
Abstract
Background:
Nutritional anemia is a public health problem among Ghanaian schoolchildren. There is need to employ dietary modification strategies to solve this problem through school and household feeding programs.
Objective:
To evaluate the effectiveness of cowpea-based food containing fish meal served with vitamin C–rich drink to improve iron stores and hemoglobin concentrations in Ghanaian schoolchildren.
Methods:
The study involved cross-sectional baseline and nutrition intervention phases. There were 150 participants of age 6 to 12 years. They were randomly assigned to 3 groups, fish meal –vitamin C (n = 50), vitamin C (n = 50), and control (n = 50), and given different cowpea-based diets for a 6-month period. Height and weight measurements were done according to the standard procedures, dietary data were obtained by 24-hour recall and food frequency questionnaire, hemoglobin concentrations were determined by Hemocue Hemoglobinometer, and serum ferritin and complement-reactive protein (CRP) were determined by enzyme-linked immunosorbent assay. Participants’ blood samples were examined for malaria parasitemia and stools for helminthes using Giemsa stain and Kato-Katz techniques, respectively.
Results:
Mean ferritin concentration was not significantly different among groups. End line mean or change in hemoglobin concentrations between fish meal–vitamin C group (128.4 ± 7.2/8.3 ± 10.6 g/L) and control (123.1 ± 6.6/4.2 ± 10.4 g/L) were different, P < .05. Change in prevalence of anemia in fish meal–vitamin C group (19.5%) was different compared to those of vitamin C group (9.3%) and the control (12.2%). Levels of malaria parasitemia and high CRP among study participants at baseline and end line were 58% and 80% then 55% and 79%, respectively. Level of hookworm infestation was 13%.
Conclusion:
Cowpea-based food containing 3% fish meal and served with vitamin C–rich drink improved hemoglobin concentration and minimized the prevalence of anemia among the study participants.
Introduction
Iron deficiency (ID) is the most prevalent hematologic disorder in childhood, 1 and it is an issue of public health concern in both developed and developing countries. It has adverse consequences on cognitive performance, growth of children, physical capacity and work performance, and immune status and morbidity from infections in all age-groups. 2 One major consequence of ID is anemia, the commonest syndrome reported by a high proportion of the world’s population. 3,4
In terms of prevalence, the numbers are staggering: 2 billion people—over 30% of the world’s population are anemic mostly due to ID. 5 Some studies have shown that 50% of anemia in the world is attributable to ID, 6,7 and nearly 245 million of the world’s children from 0 to 59 months of age have anemia. 8 In both developing and developed countries, the prevalence of anemia has a social imbalance. 9 Overall, it is the most vulnerable, poorest, and the least educated who are disproportionately affected by ID, and it is they who stand to gain the most by its reduction. 5 In Ghana, a few studies have reported prevalence of anemia as a public health concern: 76% of children younger than 5 years of age, 10 73% of children 2 to 10 years old, 11 63% of schoolchildren 5 to 12 years old, 12 and 25% of vegetarian and nonvegetarian children 13 had some degree of anemia.
The causes of ID and anemia are multifactorial, but poor iron bioavailability rather than inadequate dietary iron intake is suggested as the major contributing factor in sub-Saharan Africa and other developing nations. 14 The consumption of habitual diets of cereal and legume staples in rural Africa, which are high in antinutritional factors, is another major cause of ID and anaemia. 15 Cowpeas, as legumes, are a rich source of protein, nonheme iron, and some antinutritional factors. 16,17
Dietary modification or diversification, supplementation, and food fortification are nutritional strategies to combat ID and anemia. Dietary modification or diversification aims at improving nutritional value and iron bioavailability. The mere addition of iron to staple foods in developing countries, without providing an enhancer of iron absorption, is unlikely to have significant positive effect on iron status. 15 This finding underscores the need for new approaches to improve iron bioavailability in foods. The addition of enhancers to a diet or their consumption as part of a diet is an essence of dietary modification or diversification.
By increasing the intake of iron enhancers with a low iron bioavailable diet (5%) may result in a diet of higher iron bioavailability (10%). 18 This study evaluated the impact of fish powder and vitamin C–rich drink consumption with cowpea-based food on the iron stores, hemoglobin concentrations, and prevalence of anemia among Ghanaian schoolchildren in a malaria endemic area.
Methodology
Study Design
The study involved a 2-week, cross-sectional baseline phase and 6-month nutrition intervention phase, followed by an end line data, blood and stool samples collection and analysis. Eligibility criteria were parental and individual consent to participate, child not being allergic to cowpea-based foods, not severely anemic (hemoglobin concentration > 75 g/L), not on any iron supplements, and 6 to 12 years old. A total of 162 schoolchildren aged 6 to 12 years were selected to participate in the study. One hundred and fifty children provided blood and stool samples at baseline. These were randomized into 3 groups: fish meal with vitamin C group (n = 50), vitamin C group (n = 50), and the control group (n = 50) for the intervention study. Blood and stool samples were collected from each participant and transported on ice to Noguchi Memorial Institute for Medical Research (NMIMR) for biochemical and parasitological analyses, respectively.
Study Area
The study was conducted in Adaklu Kodzobi basic school complex in the Adaklu-Anyigbe district of the Volta Region of Ghana. Volta Region is in the Eastern part of Ghana sharing border with Togo. Adaklu-Anyigbe district is between Ho municipality, North and South Tongu districts. The main occupation of people in the area is farming. Farmers cultivate mainly maize, cassava cowpea, and beans. The sources of domestic water in Adaklu Kodzobi include pipe borne and stream. There is no usable latrine, so people tend to use nearby bushes.
