
Abstract
Aim:
This study assessed fat-related anthropometric variables and regional patterns of body size and adiposity of adolescents in Aba South LGA.
Methods:
A total number of 600 adolescents who were secondary school students aged 10 to 19 years wereselected from 61 registered secondary schools. A multi-random sampling technique was used to select the patients. Ethical approval and informed consent were obtained from the patients who participated in the study. Each patient was subjected to weight, height, mid–upper arm circumference (MUAC), and skinfolds measurements using standard methods. Body fat percentage was calculated by the formulas described by Slaughter, Siris, and Shailk equations. Descriptive statistics of frequencies, percentages, mean, and standard deviation were used to examine the gender-specific anthropometric indices. Chi-square and independent t test were also applied to determine the differences between the parameters or variables of the genders at P< .05.
Results:
The respondents aged 19 years had the highest measurement for triceps (14.60 mm), thigh (35.05 mm), and MUAC (25.95 mm), while those aged 18 years had the highest measurement for suprailiac (15.00 mm) and subscapular (16.94 mm). Females had more fat deposits than males in all the skinfold sites. They also had a significantly (P = .05) higher body fat percentage than males. A multiple regression analysis revealed that maximum calf fat was a strong predictor of body fat percentage of the patients.
Conclusion:
High prevalence of obesity was found in this study, and the 3 equations of body fat percentage showed similar findings that more females than males had higher body fat percentage.
Introduction
Adolescent obesity is a worldwide growing epidemic. High prevalence and increasing rates of adolescent obesity have been reported globally, including from countries such as United States, England, and mainland China. 1 The prevalence of overweight and obesity has increased dramatically over the past few decades in most industrialized countries. Obesity had reached epidemic proportion worldwide, especially in the developed nations both in children and in adults. 2 During the same period, many developing countries have undergone an economic transition from societies characterized by subsistence agriculture to increased urbanization and industrialization. 3
Obesity, especially central body fatness, is associated with disease morbidity and mortality and risk factors for coronary heart disease including dyslipidemia, insulin resistance, and hypertension. 4 Abdominal obesity has been established to show its onset during childhood. 4 The study of fat distribution among children and adolescents is complex because there are marked changes in circumferences and skinfold thicknesses during growth and development. Furthermore, the amount of intra-abdominal fat, which may have a primary role in adverse health outcomes, is small before adulthood. 4
It is clear that increased body fat affects health. Its distribution in the body influences the state of health of specific organs. According to its location, fat can be subcutaneous (under the skin) or visceral (around the organs). Visceral fat may interfere with the proper functioning of vital organs. There is a relationship between overall fat deposits and specific fat deposits. Fat around the middle-body section is associated with visceral fat. Abdominal fat is the most serious health risk.
Obesity is a multifactorial disease. Contributing factors include a modern environment of plentiful calories and low physical activity combined with inherited risk genes. 5 Pattern of fat distribution rather than obesity is of importance for cardiovascular morbidity and mortality. The accurate measurement of total and regional fat mass requires sophisticated and often expensive methods that have limited applicability in the clinical setting. 6 According to the authors, 6 their limited applicability in clinical setting is due to their inaccessible and unhandy nature of the equipment. Anthropometry is the single most portable, universally applicable, inexpensive, and noninvasive method available to assess the proportions, size, and composition of the human body. 7 However, it cannot differentiate between intra-abdominal and subcutaneous fat deposits. 8 The main aim of the study was to assess fat-related anthropometric variables and regional patterns of body size and adiposity of adolescents in Adolescents in Aba South L.G.A., Abia State, Nigeria.
Methods
The survey was carried out in secondary schools in Aba South LGA. A cross-sectional survey design was used. The study population consisted of secondary school students aged 10 to 19 years selected from 61 registered secondary schools (27 public and 34 private secondary schools) in Aba South LGA. A total of 600 adolescents who were secondary school students were selected.
There were 27 public and 34 private secondary schools in Aba South LGA. The names of the private and public schools were written in different pieces of papers and folded into 2 containers (one for private schools and the other for public schools). Ten secondary schools (5 public and 5 private secondary schools) were randomly selected by balloting without replacement. The sample of adolescents was selected using a multistage cluster random sampling technique. The first stage was identifying and determining the number of children aged 10 to 19 years in each of the schools. The distribution of these pupils by age and sex was obtained from class registers. The second stage involved calculating by simple proportion 10% of the children (10-19 years) in the sample size to obtain the study sample per school. This was done according to their ages and sexes. The third stage was actual selection of the respondents according to their ages and sexes in different classes. This was done using simple random sampling technique by balloting without replacement.
