
Abstract
Background:
Sub-Saharan Africa is the last region to undergo a nutrition transition and can still avoid its adverse health outcomes.
Objective:
The article explores emerging responses to “bend the curve” in sub-Saharan Africa’s nutrition transition to steer public health outcomes onto a healthier trajectory.
Methods:
Early responses in 3 countries at different stages of food system transformation are examined: South Africa—advanced, Ghana—intermediate, and Uganda—early. By comparing these with international experience, actions are proposed to influence nutrition and public health trajectories as Africa’s food systems undergo rapid structural change.
Results:
Arising from rapid urbanization and diet change, major public health problems associated with overweight are taking place, particularly in South Africa and among adult women. However, public health responses are generally tepid in sub-Saharan Africa. Only in South Africa have policy makers instituted extensive actions to combat overweight and associated noncommunicable diseases through regulation, education, and public health programs. Elsewhere, in countries in the early and middle stages of transition, public health systems continue to focus their limited resources primarily on undernutrition. Related pressures on the supply side of Africa’s food systems are emerging that also need to be addressed.
Conclusions:
Three types of intervention appear most feasible: maternal and child health programs to simultaneously address short-term undernutrition problems while at the same time helping to reduce future tendencies toward overweigh; regulatory and fiscal actions to limit access to unhealthy foods; and modernization of Africa’s agrifood food system through job skills training, marketing reforms, and food industry entrepreneurship.
Introduction
This article explores the implications of Africa’s rapid, ongoing food system transformation for consumer nutrition and public health. In the face of accelerating urbanization, the marketed share of food production now accounts for over 50% of the value of food consumed in many parts of sub-Saharan Africa. 1 Growing urban food markets, in turn, imply longer supply lines, expanded wholesale and retail distribution systems, and an increased need for storage, food preservation, processing, and packaging. 2 Parallel increases in per capita incomes trigger well-known dietary changes, including increased consumption of dairy and meat products, higher demand for fresh fruits and vegetables, and increased demand for processed and prepared convenience foods. 3 –5
As a result of these changes, Africa and other developing regions have entered the early stages of an accelerating world-wide nutrition transition. 6 –8 Popkin’s classic exposition of the nutrition transition describes how dietary changes and reductions in physical activity associated with urban lifestyles together translate into growing rates of overweight, obesity, and related noncommunicable diseases (NCDs). 3 The same risk factors—including diet change and urbanization—contribute to a parallel decline in oral health and increased tooth decay in low-and middle-income countries where oral health services and fluoride use are both limited. 9,10
Apart from South Africa, where over 40% of the adult population is now overweight, most sub-Saharan African countries have come late to the nutrition transition. 11 Some have begun to discuss possible latecomer advantages for the rest of sub-Saharan Africa, suggesting that valuable lessons can be learnt from elsewhere so as to take proactive early actions to “bend the curve” onto a more favorable trajectory (Figure 1). 7,12,13
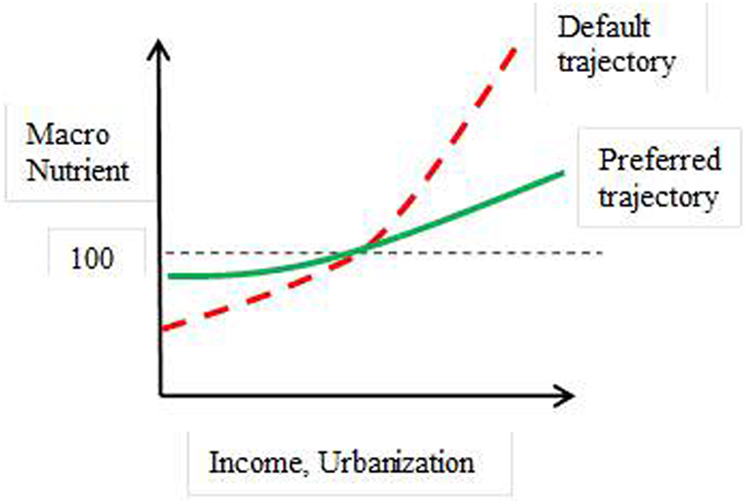
Bending the curve in Africa’s nutrition transition. Adapted from Minnaar et al. 12
The article first examines the current state of the nutrition transition in sub-Saharan Africa. This discussion highlights the significant heterogeneity in outcomes—across regions, within countries, and even within households. The article then examines emerging responses aimed at protecting consumer health in 3 African countries at different stages of the agrifood system transition. It concludes by identifying emerging early actions that could help moderate the looming negative public health consequences of Africa’s ongoing agrifood system transformation.
Methods
The following overview of the state of the nutrition transition in sub-Saharan Africa relies on secondary data from a variety of sources, including the World Health Organization (WHO), the Food and Agriculture Organization (FAO), and localized survey efforts and subject matter reviews by Africanist researchers. Analysis then turns to emerging responses from African countries at different stages in their food system transformation. For this purpose, we use the classification system developed by Kaneene et al 14 using 2 principal indicators that drive food system transformation. The first is urbanization, which largely governs the share of food marketed as well as the length of supply chains and the level of food storage, processing, packaging, and distribution. The second indicator, per capita income, drives consumer consumption diversification out of staples (such as maize, millets, sorghum, roots, tubers, and pulses) into higher value perishable foods such as meat and dairy products, fresh fruit and vegetables, processed foods and foods prepared by restaurants, fast-food outlets, and informal food outlets—a relationship often referred to as Bennet’s Law.
We have selected 3 countries for review, one at each level of food system transformation: South Africa, the most developed and most sophisticated agrifood system in Africa and with the highest rates of overweight and obesity (top tier), Ghana (middle tier), and Uganda (bottom tier).
Africa’s Emerging Nutrition Transition
Overnutrition and NCDs
Over the past 30 years, the share of overweight population has increased rapidly in Africa. Since 1980, the share of overweight adults has nearly doubled, from 17% in 1980 to 30% in 2008 (Table 1).
Prevalence of Overweight Adults (BMI > 25), by Region.a
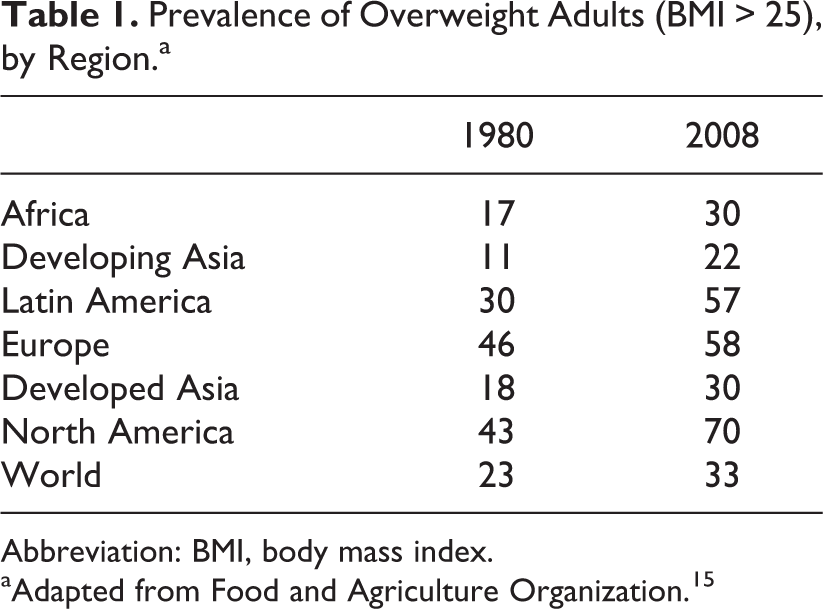
Abbreviation: BMI, body mass index.
aAdapted from Food and Agriculture Organization. 15
Regional differences have emerged very clearly, with overweight and obesity levels highest in Southern and Northern Africa and far more moderate, on average, in other African regions. Southern African tops the scales across the continent, reporting adult obesity rates of 31% (Table 2).