Study Participants
Using a power of 80% with a 2-sided test significance level of 5% and mean difference in ferritin level and standard deviation from a previous work, 19 a minimum sample size of 143 was estimated. To account for refusals (estimated at 13%), the desired sample size was increased to 162, comprising 81 females and 81 males. A sampling frame of public basic schools not benefitting from the Ghana school feeding program (GSFP) was constructed for the district, and Adaklu Kodzobi basic school was selected at random. Pupils (aged 6-12 years) in lower and upper primary as well as junior high school were randomly selected after stratification based on sex. Initially, 162 children provided assent to participate in the study, but only 150 (77 males and 73 females) subsequently provided biological samples for biochemical analysis and parasitological examinations. Reasons for refusals were religious (giving out one’s blood is giving up one’s life) and customary (it is unclean to give stool to one’s neighbor).
Data Collection and Measurements
Baseline Phase
Sociodemographic data in the form of household characteristics (parental age, occupation, education, monthly income, and household size) and community facilities (source of water, light, fuel, and food) were obtained from parents of the study participants in the form of interviews using combined open-ended and semi-structured questionnaires. Height and weight measurements were taken according to the standard procedures. 20 Weight measurements were made using electronic bathroom scale (Precision Health Scale UC-300, A and D Company Limited, Higashi-Ikebukuro, Toshima-Ku, Tokyo, Japan). The weight of each participant was measured in triplicate and recorded to the nearest 0.1 kg. The average of the 3 readings was considered the actual weight of the participant. All weight measurements were done with the participants wearing minimal clothing possible. Weight measurements were done an hour before lunch break at school. An object with a known weight was routinely weighed to ascertain the validity of scale readings. Each child’s height was taken with a wooden stadiometer in a standing position. Heights were taken in triplicate to the nearest 0.1 cm. The average of the 3 readings was recorded as the true value for each participant. Five milliliters of fasting venous blood was collected from each participant by a phlebotomist into Eppendorf tubes without anticoagulants in the morning before breakfast. Also, about 2 to 3 g spatula (teaspoon size) of stool was obtained from each participant by a parasitologist early in the morning before breakfast.
Prior to distribution of stool containers, parents or caregivers of participating children were educated on the proper way of taking the sample and all the necessary precautions to take. Stool samples were obtained early in the morning, immediately transported on ice to the Department of Parasitology, NMIMR, and analyzed for the presence of soil-transmitted helminthes.
Hemoglobin concentrations were determined immediately in the field using a Hemocue Hemoglobinometer (Hemocue AB, Angelhom, Sweden). Children with hemoglobin <75 g/L though excluded from the study were referred by the medical officer of the study team to the Ho municipal hospital for treatment. The blood and stool samples collected were transported on ice to NMIMR after preparation of thin and thick blood films in the field. Blood samples were centrifuged at 3000 rpm for 15 minutes in the laboratory and serum aliquots were prepared and stored at −80°C until they were analyzed.
Serum ferritin levels were measured using an enzyme-linked immunosorbent assay (ELISA), (Ferritin ELISA kit, Cat No. 1810; Alpha Diagnostics Inc, San Antonio, Texas). Human complement reactive protein (CRP) levels, which indicate the presence of inflammation, were determined by ELISA (CRP ELISA kit, Cat No. 1000; Alpha Diagnostics Inc). In principle, the ELISA kit was based on simultaneous binding of human ferritin and human CRP from samples to 2 antibodies, one immobilized on microtiter well plates and the other conjugated to the enzyme horseradish peroxidase. The enzymatic reaction (color development) was directly proportional to the amount of ferritin or CRP present in a sample. Malaria parasitemia was assessed from the participants’ blood samples using Giemsa staining technique. 21 Soil-transmitted helminthes were identified in stool samples using the Standard Kato-Katz technique. 21 The stool and blood examinations were carried out by a parasitologist at the Department of Parasitology, NMIMR. The children with malaria parasitemia were referred by the medical officer in the study team to the government municipal hospital for treatment. Just after collection of stool samples, all children in the school were given the anti-helminthic drug albendazole, an initiative of Ghana Education Service. That exercise was delayed for the baseline stool samples to be collected from the children. Dietary data were collected on 3 nonconsecutive days using the 24-hour recall method and a food frequency questionnaire. 22,23
Intervention Phase
Randomization
The participants were randomly assigned to 3 groups: fish meal with vitamin group (n = 50) given cowpea-based food containing 3% fish powder served with 33 mg vitamin C/100 mL of vitamin C–rich drink, vitamin group (n = 50) given cowpea-based food served with 33 mg vitamin C/100 mL of vitamin C–rich drink, and a control group (n = 50) that received cowpea-based food plus placebo drink.
Proximate Composition of Study Diets
The proximate composition of the diet of the fish meal–vitamin C group (as was eaten) was protein 21.1 g/100 g, fat 4.5 g/100 g, and iron 5.4 mg/100 g in addition to vitamin C 33 mg/100 mL of vitamin C–rich drink. The diets provided for the vitamin C group and the control group (as were eaten) had basically the same proximate composition, that is, protein 18.4 g/100 g, fat 4.3 g/100 g, and iron 4.1 mg/100 g.