Ethical approval was sought and obtained for this study from the Aba South LGA authority. Permission was also sought from local education authority and the principals of the selected schools. The nature, purpose, and procedure of the study were explained to the participants in detail. Informed consent was sought from the participants and their parents. Only participants who gave their consent were allowed to participate. For those younger than 18 years of age, consent was obtained from their parents. The biodata of each participant was taken: This included age (as at last birthday) and sex. The measurements were taken in the classroom during recess with privacy given to both sexes. Trained research assistants were used to take the measurements. All the measurements were taken in duplicate, and an average was calculated.
Each patient was subjected to weight, height, arm circumference, and skinfolds measurements.
The weight of each patient was measured using a Salter scale (CMS weights Ltd, London). The patients were weighed without shoes and in light/minimum clothing. They were asked to stand on the scale with arms on the side and knees erect, 1 at a time. The measurements were taken to the nearest 0.1 kg.
Height was measured to nearest 0.1 cm using a microtoise height measure. Measurements were taken with patients bare footed, standing erect with feet parallel, and heels put together in line with methods of Jellife and Jellife. 9 Arm circumference was measured in the left arm using a nonstretchable tape placed firmly round the midpoint of the upper arm with the arm hanging freely by the side.
One skinfold examiner rater was used to reduce the interrater precision error. Skinfold thickness was measured at the left side of the body to the nearest 0.1 mm using a Holtain skinfold caliper (Procircle Fitness Training Products (Suzhou) Co. ltd, Jiangsu, China), at the following sites. (1) Triceps: This was measured halfway between the acromion process and the olecranon process. (2) Biceps: This was measured at the same level as the triceps skinfold, directly above the center of the cubital fossa. (3) Subscapular: This was measured at 20 mm below the tip of the scapula, at an angle of 45° to the lateral side of the body. (4) Suprailiac: This was measured at 20 mm above the iliac crest and 20 mm toward the medial line. (5) Thigh: This was measured in the midline of the anterior aspect of the thigh, midway between the inguinal crease and the proximal border of the patella. (6) Calf: This was measured at the level of maximum calf circumference on the medial aspect of the calf.
Body fat percentage was calculated using the following formula:
Slaughter equation (for boys):
Slaughter equation (for girls):
Shaikh Equations

where B = biceps skinfold thickness in mm, T = triceps (in mm), S = suprailiac (in mm), M = mid-arm circumference, and A = age in months.
Body density was calculated using equation of Durnin and Rahaman 10 for boys:

where Y = density and X = log (sum of skinfold thickness at 4 sites (triceps, biceps, subscapular, and suprailiac).
And for girls, the equation of Durnin and Womersley 11 was used:

where Y = density and X = log (sum of skinfold thickness at 4 sites (triceps, biceps, subscapular, and suprailiac).
Siri equation:

where Y = body density.
Data Analysis
The data collected were subjected to various analyses. Body density was calculated using equation of Durnin and Rahaman 10 for boys and Durnin and Womersley 11 for girls. Body fat percentage was calculated by the formulas described by Slaughter, Siri, and Shailk. Statistical analysis was carried out with the aid of statistical software package SPSS version 21.0. Descriptive statistics of frequencies, percentages, mean, and standard deviation were used to examine the gender-specific anthropometric indices. The data were normally distributed. Chi-square and independent t test were also applied to determine the differences between the parameters or variables of the genders. P < .05 was considered to be statistically significant.
Results
Table 1 shows characteristics of the patients presented by sex. Females had significantly (P < .05) higher values than the males for body mass index (BMI), weight, waist circumference, hip circumference, biceps, triceps, suprailiac, subscapular, calf, and thigh measurements. It also showed the body fat percentage of the respondents derived from 3 equations. Females had a higher body fat percentage than males based on 3 different equations. The differences were significant (P < .05). The fat percentage calculated using Siri equation was higher than that of Slaughter and Shailk equations.
Characteristics of the Patients Presented by Sex.
