the 24-hour recall instrument, in which the mother was asked, “In the previous day, what has your baby been eating?”
Information recalled by both instruments was recorded as to whether the infant received breast milk only, breast milk and additional liquids (water, tea, juice, etc), or other milk or formula. We also reported the type of milk used, formula-mixing methods, feeding method, and feeding schedule using the 24-hour recall.
Breast-feeding patterns based on reported current feeding practice and the 24-hour recall were classified based on the WHO categories: EBF infants (breast milk only including milk expressed or from a wet nurse and ORS, drops, or syrups, but nothing else), predominant breast-feeding (breast milk plus other liquids such as water, tea, or juice), and partial breast-feeding (other food or milk in addition to breast milk). 7 Predominantly and partially breast-fed infants were merged into a non-exclusively breast-fed (non-EBF) category for the analysis.
Measurement of Breast Milk Intake
Breast milk and non-breast milk water intakes were measured over a period of 14 days using the DMDOT. 6,17,18 Baseline saliva samples were collected from the mother and her infant before the dose of deuterium was given to the mother (day 0). After collection of the baseline saliva samples, a dose of deuterium-labeled water (D2O, 99.8 atom% D, Cambridge Isotope Laboratories Inc, Massachusetts) was given to the mother (60 g) and disappearance of the deuterium from the mother and its appearance in the infant was followed through saliva sample collections in both the mother and the infant at 1, 2, 3, 4, 13, and 14 days after the deuterium dose was taken by the mother. Saliva samples were collected after having assured that the mother and the infant had not eaten or drunk anything in the previous 30 minutes. Saliva samples were obtained using small pieces of cotton wool. The cotton wool was transferred to the barrel of a 20-mL disposable syringe, and the saliva was transferred into sterile tubes by compressing the used cotton wool using the plunger. Samples were stored at −20°C until analysis.
Saliva enrichment of deuterium was analyzed in duplicate, using a Fourier Transform Infrared Spectrometer (FTIR-8400 S; Shimadzu, Kyoto, Japan). Intake of breast milk and water from nonmilk sources was calculated by fitting the isotopic data to a model for water turnover in the mothers and infants, and the transfer of milk from mother to the infant, using a spreadsheet template that can be downloaded from the Nutrition section of the International Atomic Energy Agency Human Health Campus. 20
The data on non-breast milk water intake were classified into 3 categories according to the study published by Haisma et al 3 as follows: EBF (non-breast milk water intake <52 mL/d), predominant breast-feeding (non-breast milk water intake = 52-216 mL/d), and partial breast-feeding (non-breast milk water intake >216 mL/d).
Body Composition
Maternal body composition was determined using the same dose of deuterium given to the mother for measuring breast milk intake. Calculations of total body water were done using the back extrapolation method and assuming hydration of the fat-free mass (FFM) was 73.2%. Total body water (TBW) was estimated from the volume of distribution of the deuterium, corrected for nonaqueous isotope exchange. TBW (kg) = dose 2H2O (mg)/enrichment 2H in saliva at time 0 (mg/kg)/1.041; FFM (kg) = TBW (kg)/0.732; fat mass (kg) is the difference between body weight and FFM. 6
Infants’ body composition was also determined using the deuterium dilution technique but using the equilibrium or plateau method, which has been extensively used in measuring infant body composition. In brief, after a 3-week washout period since maternal ingestion of the deuterium dose, a baseline saliva sample was collected from the infant, and then a small oral dose of deuterium oxide (0.5 g D2O [99.8 atom%]/kg body weight) was administered to the infant using an oral syringe. A second saliva sample was obtained 3 hours after the dose was given and stored at −20°C until analysis in duplicate using FTIR spectrometry. Total body water was estimated as TBW (kg) = dose 2H2O (mg)/enrichment 2H in saliva (mg/kg)/1.041; FFM was calculated using Fomon hydration factors. 6
Quality Control
We followed steps for good quality data in dose preparation both in the field and in the laboratory. The dose was weighed accurately to at least 0.01 g by trained staff in the laboratory. We were sure that mothers did not eat or drink, and infants had not been fed for 30 minutes before saliva sampling. At the laboratory, all measurements were made against gravimetrically prepared standards, and the laboratory took part in an interlaboratory study organized by the International Atomic Energy Agency.
