
Abstract
Background:
In recent decades, the general socioeconomic situation in Latin America and the Caribbean countries has improved, and many vitamin A programs have been implemented in an attempt to reduce vitamin A deficiency in the region.
Objective:
To examine vitamin A status in Latin America and the Caribbean based on serum retinol concentrations and to contrast available data published before and after 1998.
Methods:
A systematic review was performed. National surveys or representative studies that reported vitamin A status were selected.
Results:
Ten national surveys and six representative studies were identified. Data for children under 6 years of age indicate that Guatemala and Nicaragua have practically eradicated vitamin A deficiency (less than 2% prevalence of serum retinol < 20 µg/dL). In Costa Rica, Cuba, El Salvador, and Panama, the prevalence of vitamin A deficiency ranged from 2.8% to 9.4%. In Peru, Honduras, Argentina, Ecuador, and Brazil, vitamin A deficiency is a moderate public health problem (prevalence from 14.0% to 17.4%), while in Colombia, Mexico, and Haiti it is a severe public health problem (prevalence from 24.3% to 32.0%). Disadvantaged groups (indigenous people and those of Afro-Colombian descent) have the highest rates of deficiency. The prevalence of vitamin A deficiency is under 20% in schoolchildren and adult women. When data published before and after 1998 for children under 6 years of age were compared, most Central American countries had a reduction in the prevalence of vitamin A deficiency ( p < .05), whereas in South American countries, the prevalence of vitamin A deficiency increased over time ( p < .05).
Conclusions:
The prevalence of vitamin A deficiency in children under 6 years of age has decreased in many Central American countries, but vitamin A deficiency still remains a public health problem in numerous Latin America and Caribbean countries, especially among disadvantaged and vulnerable groups. Because of issues with the accuracy of the serum retinol biomarker reflecting body stores, these results must be interpreted with caution.
Introduction
Vitamin A deficiency has been recognized as a public health problem in many developing and low- to middle-income countries. 1 The primary cause of vitamin A deficiency is chronic malnutrition, which commonly occurs when staple foods are poor sources of vitamin A. Most prevalent during nutritionally demanding periods of life, vitamin A deficiency is the leading cause of preventable childhood blindness 2 and is a major contributor to increased morbidity and mortality stemming from infections. 3 By convention, serum retinol levels < 20 µg/dL are considered to indicate deficiency. 4 In 1998, Mora et al. 5 suggested that most of the vitamin A deficiency in Latin America and the Caribbean was subclinical and showed that the prevalence of vitamin A deficiency in children under 5 years of age ranged from 6% in Panama to 36% in El Salvador, with approximately 14.5 million children under 5 years of age affected by this condition. In 2009 the World Health Organization (WHO) estimated that 33% of the world population had vitamin A deficiency, with a prevalence of 15.4% for the Americas. 6 However, these data require special interpretation in developing countries because of the limitations associated with the use of the serum retinol biomarker. For example, because serum retinol is homeostatically controlled, its concentrations do not typically decline unless the body's reserves are limited (liver stores fall below 20 μg/g). 7 Furthermore, infection and inflammation cause a temporary decline in serum retinol that does not accurately reflect a change in body stores and may lead to an overestimation of the prevalence of vitamin A deficiency. 8 In the past few decades, the general socioeconomic situation of the Latin America and Caribbean countries has improved, and many vitamin A programs have been implemented in an attempt to reduce vitamin A deficiency in the region. 9–12 However, the application of strategies must be carefully planned, conducted, and monitored with caution, as there is also a risk of providing excessive amounts of vitamin A. 13,14 Excess intake of vitamin A may potentially occur in situations where, in addition to a successful vitamin A fortification program, traditional interventions, including vitamin A supplementation, are still ongoing and newer interventions, such as multiple micronutrient powders, are being introduced. Current interpretations of serum retinol data from Latin America and the Caribbean in this review focus on assessing deficiency, since national data covering the entire range of vitamin A status (including toxic states) were unavailable. The purpose of this systematic review is to examine vitamin A status in Latin America and the Caribbean based on serum retinol concentrations, and to compare available data published before and after 1998.
