
Abstract
Introduction
The study of human body composition includes different methodologies to examine the compartments of body mass (Wang et al., 1992). Given the negative relationship with metabolic parameters, fat mass (FM) estimation has potential relevance for clinics and nutritionists (Madden and Smith, 2016). Although dual-energy X-ray absorptiometry (DXA) and bioelectrical impedance analysis are widely used to estimate FM, these technologies require specialized equipment (Ward, 2018). In parallel, sex-specific equations based on skinfolds to predict body density and, consequently FM, were derived from hydrostatic weighing (Jackson and Pollock, 1985). Subcutaneous adipose tissue thickness was measured using a skinfold calliper (Jackson and Pollock, 1985). The equipment is portable, associated-protocols are non-invasive and consequently, skinfold callipers are often used as the most common instrument to estimate fatness (Madden and Smith, 2016).
Different type of callipers has been used in clinical practice. Note, however, protocols require standardized procedures and training in order to reduce intra and inter-individual variability measurement (Lohman et al., 1988). The instructions of international references called for the use of specific callipers which should exert a constant pressure in subcutaneous adipose tissue (Eston and Reilly, 2009). More recently, sophisticated callipers emerged as potential instruments to estimate subcutaneous adipose tissue thickness (Quintas et al., 2015; Tafeit et al., 2015). For example, a digital skinfold calliper (Adipsmeter) maintained a constant pressure of 10 gf/mm2 between tips while in traditional callipers pressure tended to decrease with the opening of jaw. The Adipsmeter is based on a Harpenden calliper, electronically adapted and incorporated a digital sensing system (LipoTool) reducing the intra-observer variability (Quintas et al., 2015). Among 49 participants, differences between estimated %FM obtained by a traditional calliper and LipoTool were considerable at higher values of fatness (Restivo et al., 2012). Comparisons between competing equipment were limited to body density estimations and did not contrast specific skinfold sites (Restivo et al., 2012). Age and sex-specific equations are systematically used by clinics to evaluate %FM. Meantime, disagreement between callipers may affects the interpretation of this parameter which in turns have impact on nutritional status and interventions.
Given the described differences between two concurrent techniques, the aim of the present study was to examine the quantitative agreement in specific skinfold sites using two different callipers (mechanical and digital) assessed by a certified observer. Since traditional callipers do not maintain a constant pressure, particularly in participants with superior values of FM, it was hypothesized differences between concurrent equipment.
Methods
Procedures and ethical requirements
The present study was approved by the Ethics Committee in the Institute Polytechnic of Coimbra (N.°92_CEIPC/2021; approval at 8th June 2021) and followed the recommendations from the Declaration of Helsinki produced by the World Medical Association for research with humans. Participants were previously informed about the nature, aim, risks of the study and, subsequently, provided written informed consent.
Participants
The sample included 22 healthy male Caucasian participants aged 19–30 years. Inclusion criteria were: (i) participants were physically active; (ii) body mass index < 30 kg.m−2.
Anthropometry
Skinfold thickness was measured at eight sites (triceps, subscapular, biceps, suprailiac, supraspinale, abdominal, thigh and calf) to the nearest 0.1 mm by certified observer and following the protocol recommended by International Society for the Advancement of Kinanthropometry (ISAK). Two different skinfold callipers were used: mechanical (see Figure 1) and digital (see Figure 2). The latter included an integrated system that also incorporates an antenna AirPCOn interfaced with a computer and a software application. Two measurements using different equipment were obtained individually for each skinfold. The mean of observations was retained for analysis.

Mechanical calliper.

Digital calliper.
Statistical analysis
Normality of distribution was checked with Shapiro-Wilk. Given the non-normality of distribution differences between two equipment were compared based Wilcoxon signed-rank test. Descriptive statistics (mean and standard deviation) for skinfolds were calculated. In addition, Bland-Altman plots and limits of agreement were calculated to visualize absolute differences and respective mean (Bland and Altman, 1986). Linear regressions were applied separately for each skinfold and sum of skinfolds. Afterwards, Shapiro-Wilk test was used to examine the distribution of residuals (i.e. normality of error) considering the two instruments.