Statistical Analysis
Study data were collected (100% double entry data) and managed using REDCap electronic data capture tools hosted at INCAP (Guatemala City, Guatemala). Comparisons between infant and maternal characteristics in each feeding pattern category and differences between breast milk and non-breast milk water intakes among groups were done using Student t test.
The validity of a test is defined as its ability to distinguish between who has a disease and who does not. In this case, we will be able to identify the ability of dietary instruments to distinguish between infants that are exclusively breast-fed or not. Sensitivity is defined as the ability of the questionnaire to identify correctly those who are exclusively breast-fed, whereas specificity is defined as the ability of the questionnaire/instrument to identify correctly those infants who are not exclusively breast-fed.
To validate reported BFPs against the classification based on the DMDOT (reference method), we calculated sensitivity, specificity, and predictive values with their respective 95% confidence intervals. Analyses were performed using STATA version 12.0.
Results
A total of 36 eligible mothers signed consent forms (response rate = 72%). Scheduling conflicts was the most frequently cited reason for mothers not agreeing to participate.
Based on the current status of feeding practices, 18 infant–mother pairs were classified as EBF, 4 pairs as predominant, and 14 pairs as partial breast-fed. Regarding 24-hour recall, 22 infant–mother pairs were classified as EBF, 4 pairs as predominant, and 10 pairs as partial breast-fed. Predominant and partially breast-fed infants were merged into a non-EBF category for further analyses. The mean (SD) age of the mothers was 26.9 (5.9) years. Mean height, BMI, and