
Abstract
Background:
Iron-deficiency anemia is a major public health problem among school-aged children in sub-Saharan Africa.
Objective:
To evaluate the effectiveness of micronutrient-fortified rice to increase hemoglobin (Hb) concentration and reduce the prevalence of anemia among schoolchildren.
Methods:
Nine hundred four schoolchildren participated in this cluster-randomized trial during a 7-month intervention period. The study was conducted in 12 primary schools in rural Burundi. Hemoglobin, socioeconomic status, febrile illness, and dietary diversity were measured at baseline and follow-up. The changes in Hb concentration and anemia status were analyzed using linear and logistic mixed models, respectively. The micronutrient formulation contained an iron-to-zinc molar ratio of approximately 2.2.
Results:
There was no significant difference in Hb concentration between the intervention and control groups (β = .09 g/dL; 95% confidence interval: −0.21 to 0.38) following the 7-month intervention. Nearly half the children reported having a fever within 2 weeks prior to baseline or follow-up. Children with febrile illness preceding follow-up were less than half as likely to show improvement in anemia status (odds ratio = 0.47, P < .001), with an average 0.56 g/dL smaller improvement in Hb at follow-up (P < .001).
Conclusion:
The high prevalence of fever and low iron-to-zinc molar ratio of the Ultra Rice formulation may have contributed to the lack of improvement in Hb. Alternatively, the detected anemia may not have been due to nutrient deficiencies. Anemia interventions in Burundi should implement multiple strategies to eliminate both iron deficiency and infectious causes of anemia.
Introduction
According to the 2013 Global Burden of Disease estimates, iron deficiency is the third largest contributor to disability-adjusted life years (DALYs) among school-aged children in sub-Saharan Africa. 1 Iron-deficiency anemia results in lethargy and reduces children’s ability to learn and play. Children with anemia are less likely to attend school, and chronic anemia can lead to severe adverse outcomes, such as impaired cognitive function, below-average motor skills, and altered social–emotional outcomes. 2 -5 The World Health Organization (WHO) estimates that one-quarter of all school-aged children and nearly one-half (48%) of school-aged children in developing countries are anemic. 6 , 7 Even mild iron deficiency can be deleterious to child health, despite the absence of clinical anemia. 8 Ultimately, the high prevalence and negative consequences of iron-deficiency anemia in all age-groups result in a median loss of more than 4% of the gross domestic product in developing countries. 9
Anemia, clinically identified by reduced red blood cell mass or low blood hemoglobin (Hb) concentration, can result from one or multiple etiologic pathways, including micronutrient deficiencies, infection, inflammation, and hemoglobinopathies. The WHO hypothesizes half of all cases with anemia to be related to insufficient dietary iron intake 10 and thus remedied with greater intake of iron-rich foods such as meat, poultry, fish, eggs, and beans. Infectious diseases can lead to anemia and are widely prevalent in sub-Saharan Africa. Common infections such as hookworm and malaria lead to anemia primarily from chronic blood loss and red blood cell lysis, respectively. Coinfection with malaria and soil-transmitted helminths falls heavily on school-aged children. 11 Other infectious agents that do not cause blood loss can also cause anemia due to the host’s response to invading pathogens. To prevent pathogens from appropriating the host’s iron, dietary iron absorption is reduced, and iron is sequestered in the blood by macrophages. 12 -14 Hemoglobinopathies are a group of diseases characterized by the production of an abnormal Hb molecule leading to anemia. Sickle cell anemia is one such hemoglobinopathy highly prevalent near the equator with levels reaching 20% to 30% in the neighboring Democratic Republic of Congo and 45% in parts of Uganda. 15 Because of these overlapping risk factors, it is likely that many cases of anemia in sub-Saharan Africa are multicausal.
Burundi has a high prevalence of many anemia risk factors. The staple diet relies heavily on cereals, legumes, and vegetables and less on animal-sourced, iron-rich foods. 16 Almost 80% of the population of Burundi lives in malaria-endemic areas, and one-quarter lives in areas of particularly high incidence. 17 As with other countries in the region, hookworm prevalence ranges from 10% to 50%. 18 According to the 2010 Burundi Demographic and Health Survey (DHS), overall prevalence of anemia is approximately 45% in children younger than 5 years and 19% in women of childbearing age. Data for the prevalence of anemia for school-aged children are not available in the DHS. 19 Although there is little information regarding the prevalence of hemoglobinopathies in Burundi, sickle cell anemia is estimated to affect 10% to 40% of the population due its periequatorial location. 15
On a population scale, iron fortification and supplementation programs are both attractive options to reduce anemia due to dietary inadequacy. Although population-based fortification strategies are engineered to prevent dietary deficiencies, supplementation programs are designed to treat and prevent clinical deficiencies. A cost-effectiveness analysis suggests that population-based iron fortification programs are economically more attractive than supplementation programs and could prevent more than 1 million DALYs due to anemia in sub-Saharan Africa. 20
Rice is a staple food for millions of people living in regions where iron-deficiency anemia is a significant public health problem and could serve as a vehicle for micronutrient fortificants. The Ultra Rice technology (“Ultra Rice” is a registered trademark in the United States of Bon Dente International, Inc, Lynden, WA, USA) uses a hot extrusion process to add micronutrients to rice flour, creating pasta-like rice kernels. The fortified rice kernels are mixed with milled (traditional unfortified) rice to produce fortified (blended) rice. Fortified rice is then cooked and served in accordance with ordinary/usual dietary practices.
