
Abstract
Background:
In Latin America and the Caribbean, anemia has been a public health problem that affects mainly women of childbearing age and children under 6 years of age. However, the current prevalence of anemia in this region is unknown.
Objective:
To examine the latest available prevalence data on anemia in Latin America and the Caribbean.
Methods:
A systematic review was conducted in 2011 and updated in 2014. Studies determining the prevalence of anemia conducted in apparently healthy populations with national or regional representativeness were included in the review.
Results:
The lowest prevalence rates of anemia among children under 6 years of age were found in Chile (4.0%), Costa Rica (4.0%), Argentina (7.6%), and Mexico (19.9%). In Nicaragua, Brazil, Ecuador, El Panama, and Honduras, anemia was a moderate public health problem, with prevalence ranging Salvador, Cuba, Colombia, the Dominican Republic, Peru, from 20.1% to 37.3%. Anemia was a severe public health problem in Guatemala, Haiti, and Bolivia. The prevalence of anemia among women of childbearing age was lowest in Chile (5.1%). In Colombia, El Salvador, Costa Rica, Nicaragua, Ecuador, Mexico, Peru, Honduras, and Argentina, anemia was a mild public health problem, with prevalence ranging from 7.6% to 18.7%. In Guatemala, Brazil, the Dominican Republic, and Bolivia, anemia was a moderate public health problem, with prevalence ranging from 21.4% to 38.3%. Panama and Haiti had the highest reported prevalence rates (40.0% and 45.5%, respectively), and anemia was considered a severe public health problem in those countries.
Conclusions:
Anemia remains a public health problem in children under 6 years of age and women of childbearing age in most Latin America and Caribbean countries for which data are available.
Introduction
Anemia is a global health problem characterized by a reduction in the number of red blood cells and the oxygen-carrying capacity of hemoglobin. The World Health Organization (WHO) estimates that half of all anemia cases are caused by iron deficiency. Thus, this article will focus mainly on anemia due to iron deficiency, since deficiencies of other anemia-associated micronutrients, such as folate and vitamin B12, do not contribute substantially to this condition. Iron deficiency affects millions of individuals throughout the life cycle, especially infants and pregnant women, but also including young children, adolescents, and women of childbearing age. 1,2 This deficiency usually occurs when the intake of bioavailable iron is insufficient for a prolonged period of time. Consequences include compromised neurological development of children, increased maternal and infant mortality, and a reduction in physical work capacity in adulthood. 2–4 Anemia can also commonly be caused by physical pathologies, including acute and chronic inflammation and hematological disorders. 5–7 It is well known that infectious diseases, such as malaria, can also increase the prevalence of anemia in vulnerable populations. 1,4 Several strategies have been implemented to prevent and control anemia in Latin America and the Caribbean, most notably mass fortification of flour (wheat, rice, maize, or cassava) and milk with iron. 4,8–10
According to the WHO 1993–2005 estimation of the worldwide prevalence of anemia, one-fourth of the total population (24.8%; 95% CI, 22.9% to 26.7%) has this disease; the prevalence reaches 47.4% (95% CI, 45.7% to 49.1%) in preschoolers and 30.2% (95% CI, 28.7% to 31.6%) in nonpregnant women. 2,11 The aim of this systematic review is to examine the latest available data on the prevalence of anemia in Latin American and Caribbean countries.
