
Abstract
Background:
Obesity has become a major public health issue in Latin America. Nutrition labels have been proposed as 1 strategy to address the obesity epidemic as they may encourage consumers to reassess their choices at point-of-purchase.
Objective:
We sought to determine the knowledge and stated use of the nutrition label in Guatemala.
Methods:
Caregivers were randomly selected from public and private schools in Guatemala City. Caregivers were interviewed to assess knowledge and behaviors related to nutrition label use. Anthropometric measurements were measured using standardized procedures. Descriptive statistics and χ2 test were used to determine the differences between school types.
Results:
Higher-income caregivers (88%) were more likely to be aware of nutrition labels, compared to those from low-income families (51%; P < .05). Furthermore, they were more likely to use it more frequently (42.2%) than their counterparts (18.3%; P = .03). Less than 50% of caregivers used nutrition labels for determining the amount of calories or nutritional content in a food portion, to compare nutrient content for different brands of the same food or to select products low in sugar, fat, and/or sodium.
Conclusions:
Our results provide evidence of the need to further explore nutritional label use and design that can better inform caregivers in Guatemala and other middle-income countries. Furthermore, given that the nutrition labels were for the most part rarely used by the participants in our study and that there are low literacy rates, other straightforward, easy-to-use strategies to communicate nutrition information at the point-of-sale could be useful to explore.
Introduction
Obesity has become a major public health issue in Latin America. 1 Between 1980 and 2008, the average body mass index (BMI) in Latin American people increased by 1 kg/m2 per decade—twice as fast as the global increase. 1 In Guatemala, between 1995 and 2009, overweight prevalence increased from 34.0% to 50.6%. 2 In response to this epidemic, many countries in the Americas have adopted specific policies and regulatory actions designed to make healthy choices the easy ones. 3
Currently, there is consistent evidence to suggest that nutrition labels are tools that stimulate food product reformulations and encourage consumers to reassess their choices at the point-of-purchase. 4 The Pan American Health Organization (PAHO) has urged governments to develop and implement norms for nutrition labeling that allow for quick and easy identification of energy-dense nutrient-poor products and sugar-sweetened beverages, which take into consideration Codex norms. 5 Currently, there are at least 50 countries worldwide that require nutrition labeling on most prepackaged foods, and several countries have developed or are using interpretative front-of-package nutrition labeling schemes on a voluntary basis (eg, Chile, Ecuador, Denmark, Norway, Sweden, Singapore, and the UK). 3 In Guatemala, according to the 2012 Central American Technical Regulation, 6 producers and retailers have to provide a list of the nutrient content of prepackaged food products, even in the absence of a nutrition or health claim. This regulation also permits and regulates the use of nutrient function and disease risk reduction claims.
In Latin America, to the best of our knowledge, only 1 study on nutritional label use has been published. 7 Therefore, this study sought to determine the knowledge and stated use of nutrition labeling in Guatemala, a Latin American middle-income country.
Methods
Caregivers were invited to participate by sending invitations with their children who attend to private (n = 3) and public (n = 3) schools in Guatemala City. After obtaining schools’ permission to invite caregivers to participate, we obtained a list of all students enrolled in prekindergarten and kindergarten (age range 4-6 years). We chose these grades, given that students at this age range mostly rely on their caregivers for food choice. We then randomly selected students to invite their corresponding caregivers to participate. Letters of invitations and consent forms (n = 650) were sent to caregivers (325 in public and 325 in private schools). School type was used as a proxy for socioeconomic status (SES). 8 Tuition fees in private schools average US$ 223.50 per month, whereas public schools are free. Therefore, caregivers of children from private schools were considered belonging to higher SES and those from public ones to lower SES.
Research assistants scheduled appointments at schools, conducted interviews, and performed anthropometric measurements. Caregivers were interviewed to obtain sociodemographic information. Caregivers’ awareness and behaviors regarding nutrition labels were assessed using a validated instrument developed by Carrillo et al. 9 Caregivers were asked if they knew what a nutritional label was and how often they used it to determine the amount of a nutrient in a food portion, compare nutritional content between brands of the same food, or select foods low in sugar, fat, and/or sodium. 9 Anthropometric measurements were taken using standardized procedures and calibrated equipment. The BMI (kg/m2) was calculated, and participants with a BMI of ≥25 were categorized as overweight/obese.