Meals Preparation
The study diets were prepared in 3 separate kitchens, each of which was supervised by a trained field assistant. Equal amount of cleaned dry cowpea (11 kg) was washed with water 3 times and added to boiling water in each of 3 aluminum pots and cooked to softness. To each pot of cowpea was added powdered pepper (13 g), onion paste (30 g), red palm oil locally called “zoomi” (400 g), and salt (40 g) to taste. In addition, 3% fish powder (which is equivalent to 330 g of dry cowpea used) was added to one of the pots (diet for fish meal with vitamin C group) with its recipe. Each study participant was served 250 g of cowpea-based food otherwise called beans stew plus 20 g of “gari” (roasted fermented cassava dough) locally termed “aborboe” and served 200 mL drink (vitamin C–rich drink or placebo drink) depending on his or her group. For a daily serving of cowpea-based food containing 3% fish meal served with vitamin-rich drink, each participant received 52.7 g of protein, 13.5 mg of iron, and 66 mg of vitamin C. Those provided with cowpea-based food served with vitamin C–rich drink received 46.0 g of protein, 10.2 mg of iron, and 66 mg of vitamin C. Each participant in the control group had a daily intake of 46.0 g of protein, 10.2 mg of iron, and no vitamin C. The food was provided during school lunch for 3 consecutive weekdays for a period of 6 months. For easy identification of participants in the 3 intervention groups, color button was fixed on each participant’s school shirt pocket. Green, yellow, and red color buttons were given to the fish meal–vitamin C, vitamin C, and control groups, respectively. The purpose was to provide each participant with the right food always and to prevent trading of the foods by participants. The teachers and field assistants supervised participants during mealtime.
End line Data Collection
One hundred and forty-two participants completed the study and provided blood and stool samples at end line. Blood and stool samples were collected from each participant in the field and transported on ice to NMIMR and processed using the same procedures as was done at baseline. The participant’s dietary intake, weight and height measurements, hemoglobin, and serum ferritin concentrations were determined in addition to malaria parasitemia and soil-transmitted helminthes according to the standard procedures used at the baseline.
Data Analysis
Data for 142 participants, fish meal–vitamin C group (n = 50), vitamin C group (n = 43), and control (n = 49), from baseline to end line were entered into the computer using Microsoft Excel 2007. After cleaning the data, they were exported to SPSS (version 16.0) for Windows and analyzed. The age-specific cutoff values for hemoglobin concentrations used to define anemia were 115 g/L for those aged 6 to 11 years and 120 g/L for those aged 12 years. 24 Low iron stores were defined as ferritin concentration <15 ng/mL (when infection and inflammation are not considered) and <30 ng/mL due to high prevalence of infection (malaria parasitemia) 25 and the high CRP concentrations (>10 ng/mL) among the study participants. Dietary data were used to estimate the amount of nutrients consumed using ESHA FPRO Software Version 6.5 and the Ghana Food Composition Table. 26 Variables were checked for normality. Hemoglobin values were normally distributed, so their summary values are presented as arithmetic means ± standard deviations. Mean hemoglobin values were compared between groups using 1-way analysis of variance (ANOVA), and where there is significant difference in mean values among groups, post hoc Scheffé analysis was done to identify groups that are significantly different. Ferritin and dietary variables were skewed and were transformed to logarithms before performing statistical analyses. Geometric means with standard deviations are quoted for skewed data that were log transformed. The results for such data are presented in the tables using original units without any log transformation. Logistic regression analysis was done to determine the differences between groups in the prevalence of anemia, low iron stores, malaria parasitemia, and high CRP levels (<10 ng/mL). Statistical significance was set at P < .05.
Ethical Considerations
Ethical approval was obtained from the institutional review board of NMIMR, College of Health Sciences, University of Ghana, Legon. Permission was obtained from the District Directorate of Education, the local chief, elders, and the head teacher of the selected school. Written informed consent was also obtained from the parents/guardians of the pupils.
Results
Household Characteristics of the Study Groups
The study groups had similar household characteristics. Most (67%-71%) of the parents were subsistence farmers, with 55% to 70% of them having attained middle or junior high school education. Many of the households (66%-76%) consisted of 3 to 6 members.
Baseline Characteristics
The average age of the participants in each of the 3 intervention groups ranged between 9.1 and 9.3 years. The sexes were evenly distributed across the 3 groups. The mean weight, height, and body-mass-index-for-age Z scores were nonsignificant among the groups (Table 1).
Baseline Characteristics of the Children by Study Group.a
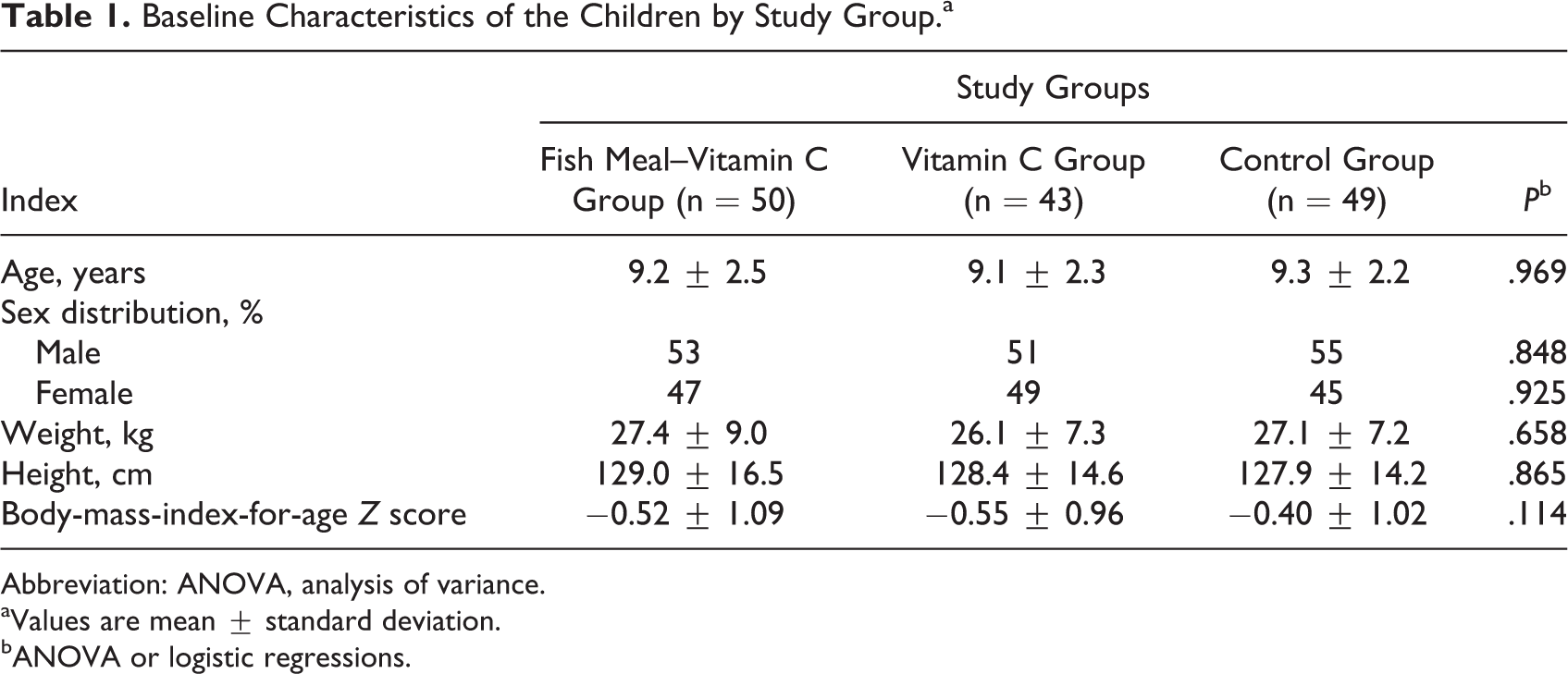
Abbreviation: ANOVA, analysis of variance.