Dimension of Africa’s Double Burden of Malnutrition, by Subregion.a
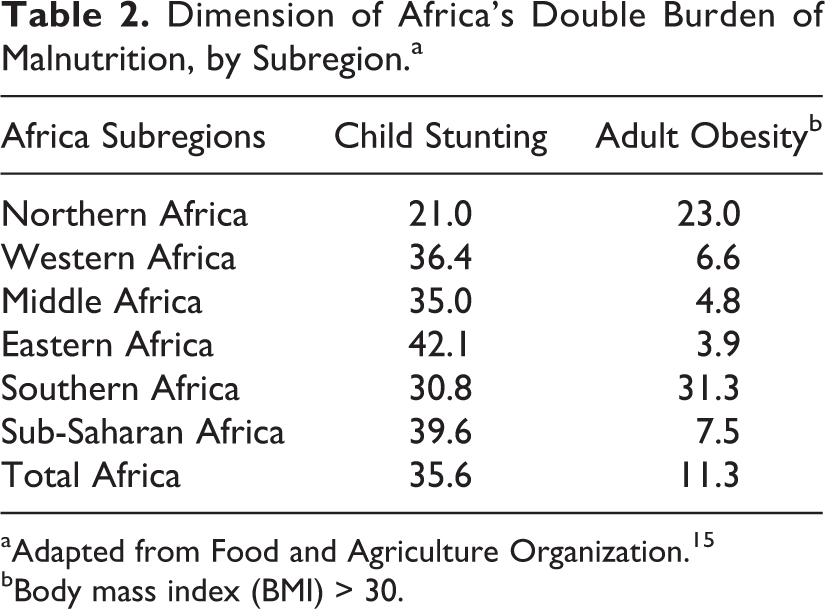
aAdapted from Food and Agriculture Organization. 15
bBody mass index (BMI) > 30.
Adult women, across all regions, have proven most vulnerable to weight gain during the nutrition transition, given biological differences in how women and men metabolize fat. In South Africa in 2012, 64% of adult women were overweight or obese compared to 31% of men. 16 Given that obese individuals face higher risk of heart disease and given the high prevalence of overweight among African women, they frequently prove more vulnerable to diabetes and cardiovascular disease than men. 17
The prevalence of NCDs such as diabetes, hypertension, and cardiovascular disease has increased rapidly in the face of these growing overweight populations. Over the past 20 years, prevalence rates of type 2 diabetes have increased by a factor of 10 in sub-Saharan Africa. 18 Projections suggest that the incidence of diabetes will more than double in Africa between 2000 and 2030, among the highest growth rates in the world (Table 3). Evidence from across sub-Saharan Africa suggests that rates of hypertension typically range between 15% and 30%, with higher rates in this range prevailing in urban areas. 20 As a result, hypertension and related cardiovascular diseases are placing increasing pressure on public health systems in Africa. 21
Millions of Cases of Diabetes, 2000 and Projections for 2030.a
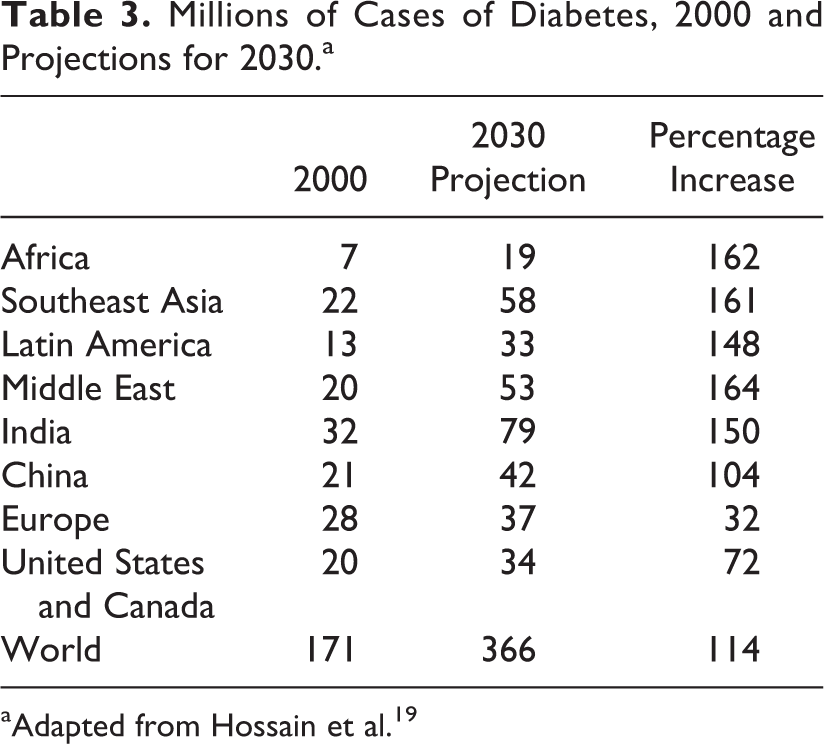
aAdapted from Hossain et al. 19
Double Burden of Undernutrition and Overnutrition
Growing numbers of overweight populations and attendant NCDs, on top of already high levels of undernutrition, have begun to place a double burden on already stretched public health systems. 7,11,22,23 This double burden has emerged most prominently in the Southern African countries of South Africa, Swaziland, and Lesotho, where rates of undernutrition and overnutrition both exceed 30% (Table 2, Figure 2). This double burden manifests itself in simultaneously high rates of underweight and overweight adult women in many countries. Already, a majority of African countries have reached the point where the share of overweight women exceeds underweight (Figure 2). Biological differences in women leave them particularly vulnerable to weight gains as diets shift to include greater proportions of oils and refined cereal and sugar-rich products. Over roughly the past 2 decades, nationally representative data from demographic and health surveys in 19 African countries identify an increasing proportion of overweight women, in both rural and urban areas. Underweight shares, though generally declining over the same period, show episodic increases in a few countries (Senegal, Rwanda, and Madagascar), possibly as a result of intermittent poor harvests or food price spikes associated with the world food crisis. 8
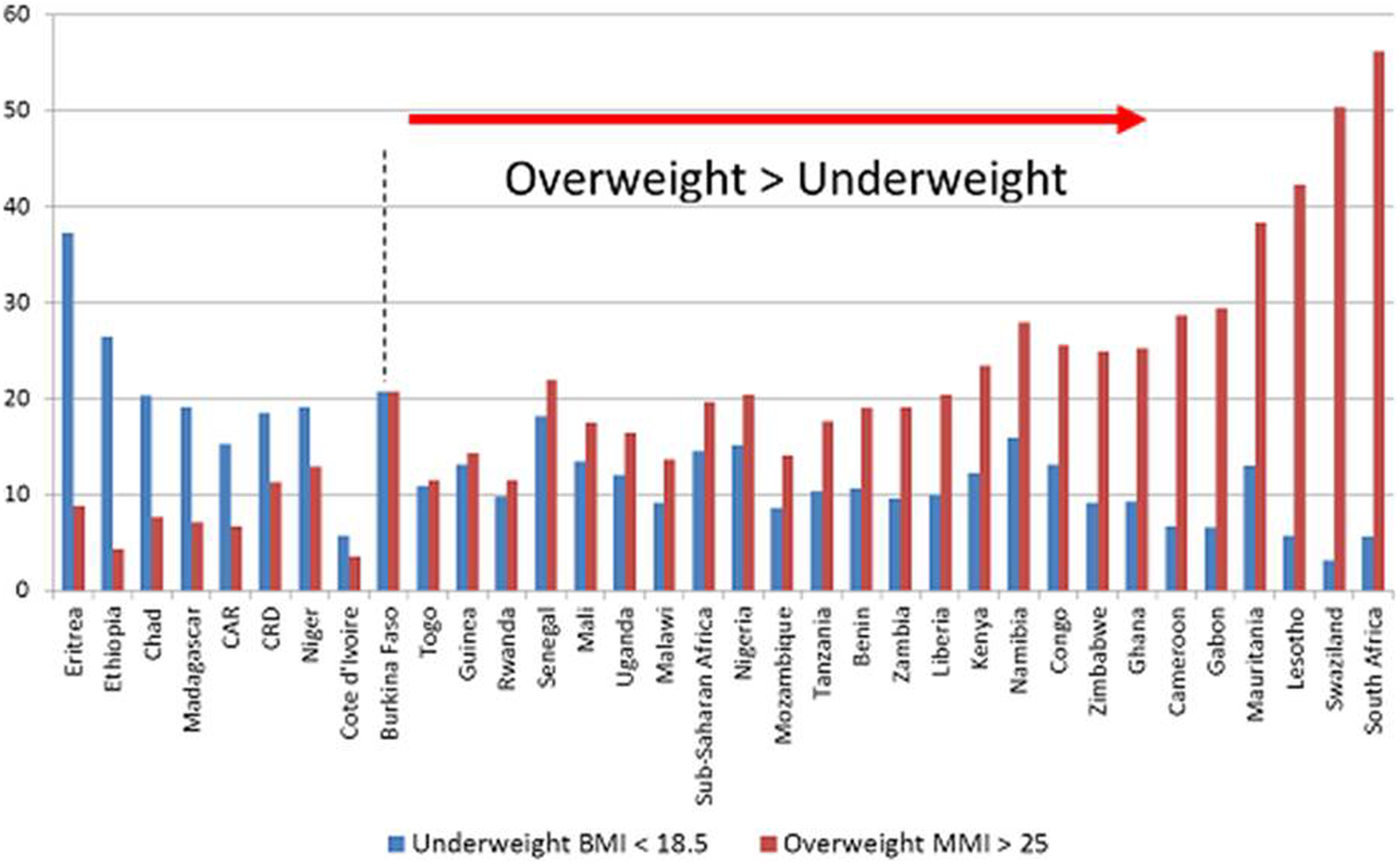
Africa’s double burden (percentage of adult females underweight and overweight). Adapted from World Health Organization. 11
A possible intergenerational biological link may, in part, explain this emerging double burden where undernutrition in one generation translates into the rapid emergence of overnutrition in the next. The Barker or “thrifty phenotype” hypothesis holds that undernourished mothers, who deliver low birthweight babies, may trigger metabolic changes in utero, which make these children more susceptible to weight gains later in life. 24 The biological responses begin when fetal deprivation triggers metabolic and endocrine adaptations that continue throughout the life of the child, into adulthood, leading to higher risk of weight gain, obesity, and heart disease in later life. A growing body of evidence consistent with this hypothesis has led to its increasing acceptance. 7,18,23,25,26 In South Africa, for example, evidence from the North West province suggests that stunted girls prove more prone to weight gains in later life than girls of normal height. 27 The thrifty phenotype mechanism may help explain why problems of overweight appear to be emerging earlier in the development process in late-developing countries and regions. 25