Methods
A systematic review was conducted between July 2011 and April 2012 and updated in August 2014. All available evidence regarding the prevalence of vitamin A deficiency in Latin America and the Caribbean since 1998 was included. PubMed, LILACS, Nutrinet, and Scielo were used to identify research articles by combining the terms “vitamin A,” “deficiency,” and “prevalence” with the name of each country in Latin America and the Caribbean. No studies were excluded on the basis of language. In addition, national surveys or national-level representative studies in apparently healthy populations were identified by accessing the websites of the ministries of health. Serum retinol was standardized to micrograms per deciliter (µg/dL) to facilitate comparisons. Vitamin A deficiency was defined as serum retinol < 20 µg/dL. 4 The magnitude of the public health problem was defined as none, mild, moderate, and severe according to prevalence rates of < 2%, ≥ 2% to < 10%, ≥ 10% to < 20%, and ≥ 20%, respectively, following WHO criteria. 6 The most recent data on the prevalence of vitamin A deficiency were compared with data published before 1998. 5 Prevalence data are reported as percentages and confidence intervals. Surveys were compared by the chi-squared test. A P value < .05 was considered to indicate statistical significance. Figures were plotted using the R programming language version 3.1.0. 15
Results
A total of 782 articles were initially identified (79 were excluded by duplication). After reviewing the titles and abstracts, 606 studies were excluded because the information was not relevant to the purpose of the review, and 10 national surveys were included, leaving the number of preselected studies at 107. After a detailed review, 91 studies were excluded because they were not representative of a Latin America and Caribbean country, were clinical trials, were studies conducted on unhealthy populations, or were reviews. In the end, 10 national surveys and 6 representative studies were selected for this review 16–31 (Figure 1).
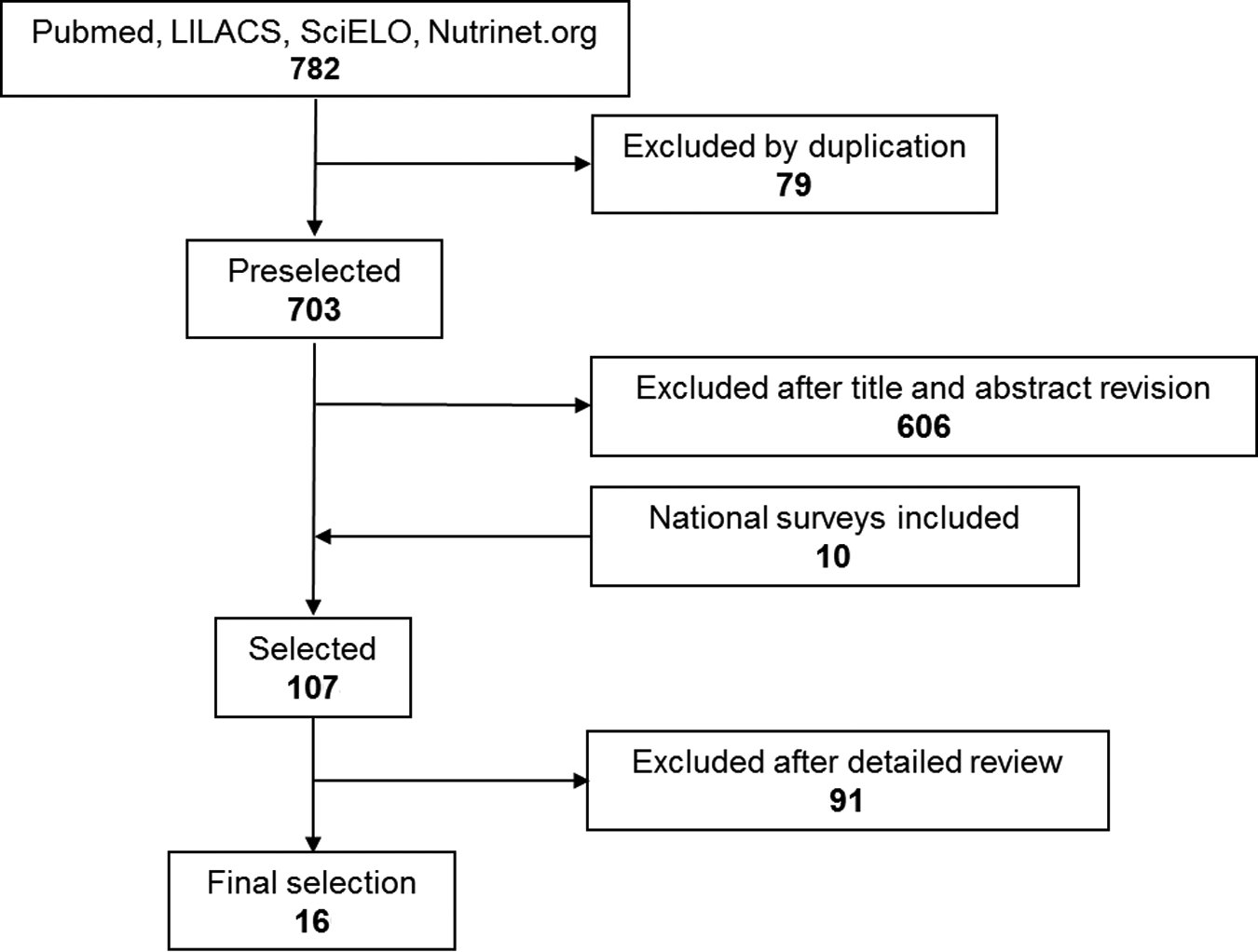
Flow diagram for selection of the studies of vitamin A deficiency in Latin America and the Caribbean from 1998 to 2014.