aValues are mean ± standard deviation.
bANOVA or logistic regressions.
Dietary Intake
The results demonstrated that fish meal–vitamin C, vitamin C, and control diet provided on average 13.3, 12.7, and 12.9 mg of iron, respectively, to the total dietary iron intake (Table 2). Also, the fish meal–vitamin C, vitamin C, and control diet contributed mean protein intake of 34.4, 21.0, and 21.1 g to the total protein intake of the study participants, respectively. Both fish meal–vitamin C and vitamin C diets contributed 66 mg of vitamin C to the total dietary vitamin C intake. Dietary data captured showed that all the participants had nutrient adequacy ratio (NAR) > 1 for iron and protein based on the 24-hour recall method. The findings on the weekly consumption pattern of various food groups among children across the 3 study groups indicated that most of them scarcely ate fruits, fats, oils, and dairy products on a weekly basis. However, all the study participants consumed cereal-based food besides fish at least 3 times in a week. The children also consumed roots and tubers, legumes and nuts, and vegetables at least once a week. There was no difference in the food sources of the participants among the study groups.
Estimates of Dietary Intake of Protein, Iron, and Vitamin C by the Children of Study Group.a
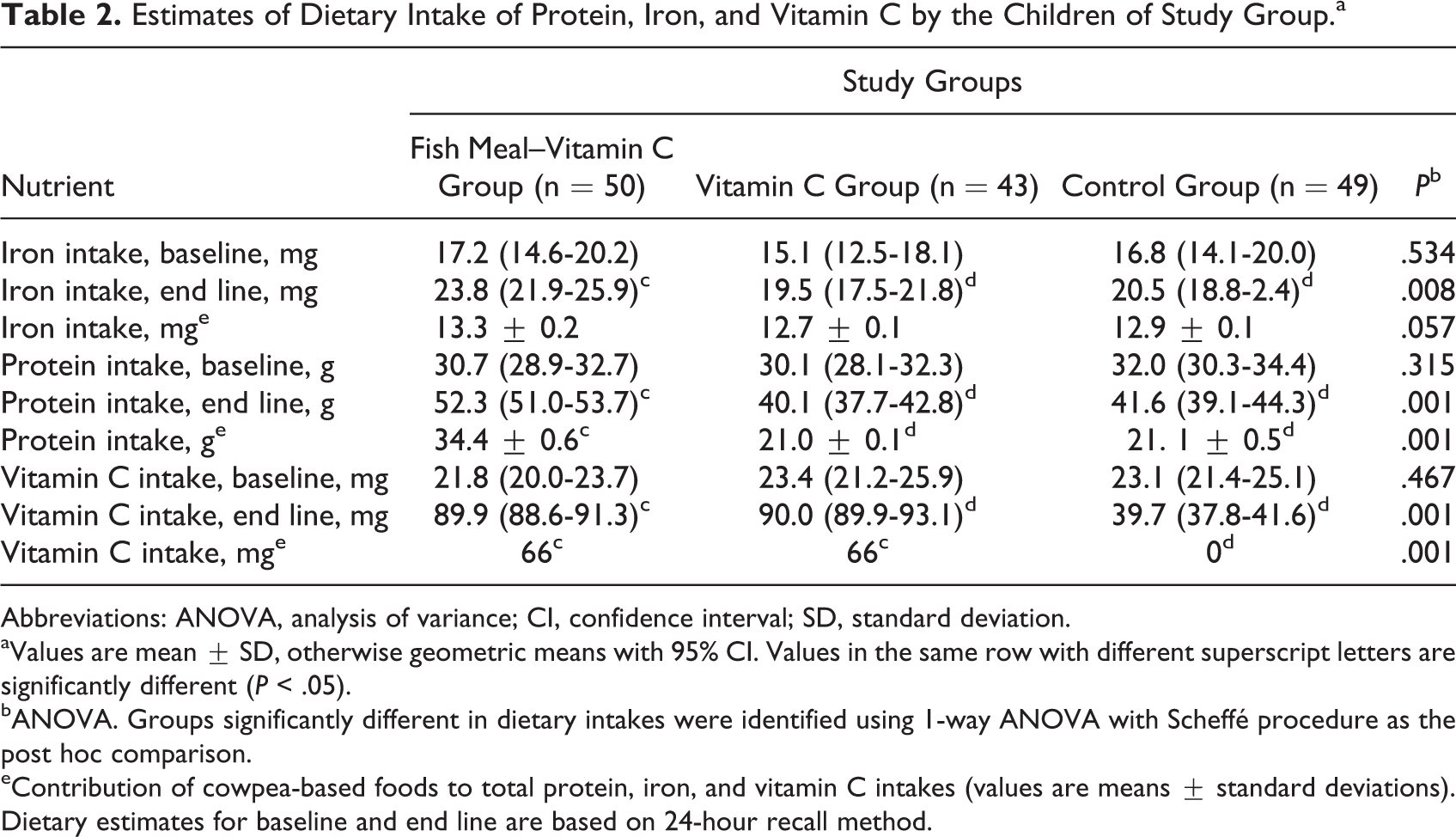
Abbreviations: ANOVA, analysis of variance; CI, confidence interval; SD, standard deviation.