Implications for Oral Health
In contrast with obesity and overweight trends—for which African countries are beginning to see growing evidence in some population groups—comparative studies of oral health suggest that Africa begins from a healthier position than many other regions. Compared to other developed and developing regions, Africa exhibits low levels of dental caries (decayed or filled teeth) 28 and tooth loss. 29 At the same time, periodontal disease (gingivitis) remains widespread and severe, poor oral hygiene remains the norm, and calculus deposits are common. 29 Some dental specialists hypothesize that natural levels of fluoride in some regions (notably in the Great Rift Valley of East Africa) may confer natural protection on some segments of the African population. 30
Evidence from other developing regions raises concerns about the potential adverse consequences of the nutrition transition for oral health. Studies from Latin America, for example, report caries in 40% to 90% of children under 6 years. 9,31,32 In small children with baby teeth, for whom Latin American and Asian studies suggest problems frequently arise, untreated dental disease inflicts chronic pain, leading to sleep loss, school absences, and reduced concentration and performance. 33,34
Specialists project a worsening of oral health in Africa in the face of ongoing, rapid food system transformation. 35,36 The growing prevalence of major risk factors underpins forecasts of rapid deterioration in oral health in Africa. Sugar consumption, a key risk factor in tooth decay, is projected to increase in Africa at among the fastest rates in the world in coming years. 34,37 –39 Urbanization, likewise, consistently emerges as an additional risk factor for tooth decay in developing countries, the likely causal mechanism being the increasing prevalence of refined cereals and prepared foods on which plaque-producing bacteria feed and thereby demineralize tooth enamel. 37,40,41 Current forecasts of rapid urbanization across Africa over the coming decades suggest that the continent will become majority urban by 2030. 42 Tobacco consumption constitutes a third key risk factor for various oral and cardiopulmonary diseases. 30 Apart from South Africa, where smoking levels have declined over the past 20 years in response to active antismoking campaigns, levels of tobacco use have risen steadily elsewhere in Africa, growing by 68% between 1990 and 2010. 43 As a result of these general increases in critical risk factors, oral health specialists project an increasing burden on dental health in sub-Saharan Africa. 28,41
Experience and Responses From African Countries at Different Stages of Food System Transformation
The following discussion compares nutritional outcomes and public health responses in 3 African countries at different levels of food system transformation: South Africa, Ghana, and Uganda.
In South Africa, where 62% of the population lives in urban areas, processed foods account for 90% of the value of foods consumed (Table 4). In contrast, Uganda houses only 16% of its population in urban areas and processed foods account for 44% of the value of foods consumed (Table 4). Moreover, the level of processing remains much lower in Uganda. Highly processed foods (note 1), such as breads, biscuits, sweets, carbonated beverages, modern alcoholic drinks, cheeses, processed meats, canned foods, and prepared foods, account for only about 19% of food purchases in Uganda compared to 55% in South Africa. 1
Contrasting Nutritional and Public Health Outcomes in Countries at Different Stages of Food System Transformation.a
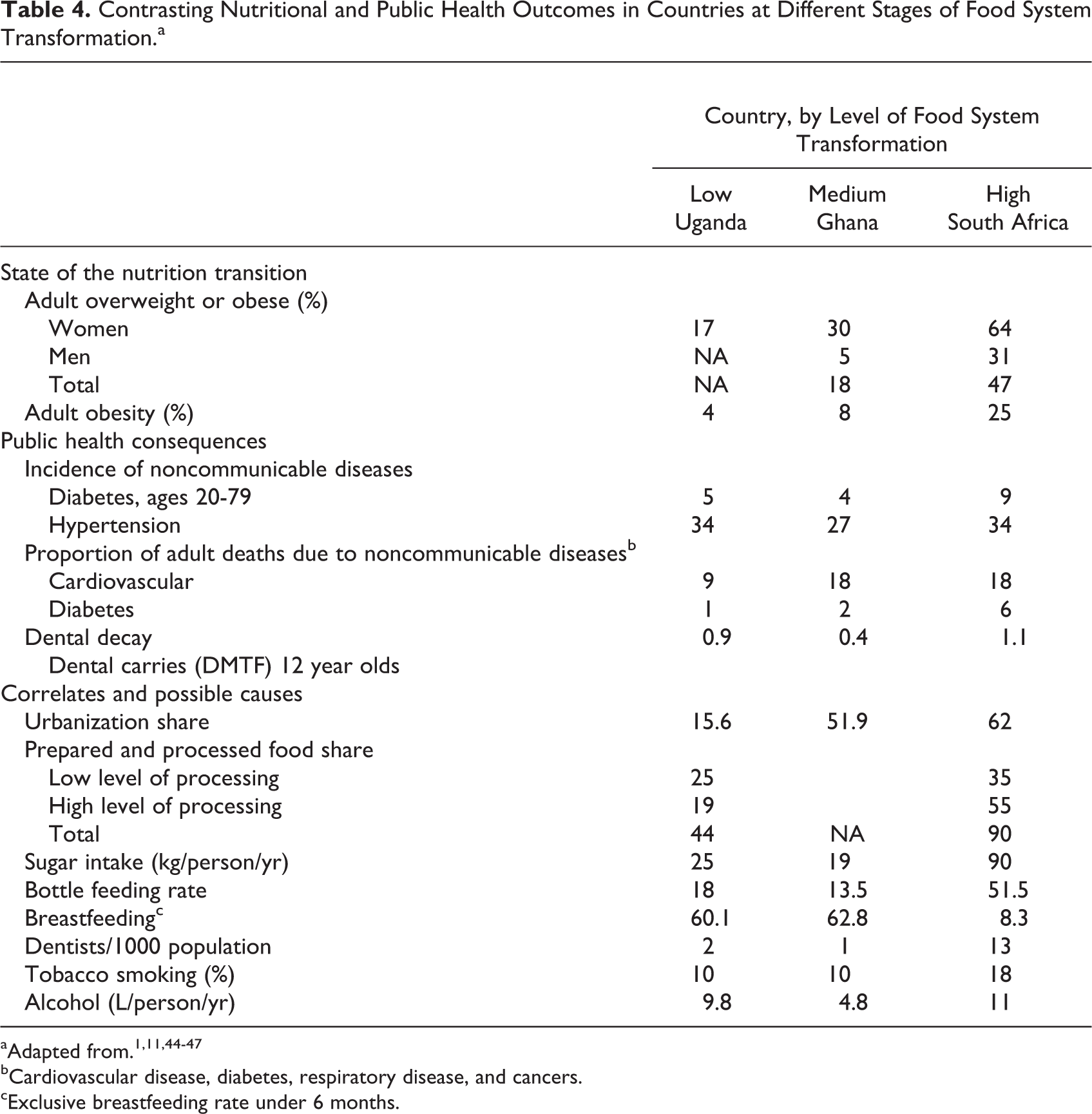
bCardiovascular disease, diabetes, respiratory disease, and cancers.
cExclusive breastfeeding rate under 6 months.