The Ultra Rice technology has been tested for its effectiveness in alleviating anemia in young children, schoolchildren, and women of reproductive age. Seven clinical trials have examined the impact of iron-only fortified rice on anemia 21 -27 ; all found consistent improvements in iron status (ie, ferritin), and 5 of the 7 also documented significant improvements in anemia status. 21 -25 Only recently has fortified rice been formulated to provide multiple micronutrients in addition to iron. However, the results from 2 published studies in India and Thailand, using multiple micronutrient formulations, provided between 6.25 and 12.5 mg of iron daily and yet reported inconsistent results for iron status. 28 , 29 It is unclear whether this is due to the differing baseline health status of the study samples, possible interactions between micronutrients in the formulations, high rates of infection among the populations studied, or other factors. Therefore, the effectiveness of the multiple micronutrient formulation to improve iron status must still be proven. Multiple micronutrient-fortified rice was recently added to the list of commodities available for purchase from the United States Department of Agriculture and will be available through programs around the world (http://www.fsa.usda.gov/Internet/FSA_File/mr24.pdf).
This cluster-randomized trial tested the efficacy of a multiple micronutrient-fortified rice formulation to improve Hb concentration and reduce anemia prevalence among children participating in a school feeding program in Muyinga Province of the Republic of Burundi. This study marks the first time that a formulation containing iron, zinc, thiamine, and folic acid has been tested in a clinical trial as well as the first time the Ultra Rice technology has been tested in sub-Saharan Africa.
Methods
This study was approved by the Comité National d’Ethique du Burundi and the PATH Research Ethics Committee. Parents of all participants provided written informed consent, and children gave verbal assent.
Study Setting and Population
The study was conducted in Muyinga Province in northeastern Burundi. Ninety-five percent of the population in this province is engaged in agriculture, and the diet consists primarily of high-starch foods such as plantains, bananas, cassava, maize, and white sweet potato, typically accompanied by beans and/or other vegetables. 30 The World Food Programme (WFP), in coordination with World Vision, operates a school feeding program for 20 schools in the Gashoho and Gasorwe communes. Twelve of these schools were randomly selected to participate in this study, and the remaining 8 schools participated in a separate operational study. The altitude of the region ranges from 1400 to 1750 m above sea level.
Children were eligible for the study if they were 7 to 11 years of age and had Hb concentrations of ≥7.0 and <12.0 g/dL upon screening; 7.0 g/dL is the upper limit/criterion for anemia treatment in Burundi and 11.9 g/dL is the WHO’s upper limit for any anemia at an altitude of 1500 m above sea level. In addition, all eligible children had received albendazole as a deworming medicine 2 weeks prior to study enrollment and planned to continue in the same school for the entire academic year. Children were excluded from the study if they had taken vitamin or iron supplements during the past 30 days, they were planning to take vitamin or iron supplements during the following 8 months (as reported by the caregiver), their parents gave verbal confirmation of chronic or acute illness, metabolic disorder, severe malnutrition, or any other serious medical ailment, or they would be unable to attend the scheduled visits or comply with the study procedures.
Rice Fortification Process
The Brazilian manufacturer, Adorella (Indaiatuba, Brazil), supplied Ultra Rice-fortified grains for this study. The study team established blending operations in a World Vision warehouse in Muyinga using a Toshniwal mixing unit (Chennai, India) to blend the fortified kernels into milled rice at a ratio of 1:100.
School Feeding Program
The study team transported milled (unfortified) rice and fortified (blended) rice once every 2 weeks to the schools. Parent committees managed the school canteens and performed all cooking, serving, and clean-up duties on a volunteer basis. Three trained World Vision food monitors supervised the school feeding program to ensure that commodities were used as intended.
Study Design
This study was a single-blinded, placebo-controlled, cluster-randomized trial. The study team randomized 12 schools to receive either fortified rice (intervention group) or milled rice (control group). All children in the schools, regardless of enrollment in the study, received the daily school lunch of rice (150-g dry ration) and beans prepared with vitamin A-fortified oil and iodized salt. All children attending the intervention group schools received a fortified rice ration containing iron (17.8 mg), zinc (8.5 mg), thiamine (1.8 mg), and folic acid (600 μg) for 5 days per week for 7 months as a part of the daily school meal. All children attending the control group schools received an equivalent ration of WFP-milled (unfortified) rice containing endogenous quantities of iron (1.2 mg), zinc (1.7 mg), thiamin (0.1 mg), and folate (14 μg). Students did not receive meals during two 2-week holiday periods: one in December and one in April, when schools were closed. Students also did not receive the meals during a 2-week period in March due to commodity procurement problems following a major fire and subsequent loss of the nation’s primary market in Bujumbura.
Questionnaire
At both baseline and follow-up, trained data collection staff interviewed parents regarding household sanitation, household assets, animal ownership, recent febrile illness in children, and bed net use. At baseline and follow-up, the staff also conducted a 24-hour dietary diversity recall to assess the child’s consumption of each food category using the Food and Nutrition Technical Assistance Project (FANTA) predefined food groups adapted to the Burundi setting. 31
Hemoglobin Testing
The study team measured enrolled children’s Hb concentrations at baseline and follow-up. A single drop of blood was obtained from each child using a 2.25-mm HemoCue Safety Lancet (HemoCue, Ängelholm, Sweden). Hemoglobin concentration was measured using a HemoCue Hb 201+ analyzer on site. Children found to have a Hb concentration <7.0 g/dL were not enrolled and were given iron supplementation tablets (in the form of iron–folic acid supplements for 3 months) procured from their local health center, in accordance with Burundi Ministry of Health treatment guidelines. These children were provided transportation to the provincial hospital, a consultation with a local doctor, and any medicines required to resolve current infections. Similar provisions were given to any child found to have a Hb concentration <7.0 g/dL at follow-up.