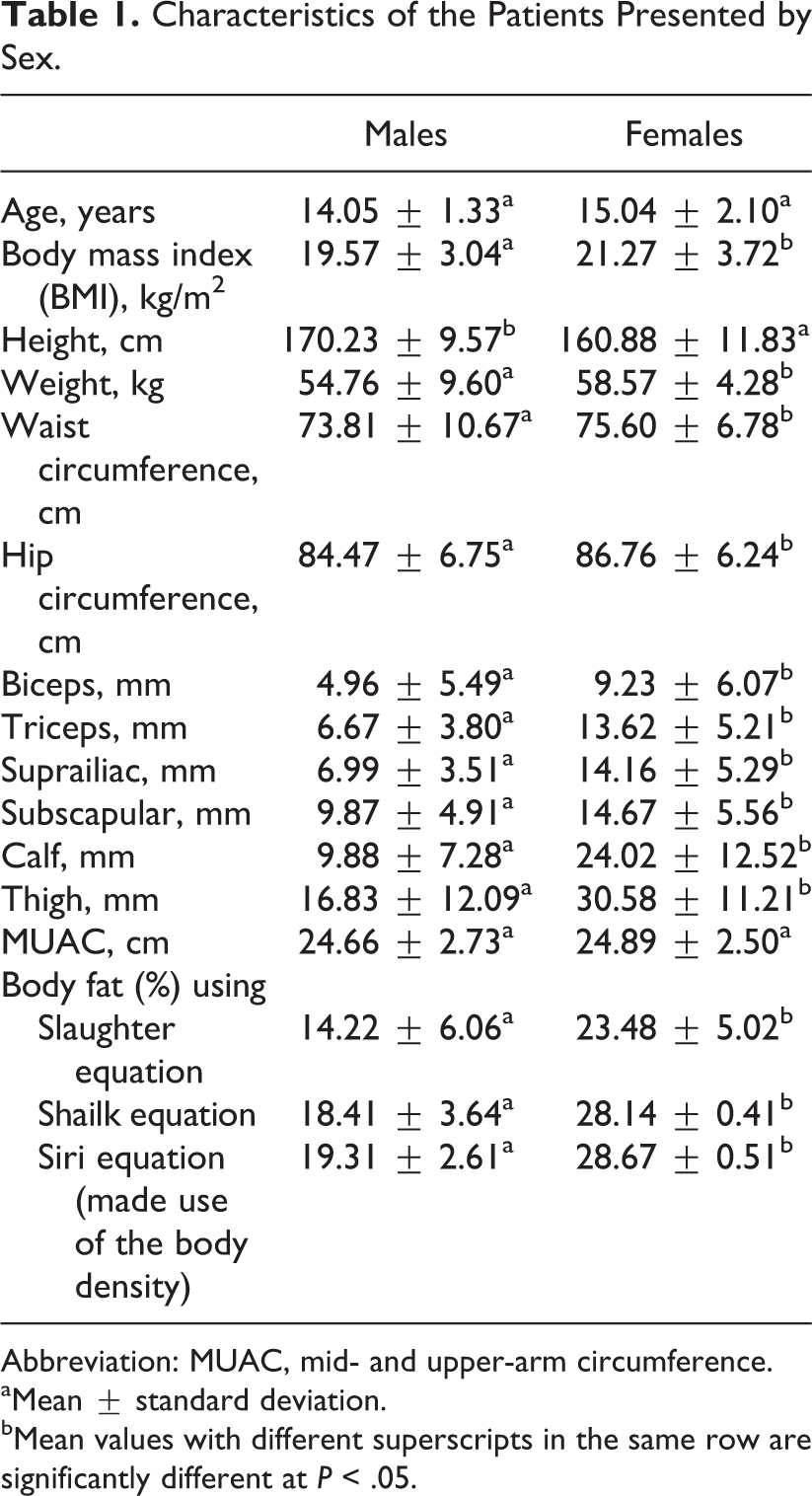
Abbreviation: MUAC, mid- and upper-arm circumference.
aMean ± standard deviation.
bMean values with different superscripts in the same row are significantly different at P < .05.
Table 2 shows that 3% of the respondents were underweight, 9.7% were overweight, and 3.5% were obese. More females were overweight and obese than the males.