Nutritional and public health outcomes differ significantly as well (Table 4). High levels of overweight and obesity in South Africa contrast with much lower levels in Ghana and Uganda. South Africa’s adult obesity rate of 25% exceeds Uganda’s 4% rate by a factor of 6. Likewise, the incidence of NCDs is generally larger in South Africa, particularly diabetes. Hypertension, however, emerges as a prominent problem everywhere affecting one-fourth to one-third of adults in all 3 countries.
Differences in risk factors reflect these differing outcomes. South Africans exhibit higher rates of urbanization, processed food consumption, sugar intake, and infant bottle feeding as well as correspondingly lower rates of breastfeeding than Ghana or Uganda. These differing situations, in turn, lead to differing levels of public recognition and response to emerging overnutrition and related health problems as the following discussion reveals.
Highly Modernized Agrifood System: South Africa
Food system
South Africa has long had a well-developed food manufacturing industry producing Western-style food products. A total of roughly 1800 food manufacturing companies operate in South Africa. 48 Large corporations dominate food manufacturing, with the top 10 companies accounting for more 50% of packaging food sales. Supermarkets dominate food retailing in South Africa. In 2010, they accounted for 68% of the retail food sales, up from 50% in the early 2000s. 49 Four companies control over half the food retail market. 48 Supermarkets shape not only consumer choices but also the supply structure of the South African postfarm food system. Most supermarket chains have developed company-specific procurement systems characterized by private procurement agents, preferred suppliers, centralized procurement through distribution centers, and the imposition of quality standards on suppliers and producers. 49
Prepared foods, “fast foods,” are also a major component of food retailing in South Africa. Steyn et al reported that in South Africa, 11.3% of the population frequently (2 or more times a week) consume street food and 6.8% frequently purchase fast foods. 50 The figures for Johannesburg and Pretoria were much higher, 18.9% and 14.7%, and much lower for the rural and very much poorer Northern Cape province, 1.8% and 2.6%, respectively.
The more diverse noncorporate component of the food market in South Africa includes general dealers, spaza shops (informal convenience stores in townships, often in people’s homes), and street food vendors. 49 The street vendors market primarily to black South Africans commuting to and from work.
Nutrition transition
The types of foods that South Africans consume and where they purchase them have been changing rapidly in recent years. In the 30 years between 1975 and 2005, the contribution of fats in total energy consumption increased from 15% to 21% in rural areas of South Africa and from 21% to 30% in urban areas. 7 In 2013, to reflect these changing consumption patterns, the composition of food items in the “basket” of goods and services used to calculate the official Consumer Price Index changed. Staple foods such as samp (coarse maize meal) and dried and frozen vegetables were removed and more processed food products, including feta cheese plus a range of beverages including mageu (fermented maize beverage), drinking chocolate, filter coffee, and mineral water were added, reflecting the rapid expansion of the black middle class in South Africa. 51
A substantial proportion of urban residents now routinely purchase snacks and meals in the form of both street foods (snacks and cooked foods sold at temporary stands/stalls, also referred to as tuck shops) and fast foods (cooked foods sold at formal and semiformal outlets). Between 2005 and 2010, sales volumes of ice cream, confectionery, sweet and savory snacks, and snack bars increased by 14.7%, 16.3%, 27.5%, and 42.6%, respectively, 48 far in excess of the 6.7% increase in population over the period. 52 Soft drink consumption has also increased. The number of Coca-Cola beverage products consumed per capita increased from 175 to 254 between 1997 and 2010. 48
Fast-food consumption has also grown rapidly. A survey in Johannesburg revealed that some 27.6% of adults aged 19 to 30 years consumed fast foods 2 to 3 times weekly. 53 The most popular food products included burgers (69.5%), pizza (56.6%), and fried chicken (38.4%), and soft drinks were the most popular beverage (56%). Similarly, a survey of 17 year olds from Soweto revealed that 50% of males and 38% of females consume 8 or more street food and fast-food meals weekly. 54 The most popular meal was a “quarter” or “kota.” This comprises one-quarter of a loaf of white bread, chips (French fries), a slice of cheese, reconstituted ham-type cooked meat, plus sauces. On average, the “quarter” provided 5970 kJ, that is, some 57% of an adolescent’s energy requirements.
Evidence of diet change also emerges from rural communities in South Africa. A survey in a rural community near Pretoria revealed that bread is supplanting traditional cereal (maize or sorghum) soft porridge as a breakfast food. 55 Vegetable and starch-based (Irish potato) salads prepared with mayonnaise have become popular foods as a result of Western food influences. Frying has become a preferred method to cook meat and certain vegetables on account of convenience and the introduction of electricity.
The clear trend toward consumption of more energy-dense foods in South Africa stems, in part, from their low cost and greater affordability by poor people. A comprehensive survey comparing food product prices with their energy content in different neighborhoods of Cape Town found that a healthier diet primarily comprising similar food products of lower energy and high nutrient density (eg, brown rice vs white rice and boiled vegetables vs fried vegetables) consistently cost 9% to 12% more than that of the current diet of low-income group people. 56 These researchers also found that in rural South Africa, the healthier diet would be far more expensive (on average 69% more) than the current diet. They concluded that the cost of such a diet would be unaffordable for most people as it would represent over 30% of their total household budget.
To study the impact of urbanization on food intake, Vorster et al 7,57 have examined data over a 30-year period, from 1975 to 2005, to assess changes in diet and in physical health among adults living in different environments in North West province: deep rural, on commercial farms, in squatter camps, in township, and in urban areas. Consistently, urban women obtain a lower proportion of energy from carbohydrate (starch) and a considerably higher proportion from fat and protein. Among urban women, the proportion of energy from fat increased from 21% to 30% and the proportion from carbohydrate decreased from 65% to 57% during the 30-year period. Similar but less dramatic trends emerged among rural women. 7 The urban group also consumed considerably more protein (particularly animal protein), vitamins, and minerals than the remote rural groups. Further, the percentages of women who were overweight or obese in the groups ranged from 48% in deep rural areas to 61% in townships and urban areas, demonstrating a clear increase with urbanization. 57 Over time, markers for cardiovascular disease, serum total cholesterol, low-density lipoprotein, and plasma fibrinogen all increased significantly across both groups.
Together, changing diets and changing activity levels associated with urbanization have led to startling increases in overweight and obese populations. In 2012, 23% of South African adults (males plus females) were overweight (25 > body mass index [BMI] > 30) and a further 25% were obese (BMI > 30). This represents an increase over the prior decade, particularly among adult women, who saw obesity rates increase from 27% in 2003 to 39% in 2012. One-fourth of adults had high systolic blood pressure, whereas 10% exhibited high systolic and diastolic pressure. 16
Recognition of emerging overnutrition problems
The increases in overweight, obesity, and NCDs have become a source of official concern in South Africa. 16,44 This has led to the formulation of a National Strategic Plan for the Prevention and Control of Non-Communicable Diseases (2013-2017). 58
In searching out causal factors, some have criticized the growing concentration of food supply, food manufacture, and food retailing in South Africa into large commercial entities. An academic paper widely reported in the general media implicates “big food” as a contributor to South Africa’s unhealthy eating patterns. 48 Steyn et al express similar concern about the high consumption of soft drinks in South Africa and its association with obesity and NCDs. 50 However, Igumbor and Sanders 48 also note that staple and packaged foods, in particular “healthy foods” sold in supermarkets, are cheaper and more affordable than in traditional outlets on account of their short supply chains and high volumes. 48 They called upon the South African government to act urgently to mitigate adverse health effects of the food environment in South Africa through public education about health risks of unhealthy diet, support for healthy foods, and regulation of big food to make healthy food more available and attractive and conversely unhealthy foods less available and appealing. Similarly, Stupar et al, 59 on the basis of focus group discussions with adolescent girls in Cape Town, recommended a comprehensive school tuckshop policy to ensure that these shops sell healthier food and that healthy school lunches, especially homemade lunches, be promoted. Recognizing the high cost and consequent unaffordability of a healthy diet for many population groups in South Africa, Temple and Steyn 60 emphasize the importance of not only educating people about the importance of a healthy diet but also explaining how to make it affordable. They advocate a strategy of government intervention to manipulate prices through taxation and subsidies.
