
Abstract
The aim of this article is to provide an overview of the role of protein quality within the first 1000 days of life. The article outlines the importance of protein quality in pregnancy and early growth and examines the potential of high-quality protein in prevention of stunting and treatment of severe and moderate acute malnutrition. The article also provides a summary of the recent changes in protein quality evaluation and the development of a new index, the Digestibility Corrected Amino Acid Score, examining the opportunities and challenges this new methodology presents in assessing protein quality.
Introduction
The role of maternal nutrition in determining birth outcomes and subsequent growth in early life is well documented. The Lancet series from 2013 has estimated that a maternal intervention package inclusive of maternal micronutrient supplements to all, calcium supplements to mothers at risk of low intake, maternal balanced energy protein supplements as needed, and universal salt iodization can save 49000 to 146000 lives. Implementation of maternal balanced energy protein supplements as needed could prevent about 80000 deaths in children younger than 5 years of age. 1 Furthermore, the newest protein requirements released by the World Health Organization (WHO) estimate that the need for protein in the third trimester is significantly higher than previously estimated with an additional 31 g of high-quality protein (safe intake) required in the third trimester. 2 The aim of this article is to provide an overview of the role of protein quality within the first 1000 days of life. The article outlines the importance of protein quality in pregnancy and early growth and examines the potential of high-quality protein in prevention of stunting and treatment of severe and moderate acute malnutrition. It also provides a summary of the recent changes in protein quality evaluation and the development of a new index, the Digestibility Corrected Amino Acid Score (DIAAS), examining the opportunities and challenges this new methodology presents in assessing protein quality.
Protein and Amino Acid Requirements in Pregnancy and Early Childhood
The new protein requirements released in 2007 are based on a consultation led by the United Nations Food and Agriculture Organization (FAO) and the WHO in 2002. 2 These requirements depart from the previous report (1985 protein and energy requirements) in that they focus solely on protein and amino acid requirements, with energy being published as a separate guidance. Furthermore, significant emphasis is placed on amino acid requirements with recent stable isotope studies allowing more accurate estimates of essential amino acids such as lysine. A key change in requirements is the reduction in the total protein per kg body weight requirement for all age-groups including infants and young children. In adults, there is an increase in requirements (both mg/kg body weight and mg/g protein) for all essential amino acids