The available evidence allowed us to examine the prevalence of vitamin A deficiency for different age groups (children under 6 years of age, schoolchildren 6 to 12 years of age, and childbearing women > 12 years of age). Most studies indicated assessment of serum retinol using-high performance liquid chromatography (HPLC), with the exception of two studies in which serum retinol was measured by spectrophotometry. 18,25 Only two studies reported adjusting the effect of inflammation on serum retinol using an acute phase protein biomarker. 16,21
Prevalence of Vitamin A Deficiency
Most of the available information was found for children under 6 years of age (14 countries). In this age group, the lowest prevalence rates of vitamin A deficiency were in Guatemala (0.3%) and Nicaragua (0.7%); thus, vitamin A deficiency in this age group is not a public health problem in these countries. 16,21 Vitamin A deficiency in children under 6 years of age was classified as a mild public health problem in Costa Rica, Cuba, El Salvador, and Panama, with prevalence rates ranging from 2.8% to 9.4% 17–20,23 (Figure 2). In Peru, Honduras, Argentina, Ecuador, and Brazil, vitamin A deficiency is a moderate public health problem in this age group (prevalence from 14.0% to 17.4%) 24–28 , while in Colombia, Mexico, and Haiti it is a severe public health problem (prevalence from 24.3% to 32.0%). 29–31 Among school-aged children (6 to 12 years), vitamin A deficiency is not a public health problem in Cuba (prevalence 0.9%); it is a mild public health problem in Costa Rica (2.1%) and a moderate public health problem in Mexico (prevalence 16.9%). 