Methods
A systematic review was conducted between July and August 2011 and subsequently updated in December 2014 to identify the latest available data on anemia in apparently healthy children under 6 years of age and women of childbearing age since 2000. PubMed, LILACS, and SciELO were used to identify studies by combining the terms “anemia,” “iron,” and “prevalence” with the name of each Latin America and Caribbean country. National Health Surveys generated by ministries of health were also identified by visiting their websites. National Health Surveys and national or regional representative studies, as well as local studies (small commune, district, province, or location) were included. Studies were not excluded on the basis of language. A sample size of at least 100 subjects per study was considered a minimum entry criterion for the review. Anemia was defined by the WHO, 12 and adjustment by altitude was considered when available. The only data in which anemia was classified by the Centers for Disease Control and Prevention (CDC) criteria were from women from Guatemala and El Salvador. 13 The confidence interval for each prevalence rate was calculated based on the reported sample sizes. The categories of public health significance of anemia were defined according to WHO recommendations as follows: prevalence ≤ 4.9%, not a public health problem; prevalence 5% to 19.9%, mild public health problem; prevalence 20% to 39.9%, moderate public health problem; prevalence ≥ 40%, severe public health problem. 2 Figures were plotted using R programming language, version 3.1.0. 14
Results
A total of 1,316 studies were identified. Of these, 308 were excluded due to duplication. After review of the titles and abstracts, a further 750 were excluded because the information was not relevant to the purpose of our review. Of the 273 preselected studies, we excluded 252 because they did not meet the selection criteria. In the end, 15 National Health Surveys were included: Argentina 2007, Bolivia 2008, Brazil 2006, Chile 2003, Colombia 2010, Costa Rica 2009, the Dominican Republic 2009, Ecuador 2012, El Salvador 2008, Guatemala 2009, Haiti 2005–2006, Honduras 2005, Mexico 2006, Nicaragua 2003–2005, and Panama 2000. Six studies with national or regional representativeness conducted on children from Chile (two regional studies in 2012 and 2013), Costa Rica (national study in 2009), Cuba (regional study in 2011), and Mexico (national study in 2007) were also included (Figure 1).
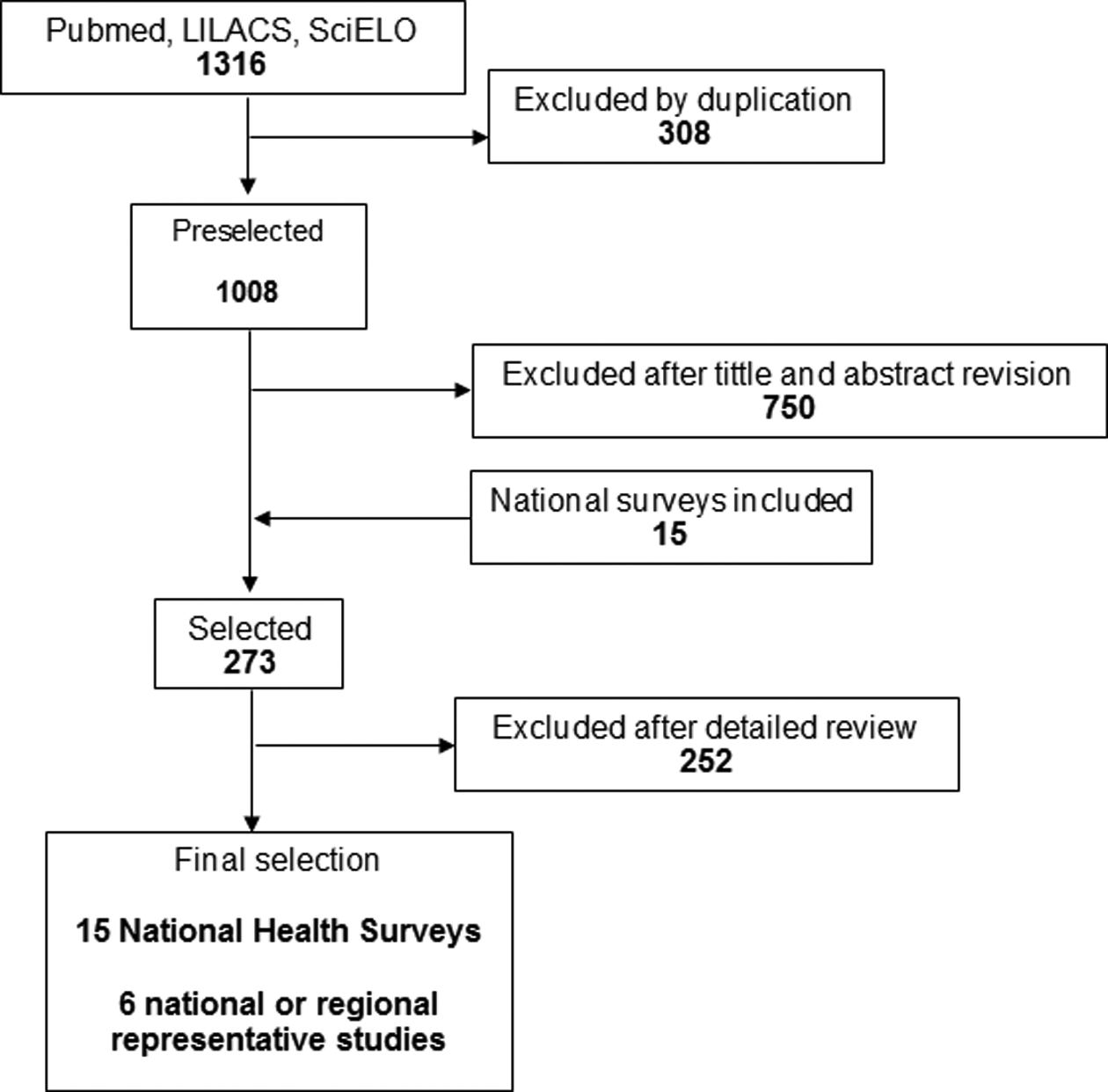
Flow diagram of selected studies.