Statistical Analysis
Data were entered and stored in CSPro 4.1, and statistical analyses were performed in Stata/SE 11.0 (StataCorp, College Station, Texas). Descriptive statistics were tabulated to consider baseline imbalances between the intervention and control groups. Mean and standard deviation were calculated for continuous variables, and percentages were calculated for binary variables. Socioeconomic status was assessed through a composite wealth index score calculated using principal component analysis (PCA), as described elsewhere. 32 Variables incorporated into the PCA score included those regarding sanitation, house ownership, assets, owned animals, and parents’ education. Dietary diversity was also assessed through a composite score using the FANTA guidelines for measuring individual dietary diversity. 31 To create the score, food recall responses were aggregated into 8 categories. Each child was given a score that reflected the sum of the food categories consumed in the past 24 hours. Consumption of iron-rich foods—including meat, poultry, fish, legumes, eggs, and leafy greens—was scored on a scale of 0 to 6.
Anemia category classifications were based on WHO standards for school-aged children at 1500 m above sea level, where Hb 11.5 to 11.9 g/dL signifies mild anemia, Hb 8.5 to 11.4 g/dL signifies moderate anemia, and Hb <8.5 g/dL signifies severe anemia. 33 Since children with Hb concentrations <7.0 g/dL were excluded from enrollment, for the purpose of this study, severe anemia was defined as ≥7.0 g/dL and <8.5 g/dL. Because of the low number of children with severe anemia (7.0-8.4 g/dL) at baseline (n = 3), moderate and severe anemia were combined into 1 group.
Two anemia outcomes were analyzed. The first was the change in Hb concentration between baseline and follow-up (Hb difference = follow-up Hb concentration − baseline Hb concentration). This model was constructed using a linear mixed model to account for clustering by school. Because of the small number of clusters, restricted maximum likelihood estimates were calculated. The second outcome was a binary variable representing an improvement in anemia status between baseline and follow-up (anemia improvement = mild anemia at baseline AND no anemia at follow-up; OR moderate anemia at baseline AND mild or no anemia at follow-up). The second model was constructed using a logistic mixed model. The primary models were not adjusted for any additional covariates, although we did conduct a sensitivity analyses to assess whether the results differed after adjustment for characteristics that were found to be imbalanced between the intervention groups at baseline. Differences between groups were considered significant at P < .05.
Prespecified interactions terms were assessed in the mixed models. These terms included age, sex, socioeconomic status quintile, recent fever, and dietary diversity. Secondary analyses explored other factors that influenced Hb status at follow-up, irrespective of the intervention group.
Results
At baseline, 2854 children were screened for anemia (Figure 1). A total of 1071 children had mild or moderate anemia and were enrolled in the study. Nine hundred four were followed up and evaluated for anemia after 7 months: 461 in the intervention group and 443 in the control group.
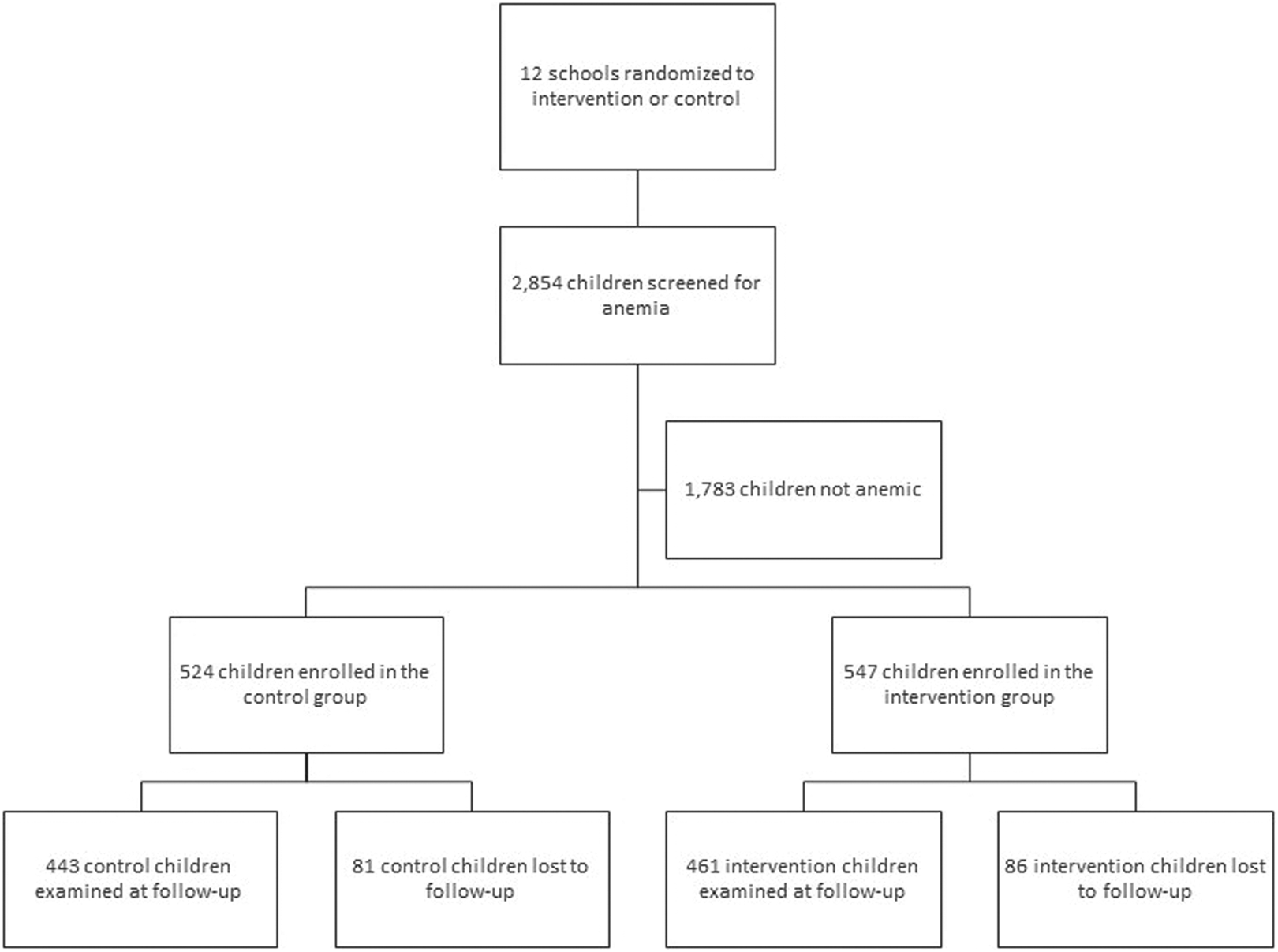
Number of children screened for anemia, enrolled in each study group, and examined at baseline and follow-up.