aValues are mean ± SD, otherwise geometric means with 95% CI. Values in the same row with different superscript letters are significantly different (P < .05).
bANOVA. Groups significantly different in dietary intakes were identified using 1-way ANOVA with Scheffé procedure as the post hoc comparison.
eContribution of cowpea-based foods to total protein, iron, and vitamin C intakes (values are means ± standard deviations). Dietary estimates for baseline and end line are based on 24-hour recall method.
Iron Status Indicators
There were no significant differences in hemoglobin concentrations and iron stores among the study groups at baseline as shown in Table 3. The mean iron stores increased for the 3 study groups from baseline to end line. The mean (with 95% confidence interval) ferritin concentrations representing iron stores at end line were 27.2 (22.9-32.2), 23.4 (19.5-28.0), and 23.0 (19.4-27.3) ng/mL for fish meal–vitamin C, vitamin C, and the control group, respectively. The change in iron stores within the fish meal–vitamin C group, 6.5 (4.7-8.6), was different, P = .001. However, the change in iron stores was not different between the groups (P > .05). The mean hemoglobin concentrations also increased for each study group at end line compared to baseline. The mean hemoglobin concentrations at end line were 128.4 ± 7.2, 126.4 ± 8.9, and 123.1 ± 6.6 g/L for fish meal–vitamin C, vitamin C, and control groups, respectively. The changes in hemoglobin concentrations were different for fish meal–vitamin C group (8.3 ± 10.6) and the control (4.2 ± 10.4), P < .05. There were no significant differences in the prevalence of low iron stores (Table 4), between the groups at baseline and end line. As a result, the changes in prevalence of low iron stores were also nonsignificant among the groups (Table 4). At end line, the prevalence of anemia reduced in fish meal–vitamin C, vitamin C, and control groups to 3.9%, 25.7%, and 18.4%, (Table 4), compared to the baseline values of 23.5%, 35.0%, and 30.6%, respectively (Table 4).
Iron Status Indices of the Children by Study Group.a
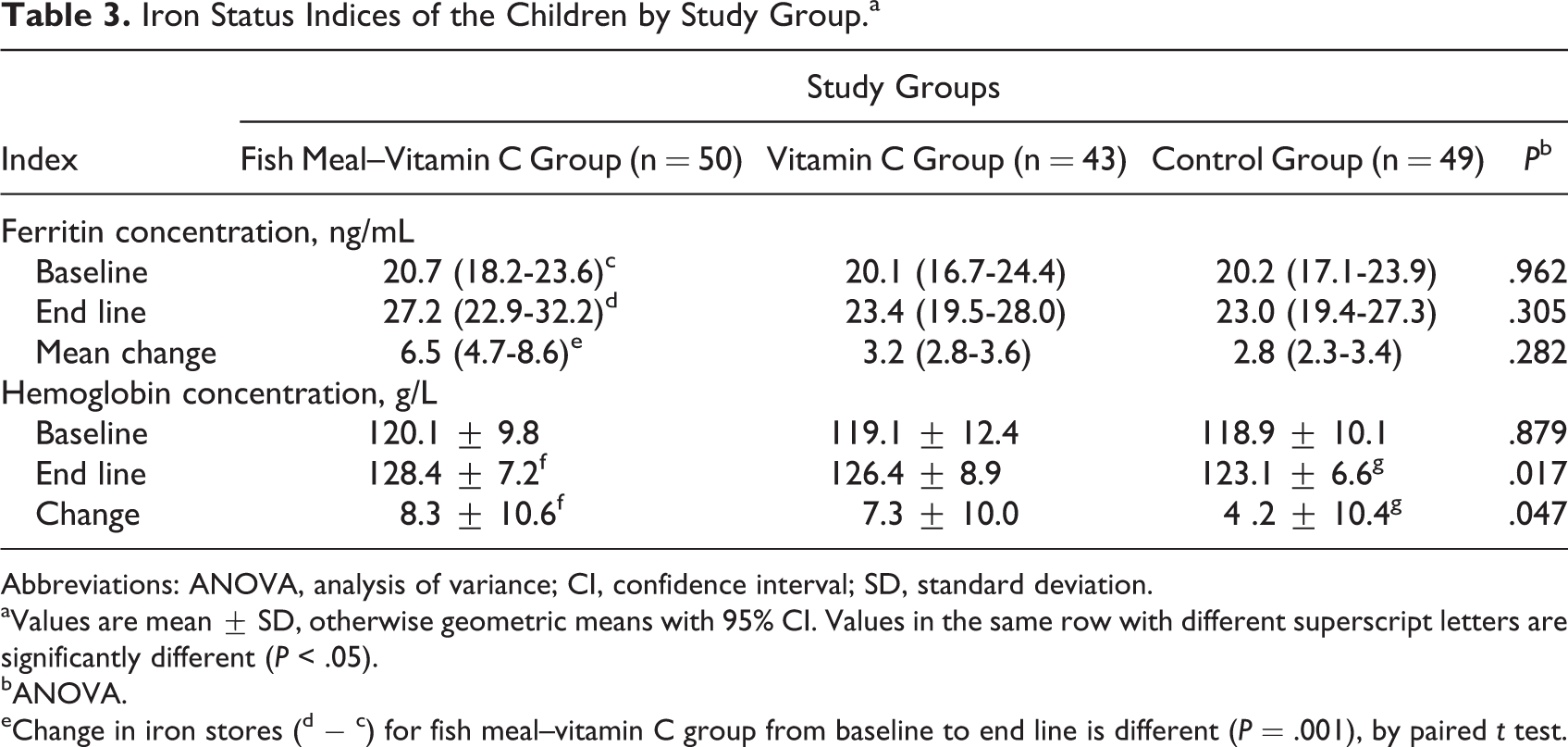
Abbreviations: ANOVA, analysis of variance; CI, confidence interval; SD, standard deviation.