17,19,30 Among adult women, vitamin A deficiency is not a public health problem in El Salvador and Nicaragua (prevalence rates of 1.0% and 1.3%, respectively), 20,22 while it is a mild public health problem in Mexico and Peru (prevalence rates of 4.3% and 8.7%, respectively) 24,30 and is a moderate public health problem in Brazil (prevalence 12.3%) 28 (Figure 2). The prevalence of vitamin A deficiency is higher in disadvantaged and vulnerable population groups. For example, Panamanian indigenous children had a higher prevalence than nonindigenous children (23.7% vs. 7.4%). 23 Colombian preschoolers of African descent or of indigenous origin have high rates of vitamin A deficiency (29.5% and 34.1%, respectively), 29 similar to the rate for Haitian children (32%). 31
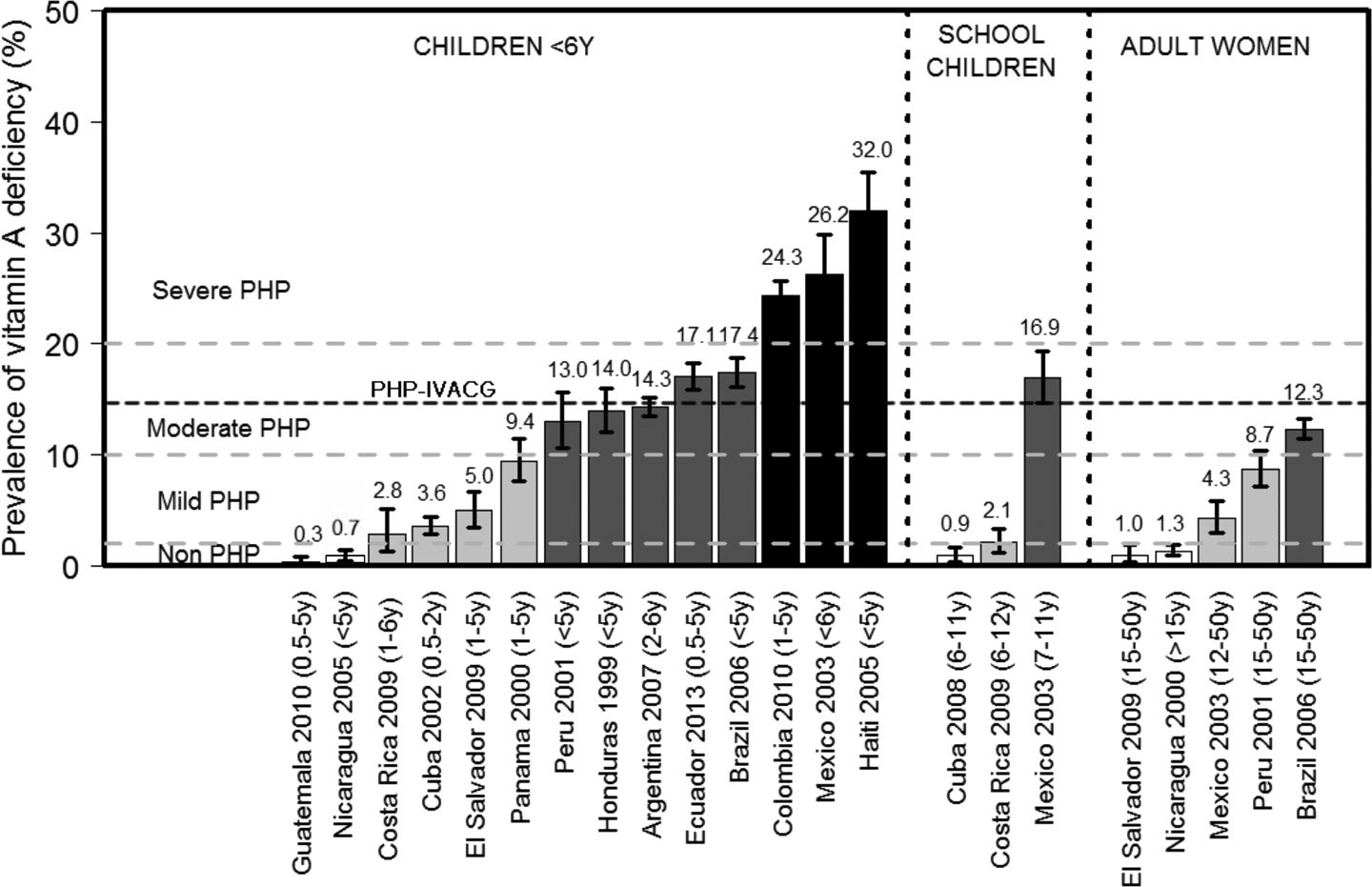
Prevalence of vitamin A deficiency in Latin America and the Caribbean from 1998 to 2014. Vitamin A deficiency was defined as serum retinol < 20 µg/dL. The magnitude of the public health problem (PHP) was defined as none, mild, moderate, and severe by point prevalence rates of < 2%, ≥ 2% to < 10%, ≥ 10% to < 20%, and ≥ 20%, respectively, following World Health Organization (WHO) guidelines; 6 the heavy line indicates the point prevalence (> 15%) defined as a public health problem by the International Vitamin A Consultative Group (IVACG). 4
Changes in the Prevalence of Vitamin A Deficiency over Time in Children under 6 Years of Age: Comparison of Pre- and Post-1998 Data in Latin America and the Caribbean
Guatemala and Nicaragua had dramatic changes in the prevalence of vitamin A deficiency, decreasing from 15.8% in 1995 to 0.3% in 2010 and from 31% in 1993 to 0.7% in 2005, respectively (p < .001); these countries are currently classified as not having a public health problem of vitamin A deficiency in this age group 16,21 (Figure 3). El Salvador had the highest reduction in the prevalence of vitamin A deficiency, from 36% in 1988 to 5% in 2009, a decrease of 31 percentage points (p < .001), resulting in a change in classification from having a severe public health problem to a mild public health problem. 