body fat were 149.8 (5.9) cm, 26.7 (3.4) kg/m2, and 36.4 (6.3) %, respectively. There were no significant differences among mothers’ characteristics between feeding patterns (P > .05) by reported current feeding practice and 24-hour recall. In general, mothers have 8.1 (3.4) years of schooling and have an average monthly income of US$291.6 (135.9). Regarding the infants’ characteristics: 50% were girls, the mean (SD) age was 3.5 (0.4) months, mean weight, length, length for age, BMI for age, and total energy intake were 6.4 (0.9) kg, 59.5 (2.2) cm, −0.9 (0.8) z-score, 0.7 (1.3) z-score, and 596.4 (106.4) kcal/d, respectively. We found significant differences in infant body composition (FFM and body fat percentage; Table 1).
Characteristics of Mother–Infant Pairs by Feeding Pattern Based on Reported Current Feeding Practice and 24-Hour Recall.
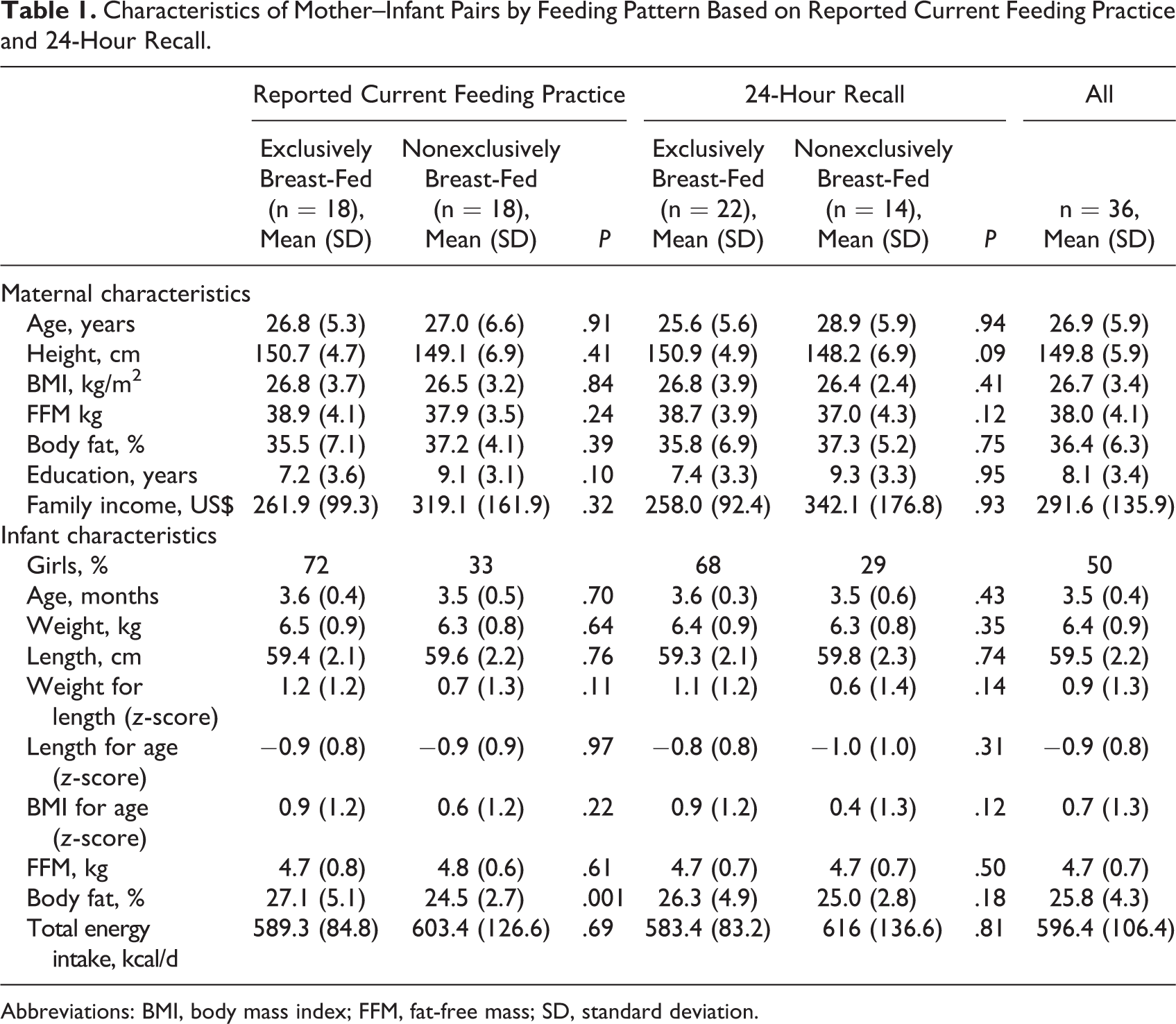
Abbreviations: BMI, body mass index; FFM, fat-free mass; SD, standard deviation.
A mean breast milk intake of 703.4 g/d was observed. The reported current feeding practice indicated breast milk intakes were higher in the EBF group than in the non-EBF group. The mean breast milk intake was 785.7 (733.4-837.9) g/d in the EBF group versus 621.2 (523.8-718.6) g/d in the non-EBF group (P = .003; Table 2). As expected, there was a lower intake of non-breast milk in EBF infants than non-EBF infants. EBF infants had a mean intake of non-breast milk water of 39.2 (17.5-60.9) g/d, a value that is within the classification (non-breast milk water intake <52 g/d) used by the DMDOT to classify EBF infants. 3 This amount was significantly higher among the non-EBF infants (Table 2).
Breast Milk and Non-Breast Milk Water Intake by Feeding Pattern Based on Reported Current Feeding Practice and 24-Hour Recall.