aValues are mean ± SD, otherwise geometric means with 95% CI. Values in the same row with different superscript letters are significantly different (P < .05).
bANOVA.
eChange in iron stores (d − c) for fish meal–vitamin C group from baseline to end line is different (P = .001), by paired t test.
Prevalence of Low Iron Stores and Anemia Among the Children by Study Group.a
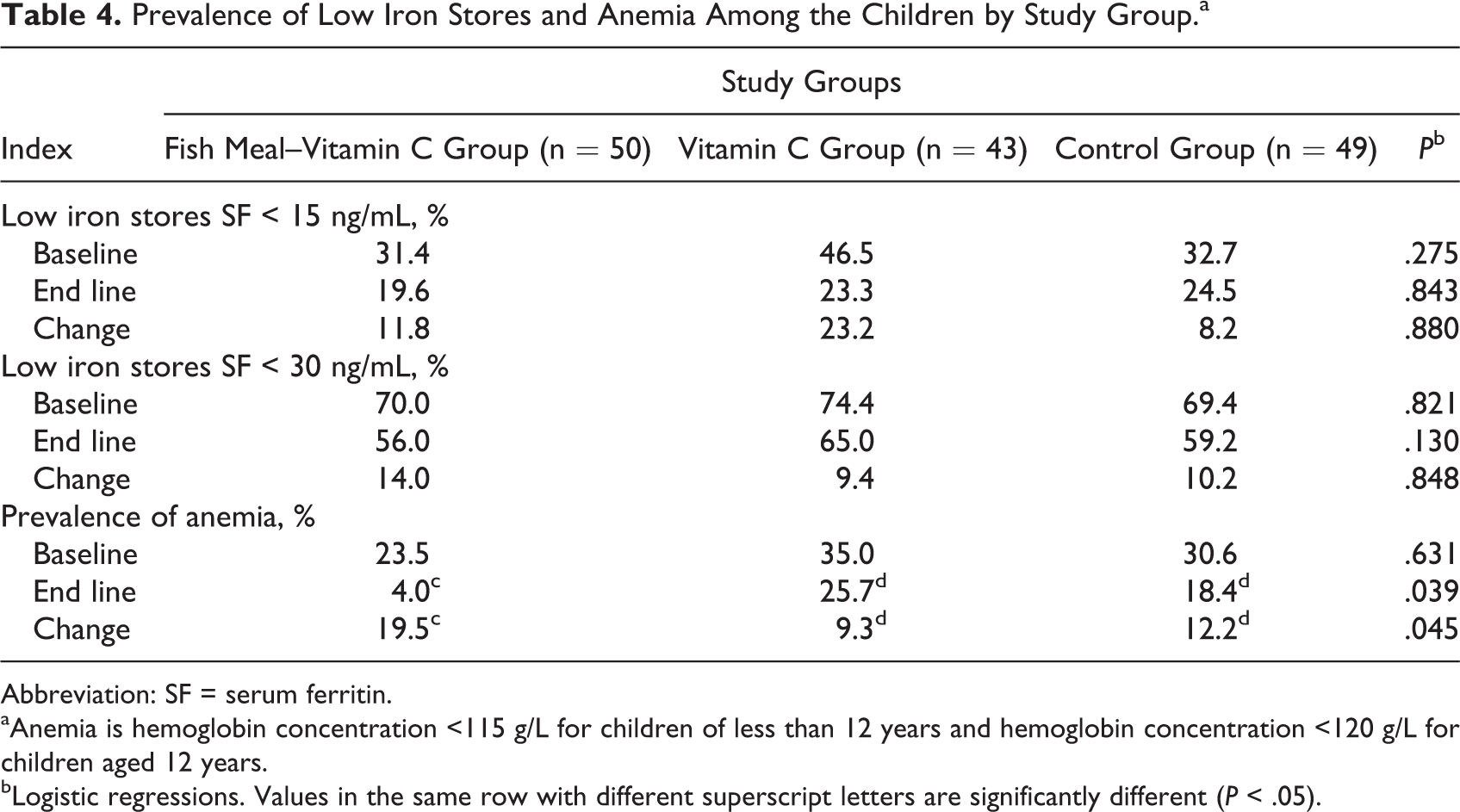
Abbreviation: SF = serum ferritin.
aAnemia is hemoglobin concentration <115 g/L for children of less than 12 years and hemoglobin concentration <120 g/L for children aged 12 years.
bLogistic regressions. Values in the same row with different superscript letters are significantly different (P < .05).