Descriptive Statistics
Baseline characteristics of the 2 groups were similar (Table 1). Overall, the mean age was 8.9 years, and about 53% of the enrolled children were female. School absenteeism was similar between the 2 groups. Socioeconomic status scores were balanced, and there was little variability in household sanitation. Nearly half of the children in both groups reportedly had a fever within the previous 2 weeks, both at baseline and at follow-up (data not shown). Children in the intervention schools, however, had a higher baseline prevalence of mild or moderate anemia (43.8%) compared with those in the control schools (35.1%; Table 2). Further, after exclusion of nonanemic students, children at the intervention schools had an average Hb concentration at baseline that was 0.3 g/dL lower (P < .05) than that of children in the control group and a higher proportion of moderately or severely anemic children (79% vs 72%; Table 3).
Baseline Characteristics of Study Participants by Group.
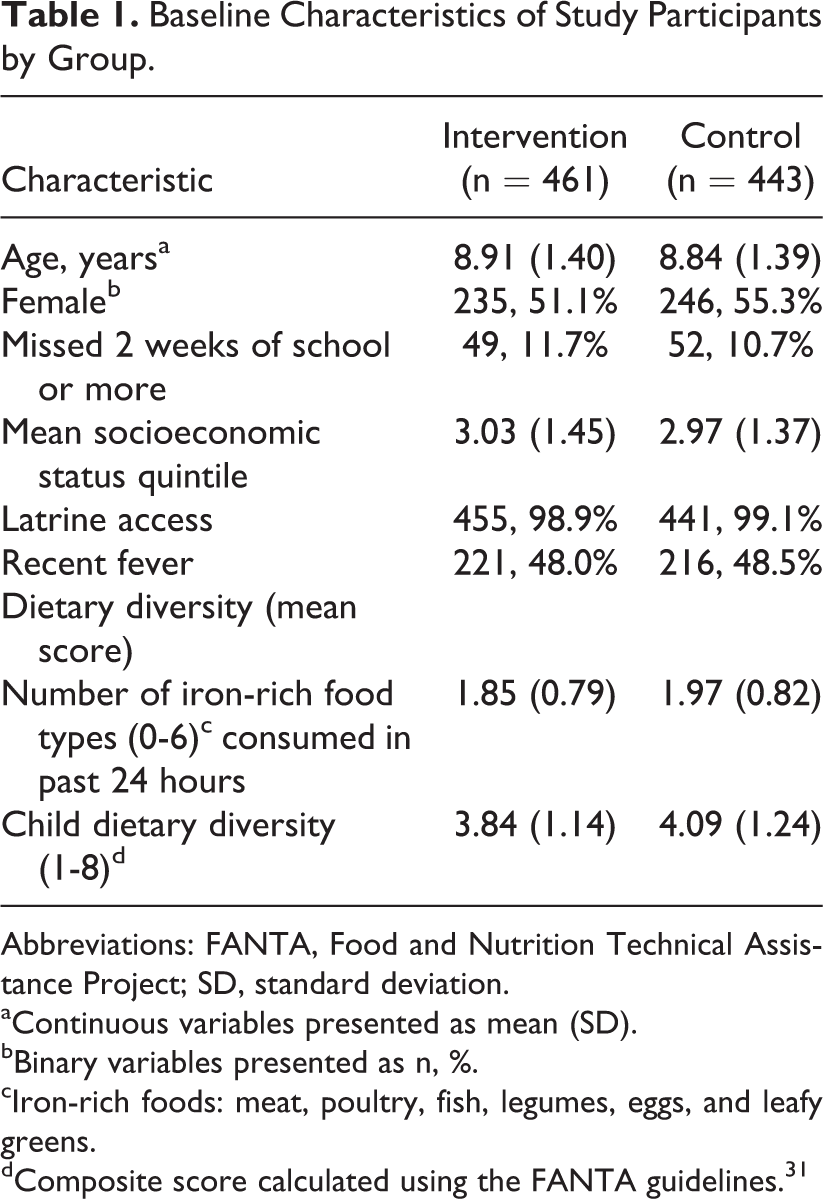
Abbreviations: FANTA, Food and Nutrition Technical Assistance Project; SD, standard deviation.
aContinuous variables presented as mean (SD).
bBinary variables presented as n, %.
cIron-rich foods: meat, poultry, fish, legumes, eggs, and leafy greens.