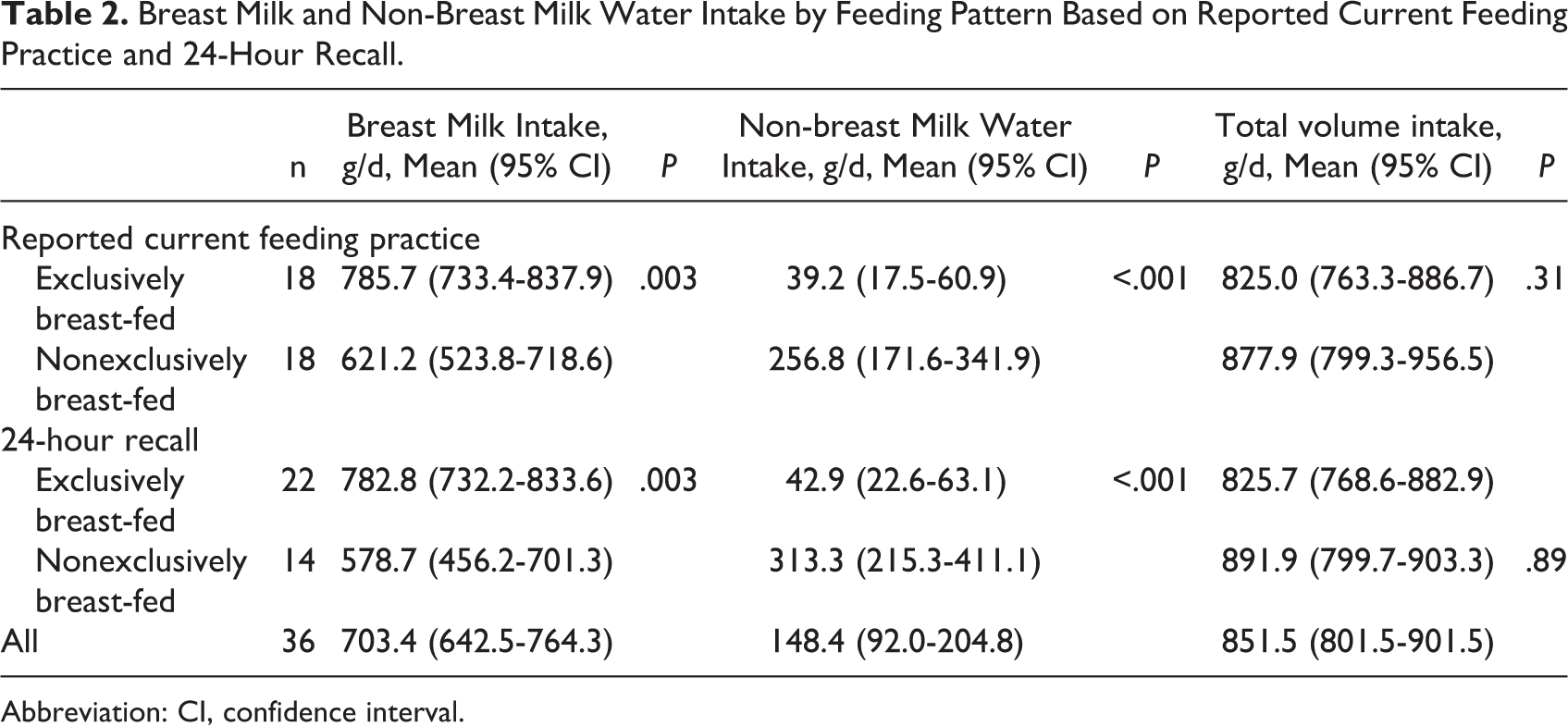
Abbreviation: CI, confidence interval.
Both self-report instruments overestimated the rate of exclusive breast-feeding. By reported current feeding practices, 50% were classified as EBF, whereas by 24-hour recall 61% were EBF, compared to 36% using DMDOT (Table 3). Thirty-three percent (n = 6) of the mothers who claimed to be EBF by reported current feeding practice were found to be non-EBF by DMDOT (Figure 2), whereas 41% (n = 9) of the mothers who claimed to be EBF by the 24-hour recall were found to be non-EBF by the DMDOT (Figure 3). It is important to note that of 4 maternal–infant pairs classified as EBF according to the 24-hour recall, 3 were correctly classified as non-EBF (according to the DMDOT) by the reported current feeding practice. Sensitivity to detect EBF infants from the mother’s report of current feeding practices was 92% (95% CI: 62%-99%) while from the 24-hour recall it was 100% (95% CI: 72%-100%, P < .01). However, specificity for both instruments was low, at 74% (95% CI: 51%-89%) for reported current feeding practice and 61% (95% CI: 39%-79%) for the 24-hour recall (P < .01).