20 Costa Rica also had a reduction in the prevalence of vitamin A deficiency, from 8.7% in 1996 to 2.8% in 2009 (p < .001). 17 In contrast, there was an increase in the prevalence of vitamin A deficiency in both Ecuador and Colombia (p < .001). Vitamin A deficiency remains a moderate public health problem in Ecuador, with an increase in prevalence from 14.1% in 1986 to 17.1% in 2013 (p < .001). In Colombia, vitamin A deficiency changed from a moderate to a severe public health problem, with an increase in prevalence from 13.6% in 1995 to 24.3% in 2010 (p < .001). 27,29 Panama was the only country in Central America where the prevalence of vitamin A deficiency increased over time (from 6.1% in 1981 to 9.4% in 2000, p < .01). However, the classification of vitamin A deficiency as a mild public health problem in Panama remains unchanged. 23
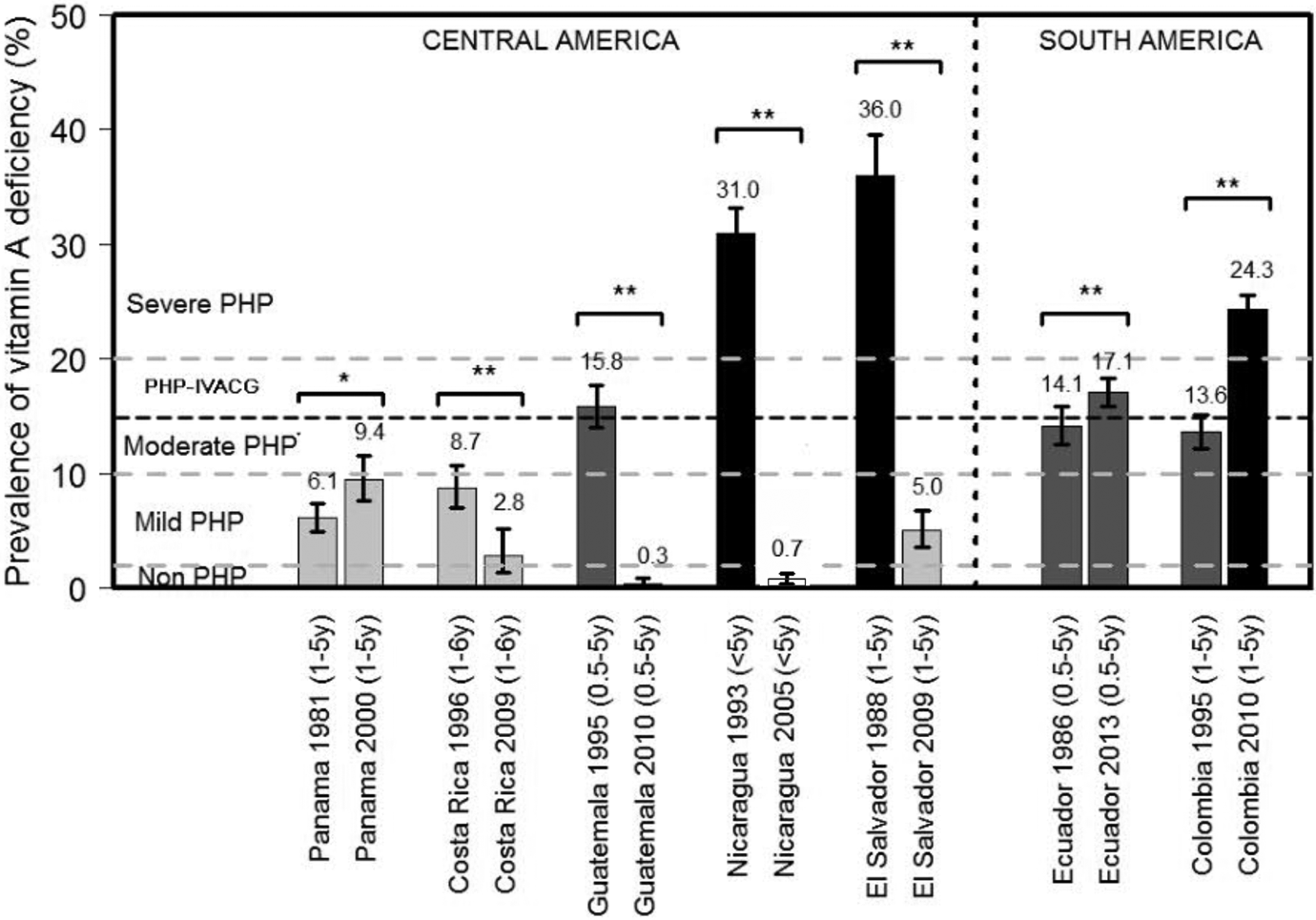
Changes in the prevalence of vitamin A deficiency over time in children under 6 years of age: comparison of pre- versus post-1998 data in Latin America and the Caribbean. The magnitude of the public health problem (PHP) was defined as none, mild, moderate, and severe by point prevalence rates of < 2%, ≥ 2% to < 10%, ≥ 10% to < 20%, and ≥ 20%, respectively, following World Health Organization (WHO) guidelines; 6 the heavy line indicates the point prevalence (> 15%) defined as a public health problem by the International Vitamin A Consultative Group (IVACG). 4 The survey results were compared with the chi-squared test. *p < .05, **p < .001.