except the sulfur amino acids. And while in infants and young children, there is also a decrease in amino acids required (absolute amounts and mg/g protein), the reduction in requirements of amino acids is not as high as that of total protein. This essentially means that while the infants’ and young children’s total protein requirement (both mean and safe levels) is lower than previously thought, the amino acid composition of those proteins, that is, protein quality, still remains important, in fact becomes a more important issue (Table 1).
Protein and Amino Acid Requirements in Pregnancy, Lactation, Infancy, and Childhood.
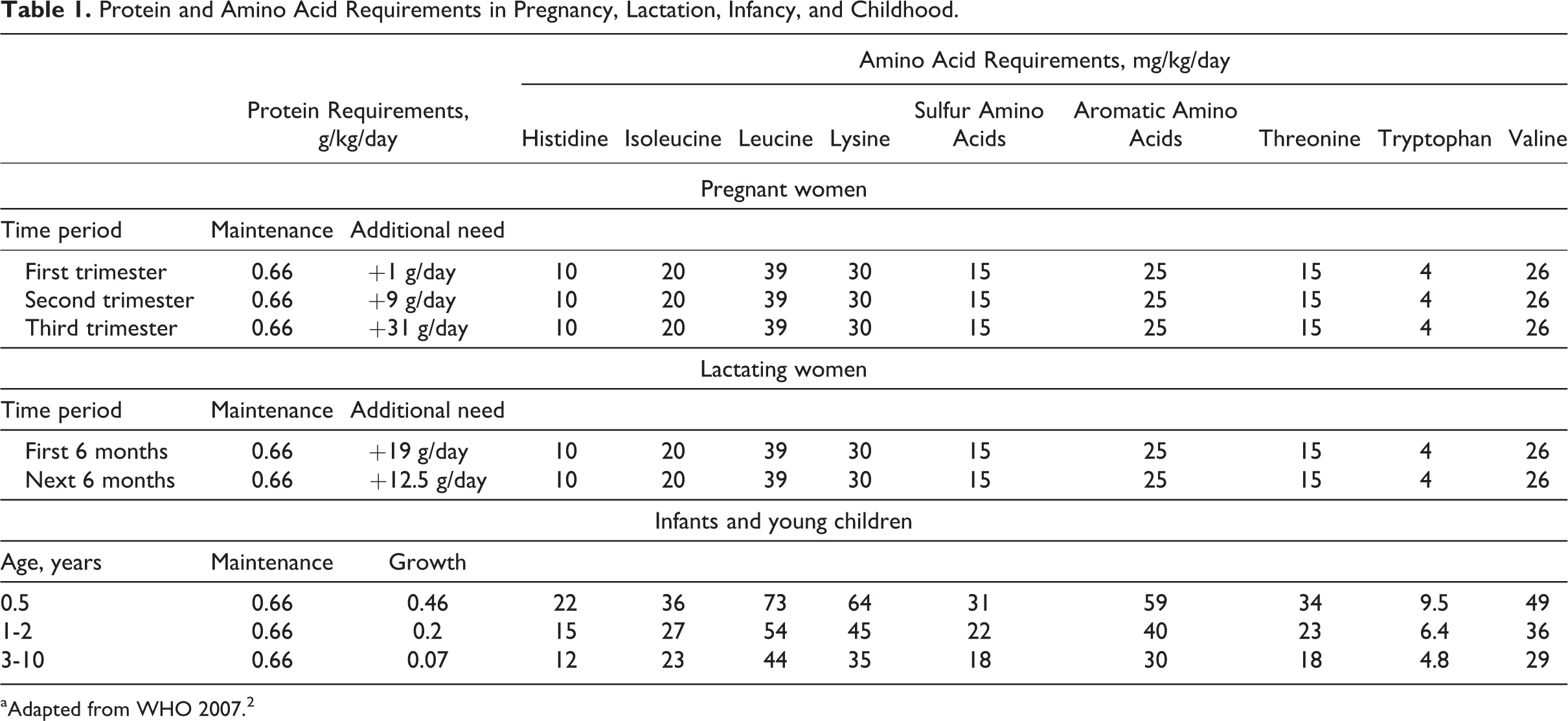
aAdapted from WHO 2007. 2
With respect to pregnancy, in the previous report (1985 protein and energy requirements), a single value was recommended through the entire pregnancy. However more recent body composition studies do not show any maternal storage in early pregnancy, thus the current report recommends increasing amounts for each trimester. 2 The highest need is recommended for in the third trimester (Table 1).
Protein Quality Evaluation
The quality of a protein is based on its ability to meet requirements for the 9 essential amino acids. While several different methods exist for the assessment of the quality of protein in a diet or food, until recently, the accepted method was to use the Protein Digestibility Corrected Amino Acid Score (PDCAAS). This involves the comparison of the amino acid content (accounting for bioavailability expressed as fecal digestibility) of a food with a gold standard (eg, amino acid composition of egg proteins) or human amino acid requirements. 3
The use of amino acid composition data to evaluate protein quality of foods (ie, amino acid scoring systems) has been widely used since the 1950s, with the first procedure utilizing the amino acid composition of egg as a standard. 3 However, since the high levels of essential amino acids in egg protein gave most food proteins a low amino acid score, subsequently, human amino acid requirements were used as a basis for assessing protein quality. Several scoring patterns have been recommended by different consultations starting from 1965 to 1973 to 1985. A FAO/WHO consultation in 1991 agreed on the use of a protein digestibility corrected amino acid score (PDCAAS). To obtain the PDCAAS of a food, the limiting amino acid score is corrected for true fecal protein digestibility. The first step involves estimating the amino acid score of 4 essential amino acids—lysine, tryptophan, threonine, and the sulfur amino acids (methionine + cysteine), which can range from 0 to 1. The score is estimated by dividing the total mg of the essential amino acid per gram of the food protein (or total dietary protein) by the reference value for that amino acid. The amino acid with the lowest score is considered the limiting amino acid. The limiting amino acid score is then adjusted for bioavailability using a fecal digestibility factor.