Results
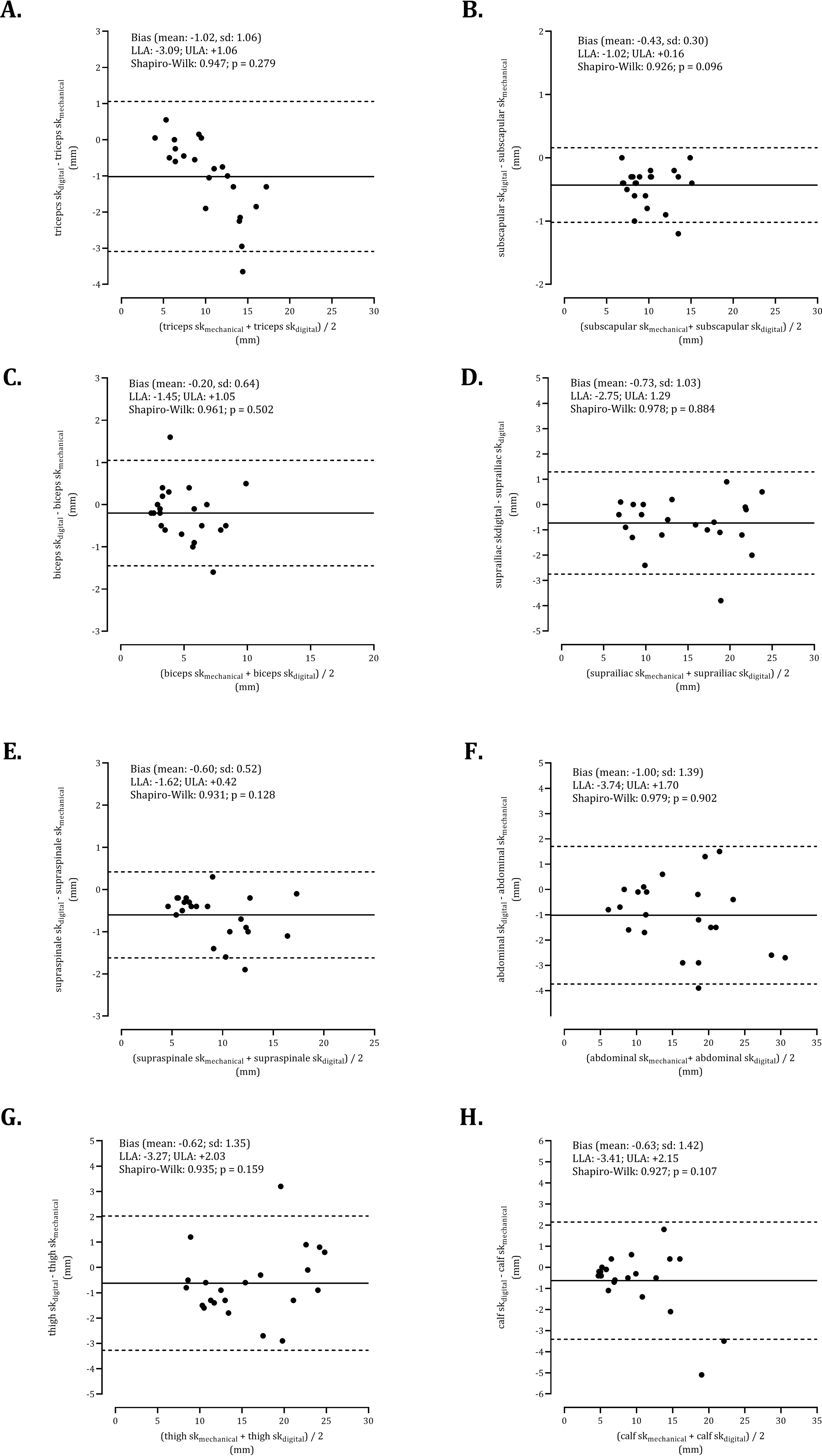
Agreement of digital and mechanical callipers for triceps (panel a), subscapular (panel b), biceps (panel c), suprailiac (panel d), supraspinale (panel e), abdominal (panel f), thigh (panel g) and calf (panel h) skinfolds.