To ensure data quality, a double data entry procedure was followed. Descriptive statistics, t test, and χ2 test were used to determine statistical differences. Analyses were performed using STATA version 12.0. This study protocol was approved by the institutional review board of the Institute of Nutrition of Central America and Panama.
Results
A total of 316 caregivers returned signed consent forms (response rate 48.7%). Caregivers’ scheduling conflict was the most frequently cited reason for nonparticipation in both school types. Mean age and BMI (± standard deviation) were 34.2 (± 8.4) years and 27.4 (± 4.9) kg/m2, respectively. Prevalence of overweight/obese was 68.4%, and there was higher prevalence in the lower SES (76.3%) than higher SES (59.2%; P = .001). Furthermore, higher-income caregivers had higher educational level (72.8%) compared to their low-income counterparts (10.7%; P < .001; Table 1).
Sociodemographic Characteristics of Guatemalan Caregivers According to Socioeconomic Status.
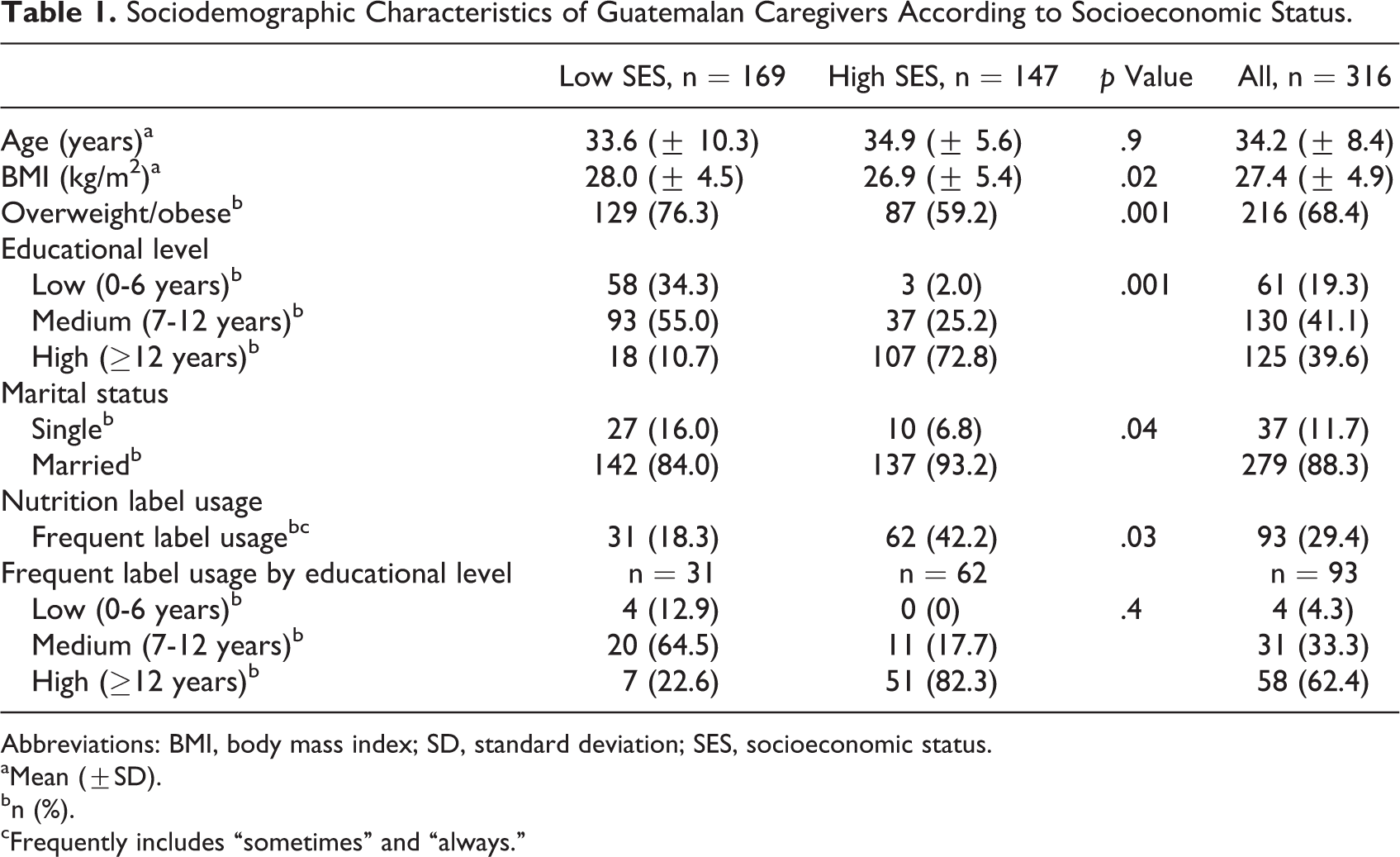
Abbreviations: BMI, body mass index; SD, standard deviation; SES, socioeconomic status.