The importance of protein quality has been documented in an ecological analysis conducted using national food consumption and stunting data from 116 countries. 4 Analysis of the risk of protein inadequacy conducted using total protein versus total utilizable protein corrected for protein quality (using the PDCAAS) showed interesting insights. Using the metric of total protein for estimating risk of protein inadequacy (uncorrected for protein quality) versus the metric of total protein corrected for protein quality led to a significant underestimation of risk, particularly in East and Southern Africa and South and South East Asia. Thus, when utilizable protein, a metric that accounts for protein quality, is used, some populations exhibit higher risk of protein inadequacy. 4
However, the PDCAAS has significant limitations. It does not credit extra nutritional value to high-quality proteins. When comparing food products for protein superiority, it is important to have a protein metric that is not truncated at a value of 1.0. Another limitation of PDCAAS is that it does not account for antinutritional factors. The digestibility measures that were used in PDCAAS are crude measures. Considerable discussion based on existing evidence has led to the conclusion that ileal digestibiity is a more accurate measure of digestiblity.
In 2011, a FAO Expert Consultation held in New Zealand evaluated the use of PDCAAS in assessing protein quality. While the metric has been used for over 20 years and has been of considerable value in practice, there was consensus of its significant limitations. Furthermore, new research has been emerging in this area, which allows for a careful assessment of the adequacy of the measure. 5 Besides the issues highlighted above, PDCAAS does not take into account, the bioavailability of amino acids while overestimating the quality of poorly digestible proteins supplemented with limiting amino acids and of proteins colimiting in more than one amino acid. The recommendations of this Consultation were to replace the PDCAAS with the Digestible Indispensable Amino Acid Score (DIAAS). The DIAAS % = 100 × ([mg of digestible dietary indispensable amino acid in 1 g of the dietary protein]/[mg of the same dietary indispensable amino acid in 1 g of the reference protein]). The ratio is calculated for each indispensable amino acid and the lowest value designated as the DIAAS. A key difference between the DIAAS and the PDCAAS is the use of ileal digestibility, which is based on true ileal digestibility of each amino acid determined preferably in humans or in growing pigs or rats. 5 Furthermore, DIAAS can have values below or above 100%, with values above 100% not being truncated unless the DIAAS is being used for estimating protein and amino acid intakes from mixed diets or sole source foods. The recommended amino acid scoring pattern to be used for DIAAS include the pattern of breast milk for infants (birth to 6 months), the pattern for the 0.5-year-old infant for young children 6 months to 3 years, and the pattern for the 3- to 10-year-old for older children, adolescents, and adults. 5
There will be challenges in implementing the DIAAS, particularly due to a lack of ileal digestibility data. The consultation recommended the convening of a working group to agree upon an experimental protocol to enable the development of a more robust data set of true ileal digestibility and outline the method for assessment of the impact of the use of true ileal digestibility data. The FAO is committed to generating these data themselves or via academic laboratories, so they can then be compiled into food composition tables. Furthermore, while the PDCAAS has been used to evaluate food products and for regulatory purposes, it was not as extensively used for population assessments. As noted in the report, to facilitate the transition from the PDCAAS to DIAAS, the FAO intends to develop guidance documents so that policy makers, academics, and industry can use the DIAAS much more effectively to make protein-related claims or in evaluating mixed diets. 5
Role of Protein Quality in Pregnancy