Means and standard deviations for mechanical and digital callipers, z-score and significance value extracted from Wilcoxon signed-rank test.
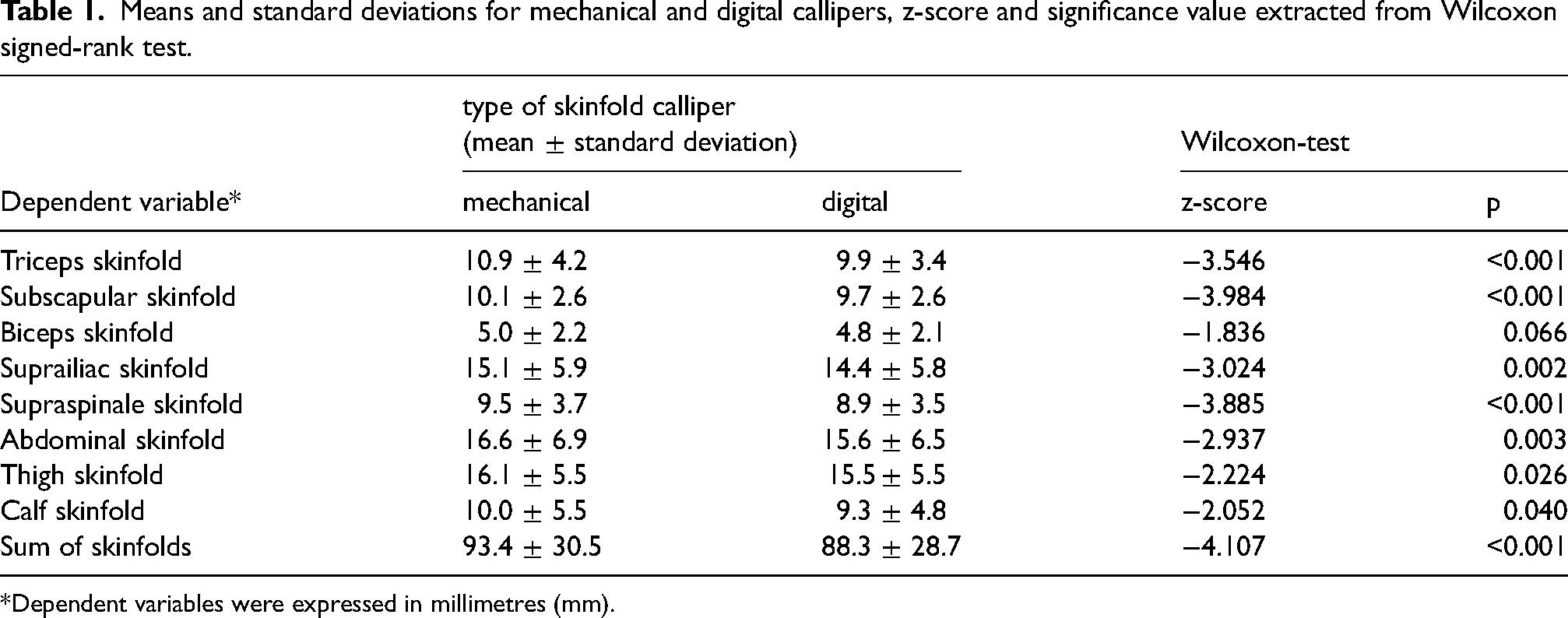
*Dependent variables were expressed in millimetres (mm).
Discussion
The aim of this study was to test the concordance between competing skinfold callipers. Adipsmeter which is part of an integrative system tended to produce systematically less values than mechanical calliper. Additionally, the agreement between callipers showed that the error was constant. Comparisons between different type of skinfold callipers were reported in studies of youth (Tafeit et al., 2015), adult and elderly (Restivo et al., 2012). For example, among 371 Estonian males aged 9–13 years, skinfolds measured using a plastic calliper were systematically higher in comparison to a lipometer. Meantime, the agreement between calipers decreased above 10 mm and thigh emerged as the most problematic skinfold (Tafeit et al., 2015). In the present study, differences between concurrent equipment were constant. The contrasted results across studies may reflect sampling, age variation or callipers used. The sample of this study considered healthy adult participants while, the Estonian sample involved pre-pubertal and adolescent males.