Body Mass Index of the Respondents According to Sex Defined by IOTF Cutoff Point.a
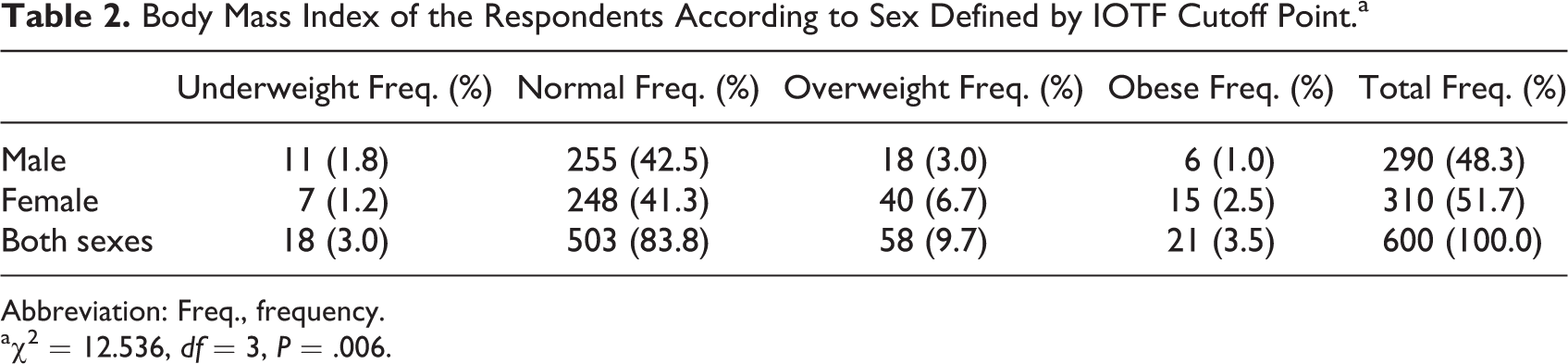
Abbreviation: Freq., frequency.
aχ2 = 12.536, df = 3, P = .006.
Table 3 shows the skinfold measurement of the respondents according to their ages. Respondents aged 10 years had the highest measurement for biceps (9.27 mm) and calf (31.33 mm). Respondents aged 19 years had the highest measurement for triceps (14.60 mm), thigh (35.05 mm), and MUAC (25.95 mm), while those aged 18 years had the highest measurement for suprailac (15.00 mm) and subscapular (16.94 mm).
Skinfold Measurement of the Respondents According to Their Ages (Mean ± SD).a
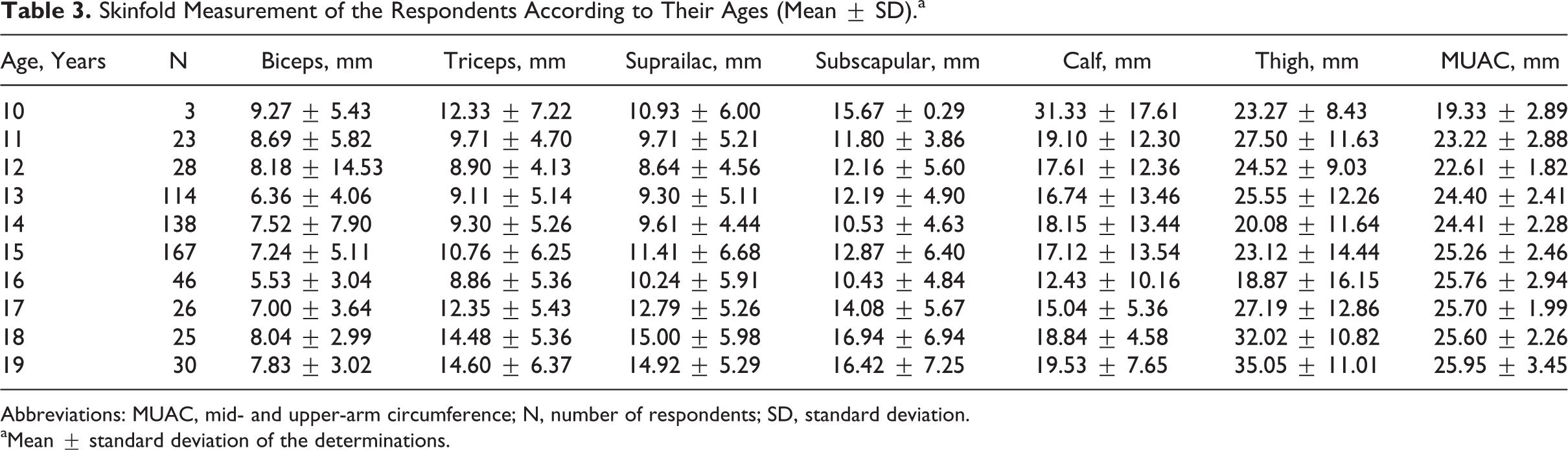
Abbreviations: MUAC, mid- and upper-arm circumference; N, number of respondents; SD, standard deviation.