The consequences of maternal energy and protein restriction are widely documented. 6, 7 Approximately 30 million newborns in developing countries are affected by intrauterine growth retardation (IUGR), with the highest burden of low birth weight (LBW) and IUGR in South Central Asia. Intrauterine growth retardation is defined as being born with a birth weight under the 10th percentile of the birthweight-for-gestational-age reference curve. 8 Low birth weight/IUGR prevalence was found to be as high as 75% in Asia, 20% in Africa, and 5% in Latin America, 7, 8 with many countries exceeding the internationally recommended IUGR and LBW levels. 8 Infants less than 2500 g are 4 times more at risk of neonatal death compared to those weighing 2500 to 3000 g and 10 times more likely than infants weighing 3000 to 3499 g. 9 Risk of postneonatal death is 2 times higher and 4 times higher, respectively. Infants less than 2500 g at birth (small for gestational age) are at an increased risk of diarrhea and pneumonia. 9 A review of long-term effects in relation to body size and body composition indicates that IUGR infants were less likely to exhibit postnatal growth retardation, however at adolescence, they were shorter, lighter, and weaker than infants from a non-IUGR group. 10
Maternal nutritional status has an impact on infant weight and body proportions. Mothers of low weight, height, or body mass index (BMI) are more likely to have lighter, shorter, and thinner babies. 11 There is a link between composition of the mother’s diet and birth outcomes. 12 Moore et al found that consumption of a high percentage of energy from protein in early pregnancy was positively and significantly associated with birth weight (P = .02) as well as placental weight (P = .05). This association was independent of effects of energy intake, weight gain, and confounders such as maternal age, parity, and smoking and was specific to women who had met prespecified criteria of reliable data. For every 1 percentage point (isoenergetic) increase in protein in the diet, a 16 g increase was observed in birth weight (95% confidence interval [CI], 2.8 to 29.2 g) and a 4.2 g increase was found in placental weight (95% CI, –0.4 to 8.5 g). 12 Furthermore, percentage of energy from carbohydrates in early and late pregnancy was negatively associated with ponderal index (a measure of leanness calculated as body weight/height 3 ). The percentage of energy from dairy protein was also associated with birth weight and with ponderal index more strongly than from other sources. For every 1 percentage point increase in dairy protein consumption, a 24 g increase in birth weight (P = .02) and a 0.12 kg/m3 increase in ponderal index (P = .05) was observed. 12 Similarly, women with high intakes of carbohydrate in early pregnancy and low intakes of dairy protein in late pregnancy were likely to have infants who were thin at birth, and women who were low birth weight babies themselves were likely to have thin infants with the infant’s ponderal index falling from 28.3 kg/m3 to 26.2 kg/m3, as the mother’s birth weight decreased from 4000 g to 2500 g or lower. 13
There are very few studies that assess fullfilment of protein needs through pregnancy, however a systematic review of several intervention studies indicated that balanced protein and energy supplementation can have an effect on birth outcomes and could reduce the risk of small-for-gestational age infants (as an indicator of intrauterine growth retardation) by 32%. 6, 7, 14 One study specifically examined the relationship of milk and protein intake by pregnant women and the growing fetus (through ultrasound measurements). Borazjani and coworkers conducted a cross-sectional study of 152 affluent pregnant Indian women recruited from health clinics. These women underwent at least 3 fetal ultrasounds through their gestation. 15 Fetal head circumference, abdominal circumference, femur length, and bioparietal diameter were measured between 16 and 38 weeks of gestation. The mothers’ diets were also evaluated using a 24-hour recall and food frequency questionnaire. Mean protein intake was about 13% of energy, and mean energy was about 2100 kcal/d. The maternal intake data were then stratified into 3 groups according to volume of milk consumed and correlated with the 4 fetal anthropometric measurements. Most of the women (n = 100) fell in the middle milk consumption category, which was about 156 to 456 mL of milk/day. Women in the middle milk category had better fetal measurements than the lower intake group/day (milk consumption less than 156 mL/day, n = 33) as well as the higher intake group (milk consumption greater than 456 mL/day, n = 19). Literature supports the association of not only low protein diets on increased risk of growth retardation but also high protein diets which may lead to increased dietary thermogenesis, thereby leading to a lower availability of energy to the fetus. It should also be noted that the sample size in the third group (high protein) is quite low. 15 A limitation of this study is that the maternal dietary intake measurements were collected after the fetal measurements, so there is an assumption that this one measure of diet is reflective of what happened in the past. The study also would have been enhanced if birth outcome data had been collected.