Prevalence of Anemia in Children Under 6 Years of Age
Among children 19 to 72 months of age, the lowest prevalence of anemia (4%) was found in Chile 15 and Costa Rica. 16 Among younger children, low prevalence was reported from Chile (12 to 18 months, 14%), 17 Argentina (12 to 18 months,16.5%), 18 and Mexico (< 2 years, 19.9%). 19 Anemia was a moderate public health problem among children in Nicaragua, 20 Brazil, 21 Mexico (12 to 59 months), 22 Ecuador, 23 El Salvador, 24 Cuba, 25 Colombia, 26 the Dominican Republic, 4 Peru, 27 Panama, 28 and Honduras, 29 with rates ranging from 20.1% to 37.3%. Guatemala, 30 Haiti, 4 and Bolivia 31 had the highest prevalence rates among children, ranging from 47.7% to 61.3%, indicating a severe public health problem (Figure 2).
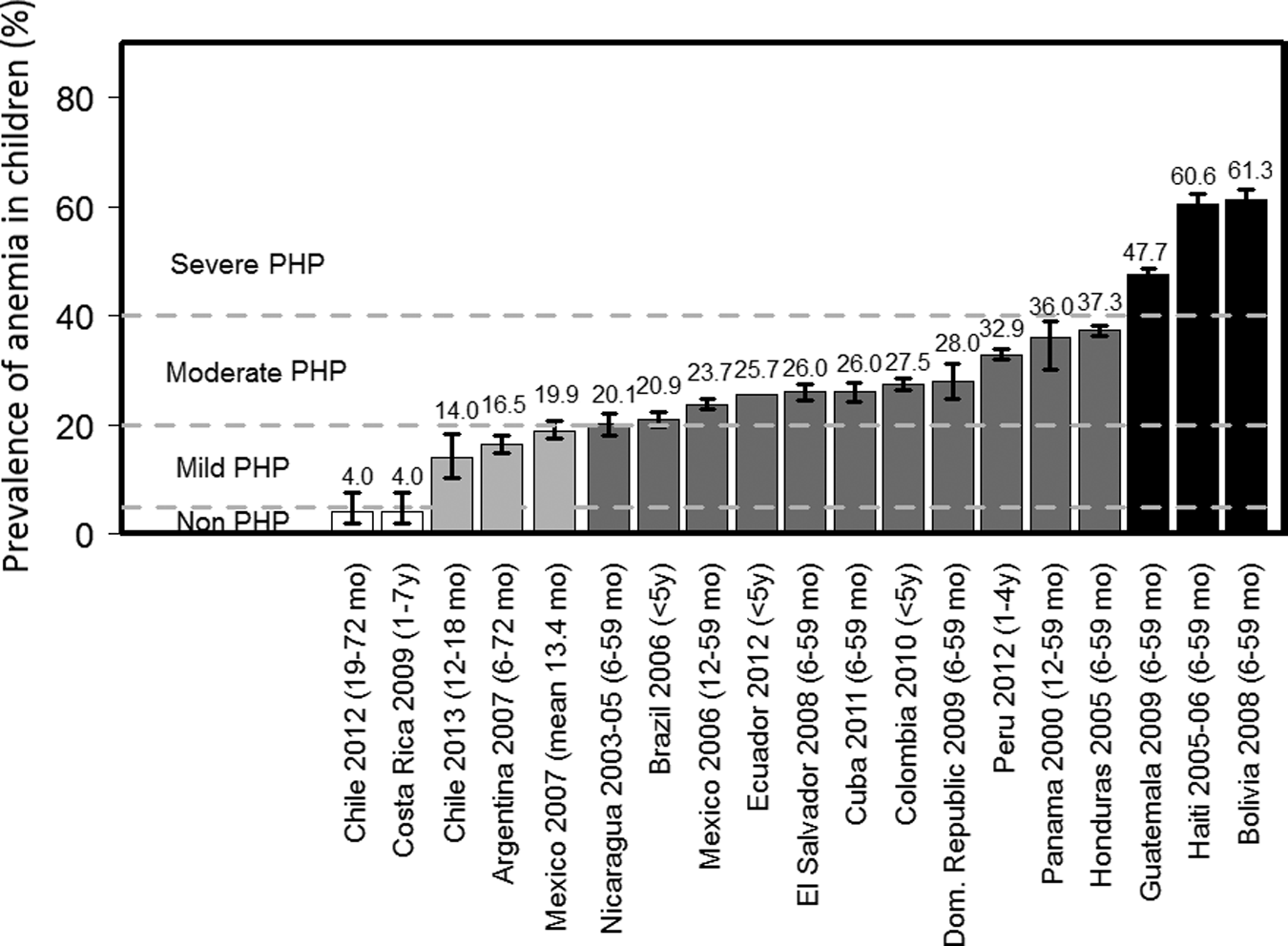
Prevalence of anemia in Latin American and Caribbean children under 6 years of age. The gradient in each bar from white to black represents increasing severity of the public health problem (PHP).
Prevalence of Anemia in Women of Childbearing Age
Chile had the lowest prevalence of anemia in the region among women of childbearing age (5.1%). 32 In Colombia, 26 El Salvador, 24 Costa Rica, 16 Nicaragua, 20 Ecuador, 23 Mexico, 22 Peru, 27 Honduras, 29 and Argentina, 18 anemia in this population was a mild public health problem, with prevalence ranging from 7.6% to 18.7%. In Guatemala, 30 Brazil, 21 the Dominican Republic, 4 and Bolivia, 31 anemia was a moderate public health problem, with prevalence ranging from 21.4% to 38.3%. Panama 28 and Haiti 4 had the highest prevalence rates of anemia among women of childbearing age (40.0% and 45.5%, respectively) (Figure 3).