aMean (±SD).
bn (%).
cFrequently includes “sometimes” and “always.”
Higher-income caregivers were more likely to be aware of nutrition labels (88%), compared to those from low income (51%; P < .05). Furthermore, they were more likely to use it frequently (42.2%) than their counterparts (18.3%; P = .03; Table 1). Also, among high SES, caregivers with more education were more likely to use it frequently; and regardless of the SES, there was a significant difference in nutrition label usage based on educational level (62.4% vs 4.3%; P = .008; Table 1).
Less than 50% of caregivers used nutrition labels for determining the amount of calories or nutritional content in a food portion, to compare nutrient content for different brands of the same food, or to select products low in sugar, fat, and/or sodium (Table 2). Regarding label use to compare 2 different brands, the highest prevalence was found among those of higher income (33% vs 12%). One-fifth of high-income caregivers used labels frequently to choose products low in sodium compared to 8% in low-income caregivers (P < .05; Table 2). Additionally, the caregivers were most interested in, regardless of their SES, total fat (45%), sugar (29%), and calories (20%). The main barriers to use the label included information is not clear (65%), lack of time (51%), and taste is more important (35%).
Percentage (95% Confidence Interval) of Guatemalan Caregivers Who Frequentlya Use the Nutrition Label and What They Use It for by Socioeconomic Status.
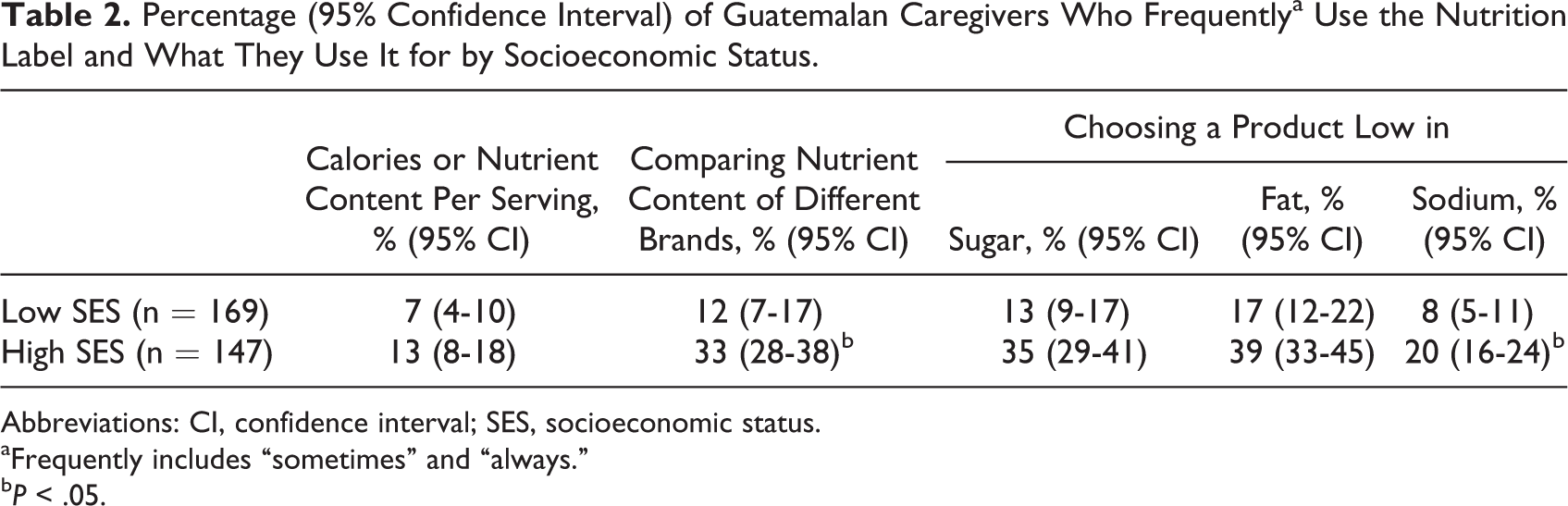
Abbreviations: CI, confidence interval; SES, socioeconomic status.