Morbidity Indicators
The prevalence of malaria parasitemia was in the range of 58.0% to 80.0% among the study participants. This was not significant between the groups (Table 5). On average, the prevalence of high CRP > 10 ng/mL was 55%, 77%, and 68% in the fish meal–vitamin C, vitamin C, and control groups, respectively (Table 5). There was moderate decline in prevalence of malaria parasitemia among the 3 study groups, at the end of the study. The prevalence of malaria parasitemia were 62.7%, 58.1%, and 69.4% for fish meal–vitamin C, vitamin C, and control groups, respectively, but this was not significant between the groups (Table 5). The prevalence of high CRP remained the same as at the baseline for the fish meal–vitamin C group, decreased slightly in vitamin C group (79%), and increased in the control group (69%) at end line.
Prevalence of Inflammation Indicators Among the Children by Study Group.
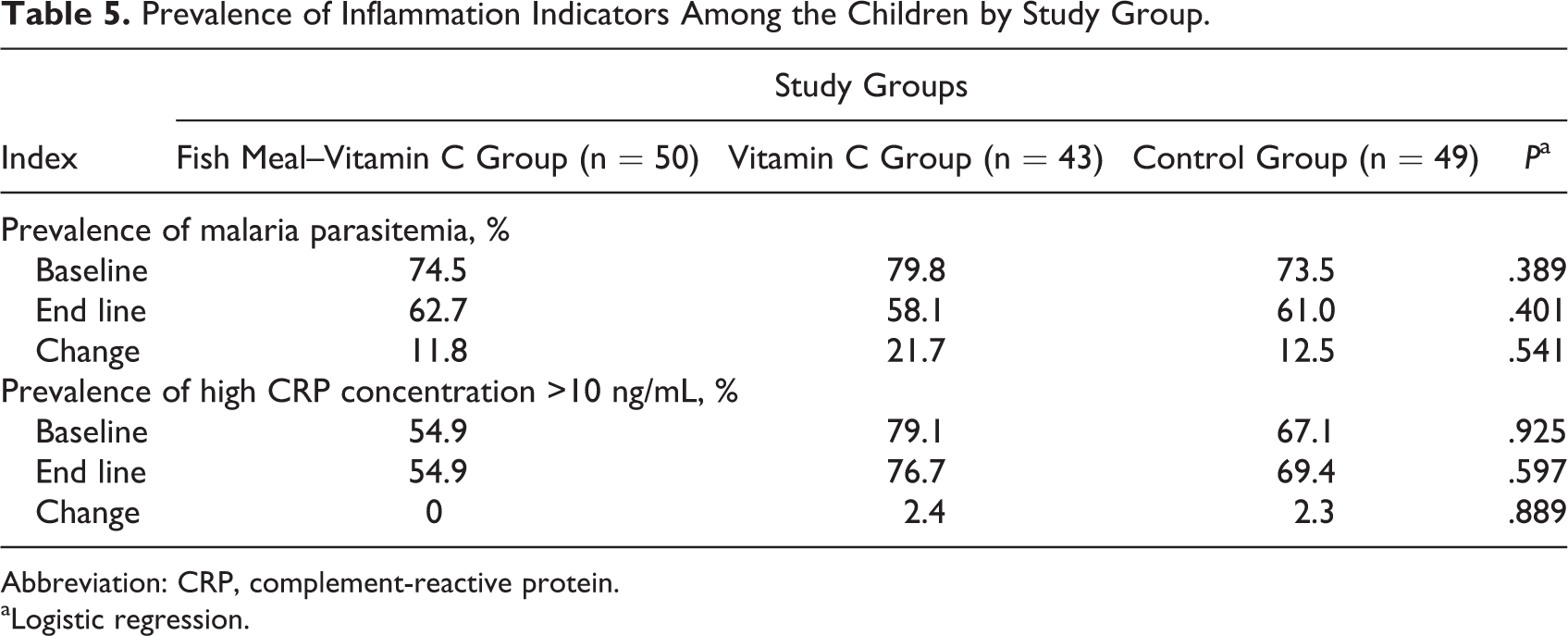
Abbreviation: CRP, complement-reactive protein.
aLogistic regression.
Discussion
To our knowledge, the present study is the first of its kind to investigate the combined effect of fish meal and vitamin C on the iron stores and hemoglobin concentration of school-aged children who consumed cowpea-based food thrice a week in a school feeding program in a malaria endemic area in Ghana. The findings show that it is possible to improve the hemoglobin concentration of the study participants significantly and also minimize anemia prevalence among them using cowpea-based food containing 3% fish meal served with vitamin C–rich drink (which contains 66 mg vitamin C per 200 mL). Within each of the study groups, there was difference in hemoglobin concentration from baseline to end line. The change in hemoglobin concentrations between fish meal–vitamin C and vitamin C groups was not different but that between fish meal–vitamin C group and the control was different (P < .05). The findings show that mean ferritin concentration (iron stores) improved significantly within the fish meal–vitamin C group from baseline to end line. However, the change in iron stores between the 3 groups was not different (P > .05). The change (reduction) in the prevalence of anemia was different between fish meal–vitamin C, vitamin C, and control groups. The results of the present study demonstrated that the consumption of cowpea-based food that contained fishmeal and was served with vitamin C-rich drink is likely a potential diet for controlling anemia among the participants.