Responses
The South African government has actively addressed malnutrition issues for many years through fiscal legislation. More recently, they have focused specifically on the undesirable consequences of the nutrition transition. Since the 1980s, government policy has exempted 19 basic foodstuffs from the otherwise almost universal 14% value-added tax (VAT) levied on goods and services. The list comprises nutritious staple foods and includes canned pilchards, eggs, dry, fresh and fermented milk, cereal staples (maize meals, brown bread, and rice), legumes and pulses, fresh fruits and vegetables, and vegetable oil. 61 However, the impact of these tax exemptions on consumer food purchases is not known.
In 2003, the South African Department of Health mandated fortification of all maize meal and wheat flour products with 8 micronutrients. 62 This requirement emerged in response to data revealing that one-third of South African children were vitamin A deficient and 20% were anemic. The required micronutrients include provitamin A, thiamin, riboflavin, niacin, folic acid, pyridoxine, iron, and zinc. 63 Unfortunately, the impact of fortifying these major food staples on the micronutrient status of South Africans is not known and still remains to be assessed. 64
Recently, the government began regulating the salt content of foods in response to clear links between salt intake and high blood pressure, coupled with evidence indicating that hypertension accounts for some 9% of all deaths of people aged 30 and older in South Africa. 65 In 2013, the South African Department of Health introduced regulations mandating progressive reduction in the levels of sodium in a range of food products. 66 The legislated products include bread, breakfast cereals, savory snacks, processed meats, and dry product such as gravy and sauce powders.
An innovative private sector initiative is the Vitality Programme of Discovery Health, South Africa’s largest medical insurance scheme. 67 Scheme members who opt into the Vitality Programme can purchase discounts on certain “healthy” food products, the level of discount being related to the level of participation in wellness programs such as health risk assessments, stopping smoking, weight reduction programs, and even membership of gyms. Data from the program indicate that participating members eat more healthily and importantly are highly significantly less obese (P < .001). It must, however, be pointed out that due to income inequality, some 80% of South Africans have no health-care insurance and hence cannot be beneficiaries of such a program.
Justifiably, there has been criticism by South African nutrition researchers that the country’s school nutrition education curriculum has not received the emphasis it requires. 68 Nutrition education in secondary schools appears as only one of many subjects in a Life Orientation syllabus. As a consequence, the authors found that the nutrition knowledge of school nutrition educators and the study materials available to them were inadequate. Based on the positive outcome of a pilot nutrition education program (NEP) for educators, the study concluded that the school nutrition education can be improved by such NEPs.
Academics in South Africa are widely engaged in addressing the country’s nutrition-related problems, for example, through participation in government advisory boards such as the Department of Health’s Food Legislation Advisory Group and health advocacy groups and through action-oriented training programs. 7,12,48 The University of Pretoria, for example, launched an Institute for Food, Nutrition and Well-being in 2012 to link training and research across multiple disciplines. A broader South African response to the challenge of food insecurity has emerged through the Centre of Excellence in Food Security launched in 2014. The center is an initiative of the South African National Research Foundation and has received long-term funding from the government’s Department of Science and Technology. 69
Middle-Tier Agrifood System: Ghana
Food system
Macro-level successes of the structural adjustment programs of the 1980s and poverty reduction programs of the late 1990s have had a combined positive effect on Ghana’s economic, social, and political life. 70 Ghana has transformed itself into an attractive country for foreign investment in West Africa. Many multinational businesses and organizations have either established or expanded their presence in Ghana. 70 The recent discovery of oil in Ghana has also produced an influx of international oil and gas companies and their employees into the country. The net effect has been the creation of wealthy, cosmopolitan consumers and a general expansion of the Ghanaian middle class. Rapid urbanization has also occurred in tandem with this socioeconomic transformation. 70 If current trends continue, it is estimated that the rate of urbanization will reach 65% by 2030. 71
The food industry in Ghana is not as developed as in other African countries such as Kenya and South Africa. Local food processing for domestic consumption tends to be dominated by informal sector activities that account for the bulk of informal employment and manufacturing in Ghana. These activities include cassava processing into flour, dried cassava, and starch; fish processing, including smoking; groundnut oil extraction; and milling or grinding millet, sorghum, and maize for own use. 72 Although there are private local food processing companies, Ghana still remains fertile ground for investment in food processing in the formal sector.
There is a growing segment of middle-income households (about 5% of the population), and this could provide a significant consumer base for locally processed foods. However, current levels of local food processing are not enough to meet local demand, and as a result, there is significant importation of high-value food products. 73 Although the government has introduced tax incentives to promote food processing, problems such as lack of space, infrastructure and finance appear to stifle growth. In this regard, the entry into the Ghanaian market of a South African food retailer in 2003 started to bring significant spin-off effects for the agriculture and agribusiness sector as international supermarket supply chains expand. 73
Nutrition transition
This socioeconomic transformation and rapid urbanization has inevitably had an effect on food and dietary choices. Accra, the capital city, has a large number of restaurants that offer a wide variety of regional and international cuisine. International franchise Western-style fast-food restaurants are also being established. These restaurants tend to be located in wealthy neighborhoods, shopping malls, and petrol filling stations and are normally patronized by wealthier, more upmarket clients. 70 There are also a large number of cheaper kiosk versions of fast-food or local restaurants popularly referred to as “chop bars” that serve traditional Ghanaian meals. These tend to be located in open markets, truck stations, or along the busy roads and are normally patronized by the less wealthy. 70 A general feature of the modern fast foods and the meals served at the local chop bars is that they are usually foods that are energy dense with high levels of sugar, salt, and fats and usually consumed with sugar-sweetened carbonated soft drinks. Indications are that significant portions of individuals’ budgets are being spent on fast foods from these restaurants. Food consumption patterns in the big cities of Ghana, notably Accra have changed from traditional diets comprising coarse grains to imported energy-dense diets. 74
The effects of the nutrition transition in Ghana are evident in the burden of chronic NCDs in the country. There has been a shift in the major causes of death in Ghana from predominantly communicable diseases to a combination of communicable and chronic NCDs. Diseases such as hypertension, stroke, diabetes, and cancers have grown in importance to become top 10 causes of death. 75 Across the country, there is clear evidence of increased prevalence of chronic diseases such as hypertension and diabetes and increased mortality from these conditions. 70 Estimates from the WHO indicate that NCDs account for about 34% of deaths and 31% of disease burden in Ghana. 76
Obesity levels in Ghana increased 2.5-fold between 1993 and 2003, with the highest prevalence observed in the greater Accra region. 77 Child obesity is an emerging problem in Accra, where small sample studies suggest that the prevalence of childhood obesity increases with socioeconomic status and is more common in females than in males. 78 Likewise, in urban areas of Northern Ghana, the prevalence rate for overweight and obesity among school-age children has reached 17.4%. 79 Significantly, comparisons across West Africa indicate that the most rapid increase in overweight and obesity has occurred in Ghana. 80
Amoah et al 81 refer to very early research conducted on prevalence of diabetes in Accra, which reported the prevalence of 0.4% among 4000 individuals in one study in 1958 and of 0.2% among 5000 individuals in another study in 1964. The authors pointed out that these figures created the impression among policy makers that diabetes was rare among Ghanaians. As a result, the health-care policy in Ghana placed little emphasis on diabetes control and prevention. Subsequent studies have reported diabetes prevalence of 6% among Ghanaian women in Accra 82 and 9% among individuals studied in Kumasi. 83
Information from the Ghanaian Ministry of Health indicates that outpatient cases of hypertension in public and mission facilities, excluding teaching hospitals, increased from about 60 000 cases in 1990 to about 700 000 cases in 2010. 76 For more than 15 years, hypertension has featured in the top 5 outpatient diseases and accounts for 3% to 5% of all new outpatient diseases across all ages. It ranks as the third most common newly diagnosed outpatient disease among adults. In 2008, cardiovascular diseases became the leading cause of reported institutional deaths accounting for 14.5% of institutional deaths compared to malaria, which accounted for 13.4% of the deaths. 84
Recognition of emerging overnutrition problems
A growing literature attests to the increasing awareness about problems of overweight and NCDs in Ghana. Both Ghanaian and international researchers have published widely on the nutrition transition and the burden of NCDs in Ghana. 70,75,78,80 –82,85 –87
Policy makers have taken notice. The Ghana National Health Policy acknowledges that lifestyle changes associated with consumption of high sugar, salt, and fat diets, lack of physical exercise, lack of rest and recreation, and other factors are changing the epidemiology of morbidity and mortality in Ghana. 88 Ghana’s national health policy now emphasizes the need to undertake programs for reducing risk factors associated with NCDs such as lack of exercise and poor eating habits. 76
Responses
The Ghanaian Ministry of Health has instituted several initiatives in response to the growing burden of NCDs. The National Health Policy 76 identifies 7 priority areas of action, the first of which is to promote healthy lifestyles and healthy environments. Several programs are proposed as a means of addressing these areas of action, and these include promoting good nutrition across the life span and reducing risk factors associated with NCDs such as lack of exercise and poor eating habits. These programs emphasize the importance of empowering individuals, households, and communities to make informed choices for their health through provision of information and education. They promote branding and marketing of healthy living choices by providing population groups such as mothers, children, adolescents, and adults with relevant messages on healthy eating, exercise, rest, and recreation.