dComposite score calculated using the FANTA guidelines. 31
Baseline Anemia Prevalence at Each Participating School.a
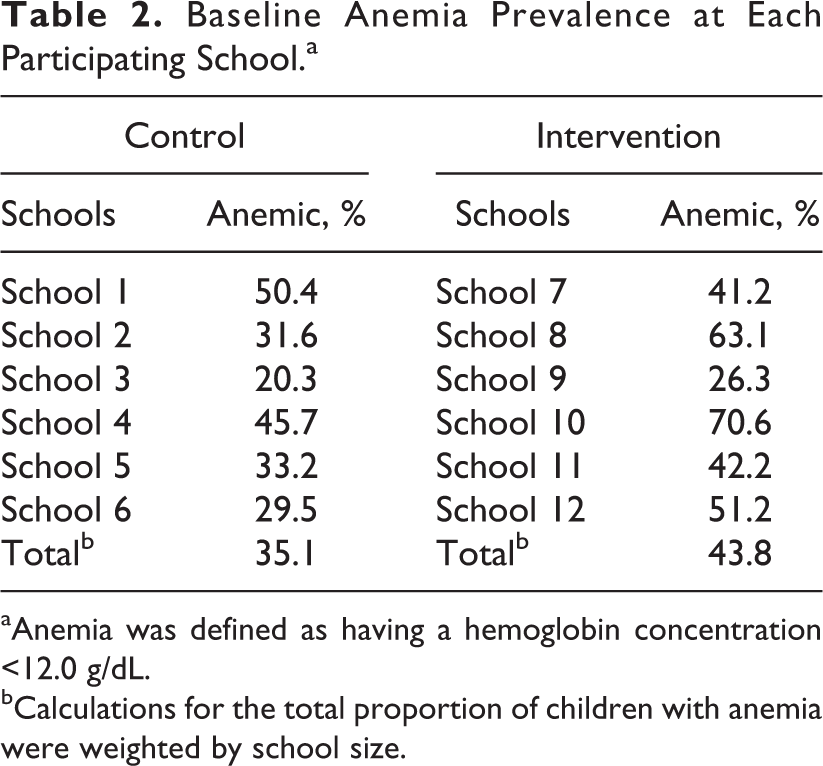
aAnemia was defined as having a hemoglobin concentration <12.0 g/dL.
bCalculations for the total proportion of children with anemia were weighted by school size.
Description of Hb and Anemia Status of Study Participants by Group.a
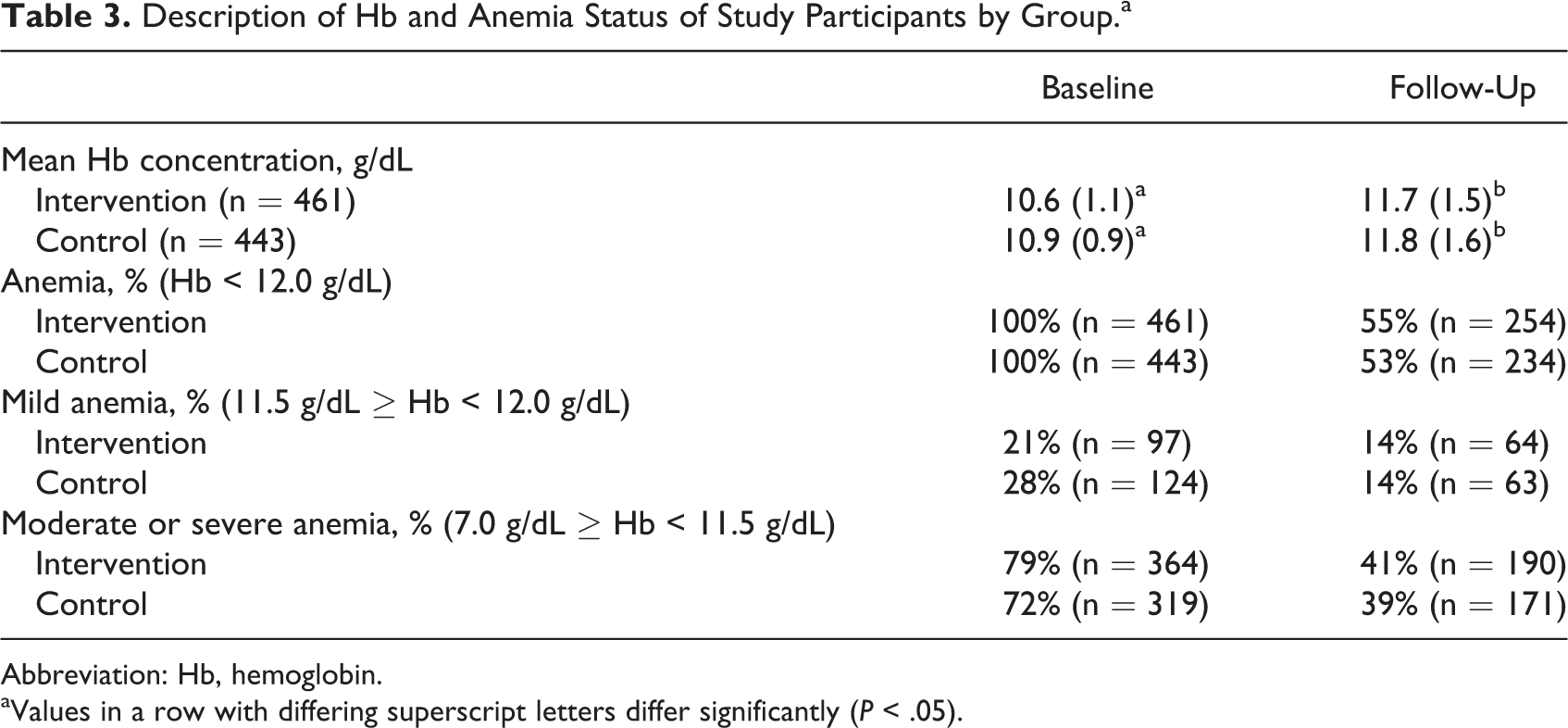
Abbreviation: Hb, hemoglobin.
aValues in a row with differing superscript letters differ significantly (P < .05).