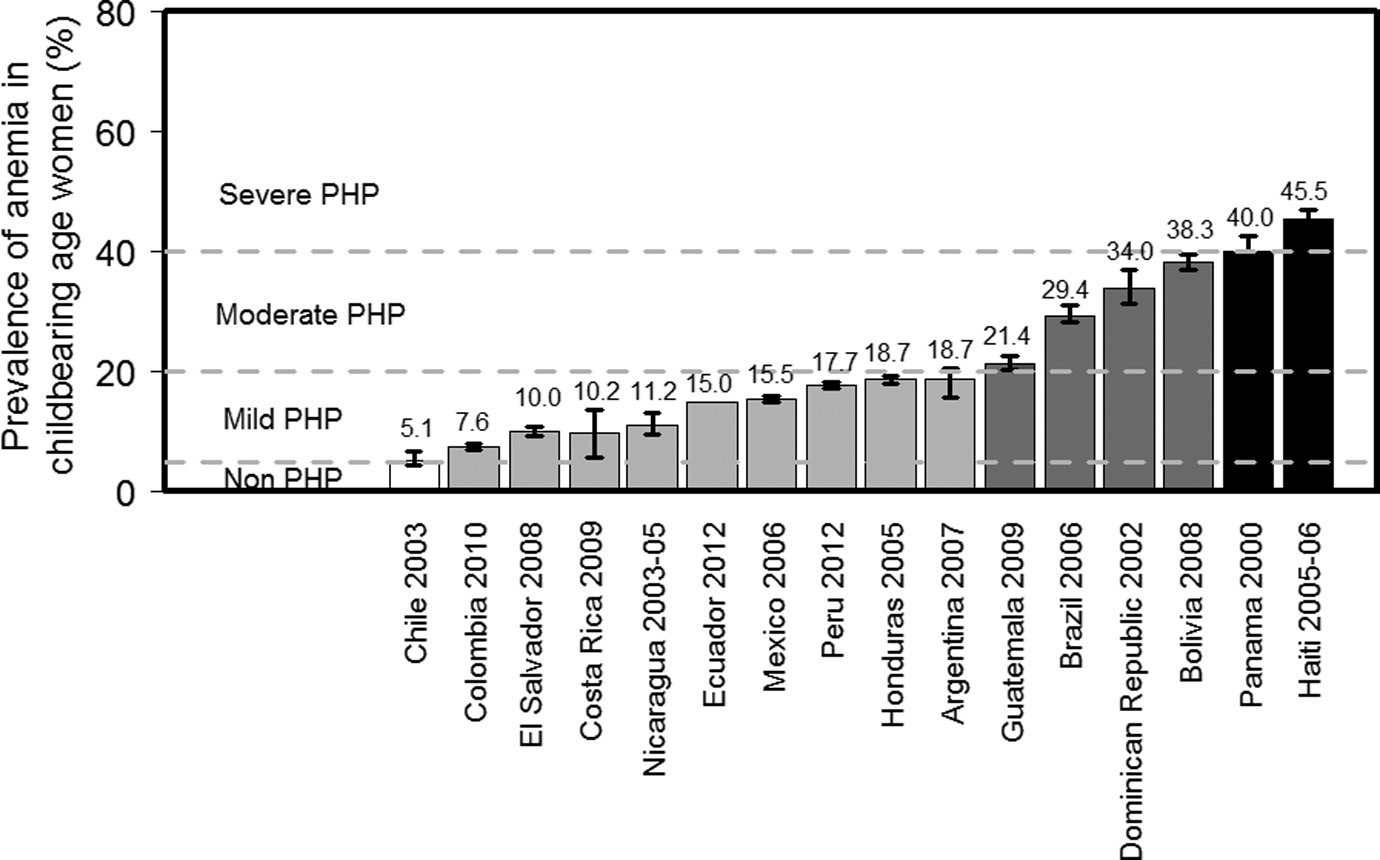
Prevalence of anemia in Latin American and Caribbean women of childbearing age. The gradient in each bar from white to black represents increasing severity of the public health problem (PHP).
Discussion
We examined the latest representative data on the prevalence of anemia in Latin America and the Caribbean. The prevalence ranged from 4.0% to 61.3% in children under 6 years of age and from 5.1% to 45.5% in women of childbearing age. Few data were available from the Caribbean. In most countries, anemia was classified as a mild or moderate public health problem for both children under 6 years of age and women of childbearing age, but there were countries where anemia was still a severe public health problem.
Anemia can result from many conditions, including acute or chronic inflammation, infectious disease, and hematological disorders, as well as insufficient intake of iron, folate, or vitamin B12. 1,2,4 For the purposes of this review, we will focus on the nutritional aspect of this condition and discuss the interventions, specifically including iron supplementation and fortification, that are being implemented in an effort to alleviate anemia caused by iron deficiency.