In 2005, the Ministry of Health adopted a Regenerative Health and Nutrition Programme, which was piloted in 2006. 86 This initiative formed part of the effort of the government to reduce the incidence of preventable diseases and to promote regenerative health in the country. The main objective of the program was to promote healthy lifestyles, dietary practices, and mother and child care practices that would help eliminate diseases that impact on the health and well-being of Ghanaians. Tagoe and Dake 86 conducted a study to examine the lifestyle behavior among Ghanaian adults after introduction of the program. Their results showed that relatively fewer people adhered to consuming the recommended amount of fruit and vegetable servings per day in 2008 compared to 2003. Overall, more females (7%) exhibited healthier lifestyles and more males (9%) exhibited risky lifestyle behaviors after introduction of the policy.
In August 2012, the Ministry of Health issued a National Policy for the Prevention and Control of Chronic Non-communicable Diseases in Ghana. 76 The policy focuses on 4 major NCDs that make the largest overall contribution to NCD mortality, namely, cardiovascular disease, diabetes, cancer, and chronic respiratory disease. These share common risk factors including tobacco use, alcohol, unhealthy diet, and physical inactivity. Five main strategic areas are identified under which interventions will be initiated. These include primary prevention, early detection and clinical care, strengthening of the health system, research and development and surveillance of NCDs, and their risk factors.
Although still in its early stages, some of the proposed interventions directly relate to addressing the adverse effects of the nutrition transition. The policy proposes to promote health by encouraging intake of fruits and vegetables; high-fiber diet, moderate physical activity; reducing intake of energy-dense foods, salt, trans-fatty acids, and sugar; avoiding tobacco; reducing excessive alcohol intake; and undergoing periodic medical checkups. It proposes that marketing of “diet” soft drinks will not be encouraged due to their doubtful value and potential harmful effects. The policy also proposes the use of the Regenerative Health and Nutrition approach in a bid to reinforce actions that improve healthy eating, physical activity, relaxation, and hygiene. Furthermore, wellness programs in clinics, communities, schools, and workplaces including trade-learning centers will be established and supported. National awareness months for cancers, diabetes, and hypertension will be instituted and know your blood pressure, blood sugar, and blood cholesterol level campaigns will be promoted. In sum, Ghana recognizes its growing overnutrition problem and has instituted a framework for action, which is now in its formative stages.
Early Food System Transition: Uganda
Food system
Uganda’s food production and distribution system remains primarily rural, small scale, and informal. The country’s broad basket of staple foods include matoke (cooking banana), cassava, maize, sweet potatoes, and beans, most of which involve only simple hand processing by rural women or, in the case of maize, mechanical hammer mills. Given a mere 16% urban population share, Uganda remains one of the Africa’s most rural countries. As a result, unprocessed and home-grown food accounts for over 50% of the value of foods consumed, whereas informal processing by hammer mills and by artisanal methods accounts for 25%. Only 19% of food consumed are modern-type processed food products (including bread, packaged foods, pasta, processed canned foods, and dairy products) often sold through supermarkets. 1
Despite its small urban population, the capital city of Kampala and its emerging middle class are growing rapidly enough that they have attracted a string of regional supermarket chains from Kenya and South Africa. 89 In addition, many smaller local supermarkets have sprung up, particularly in Kampala. Free trade agreements through the East African Community facilitate the emergence of regional supply chains that feed into the supermarket chains. In urban areas, supermarkets distribute primarily processed foods, which account for 64% of sales, whereas basic staples (maize and rice) account for 30% and fresh fruits and vegetables only 6%. 89 As elsewhere, traditional wholesale markets and outdoor retail markets dominate fruit and vegetable retailing. 90,91 As in much of Eastern Africa, galloping urbanization has overwhelmed the urban market infrastructure in many horticulture wholesale markets, where a combination of heavy traffic congestion, poor sanitation, and rudimentary infrastructure results in high losses (in the range of 40%-50%), increased price risk for traders, and unnecessarily high prices for consumers. 92,93
Fast-food chain retailing has likewise established a foothold in urban Uganda, with international fast-food retailers operating alongside local food outlets. 94 These chains, however, probably only account for a tiny proportion of snacks and meals that are now being purchased outside the home. A survey in Kampala revealed that 90% of respondents consumed fast foods, with most commonly consumed items including potato chips (French fries), deep fried chicken, sausages, deep fried meat, and “chaps” (miscellaneous meat dish). 94
Nutrition transition
Rates of overweight (17% among adult women) and obesity (4%) in Uganda currently lie far below those prevailing in South African and Ghana (Table 4). Yet rates appear to be rising on the heels of advancing urbanization, rising incomes, and changing lifestyles. Data from the 2011 Uganda Demographic and Health Survey (UDHS) indicate that the proportion of overweight adult women in urban areas (32%) significantly exceeded average levels observed in rural areas (13%). 95 In some rural areas, changing lifestyles and emulation of urban behavior and risk factors are resulting in high BMI, reduced levels of physical activity, and low fruit and vegetable consumption. People living in villages with the highest urbanicity rating attained the highest BMI levels and were nearly 50% more likely to be physically inactive and 20% more likely to consume low levels of fruits and vegetables compared to more remote rural areas. 96
Among adults (35-60 years) in rural Uganda, abnormal glucose regulation (a risk factor for diabetes) is highly significantly associated with obesity (BMI of ≥30) and significantly negatively associated with high dietary diversity. 97 Moreover, hypertension among this cohort is significantly associated with a high BMI (≥25) and negatively associated with moderate dietary diversity. 98
Obesity in young adults (18-30 years) in Uganda is significantly correlated with urban residence, alcohol consumption, smoking, failure to engage in sports, and commuting to school in a taxi or private vehicle. 99 Among adolescents (13-15 years), the prevalence of overweight or obesity is much higher in girls (10.4%) than boys (3.2%) in Ghana and Uganda. 100
Recognition of emerging overnutrition problems
Though at an early stage, emerging evidence of overnutrition and associated NCDs has begun to attract attention in Uganda. In a commentary on the findings of research into the distribution of cardiovascular disease risk factors among people in rural Uganda by Maher et al, 101 it was suggested that the next epidemic in Uganda (following HIV/AIDS) may be NCDs. 102 Moreover, rates of hypertension remain high (Table 4), and these prove to be the most common risk factor for cardiovascular disease. 101
Responses
The cornerstone of Ugandan Government nutrition and health policy is the Uganda Nutrition Action Plan 2011 to 2016. 103 The action plan focuses on reducing malnutrition (undernutrition) among women of childbearing age, infants, and young children with the aim of ensuring that all Ugandans are properly nourished. Given the slow pace of the nutrition transition in Uganda, the plan mentions obesity only once. “Uganda is faced with a double burden of malnutrition—the increasing coexistence of obesity and malnutrition in communities across the country.” The 2006 UDHS showed high levels of overweight among women living in urban centers, as well as in many rural areas of Western and Central regions. 103 Noncommunicable disease consequences of obesity such as diabetes and cardiovascular disease are not mentioned. Although recognizing an emerging overweight problem among women, the Government of Uganda focuses its full attention on the far greater current problem of undernutrition.