The 24-hour dietary diversity recall showed that the intervention and control groups had similar numbers of recently ingested iron-rich foods at both baseline and follow-up. Consumption of each food group was very similar between the groups at both baseline and follow-up (data not shown), with only 1 difference at follow-up: 43% in the control group had recently eaten meat, poultry, or seafood in comparison to only 30% in the intervention group. Despite this one difference, the food group consumption of the 2 groups was combined in Figure 2 to illustrate seasonal differences between November 2012 (baseline) and June 2013 (follow-up). At baseline and follow-up, children in both the intervention and control groups had a mean intake of approximately 4 food groups within the previous 24 hours (Table 1). Although there is no reference standard for dietary diversity among school-aged children, FANTA has proposed categories for young children where 0 to 2 food groups constitute low dietary diversity, 3 to 4 food groups represent medium diversity, and 5 or more constitute high diversity. 34
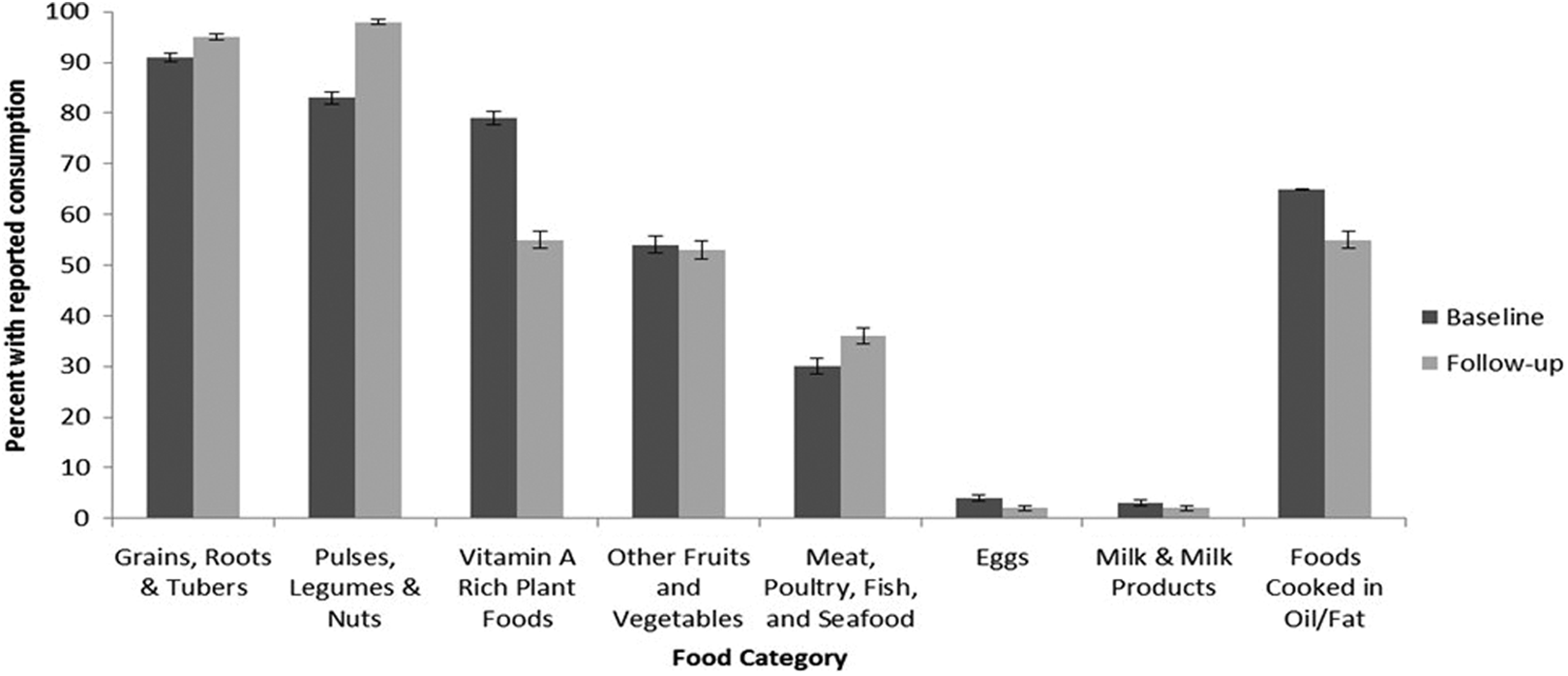
Percentage of children reporting consumption of at least 1 food from each food group at baseline (November 2012) and follow-up (June 2013; n = 904).
Biochemical/Hematological Outcomes
At follow-up, 55% and 53% of children in the intervention and control groups, respectively, were still classified as anemic, and the prevalence of mild and moderate or severe anemia did not significantly differ between the groups. Both the intervention and control groups had improved Hb levels and anemia status, with an overall average improvement in Hb concentration of 1.0 g/dL. According to the linear model, the intervention group had a 0.09 g/dL (95% confidence interval [CI]: −0.21 to 0.38) greater increase in Hb concentration between baseline and follow-up compared with the control group, but this difference was not statistically significant (P = .57; Table 4). According to the logit model, the intervention group did not show greater improvement in anemia status compared with controls (odds ratio [OR]: 0.85; 95% CI: 0.51-1.43; P = .55; Table 4). The proportion of females and dietary diversity scores was slightly imbalanced between the intervention groups at baseline. After adjusting for these 2 characteristics as a sensitivity analysis, we did not see meaningful differences in the results of the primary models as reported previously.