aMean ± standard deviation of the determinations.
Table 4 shows the relationship of triceps, subscapular, calf, and thigh measurements on the body fat (%) of the respondents using multiple regression analysis for males and females. There was a significant (P < .05) relationship between the mean adjusted body fat (%) in calf measurements in males and females and in mid-thigh fat measurements in females only after allowing subscapular and mid-thigh measurements, respectively.
The Effects of Triceps, Subscapular, Calf, and Thigh Measurements on the Body Fat (%) of the Male and Female Respondents Using Multiple Regression Analysis.
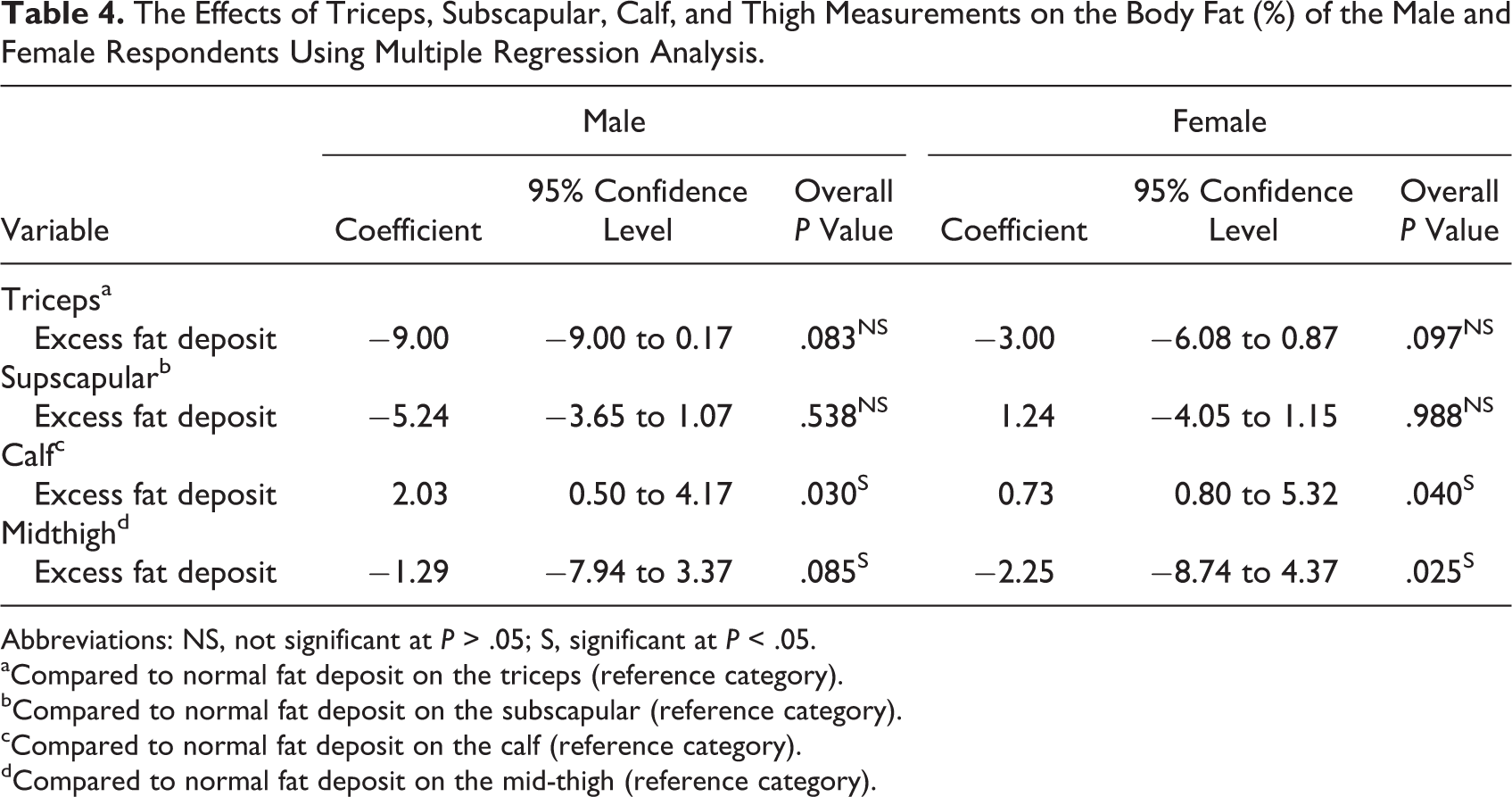
Abbreviations: NS, not significant at P > .05; S, significant at P < .05.