Governmental nutrition interventions, although aimed at undernutrition, may in some cases promote actions beneficial to alleviating incipient overnutrition and NCDs. Breastfeeding and prenatal care for pregnant women, for example, remain centerpieces of government efforts to combat malnutrition. Given long-term benefits for children and mothers, these efforts to reduce undernutrition in the short run may generate long-term health benefits in the form of reduced propensity for overweight in later life. Likewise, health and nutrition education aim to increase overall nutritional awareness about healthy foods.
In 2002, the Ugandan government established a national working group on food fortification, and in 2011, it passed legislation on fortification of 3 staple foods: maize meal, wheat flour, and vegetable oil. 104 By 2012, some 10 food companies were fortifying these products, with 95% of vegetable oil being fortified with provitamin A and 40% of wheat flour being fortified with iron. The plan is to fortify maize meal with a similarly wide range of micronutrients—provitamin A, B group vitamins, iron, and zinc. 105 All mills with a production capacity of at least 20 tons per day must fortify.
Outside of government, several joint university and private sector initiatives have focused on food processing and supply-side interventions that aim to help moderate food system trajectories and improve nutritional outcomes. Makerere University’s Agshare program supports student and faculty research on food production and processing problems in small-scale local processors through participatory research and student involvement at community level. Agribusiness incubators at Makerere and Kyambogo Universities link food processing research on indigenous foods and animal products with agribusiness entrepreneurs to develop marketable new products of good quality and shelf-life using local food products and linking them to modern distribution systems. 106 Joint efforts between Makerere University and the Uganda government, supported by special presidential initiatives, aim to develop alternative educational and community transformation models that promote industrial value chain development for better health, wealth, and livelihoods. 107 Makerere has also helped to found and operate a regional RISE-African Natural Product Research Network, which aims to apply modern research to make local food and plant products commercially available to a broad market. 108 These initiatives share a common interest in increasing utilization of high-value, healthy foods by focusing food processing research and entrepreneurship support to help small food processors emerge.
Prospects for Bending the Curve in Sub-Saharan Africa’s Nutrition Transition
Good News and Bad News
Optimists note that sub-Saharan Africa enjoys a latecomer advantage that opens the possibility of learning from experiences elsewhere. Pessimists, however, identify corresponding disadvantages in Africa’s latecomer status. Accelerating penetration of Western-style processed foods, sugar-sweetened beverages, infant milk formulae, and food advertising accompany the increasing globalization of agribusiness supply chains. 2,90,48,109 Increasingly, sophisticated food processing, marketing, and distribution systems confront poorly funded public health systems, making Africa arguably more vulnerable to pernicious public health outcomes than other regions. Africa, with generally weak public health systems and dental hygiene services, risks following the Latin American model in which overweight populations with decayed teeth become increasingly common.
If the optimists prove right, then Africans can study, learn, and apply preventative early actions based on lessons learned elsewhere. If the pessimists are right—that Africans face conditions far more difficult than elsewhere—then learning from others becomes all the more imperative. In either case, early actions likely offer the best hope for bending the curve in Africa’s nutrition transition.
Emerging Early Actions in Sub-Saharan Africa
Public health responses to emerging overweight populations and related NCDs have proven limited to date in sub-Saharan Africa. Instead, most public health services continue to focus their limited resources on reducing undernutrition and communicable diseases such as malaria and HIV/AIDS. Only in South Africa, where obesity levels rival those in the developed world, have policy makers moved aggressively to combat overnutrition.
In contrast, supply-side food system pressures appear to emerge earlier and elicit responses sooner than the classic public health reactions to emerging consumer problems of overnutrition. The preceding review of responses by countries at differing levels of food system transformation suggests that pressures on the supply side of the agrifood system, in obviously overstretched urban wholesale markets and on agricultural education and training institutions from dissatisfied agribusiness employers, emerge sooner than widespread overweight and public health concerns. As a result, even countries at very early stages in the nutrition transition have already begun to recognize and respond to supply-side pressures on the agrifood system through job training in food processing, storage, logistics, and distribution; market infrastructure and management reforms; food industry entrepreneurship programs; and product development efforts focusing on healthy and often neglected indigenous foods. 1,12,93,108,110 This suggests that the sort of systemic supply-side reforms in food systems advocated by Goméz and Ricketts 91 (such as introducing nutritional considerations from plant breeding through to policy incentives governing agribusinesses behavior) may prove feasible at an earlier date than the classic public health responses to overnutrition.
The Standard Public Health Agenda
Globally, public health responses to overnutrition have emerged late in the nutrition transition, well after overweight and related public health problems attain widespread visibility. Responses typically revolve around motivating and enabling behavioral change through healthier diets and increased physical activity. 2 Experiences from elsewhere offer a menu of options for sub-Saharan Africa, though surprisingly little firm evidence on impact.
Given the complexities of urban and rural lifestyles, efforts to change behavior confront complex systemic problems that require multiple actions across many fronts. For this reason, many specialists advocate a broad agenda of integrated nutrition and public health interventions. 7,27,111 Mexico and Brazil, 2 middle-income countries experiencing rapid increases in overweight population, have launched comprehensive, multisectoral efforts to combat the steady rise in overweight and NCDs. 112 –114 Brazil’s program indicates the breadth of these multisectoral efforts, with activities including (1) incorporation of obesity in health, nutrition, food, and nutritional security policies, (2) mobilizing different governmental departments to conduct food and nutrition education, (3) building an integrated interdepartmental governmental response to prevent and control obesity, (4) promoting and providing healthy foods in schools, (5) directing healthy diet promotion and obesity prevention actions to occur in the primary health-care sector, (6) promoting physical activity in the community, (7) regulating the food industry advertising and marketing practices to young children, and (8) social action and community empowerment through mass communication and capacity development of local nongovernment organizations. 114 Although the impact of these actions is still not clearly documented, sub-Saharan African countries can learn from these experience about the range of potential interventions as well as the inherent challenges in steering multisector and multistakeholder actions to combat the double burden of malnutrition.
Evaluating the impact of specific interventions becomes similarly complex, given the many interlinked individual and environmental factors that shape dietary choices, time allocation, physical activity levels, and nutritional outcomes. As a result, careful studies examining the impact of alternative health and nutrition interventions on diet and obesity remain surprisingly limited. 25 Efforts to motivate and enable behavioral change can be grouped into 4 main categories: education, food industry regulation, price incentives, and maternal–child health interventions.
Nutrition and public health education
Nutrition education programs have formed a major focus of global efforts to combat the health problems associated with growing overweight populations. Many efforts center on schools, including a mix of classroom nutrition education, school gardens, school feeding programs, and restrictions on vending machines and snack foods. Since 2001, Brazil’s nationally funded school lunch program has mandated that 70% of program funds be spent on fresh vegetables, fruits, and minimally processed foods. 113 Related educational efforts involve community outreach of nutrition guidelines through health workers, clinics, social media, and civil society groups. Over the long run, these efforts aim to build educated consumers and more effective consumer lobbying groups.