Mixed Models of the Change in Hemoglobin and Anemia Status Between the Baseline and the End of Study Comparing the Intervention Group to Controls.
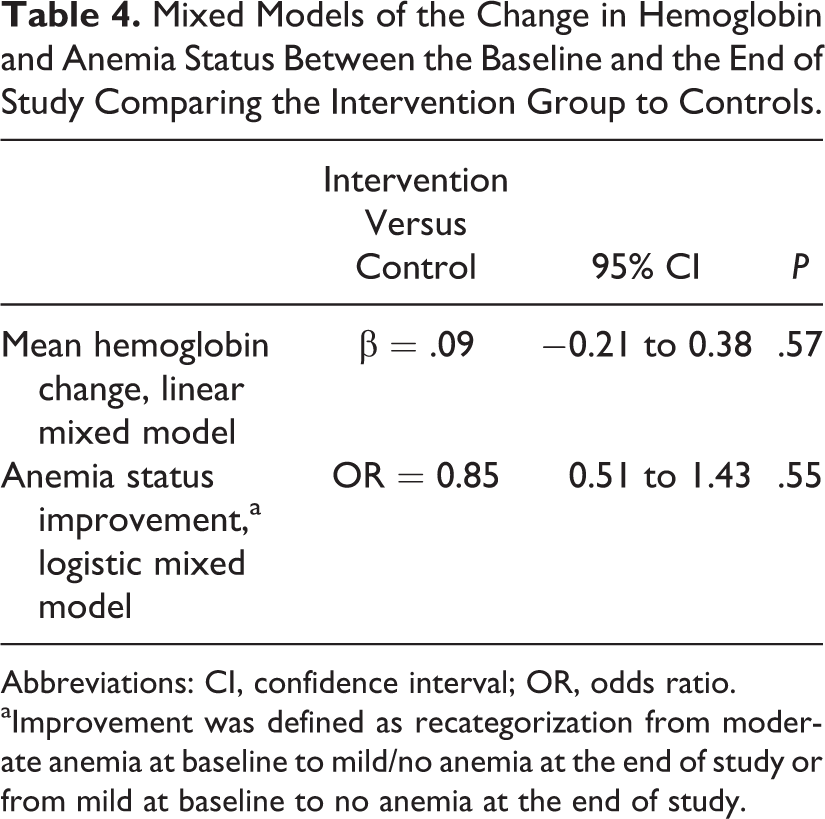
Abbreviations: CI, confidence interval; OR, odds ratio.
aImprovement was defined as recategorization from moderate anemia at baseline to mild/no anemia at the end of study or from mild at baseline to no anemia at the end of study.
Secondary analyses did not reveal any meaningful interactions between the intervention and age, sex, socioeconomic status, fever, or dietary diversity. However, we found that fever strongly influenced Hb concentration, irrespective of the group. Those with fever within 2 weeks of baseline measurement had a mean Hb level 0.20 g/dL lower than those without fever (P < .01). Those with fever within 2 weeks of follow-up were less than half as likely to show improvement in anemia status between baseline and follow-up (OR: 0.47, P < .001), with an average 0.56 g/dL smaller improvement in Hb levels at follow-up (P < .001).
Discussion
This 7-month, cluster-randomized trial tested whether a formulation of fortified rice containing iron, zinc, thiamine, and folic acid could successfully treat anemia among schoolchildren in Burundi. We did not observe significantly different improvements in Hb concentrations between the intervention and control groups. Similar results have been found in previous studies 26 feeding rice fortified with multiple micronutrients. Possible reasons for the lack of demonstrated intervention effect may include interactions among micronutrients 35 , 36 or fortificant compounds used, the quality of the total diet, the health of the sample population at baseline, the presence of infection or inflammation, or simply that nutrient deficiencies may not be the primary cause(s) of anemia within this sample. 12 , 37
To date, 2 studies using rice fortified with multiple micronutrients have been published. In India, fortified rice containing iron (6.25 or 12.5 mg), zinc (3 mg), vitamin A (0.5 mg), thiamine (0.4 mg), niacin (5 mg), vitamin B6 (0.4 mg), folic acid (75 μg), and vitamin B12 (0.75 µg) was provided per 100-g dry ration to a combined sample of anemic (61%) and nonanemic schoolchildren exhibiting very low levels (7%) of iron deficiency (<15 µg/L of ferritin) at baseline. 29 In Thailand, fortified rice containing iron (10 mg), zinc (9 mg), and vitamin A (890 µg) was provided to zinc-deficient schoolchildren with low baseline levels of anemia (10%), iron deficiency (9%), and vitamin A deficiency (3%). 28 Neither study found significant improvements in iron status but documented improvements in zinc, vitamin A, and vitamin B12 status, as well as physical performance. Although not all enrolled children were anemic, the average Hb concentrations were low (near the WHO cutoff of 11.5 g/dL).