aFrequently includes “sometimes” and “always.”
b P < .05.
Discussion
According to our results, lower-income caregivers are less likely to use nutrition labels. Nutrition labels are required on all packaged foods and are regulated by the Guatemalan Food Control and Regulation Department according to the Central American Technical Regulation. 6 This regulation mandates reporting nutrients but does not specify the font size and location of the label. Although the labels have been implemented to provide consumers with nutrition information, their impact has yet to be determined in Guatemala. It is important to review the actual health impacts. 10 Our results showed that higher-income caregivers were more likely to be aware of what a nutrition label was and to use it more frequently than low-income caregivers. Also, within high-SES, caregivers with more education were more likely to use it frequently. Our findings are similar to other regional reports, 1 study in Mexico found that consumers with a high income were more likely to use nutrition labels than consumers of low income. 7 In high-income countries, nutrient lists are used more often by consumers with higher levels of nutrition knowledge, healthy eating behaviors, or incomes. 11 –13
Difficulty understanding nutrition labeling and lack of time at point-of-purchase have consistently been reported as the main barriers to use the label. 7,13,14 Our study population also reported that the taste was more important when purchasing. The knowledge of consumer behavior is helpful in designing other nutritional strategies to address the barriers in using the nutrition label. Our results indicate that information should be provided in a single easy-to-read format like the traffic light system implemented in Ecuador or warning labels in Chile. 15 –19 Additionally, other consumer strategies such as placing healthy food options in attractive and easily accessible settings should be explored. 20
Our study had strengths and limitations. To the best of our knowledge, this is the first published study assessing nutritional label in a middle-income country. However, our sample is not meant to be representative of the entire country, including rural Guatemala. Using school type (private vs public) as a proxy for SES might not fully explain the relationship between SES and nutrition label use. In addition, there is potential for selection bias if those who chose to respond were systematically different from nonresponders, with respect to both nutrition label usage and sociodemographic predictors. Finally, to look for an alternative, key informant interviews are needed to better understand the barriers to reading labels.
In conclusion, our results provide evidence of the need to further explore nutritional label use and design that can better inform caregivers in Guatemala and other middle-income countries. Furthermore, given that the nutrition labels were for the most part rarely used by the participants in our study and that there are low literacy rates, other straightforward, easy-to-use strategies to communicate nutrition information at the point-of-sale could be useful to explore.
Footnotes
Authors’ Note
Joaquin Barnoya supervised the research and made contributions to the manuscript, and Monica Mazariegos designed the research and was involved in data collection, performed statistical analysis, and wrote the manuscript. Both authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was carried out with the aid of a grant from the International Development Research Centre, Ottawa, Canada (Project number 107213-001). Joaquin Barnoya receives additional support from an unrestricted grant from the American Cancer Society and from the Foundation for Barnes & Jewish Hospital. Additional support was received from the Fogarty International Center and National Institute of Aging of the National Institutes of Health under Award Number D43 TW009315.