Discussion
We examined the latest data on the prevalence of vitamin A deficiency in Latin America and the Caribbean based on the serum retinol biomarker. The Central American countries had the highest reduction of vitamin A deficiency in children under 6 years of age. Guatemala and Nicaragua are the only countries that have nearly eradicated vitamin A deficiency, with prevalence rates of less than 2%. This is probably attributable to multiple strategies the countries have undertaken to control this deficiency, most notably universal fortification of sugar. 32,33 Costa Rica and El Salvador also had improvements in vitamin A status, presumably as a consequence of the implementation of national sugar fortification programs. 12,14,33 On the other hand, an increase in the prevalence of vitamin A deficiency was observed in the only two South American countries where data were collected before and after 1998 (Ecuador and Colombia). The highest rates of deficiency in these two countries are found among the most disadvantaged and economically vulnerable groups, indigenous people and people of African descent. 23,29 It is promising to observe reductions in the prevalence of vitamin A deficiency over time in preschool-age children in Costa Rica, Guatemala, Nicaragua, and El Salvador. However, there are countries where vitamin A deficiency is still a severe public health problem (Colombia, Mexico, and Haiti) and/or the prevalence of vitamin A deficiency has increased over time (Panama, Colombia, and Ecuador). Unfortunately, only a few of the available surveys assessed vitamin A status in school-aged children (Cuba, Costa Rica, and Mexico) or adult women (El Salvador, Nicaragua, Mexico, Peru, and Brazil); in these countries, vitamin A deficiency ranges from not being a public health problem to being a moderate public health problem in both school-aged children and adult women.
Interestingly, a higher prevalence of vitamin A deficiency was observed in South American countries with emerging economies (Ecuador, Brazil, Colombia, and Mexico) than in several Central American countries that are still in the developing economy stage (Guatemala, Nicaragua, and El Salvador). In Guatemala, the introduction of fortification of sugar with retinyl palmitate in 1975 resulted in a substantial increase in vitamin A status one year after the program’s implementation. 12 El Salvador, Honduras, and Nicaragua later implemented national sugar fortification programs because of its cost-effectiveness. 33 As shown by the most recent surveys, Guatemala (prevalence 0.3% in 2010, a decrease of 15.5 percentage points from 1995) and Nicaragua (prevalence 0.7% in 2005, a decrease of 30.3 percentage points from 1993) essentially eliminated vitamin A deficiency; El Salvador was the country with the highest reduction in prevalence, with a decrease of 31.0 percentage points. It is believed that the reduction of vitamin A deficiency in at-risk populations is mostly a consequence of sugar fortification programs. Other actions have also been implemented, including vitamin A fortification of other staple foods, such as fats, oils, margarines, and cereals, 34 and periodic delivery of supplements to preschool-age children and infants 9 during immunization visits, especially during poliomyelitis eradication campaigns. 10,11 In view of these multiple potential sources of vitamin A, it is important to pay special attention to the possible excess intake of vitamin A in these countries. Updated reports are especially required for countries that have instituted fortification programs, including Honduras and Panama, whose latest surveys were in 1999 and 2000, respectively. 23
The few available surveys among children under 6 years of age in South America indicated that vitamin A deficiency is still a national public health problem in Peru, Argentina, Ecuador, Brazil, and Colombia. Peru has the lowest prevalence. Since 1999, this country has implemented a national strategy (Good Start in Life) that is based on the delivery of vitamin A and other micronutrients in fortified foods to poor rural communities of the Andean highlands and Amazon forest, covering 75,000 children under 3 years of age, 35,000 mothers, and 1 million inhabitants from 223 poor communities. Although the latest national report from 2001 indicated that vitamin A deficiency was a moderate public health problem, an external evaluation of this program (from 2000 to 2004), without national representativeness, showed that the rate of vitamin A deficiency decreased from 30.4% to 5.3% (p < .01). 35 The effectiveness of these programs will require updated national data on the prevalence of vitamin A deficiency in order to confirm changes over time. Similarly, national data on vitamin A deficiency in Brazil and Mexico require an update to enable reasonable comparisons to be made. Ecuador and Colombia are the only countries where data were collected before and after 1998. The data showed a higher increase in the prevalence of vitamin A deficiency over time in Colombia (24.3% in 2010, an increase of 10.7 percentage points from 1995) than in Ecuador (17.1% in 2013, an increase of 3 percentage points from 1986). This high rate of increase in Colombia is presumably due mainly to the higher prevalence of vitamin A deficiency in disadvantaged and vulnerable groups in that country, which include children of African descent and those of indigenous origin. In 2010, these two groups had rates of vitamin A deficiency of 29.5% and 34.1%, respectively, similar to the 32% rate among Haitian children. The main causes of these high rates are probably the low availability of vitamin A in the food sources; cultural differences, given that indigenous people have their own distinct languages and social and political institutions that differ from those of mainstream society, which may lead to problems of supply, distribution, and stock points in the delivery, storage, and coverage of foods or supplements containing vitamin A delivered by national programs implemented by governments; poverty; lack of access to medical services; lack of national food program coverage; and high rates of infection and inflammation. 36,37
The data on the prevalence of vitamin A deficiency reported by Mora et al. 5 have not been updated for most Caribbean countries. Mora et al. reported vitamin A deficiency ranging from not a public health problem to a mild public health problem in St. Vincent (prevalence rates of 1.1% to 6.2%), a mild to moderate public health problem in Dominica (prevalence rates of 1.2% to 10.7%), a moderate public health problem in Antigua (prevalence of 18.7%), and a moderate to severe public health problem in the Dominican Republic (prevalence rates of 15.0% to 27.6%). Thus, the current prevalence of vitamin A deficiency in these countries is unknown. In the Caribbean, surveys conducted after 1998 indicate that vitamin A deficiency is a mild public health problem in Cuba and a severe public health problem in Haiti.