Because vulnerable populations in resource-poor settings frequently have both iron and zinc deficiencies, providing both nutrients in a formulation with multiple micronutrients could be an efficient approach. Although some studies have indicated that separating the supplementation of iron and zinc may be more effective on child biochemical outcomes than combining iron and zinc into one therapy, 35 , 36 , 38 other studies have not demonstrated the same relationship. 39 , 40 Thus, there is no strong evidence to discourage joint supplementation or, by extension, fortification. 5 In our Burundi trial, both the intervention and control groups demonstrated improvements in Hb concentration after 7 months, but the intervention group did not improve significantly more than the control group. Since this study did not measure serum ferritin, no conclusions can be made regarding the effects of this multiple micronutrient formulation on iron stores. Preliminary investigation into this topic with Abbott Nutrition has suggested the iron-to-zinc molar ratio may determine the level of Hb and ferritin improvement. 41 The effective iron-only rice formulations 21 -25 had iron-to-zinc molar ratios ranging from 13 to 27, whereas the multiple micronutrient formulations had iron-to-zinc molar ratios below 4. Although a closer examination of the formulation is necessary, the food used as the nutrient delivery vehicle must also be investigated because food crops such as rice and wheat may bind zinc more readily, thereby delivering it to the body more effectively than iron. 42
Rice fortification presents a technical challenge because it requires using an iron source that is white in order to mimic the appearance of traditional rice. Unfortunately, the most bioavailable forms of iron used in food fortification (eg, iron sulfate) are brown in color and therefore unsuitable for rice. Currently, the most appropriate iron source for rice fortification is ferric pyrophosphate (FePP), a white compound with reduced bioavailability. Micronized versions of FePP are used to enhance surface area and thus iron solubility, but this compound remains less effective than traditional iron sources as a fortificant and may be more sensitive to zinc. 41
The lack of improvement in Hb concentration and anemia status may also have been influenced by the quality of the overall diet and parasitic infections. The traditional diet among our study population was not likely to provide sufficient quantities of vitamin A, vitamin C, riboflavin, and vitamin B12 to support iron absorption and utilization of iron for Hb synthesis. 43 -46 It is estimated that only 34% of anemia in Africa can be corrected via supplementation, 47 suggesting other issues are at play. Burundian children are at risk of anemia-causing parasitic infections such as malaria and hookworm. Whereas febrile malarial infection causes anemia by destroying red blood cells and decreasing production of erythrocytes in the bone marrow, afebrile malaria can cause anemia by causing inflammation, increasing hepcidin, and reducing iron absorption. 48 Current statistics indicate the prevalence of hookworm in this region to be moderate (30%), and anemia due to heavy hookworm infections within individuals may be rare. 18 Since all children were provided with albendazole biannually and nearly all families had access to latrines, hookworm infection was an unlikely cause of anemia.
The most notable association from secondary analyses was the strong relationship between fever and anemia status. Irrespective of the group, fever reported in the 2 weeks before baseline was strongly related to Hb levels at baseline. Fever reported within the 2 weeks before follow-up was associated not only with low follow-up Hb concentrations but also with whether the child’s Hb concentration had improved from baseline. Nearly half of the children reported experiencing a fever before baseline, and nearly half reported a fever before follow-up; 70% reported fever at either/one or the other time point. The major causes of fever in Burundi include malaria, respiratory illness, and diarrheal illness. 1 Recent Burundi DHS reports of malaria show that Muyinga province region has the country’s highest prevalence of malaria parasitemia in children younger than 5 years, indicating a high level of transmission. 19 Febrile illness, due to either malaria or other infectious etiology, likely caused a large proportion of the anemia burden in this study sample, and those affected are unlikely to improve via food fortification.
Limitations
This study was limited in that it measured Hb but not biomarkers of other nutrients added to the rice. It was the original intention of this study to measure both ferritin and C-reactive protein, but logistical and budget issues prevented this from happening. Without ferritin data, it is impossible to determine whether the intervention improved child iron stores, which can occur without a change in Hb in areas with high prevalence of febrile illness. Although this study enrolled only children with anemia, it is unclear whether the anemia was due to dietary deficiencies, and such determinations should be required for enrollment. The high rates of anemia resolution in both groups may be due to the incorporation of an extra meal into the children’s diets or may be related to the biannual deworming events, and baseline anemia tests were conducted following the first school year deworming event when Hb concentrations would have been lowest. Another plausible explanation is the phenomenon of regression to the mean, whereby a proportion of children with anemia naturally resolved the condition on their own without intervention. In addition, although each child was given an equal ration of rice, the quantity consumed was not measured. There was at least one report of a child saving his/her lunch so it could be shared with his/her family at dinner time. Lastly, this study might have gained additional insight by conducting a 3-day weighed food record with a random sample of study participants to calculate the typical amount of phytic acid consumed and the average iron-to-phytic acid molar ratio. Phytic acid binds iron, reducing its availability for absorption into the body. 49
Conclusion
Successfully addressing anemia among school-aged children in Burundi will likely require multiple, simultaneous interventions but first requires data on the prevalence of iron deficiency and iron-deficiency anemia to ensure it is an issue. Future studies are likely to continue to confirm the effectiveness of fortification programs, but clinical anemia will not be overcome until comprehensive interventions, both nutrition specific and nutrition sensitive, address all underlying causes.
Footnotes
Acknowledgments
The authors thank the families who participated in this study.
Authors’ Note
All authors participated in the design and/or analysis and interpretation of the data and revision of the manuscript. Emily Mosites and Megan E. Parker conducted the statistical analyses, reviewed the literature, and prepared the manuscript with assistance from Melody Waring, Dipika Matthias, Kathryn Reider, Nicolas Ndayishimiye, and Leonidas Ndikuriyo. Dipika Matthias designed the study and the study’s analytical strategy and revised the manuscript. Dipika Matthias and Gloriose Nyandimbane coordinated the implementation of the study and assisted with data interpretation and manuscript revisions.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this study was provided by the United States Department of Agriculture (USDA) grant #2010-38418-21635 with supplemental funding from Open Road Alliance.