Food industry regulation
Because newly educated consumers, managers, and policy makers require reliable information to make informed choices, a growing number of countries mandate front-of-the-package food labeling of calorie and nutrient counts to help inform consumers and support nutrition education efforts, often following guidelines promoted by Choices International. Middle-income countries such as Chile and Brazil have likewise introduced controls on advertising of unhealthy food marketed to children, whereas Mexico has established a task force to investigate best practices in protecting children from unhealthy foods. 25,112,114
Some regulations directly limit nutrient levels or unhealthy foods. Salt regulations, such as those introduced in South Africa, aim to protect consumers from unhealthy levels of sodium intake in many processed foods. For similar reasons, over 20 countries prohibit vending machines in schools. 25
Regulatory efforts often generate pushback from the food industry. Following food industry challenges, for example, Brazilian authorities suspended their 2006 proposal to regulate advertising of foods high in sugar, sodium, saturated fat, and trans fats. 114 Mexico’s gradual efforts to introduce food and beverage guidelines for school, over the period from 2011 to 2014, met with similar resistance. The original guidelines called for banning carbonated soft drinks in schools and placing limits on other sweetened beverages, whole milk, added sugar, salt saturated fat, as well as an energy-density criterion to limit high-energy snacks and portion sizes. 112 Although nearly two-thirds (63%) of public comments received before the official review commission favored implementation of the guidelines, 99% of food industry comments opposed the regulations, whereas 86% from civil society and academia supported them. Ensuing negotiations led to relaxation of the energy-density criterion. Although the carbonated soft drink ban survived beverage industry objections, other sweetened beverages were allowed. Given frequent industry pushback, triggered by conflicting pressures between industry profit and public health objectives, many researchers argue that industry self-regulation will not prove sufficient and that public regulation of food industries will be necessary to ensure consumer health. 111
Price incentives
Poor households in developing countries frequently spend over 50% of their income on food. As a result, changes in relative food prices can shape consumption decisions significantly, particularly among low-income groups. Emerging “fat taxes” and “soft drink taxes” on sugar-sweetened carbonated drinks aim to exploit this resulting price sensitivity to discourage consumption of unhealthy foods. In January 2014, Mexico introduced a tax of 1 peso per liter (approximately 10%) on sugar-sweetened beverages, estimating that this would decrease soft drink consumption by roughly 10%. 112 At the same time, they introduced an 8% tax on nonessential, unhealthy foods, defined as those deemed to contain excessive quantities of saturated fat, sugar, or sodium. South Africa’s VAT exemption for 19 “basic foods” works in the opposite direction, providing an implicit price subsidy of 14% by exempting basic healthy foods.
How much these tax-induced price incentives will affect consumption of targeted foods remains the subject of a small but growing volume of empirical research. A review of 32 consumption studies suggests a small but positive impact. 115
Price incentives may also induce increases in physical activity. South Africa’s private health insurance scheme, the Vitality Programme, outlined above, offers discounts on healthy foods in return for participation in various wellness programs. Although early results do suggest behavioral change, these opportunities remain restricted to an elite membership with access to health insurance, currently a limited constituency in sub-Saharan Africa. Looking forward, however, Africa’s emerging urban middle class represents a growing target group for these sorts of incentive programs, given their high vulnerability to overweight problems and their increasing means and access to formal insurance services.
Maternal–child health
Growing evidence suggests an intergenerational link between the health status of mothers and the risk of obesity and NCDs in their children. 23,25,26 Given these potential long-term linkages between the nutritional status of pregnant women, infant feeding practices, and susceptibility to overnutrition in their offspring, interventions in utero and in early childhood may offer considerable leverage for decelerating obesity and NCD risks in future generations. 25,116 Initiatives such as the Scaling Up Nutrition movement and maternal and child health programs may offer the most feasible path for early public health interventions aimed at bending the curve in sub-Saharan Africa’s nutrition transition. 117
Expanded Options for Bending the Curve
The budgets and political will required to underwrite major public health responses to looming problems of overnutrition have yet to emerge in sub-Saharan Africa, with the exception of South Africa. In most of sub-Saharan Africa, underfunded public health systems face difficulties responding to pressing current needs of undernutrition and contagious diseases.
In contrast, action on the supply side of the food system has begun and these efforts offer additional possibilities for intervention and for associated research monitoring inputs and outcomes. Work by Minnaar et al 12 inventorying needs in postfarm food technology and training, by Gustavsson et al 93 on food losses and potential marketing system reforms, and by Gómez and Ricketts 91 on the potential nutritional impact of alternative supply chain structures can help in the development of a feasible, forward-looking, nutritionally aware agenda for agrifood system reform. These suggest several promising areas for nutritionally responsive systemic interventions in food supply systems.
Train a new generation of food industry professionals bridging food technology, public health, and human nutrition
The most rapid employment growth in African agrifood systems over the coming 3 decades will occur in postfarm segments of the food system. 1 These changes offer a window of opportunity for agricultural training institutions as they gear up to equip students with the technical skills required by private food industries and public health services. In order to seize this opportunity, both Amuna and Zotor 18 and Minnaar et al 12 advocate broadening of professional curricula to integrate training in food sciences with public health and human nutrition.
Facilitate development of healthy, low-cost foods
Low-income consumers face the basic reality that processed and prepared convenience foods provide appealing taste and low-cost calories. 48 Hence, education efforts promoting healthier food choices often run headlong into the realities of urban poverty and highly constrained consumer budgets. In response, a variety of promotional efforts have emerged to increase the availability and lower the costs of healthier food choices. Two, in particular, merit mention.
Indigenous food entrepreneurship and product development
Africa’s growing demand for processed convenience foods offers potential new markets for packaged indigenous foods, which cater to local tastes but which most Western food industries fail to deliver. Food industry professionals can contribute to the research and product development necessary to generate a range of tasty, inexpensive nutrient-dense food products by building on taste preferences for local foods, green leafy vegetables, and local whole grains favored by local palates but often unavailable in congested, growing cities. Research on basic fermentations and preservation processes is required to bring new products to market. 118 University-linked agribusiness incubators across a range of African settings—including Ghana and Uganda—are beginning to provide the food research and agribusiness start-up support required. 119 –121 Related emerging experience from Brazil’s legally mandated locally supplied school feeding program may offer further insights for these ongoing Africa-based efforts. 113,114
Wholesale horticulture market reforms
Many overwhelmed urban horticultural wholesale markets suffer from poor sanitation, traffic congestion, rudimentary infrastructure, and consequently excessively high produce losses. 93,122 Roughly 80% of these losses (38% of 48%) occur in the postfarm segment of the supply chain, in assembly, wholesale, and retail markets. 93 As a result, investments in urban horticulture market infrastructure and management systems and improved urban planning can significantly reduce losses, increase efficiency, and improve public health. 92,93 Improvements in horticulture market infrastructure and management offer prospects for raising farm incomes, lowering urban consumer prices for fresh fruits and vegetables, and increasing urban consumption of nutrient-dense horticultural commodities.
Conclusions
Without significant early actions, sub-Saharan Africa seems likely to follow the default trajectory of accelerating growth in overweight populations accompanied by increasing noncommunicable and oral diseases. Despite this looming threat, most countries in sub-Saharan Africa understandably continue to prioritize public health actions that confront the serious present threats posed by undernutrition and communicable diseases. Only in South Africa, well after the emergence of large-scale overweight problems, are public health officials moving strongly to combat problems of overnutrition.
Within the standard public health and nutrition policy tool kit, 2 categories of intervention appear most feasible for moderating nutritional trajectories in the face of continued budget constraints and continuing undernutrition problems. First, maternal and child health programs offer prospects for serving double duty—simultaneously addressing short-term undernutrition problems while at the same time helping to reduce future tendencies toward overweight. Second, regulatory and fiscal actions that limit access to unhealthy foods, tax unhealthy foods, or subsidize healthy foods offer the twin advantages of low implementation cost and likely improvement in nutritional outcomes.
Supply-side pressures emerge earlier in food system transitions than consumer public health problems. As a result, efforts to moderate nutritional trajectories need to consider opportunities on the supply side of the food system—in areas such as job skills training, marketing reforms, and food industry entrepreneurship. Early actions on the supply side of the agrifood system offer additional tools for influencing food system trajectories as well as opportunities for associated research monitoring of nutritional and public health outcomes.
Given the surprising paucity of careful evaluations of efforts to bend nutritional curves in developing and middle-income countries, more research will be required to help steer sub-Saharan Africa’s nutrition transition in a more positive direction. Continuing budget constraints amplify the need to determine the cost-effectiveness of alternative actions. For these reasons, a careful research agenda evaluating the impact and cost of emerging early efforts to alter nutritional trajectories will constitute a necessary component of an effective early action agenda for bending the curve in sub-Saharan Africa’s nutrition transition.
Footnotes
Note
Acknowledgments
The authors gratefully recognize financial contributions from the International Fund for Agricultural Development (IFAD) and the USAID’s Food Security Policy Innovation Laboratory which made this work possible.
Authors’ Note
Steven Haggblade conducted the overview of the nutrition transition in Africa as well as the summary of past efforts at bending the curve. Kwaku G. Duodu and Nelson K. O. Ojijo prepared the Ghana review. John D. Kabasa worked primarily on the Uganda section of this article, while Amanda Minnaar and John R. N. Taylor prepared the South Africa review. Steven Haggblade and John R. N. Taylor integrated these materials and, together with Amanda Minnaar, distilled the principal findings.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received financial support for travel costs associated with this work but no direct personal emoluments for the research, authorship, and/or publication of this article.