The prevalence of vitamin A deficiency varies with age. In two of the studies in which data were collected both in children under 6 years of age and in school-age children within the same country (Cuba and Mexico), the prevalence was lower in school-age children (p < .05) (Figure 2). Among Mexican school-age children, stratification by age showed that the prevalence was higher in children aged 7 or 8 years (25.1%) than among children aged 9 or 10 years (12.5%) or 11 years (9.7%). 30 The prevalence of vitamin A deficiency can also vary according to a combination of age and sex, as evidenced from data collected on adult women. In fact, in all five instances in which data were collected within the same country for both children and adult women (El Salvador, Nicaragua, Mexico, Peru, and Brazil), adult women had a lower prevalence of vitamin A deficiency (p < .05) (Figure 2). The observation of higher prevalence rates of vitamin A deficiency in Latin America and Caribbean preschool-age children (< 6 years) is in agreement with global vitamin A deficiency prevalence data. 2 It must be noted that the criteria to interpret serum retinol concentrations are applicable to preschool-age children, whereas data from the older groups have not been validated. Thus, using the same cutoff point (< 20 ng/mL) 4 may not be legitimate, since the physiological conditions are different. For example, serum retinol concentration increases with age independently of vitamin A status. 38 This may explain why older children and women may have higher serum retinol concentrations and lower rates of vitamin A deficiency. Additional research is needed to clarify this issue.
This review aimed to summarize available evidence based on serum retinol, the most commonly used biomarker for assessing vitamin A deficiency. However, we must mention the case of Bolivia, where a recent study with national representativeness of children 6 to 24 months of age used serum retinol-binding protein (SRBP) as a proxy for vitamin A status. The results showed a high prevalence of vitamin A deficiency in this age group (41% with SRBP < 20 ng/mL), after exclusion of children with high concentrations of the inflammatory markers C-reactive protein (CRP) (> 25 mgl/L) and alpha-1-acid glycoprotein (AGP) (> 1 g/L). 39 Based on this evidence, we believe that vitamin A deficiency should be also classified as a public health problem in Bolivia. In most reported surveys, vitamin A status was measured by standardized laboratory techniques (serum or plasma retinol determined by HPLC). Serum retinol has been used for years as the prime indicator for routine assessment of vitamin A deficiency. 40 However, because vitamin A is homeostatically controlled within a narrow range, it may not properly reflect body vitamin A stores unless the stores are very high or very low. Although biomarkers capable of indirectly assessing liver stores (the stable isotope dilution and dose–response tests) may be ideal, either they have not been accepted as standard tests or their cost prohibits their widespread use and they are not easily practicable in field studies. Another common issue with the accuracy of the serum retinol biomarker is that infection and inflammation have a negative effect on retinol concentrations. 41,42 Because RBP is an acute phase protein, when its values increase there is a consequential decline in retinol concentration unrelated to vitamin A status that can result in a misidentification of vitamin A deficiency. Therefore, it would be ideal for surveys to apply correction factors for serum retinol using CRP and AGP measurements in order to provide a more accurate assessment of vitamin A status. 37 In this review, the survey from Guatemala showed a prevalence of vitamin A deficiency of 0.3% in children who presented with AGP < 1.0 g/L and 1.0% in children who presented with AGP ≥ 1.0 g/L, after adjustment for inflammation using retinol as a biomarker. 16 Similarly, in Nicaragua the prevalence of vitamin A deficiency was 0.7% in children who presented with normal AGP and 1.8% in children who presented with high AGP. 21 Thus, the magnitude of the prevalence of vitamin A deficiency in other countries could be somewhat overestimated. As a result, it is difficult to interpret these prevalence rates from a public health perspective, as is the case in Costa Rica, El Salvador, and Nicaragua. Although these countries are classified as having mild public health problems, with prevalence rates of 2% to 10%, this may not be accurate. There is some disagreement about the classification of vitamin A deficiency between WHO and the International Vitamin A Consultative Group (IVACG). We used the WHO reference to define the magnitude of the public health problem of vitamin A deficiency. 6 The WHO definition of a moderate public health problem (prevalence rates of 10% to 20%) actually includes the minimum prevalence cutoff of 15% currently recommended by the IVACG (Figures 2 and 3). 4 Furthermore, since many of the reports did not correct for inflammation or infection, the use of stricter criteria for the magnitude of the vitamin A deficiency problem (prevalence rates of 2% to 10% indicating a mild public health problem) may not be advisable.