Chile and Costa Rica had the lowest prevalence of anemia in children under 6 years of age and 1 to 7 years of age, respectively. 15,16 In Chile, the low prevalence of anemia is very likely a consequence of the commonly consumed iron-fortified milks provided by the National Complementary Feeding Program. 33 This program delivers powdered whole cow’s milk (26% fat) fortified with iron, zinc, copper, and ascorbic acid to children who have been spontaneously weaned until they are 18 months of age. In addition, a fat-reduced version of the same milk (18% fat) is delivered to children 19 to 72 months of age. 15 As a potential indication of this program’s effectiveness, a recent study showed that beneficiaries of this program 11 to 18 months of age whose mothers admitted not giving them the fortified milk had twice the prevalence of anemia as beneficiaries who regularly consumed these products. 17
The low prevalence of anemia in Costa Rican children may be explained by the consumption of iron-fortified wheat flour (60 mg/kg), maize flour (22 mg/kg), and liquid and powdered milk. 4,16 Prior to iron fortification, national data from 1996 reported that the prevalence of anemia was 19.3% in this group. 16 However, a study in urban and rural Costa Rican children reported that the prevalence of anemia decreased by 10 percentage points between 1999 and 2008. 16 In addition, in 2001 and 2002, the bioavailability of iron from wheat flour and powdered milk was increased by replacing reduced iron with ferrous fumarate.