The prevalence rate of anemia among the study groups in the current study at baseline is below the values reported elsewhere for Ghanaian school-aged children. 10,11,12 In the current study, the level of anemia at baseline (30.1%) is above the global prevalence (25%) reported among schoolchildren worldwide, however, 9 which is a troubling factor for these authors. This level of anemia is in agreement with the findings of Milman 27 that anemia is a major public health problem globally, especially in developing countries. Nevertheless, it is important to state that the study participants (aged 6-12 years) had mild to moderate anemia with hemoglobin concentrations between 90 and 115 g/L. Since hemoglobin levels increased and anemia prevalence declined within all the study groups, the role of other nutrients could not be ruled out. However, the increase in hemoglobin concentration with greater reduction in prevalence of anemia observed for the fish meal–vitamin C group would likely be attributed in part to the heme iron content of the diet in addition to bioavailability of nonheme iron in the presence of fish meal and vitamin C. Meat (or fish) and vitamin C are known enhancers of nonheme iron bioavailability. Our findings confirm the suggestions by an earlier study that mere addition of iron to staple foods in developing countries, without providing enhancers of iron absorption, is unlikely to have significant effect on iron status. 15
The sources of food for the study participants as indicated by results of the 24-hour recall and food frequency questionnaire were staple diets made from cereals, roots, and legumes. Diets prepared from cereals, roots, and tubers with negligible amounts of nonheme iron enhancers may be characterized as very low (5%) iron bioavailable diets. 18 Children’s habitual consumption of cereals and legumes as staples might put them at high risk of iron deficiency as was suggested by Zimmermann et al. 15 Zimmermann et al 15 suggested that low iron bioavailability from legumes and cereal-based diets could be the cause of iron deficiency in children in rural Africa. All the children had NAR >1.0 for dietary iron intake both at baseline and at end line. The intervention and control diets contributed at least half of the total dietary iron intake. No significant difference was established among the groups for the contribution of the intervention diets to total dietary iron intake. In view of this, it is suggested that the fish meal mainly served as an enhancer in addition to the vitamin C–rich drink for innate nonheme iron bioavailability in the diet.
The findings indicated the prevalence of malaria parasitemia and high CRP levels among the participants both at baseline and at end line was of public health significance. Serum ferritin (storage iron) is an acute phase protein whose levels increase with prevalence of infection, in the presence of inflammation, or both. In view of this, it has been suggested that biochemical markers of iron status would be likely unreliable in tropical countries with prevailing conditions of infection and inflammation. 25,28 Hence, it is suggested that potential misclassification is the main concern regarding the use of serum ferritin concentration in diagnosis of ID in tropical countries: children who are iron deficient may be categorized as iron replete if their ferritin levels are falsely high due to concomitant malaria, inflammation, or both.
In order to control the influence of infection and inflammation in the current study, as the results indicated high prevalence of malaria parasitemia (in the range of 58%-80%) and high CRP > 10 ng/mL (55%-79.0%), we used serum ferritin cutoff value of <30 ng/mL as was done in other studies 25,29,30 to report the prevalence of low iron stores (iron deficiency) among children in addition to the normal ferritin cutoff value of <15 ng/mL. At normal ferritin cutoff value (<15 ng/mL), we would underestimate the prevalence of low iron stores among the 3 study groups. Nevertheless, at a cutoff value <30 ng/mL, we would also probably overestimate the prevalence of low iron stores. For any studies like ours, among participants with high level of infection and inflammation indicators, it is suggested that prevalence of low iron stores should be stated as estimates. Based on ferritin concentration <30 ng/mL, our results indicated that estimate of change (reduction) in prevalence of low iron stores was greater within the fish meal–vitamin C group compared to the vitamin C and control groups. However, the reduction in prevalence of low iron stores was not different between the groups.
Strengths and Limitations
This study is the first nutrition intervention study in the Adaklu Anyigbe district involving its pupils (aged 6-12 years). The study included biochemical, anthropometric, and dietary assessment of nutritional status as well as screening for infection and inflammation among older pupils. A few limitations of the current study deserve acknowledgment. The study participants were only pupils (aged 6-12 years) from public school not benefiting from the GSFP.
The study results, therefore, cannot be generalized to out-of-schoolchildren or those who were not benefitting from the GSFP. Secondly the use of 24-hour recall method and food frequency questionnaires for nutrient intake assessment probably would influence the actual nutrient intake outside the intervention program. These procedures (though identified as weakness) were appropriate to capture nutrient intake outside the feeding program. Nutrient intakes from the intervention meals were captured by direct weighing of daily servings and leftovers. Due to the prevalence of malaria parasitemia and high CRP levels among participants, the cutoff point for serum ferritin was raised to 30 ng/mL, instead of the normal 12 or 15 ng/mL. This was to cater the influence of infection and inflammation that would cause elevated ferritin levels.
Conclusion
The consumption of cowpea-based food containing 3% fish meal served with vitamin C–rich drink for 6 months by Ghanaian schoolchildren was shown, in this trial, to control the prevalence of anemia when compared to the drink alone or no dietary intervention. It also improved the hemoglobin concentration compared to the control situation. Hence, cowpea-based food containing fish meal and served with vitamin C–rich drink has the potential as a public health measure to reduce anemia in this population.
Footnotes
Authors’ Note
Godfred Egbi was responsible for data collection, statistical analysis, data presentation, drafting, and review of the article. Irene Ayi was responsible for data collection, data presentation, and review of the article. Firibu Kwesi Saalia was responsible for data collection, data presentation, statistical analysis, and review of the article. Francis Zotor was responsible for data presentation, drafting, and review of the article. Theodosia Adom was responsible for data presentation and review of the article. Eric Harrison was responsible for data presentation and review of the article. Collins Ahorlu was responsible for data presentation and review of the article. Matilda Steiner-Asiedu was responsible for data collection, data presentation, statistical analysis, and review of the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Nestle Foundation, the College of Health Sciences at the University of Ghana, Legon, and African Doctoral Dissertation Research Fellowship award offered by the African Population and Health Research Center (APHRC) in partnership with the International Development Research Centre (IDRC).