The use of serum retinol concentration lower than 20 µg/dL as an indicator of vitamin A deficiency in children is not clearly supported by any physiological or metabolic evidence. 7 An additional option for estimating the severity of this public health problem in countries with a high prevalence of vitamin A deficiency is to monitor rates of clinical manifestations of vitamin A deficiency, such as xerophthalmia (including night blindness, Bitot’s spots, and corneal xerophthalmia). 43 A cut point of a 5% prevalence of night blindness is used to define a public health problem in pregnant women, while multiple cut points ranging from > 0% to > 5% are used to designate it as a mild to severe public health problem in children 24 to 71 months of age. 6
Although fortification is a cost-effective strategy and has been successfully implemented with many micronutrients, there is a potential for overconsumption. 13,14 Thus, monitoring the possible occurrence of excess intake is recommended, especially considering the adverse effects of vitamin A excess, such as bone disease, intracranial hypertension, and altered liver function. 44 Further research is needed to ascertain whether subclinical toxicity exists and, if so, what are its effects on overall health and well-being. A survey from Guatemala reported that 3% of the studied sample had serum retinol concentrations above 60 μg/L, 16 while studies of human vitamin A stores in Nicaragua 14 and consumption of fortified sugar in Guatemala 13 have been suggestive of excessive intake. Continuous monitoring of fortification concentration, the number of foods fortified, consumer intake, and markers of vitamin A status is advised in order to reduce the risk of excess vitamin A consumption, especially in countries where there is an accelerated decrease in the prevalence of vitamin A deficiency.
We cannot rule out that some surveys and studies have over- or underestimated the prevalence of vitamin A deficiency due to factors such as sampling procedures, laboratory bias, and the influence of infection or inflammation on serum or plasma retinol. Moreover, comparisons were performed between surveys from the same country depending on the year of data collection and thus represent a general overview. This is especially true, considering that reports with more recent information may be available but are difficult to retrieve, and some data (i.e., data from Brazil, Mexico, Peru, Honduras, and Panama) are relatively old. Nevertheless, this review summarizes the trends of vitamin A deficiency in Latin America and the Caribbean, highlighting the significant efforts being made by a number of countries to control and prevent vitamin A deficiency, predominantly through universal or targeted fortification of food with vitamin A, which have contributed to the decline of vitamin A deficiency in numerous Latin America and Caribbean countries. Currently, new strategies are being promoted with the aim of improving dietary intake by introducing plant sources of vitamin A in at-risk populations. Such efforts include the implementation of home and community gardens, dietary diversification education, and advances in biofortification of staple crops to increase vitamin A content and bioavailability in foods such as maize, rice, cassava, beans, wheat, and sweet potatoes. 45,46 These new strategies may be considered in future programs, since they are self-sustainable and the forms of vitamin A consumed (provitamin A carotenoids) are not toxic, even if consumed in high amounts. Moreover, with the increasing variety of strategies now available, it is necessary to be aware of potential coverage overlap among the different options during their implementation. 46
Conclusions
Based on the evaluation of serum retinol concentrations, the prevalence of vitamin A deficiency in children under 6 years of age has been reduced in many Central American countries (practically eradicated in Guatemala and Nicaragua), but it still remains a public health problem in other countries in Latin America and the Caribbean. Most published data on vitamin A deficiency among vulnerable groups vary between countries according to geographic, ethnic, age, or socioeconomic characteristics. A high prevalence of vitamin A deficiency was reported in Colombian and Haitian young children, especially in Afro-American and indigenous individuals, and in Mexican children and adolescents. Because of issues with the accuracy of the serum retinol biomarker reflecting body stores, these results must be interpreted with caution. Given current programming efforts, a stronger commitment by most governments in Latin America and the Caribbean to implement integrated national programs utilizing effective intervention strategies is required in order to accomplish international goals established by both governmental and international agencies to safely and effectively reduce vitamin A deficiency.
Footnotes
Authors’ Contributions
Gustavo Cediel, Manuel Olivares, Alex Brito, and Daniel López de Romaña designed the study; all authors interpreted the data and helped to prepare the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Gustavo Cediel, Manuel Olivares, Alex Brito, Daniel López de Romaña, and Michael R. La Frano have no conflict of interest. Héctor Cori is Nutrition Science Director in Latin America for DSM Nutritional Products.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study received financial support for the research and publication by DSM Nutritional Products.