A previous study examined the agreement between estimated %FM using LipoTool (a similar calliper was used in the current study) and Harpenden callipers (Restivo et al., 2012). Among male and female participants, Harpenden calliper tended to produce systematically lower values than LipoTool which is consistent with the findings of present study. Interestingly, differences between equipment were considerable at higher values of %BF. These results may be explained by the differences between callipers. Nevertheless, the digital calliper has a unique characteristic – a transmission rate of 60 samples per second which in turns is related with the constant tissue compressibility during skinfold measurement (Quintas et al., 2015).
Differences between the mechanical and digital callipers were noted on the skinfolds examined in the present study. However, particular skinfolds emerged as relevant to estimate fat mass. The impact of lower limb skinfolds was previously assessed in a study with 21 male adults. Overall, thigh skinfold explained 79% of %FM assessed by dual energy x-ray absorptiometry (Eston et al., 2005). Additionally, triceps, suprailiac and abdominal skinfolds were included to predict body density (Jackson and Pollock, 1985). Therefore, associated-variation in skinfold callipers measurements should be considered when different studies are compared on estimated body composition.
The present study compared skinfold measurements using two type of skinfold callipers and did not test the concordance between equations. Future studies should contrast FM estimated by anthropometric equations (using the LipoTool) with more sophisticated methods of measuring FM or fat tissue (i.e. ultrasound imaging, air displacement plethysmography or DXA). In summary, assessment of subcutaneous adipose tissue using competing skinfold callipers showed different estimations in specific sites. This study highlighted the differences between equipment for measuring fatness with potential implications during clinical assessment.
Footnotes
Acknowledgements
Not applicable.
Funding
Not applicable.
Availability of data and materials
Data is available under a reasonable request of corresponding author.
Authors’ contributions
Faria A: conceptualization (lead), data curation (lead), formal analysis (lead), investigation (lead), methodology (lead), project administration (lead), resources (lead), supervision (equal), validation (equal), writing-original draft (lead) and writing-review and editing (lead); Martinho DV: conceptualization (lead), data curation (lead), formal analysis (lead), investigation (lead), methodology (lead), resources (supporting), software (lead), supersvision (equal), validation (lead), visualization (lead), writing-original draft (lead) and writing-review and editing (lead); Abreu B: data curation (equal), formal analysis (equal), methodology (equal), resources (equal), software (equal), validation (equal), visualization (equal) and writing-original draft (equal); Franco B: data curation (equal), investigation (equal), methodology (equal), resources (equal), software (equal), validation (equal), visualization (equal) and writing-original draft (equal); Carrilho L: data curation (equal), formal analysis (equal), investigation (equal), methodology (equal), software (equal), validation (equal), visualization (equal) and writing-original draft (equal); Azaruja M: data curation (equal), formal analysis (equal), investigation (equal), methodology (equal), software (equal), validation (equal), visualization (equal) and writing-original draft (equal); Mendes P: data curation (equal), methodology (equal), software (equal), validation (equal), visualization (equal) and writing-original draft (equal); Serra M: data curation (equal), methodology (equal), software (equal), validation (equal), visualization (equal) and writing-original draft (equal); Lemos J: data curation (equal), formal analysis (equal), methodology (equal), software (equal), validation (equal), visualization (equal) and writing-original draft (equal); Figueiredo JP: data curation (lead), formal analysis (lead), methodology (lead), resources (equal), software (equal), validation (equal), visualization (equal) and writing-original draft (equal)
Consent for publication
Not applicable.
Ethical approval
The present study was approved by the Ethics Committee in the Institute Polytechnic of Coimbra (N.° 92_CEIPC/2021; approval at 8th June 2021) and followed the recommendations from the Declaration of Helsinki produced by the World Medical Association for research with humans.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.