Chile also had the lowest prevalence of anemia among women of childbearing age. The fortification of wheat flour with 30 mg of iron per kilogram starting in 1950 was probably a major factor in ensuring an adequate intake of iron, 34,35 especially considering that the average daily intake of bread in this group is approximately 240 g of wheat flour. Argentina also had low rates of anemia (a mild public health problem) in both children under 6 years of age and women. 17 This country has also implemented supplementation with 12.5 mg of iron per day for children under 2 years of age. 4 Interestingly, although it was reported that only 20% of children received this supplement on a daily basis, the same survey indicated that approximately 80% of Argentinian children (6 to 23 months) had an adequate intake of iron. 17 This may be partially explained by the fact that since 2001, many Argentinian children under 2 years of age have received powdered milk fortified with 20 mg of iron per kilogram. 17 In addition, Argentina fortifies wheat flour with 30 mg of iron per kilogram, 4 which could explain the low prevalence of anemia in both children and adult women. Adult women are reported to consume an average of 200 g of wheat flour per day, which would provide a sufficient intake of iron. 36
In Mexico, the prevalence of anemia was relatively low in children under 6 years of age (19.9%). Mexico has a national program, PROGRESA, currently named “Oportunidades”. 37 This social and nutritional program provides a milk-based complementary food fortified with iron, zinc, and multiple vitamins to children aged 6 months to 2 years. The program has been shown to improve linear growth and reduce the prevalence of anemia in Mexican children. 37 Also potentially contributing to the low prevalence of anemia is the fortification of wheat and corn flours with iron (35 and 24 to 40 mg/kg, respectively). 4
Children under 6 years of age in Colombia, Ecuador, El Salvador, Honduras, Nicaragua, Panama, and Peru are beneficiaries of daily or weekly supplementation with 12.5 to 25 mg of iron. 4 El Salvador, Nicaragua, Honduras, and Panama fortify maize flour with approximately 22 mg iron/kg. 36 Since 2003, Cuban children 6 months to 3 years of age have received a fruit puree fortified with 2 mg of iron/100 g. Cuban children under 1 year of age also receive milk fortified with 10 mg of iron/1,000 mL. 25,38 In Panama, wheat flour is fortified with iron for an average consumption of 73 g of iron per day 36 ; women aged 15 to 49 years are provided a weekly supplement of 60 mg of iron plus 400 µg of folic acid for 16 weeks per year; and children are provided a daily supplement of 30 mg of iron for those under 2 years of age and 60 mg for those 2 years of age or older. 4 As confirmation of the effectiveness of iron fortification, a study conducted in Panamanian indigenous children showed a decrease in the prevalence of anemia from 47.3% to 19.4% after 6 months of delivery of maize cereals fortified with ferrous bisglycinate. 39 Despite these efforts, anemia in children under 6 years of age was classified as a moderate public health problem in these countries, possibly due to the low consumption of fortified foods and low coverage of supplementation programs. For example, the latest Colombian national survey indicated that only 32% of children over 6 months of age regularly consumed Bienestarina, a complementary food fortified with iron (14.1 mg/100 g) and multiple vitamins. 26,40 Coverage of iron supplementation programs has been reported as low in several countries. For example, in Peru, Honduras, and Ecuador, coverage for children under 6 years of age was only 12%, 28%, and 29%, respectively. 4 Although it was still insufficient, coverage of children between 24 and 59 months of age with iron supplementation was slightly higher in Panama (60%). 4
The highest prevalence of anemia in children under 6 years of age was reported in Guatemala, Haiti, and Bolivia, indicating a severe public health problem. 4,30,31 However, these countries do have programs in place that are attempting to address anemia due to micronutrient deficiencies. Bolivia and Guatemala have incorporated iron supplementation (12.5 to 25 g of iron/weekly) to children aged 6 to 59 months. However, the coverage was around 60% in Bolivia and approximately 20% in Guatemala. 4 The latest national Bolivian survey reported that only 45% of children consumed iron supplements. 31 In addition, vitamin and mineral sprinkles (Chispitas) fortified with 12.5 mg of iron per sachet and a complementary food (Nutribebe) fortified with 22 mg of iron per 100 g are delivered to Bolivian children aged 6 to 24 months. 4 In 2007, it was reported that the acceptability of Chispitas by children was 52%, 41 and it has been shown that only 58.1% of children receive this complementary food. 42 A study in Haitian children aged 9 to 24 months showed that the use of sprinkles reduced the prevalence of anemia from 54% to 24% after 2 months. 43 Despite the high prevalence of anemia in children and women, Haiti has not established a national intervention to reduce anemia.