Role of Protein Quality From Birth to 24 Months
The time from birth to 24 months of age is the second half of the first 1000 days of life. Work done by Shrimpton et al in 2001 and then updated by Victora et al in 2010 showed a consistency in the pattern of linear growth deficits within the first 1000 days globally with the Z score for height-for-age being around 0.5 at 1 month of age, indicative of fetal malnutrition. 16, 17 Protein and amino acids in infancy and childhood play a role in growth, including muscle protein synthesis and linear growth. Evidence indicates that protein restriction leads to low levels of insulin-like growth factor 1 (IGF-1) in healthy children. 18 When older children in the study underwent energy restriction (50% reduction in intake) or protein restriction (reducing protein from 1.0 to 0.66 g/kg body weight per day), both forms of restriction led to a significant decrease in nitrogen balance and decline in IGF-1 concentrations as well as concentrations of specific IGF-binding proteins. Insulin-like growth factor binding protein 2 (IGFBP-2) was responsive to refeeding only in the children who were protein restricted. There is also significant impact of the type and quality of protein on gene expression, especially genes associated with IGF-I and IGFBP-I, both of which play an important role in whole-body protein synthesis and growth promotion and body composition. 19- 22
In the ecological analysis previously referred to, countries with high utilizable protein intakes were found to have a significantly lower prevalence of stunting. A regression analysis examined the association of the prevalence of stunting and total protein or utilizable protein corrected for total energy and income. There is a significant negative relationship between stunting and total energy alone as well as stunting and total protein alone; however, adjusting the model with total protein with total energy makes that latter relationship insignificant. In contrast, when total utilizable protein is used, not only is it strongly and significantly negatively associated with prevalence of stunting, the significant association is retained even when adjusted for total energy. Higher income countries, which have a higher amount of utilizable protein, also show the same relationship. Analysis of the interactions of linear growth and protein quality at the subnational level is undergoing in Uganda. Preliminary findings (unpublished data) indicate a significant positive relationship (unadjusted) between height-for-age Z-scores and the presence of cow’s milk in the diets of Ugandan children aged 6 to 24 months (n = 1300). Logistic and linear regressions were undertaken to determine the factors associated with stunting and height-for-age, respectively. Preliminary results show a strong relationship between stunting and weight-for-height Z scores along with cow’s milk, geographic, social, economic, and education factors. Thus, wasting, having cow’s milk, geographical location, the age, BMI and height of the caregiver as well as being in a cash crop household were strongly associated with being stunted or not in these households (Ghosh et al unpublished).
Protein Quality in the Treatment of Moderate Acute Malnutrition
An area where protein quality is of significant importance is in the food products that are used for the treatment of moderate acute malnutrition (MAM). There are about 20 different products available for the treatment of MAM which may or may not contain a dairy source. It has been of interest to determine how these products perform and compare in terms of changes in linear growth and growth markers as well as in terms of malnutrition, specifically MAM. A recent Cochrane review by Lazzerini et al examined the effectiveness of treating children with MAM in low- to middle-income countries. 23 Qualifying studies looked specifically at different types of formulated foods that were given in full dose, whether they were ready-to-use supplementary foods such as lipid nutrient supplements (LNS) or cereal/legume blends enhanced with dairy or not. The analysis concluded that both LNS and blended foods do have some effect in reducing MAM. Specifically, for LNS, the analysis found that the number of children who recovered was higher by 10%; furthermore, LNS decreased the number of nonrecovering children and slightly improved the nutritional status among the recovered. The analysis also concluded that Corn Soy Blend with added vitamins, minerals and dairy ingredient (CSB++) resulted in similar outcomes compared to LNS. 23
Conclusion
The aim of this article was provide an overview of the role of protein quality within the first 1000 days, emphasizing the importance of protein quality in pregnancy and early growth, examining the potential of high-quality protein in prevention of stunting and treatment of SAM and MAM. The article also provides a summary of the recent changes in protein quality evaluation and the development of a new index, the DIAAS, examining the opportunities and challenges this new methodology presents in assessing protein quality. While the DIAAS will more accurately reflect the quality of the protein, considerable amount of work is still needed for the operationalization of this measure. Protein needs in pregnancy are significantly higher than previously thought. Protein in infancy and early childhood supports both maintenance and growth and needs are the highest across all age-groups in per kg/body weight. This is similarly the case for amino acid requirements as expressed in mg/kg body weight and the amino acid pattern (mg of amino acid/g of protein). The evidence on the effects of balanced protein and energy supplementation during pregnancy is moderately strong, and the impact of protein quality and quantity needs to be considered within the context of interventions that target pregnant women for prenatal services. More data are needed on the role of protein quality and its link to linear growth in infants and young children.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.