Sensitivity, Specificity, PPV, and NPV of Reported Current Feeding Practice and 24-Hour Recall.
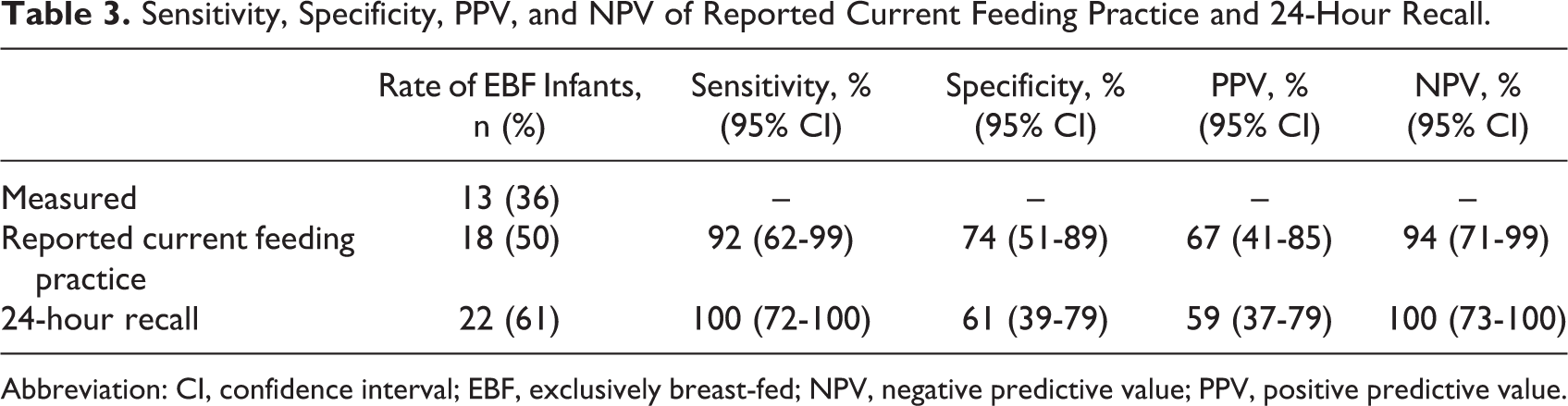
Abbreviation: CI, confidence interval; EBF, exclusively breast-fed; NPV, negative predictive value; PPV, positive predictive value.
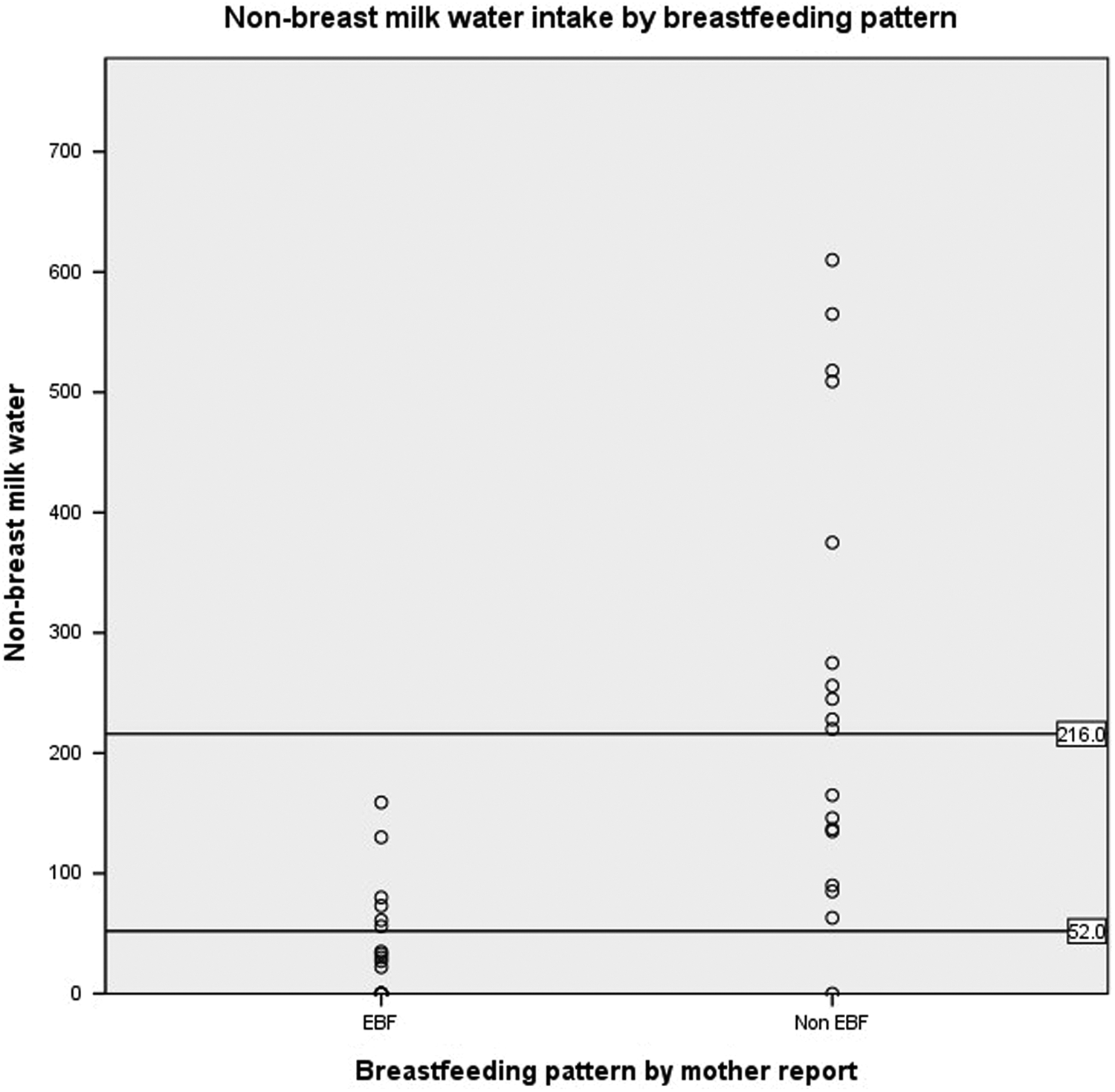
Misclassification of breast-feeding pattern by reported current feeding practice.
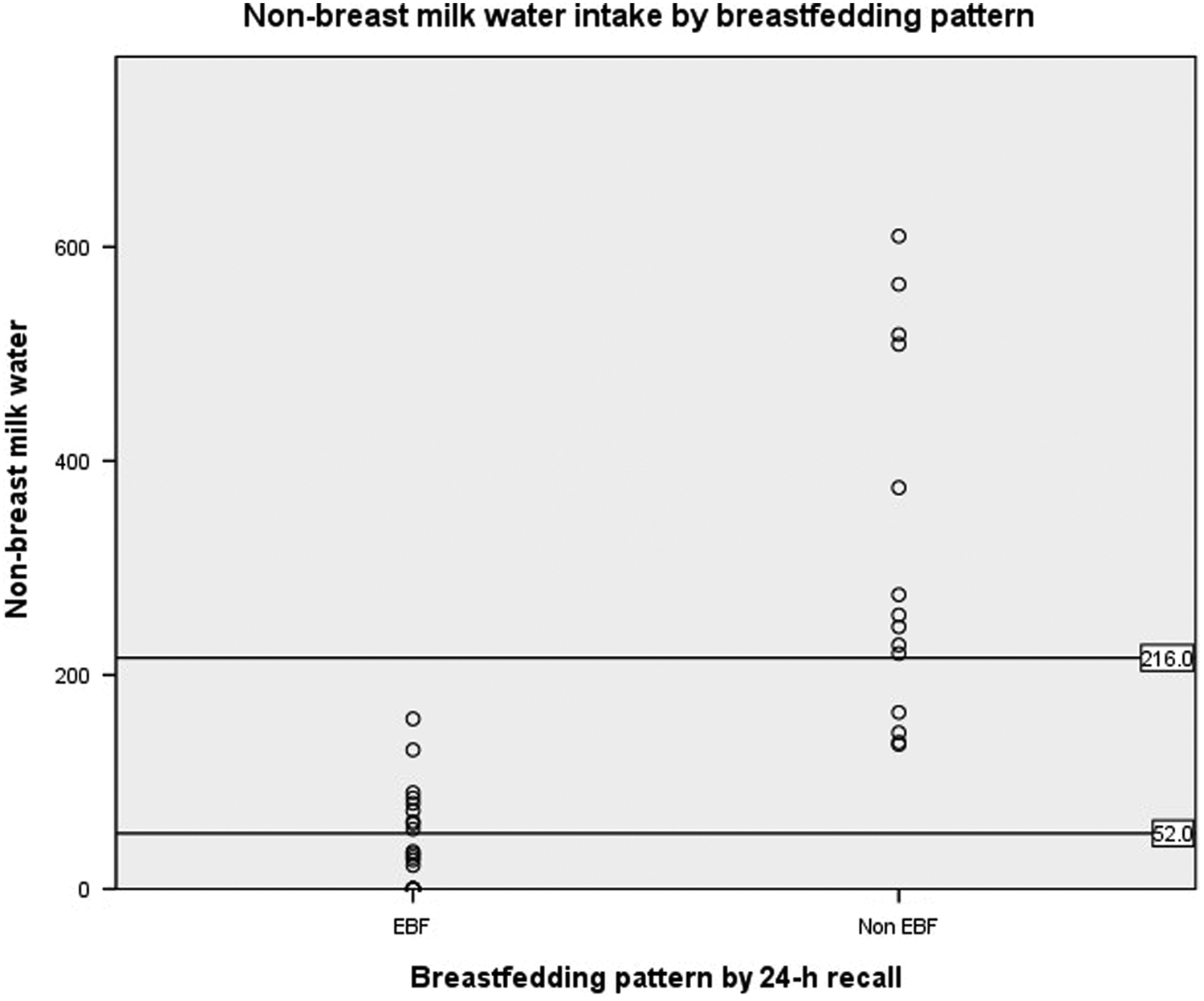
Misclassification of breast-feeding pattern by 24-hour recall.
Discussion
In the validation study of the DMDOT method against test weighing, the mean difference in breast milk intake between the methods was 12 ± 32 g/d. 19 The volume of non-milk water intake predicted by the model for exclusively breast-fed infants was 24 ± 30 g/d, although