As previously mentioned, the multiple causes for the lack of success of existing programs in Latin America and the Caribbean focusing on the control of anemia are low coverage rates and/or lack of monitoring, surveillance, and quality control of the existing programs. 4 WHO has suggested that it is relevant to consider an adequate delivery system for food fortification and supplementation. 12 Moreover, adherence to supplementation programs could be affected by secondary effects of supplementation such as epigastric pain and other gastrointestinal side effects. 12,44,45
It is likely that most of the anemia reported in Latin America and the Caribbean is due to iron deficiency. 1,4 The diet in most of these countries has a low amount of bioavailable iron (heme), which increases the difficulty of meeting the requirements. 1,2 In some countries, this situation coexists with high rates of gastrointestinal infections and parasitic diseases, which impair the absorption of iron. 46 For example, a recent study in Latin America reported a continuous decrease in the rate of malaria from 1959 to 2011. 47
Iron requirements increase due to growth during childhood and blood loss in women during menstruation, pregnancy, and childbirth, making children and women of childbearing age at higher risk for iron deficiency. 1–4 Iron-deficiency anemia is characterized by a deficient synthesis of hemoglobin in an advanced stage of iron deficiency, 48 but we cannot rule out that some of the reported anemia is due to other causes. Hemoglobinopathies can also be involved in iron deficiency, and other nutritional deficiencies have been related to anemia. Furthermore, vitamin A deficiency is considered the second most common cause of mild anemia, inducing iron sequestration and decreasing its mobilization for erythropoiesis. 49 In addition, studies indicate that deficiencies of vitamin B12, folate, and riboflavin can cause anemia. 50
Fortification and supplementation strategies focus on preventing anemia by providing adequate intakes of micronutrients associated with this condition. 1–3 Iron-specific interventions focus on the prevention of the main consequences of iron deficiency, such as physiological and immune system disorders, decrease in work productivity, impaired psychomotor development, increased incidence of preterm births, and low birthweight, as well as an increase in maternal and infant mortality, among other effects. 51–53 However, to effectively address the issue of anemia, it is important to consider the diversity of cultures and food habits, as well as improving dietary diversity, health care, sanitation levels, feeding practices, and parasitic disease control programs, among others. These actions may help reduce the prevalence of anemia.
Although we acknowledge that it is important to support national programs aimed at reducing anemia based on food fortification and supplementation, we would like to highlight that the implementation of surveillance and monitoring systems is also important, not only to provide adequate intake but also to prevent excessive repletion with iron. Unintentional negative consequences of elevated intakes of micronutrients can be avoided if programs are well designed. Potentially negative consequences of consumption of high doses of iron from supplementation or fortification include negative effects on the gut microbiome, including overgrowth of pathogenic bacteria and reduction of beneficial bacteria. 54 A common consequence of excessive consumption of iron is diarrhea, which may further limit the body’s ability to absorb micronutrients. Finally, it is also important to consider that several countries in Latin America and the Caribbean are undergoing economic transition, with consequent high rates of overweight and obesity. 55–57 We recommend reporting further stratifications of the prevalence of anemia and iron status by body mass index (BMI) or preferably on anthropometric or adiposity measurements in ongoing studies. Obese women are reported to have significantly lower iron absorption than women with normal BMI. 58 Among many possibilities, this may be related to increases of proinflammatory molecules, such as C-reactive protein and hepcidin, that can negatively affect iron absorption. 59,60
The prevalence of anemia has been reported in most countries of Latin America and the Caribbean. However, there is a lack of multiple prevalence reports spanning a wide range of years. Only a few countries reported information about changes in anemia prevalence in national or regional representative populations over time. In most of the included studies, there was no information about nutritional causes of anemia, such as iron, folate, or vitamin B12 deficiency. In addition, we did not report other causes of anemia besides micronutrient deficiency that may be influencing the data being reported. Despite these limitations, this study provides information about the recent prevalence of anemia in national or regional representative populations in Latin America and the Caribbean. The present computer-based systematic search of studies, complemented by National Health Surveys, indicates that anemia is still a public health problem in children under 6 years of age and women of childbearing age in most countries in Latin America and the Caribbean.
Footnotes
Authors’ Contributions
María F. Mujica-Coopman, Alex Brito, and Manuel Olivares designed the study; all authors interpreted the data and helped to prepare the manuscript; Manuel Olivares had primary responsibility for the final content. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Héctor Cori is Nutrition Science Director in Latin America for DSM Nutritional Products.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: DSM Nutritional Products provided funding for this study.