aCompared to normal fat deposit on the triceps (reference category).
bCompared to normal fat deposit on the subscapular (reference category).
cCompared to normal fat deposit on the calf (reference category).
dCompared to normal fat deposit on the mid-thigh (reference category).
Discussion
In this study, there were more females (11.2%) who had significantly (P < .05) higher body fat percentage than males. It is well established that women generally have a higher percentage of body fat than men. The higher body fat in girls could be attributed to the fact that adolescent girls tend to lay down more subcutaneous fat layer than boys during the growth spurt at puberty. 12 The percentage of body fat reported by Cole et al, 13 Onimawo and Ukegbu 14 on female adolescents, and Osisanya et al 12 on male adolescents are identical to that of this study. However, our results compared to that of Ijarotimi et al, 15 the respondents in this study had higher percentage body fat than theirs. Again the respondents in this study had lower BMI and body fat compared to their American counterparts but showed higher body fat values than Indian adolescents as reported by Deshmukh et al 16 and Mukhopadhyay et al. 17 The variations in the results can be linked to the place and time of these studies.
The study revealed that more females (51.7%) than males (48.3%) participated in the study. In this study, the prevalence of overweight and obesity was 9.7% and 3.5%, respectively. This was lower when compared to the prevalence of overweight (15%) and obesity (5%) in Iranian adolescents 18 and Indian adolescents (11.1% for overweight and 14.2% for obese). 19 The possible reasons for higher prevalence of overweight and obesity may be linked to their food habit, westernization, and government policies in these countries. The skinfold measurements of the patients in their different ages showed that it was not evenly distributed in the sample studied. The triceps, thigh, MUAC, suprailac, and subscapular measurements were higher in late adolescence. This implies that in this study, these skinfold measurements (triceps, thigh, MUAC, suprailaic, and subscapular) increase with age. This is not in agreement with a study done by Chun et al 20 who found that the thigh measurement of their respondents decreased with increased age. A greater percentage of females had excess fats deposits than males in these various skinfold measurement sites (triceps, subscapular, maximum calf, and midthigh). When triceps skinfold thickness was used as a measure of obesity in term of overfatness, fewer adolescents were classified as obese when compared to the prevalence of obesity using BMI. Only 1.5% of the respondents were classified as obese using triceps measurement though higher in females than in males. This finding was similar to the findings of Akinpelu et al 21 and Monyeki et al 22 who observed more females were obese than males when tricep skinfold measurement was used as the basis of obesity. Females are known to have more fat deposits than males. Thomas et al 23 and Novotny et al 24 have shown that a given level of subscapular skinfold (central body fat measure) remains a significant and independent predictor of coronary heart disease risk in adolescence. Obesity, especially abdominal adiposity, has been shown to be important determinants of insulin resistance. 25
Conclusion
Fat distribution assessments of the patients showed that some of them are at high health risk which might be implicated in noncommunicable diseases such as diabetes and cardiovascular diseases later in life. It was more prevalent in the adolescent females. The 3 different equations used in this study to measure fat percentage showed no differences which implied that one could be used instead of the other with expectation of similar result in a clinical setting. Periodic assessment of weight and fat distribution of children and adolescents should be carried out in schools and communities as part of school health program. This is essential for early detection, planning, and implementation of intervention programs to reduce morbidity and mortality associated with overnutrition.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.