mothers reported none. This is a reflection of the errors introduced by the assumptions of the method. In the study of Haisma et al, 3 the range was 0 to 24 g/d in infants who were determined to be exclusively breast-fed (n = 35), based on a food frequency and amount questionnaire, which was applied on the last day of the deuterium study, and 53 to 216 g/d in infants who were predominantly breast-fed (n = 16). In this study, and the study of Medoua et al, 2 an arbitrary cutoff of 52 g/d was used, which is 1 g/d less than the non-breast milk water intake found in predominantly breast-fed infants in the Haisma study, which was based on 51 infants who were exclusively or predominantly breast-fed compared to only 9 infants in the original validation study, due to the difficulty in conducting this type of study. Considering that the WHO definition of exclusive breast-feeding only allows 5 mL essential medications and nothing else, it is unlikely that the use of this cutoff is grossly underestimating the true rate of exclusive breast-feeding.
According to our results, both reported current feeding practice and the 24-hour recall instruments overestimated exclusive breast-feeding. Nevertheless, the use of reported current feeding practice provided more accurate data to assess BFPs, as exclusive breast-feeding can occur in the previous 24 hours but not on a current daily basis. Our findings indicate that a large proportion of maternal–infant pairs are not EBF even though the 2 maternal recall methods indicate they are.
Measurement of breast milk intake has been recognized as a difficult task. 21 The use of the DMDOT to quantify breast milk and non-breast milk water intakes has several advantages over previously used methods such as test weighting and feeding frequency assessment. As it is an isotopic method, it does not interfere with normal behavior, and it is not subject to social desirability bias. 2
The mean total breast milk intake (703.4 of g/d) was comparable to the values found in other studies that have used the DMDOT. 2,3,22 Our data showed that the introduction of formula or other liquids significantly reduced the quantity of breast milk intake. This phenomenon was previously documented by Haisma et al. 3 In our study, mean intakes of both breast milk and non-breast milk water were significantly different between EBF and non-EBF groups. Total water intake was not different between the groups, suggesting volumetric intake consistency between the BF categories as classified according to the DMDOT method.
The 24-hour recall overestimates EBF rates by nearly twice the proportion determined using the reference method. Since Guatemala surveys, as well as many other population-based surveys in other countries, use the WHO-recommended 24-hour recall instrument to estimate EBF rates, it is possible that the reported EBF (49.6%) might be an overestimation of the true proportion of EBF infants. Although there is a small day-to-day variation in food intake in infants, 23 the main issue that has been reported when using the 24-hour recall instrument is that it overestimates the number of EBF infants, as some infants who are given other liquids (water, tea, and juice) may not have received them in the day before the survey. 7,10 Using the reported current feeding practice is likely to result in a lower proportion of infants misclassified as EBF compared to the 24-hour recall instrument.
A proper understanding and interpretation of population-based surveys of breast-feeding is important for public health decision makers to identify trends accurately and to design health policies and programs to improve EBF rates. 24 We suggest that more accurate data about BFPs are likely to be obtained by asking the mother, “Currently, how are you feeding your baby?” and give her these options: breast milk only; breast milk and additional water, tea, or juice; breast milk and formula; or formula only, rather than “In the last 24 hours, what has your baby been eating?”. Adding these responses to the question does not represent an increase in cost or time when interviewing mothers.
Our study had strengths and limitations. To our knowledge, this is the first study using the DMDOT to validate reported BFPs in Latin America. The advantage of using this technique is that it is independent of self-reporting and it is not subject to social desirability bias. Furthermore, it is unlikely that our results have been due to incorrect measurement or incorrect interpretation of the DMDOT method, as we used a standardized technique and the error in the curve fitting, as indicated by the square root of the mean square error, was small (<60 mg/kg). However, our findings should be considered in light of some limitations, as our sample was not representative of the Guatemalan population, and the present analyses were not meant to describe the breast-feeding situation in Guatemala. Furthermore, both methods were asked one after the other, and we did not mix up the order of these 2 recall methods. It should be noted that the number of mother–infant pairs by feeding pattern in the present study was too small, and predominantly and partially breast-fed infants were merged into a non-EBF category for the analysis. This did not allow us to study differences between the WHO-established breast-feeding categories.
In conclusion, the reported current feeding practice had similar sensitivity but higher specificity and concordance compared to the 24-hour recall although both methods overestimated EBF. The reported current feeding practice is the easiest and most accurate instrument to assess BFP in a public health setting. Furthermore, population-based surveys should consider the overestimation of EBF caused when using these BFP instruments.
Footnotes
Authors’ Note
The authors’ responsibilities were as follows—Manuel Ramirez-Zea designed the research study and reviewed the manuscript. Monica Mazariegos did data collection, performed statistical analysis, and wrote the first drafts of the manuscript. Christine Slater provided technical guidance on the use of the stable isotope technique, reviewed the manuscript, and made minor corrections to the English language. All of the authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Christine Slater is a technical officer employed by the International Atomic Energy Agency but has no part in decisions regarding financial matters. Monica Mazariegos and Manuel Ramirez-Zea had no conflicts of interest to declare.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was carried out with the support from the International Atomic Energy Agency. Additional support was received from the Fogarty International Center and National Institute of Aging of the National Institutes of Health under Award Number D43 TW009315.