
Abstract
Background:
Proximal hamstring complex injury (PHCI) is a common injury among professional athletes, particularly those participating in pivot contact sports. Previous studies have suggested that surgery can be effective in restoring function and allowing athletes to return to sport (RTS), but the factors influencing successful RTS have been less clear.
Purpose:
To assess RTS capabilities after surgical treatment of PHCI in professional athletes and to identify favorable predictors of RTS.
Study Design:
Case series; Level of evidence, 4.
Methods:
This study (2002-2022) was conducted on professional athletes who underwent surgical treatment for PHCI at a sports surgery center. The primary outcome of the study was the RTS capability, evaluated based on the rate of athletes’ return to their preinjury level of competition, time delay to RTS, and quality of RTS as measured using their level of performance and progression of scores on activity scales such as the Tegner Activity Scale (TAS) and University of California, Los Angeles (UCLA), scale. “Maintained performance” was defined as athletes returning to the same preinjury activity level (per the TAS and UCLA scale) and perceiving themselves to have maintained their performance. Secondary outcomes covered the potential RTS predictors and complication rate. The study distinguished 2 types of PHCI: proximal hamstring tendon avulsion injury (proximal rupture with empty footprint, or having a “positive dropped ice cream sign”) and complete proximal hamstring free tendon rupture (PHTR; proximal rupture without empty footprint, or having a “negative dropped ice cream sign”).
Results:
The study examined 64 professional athletes (mean age, 27.3 years; 82.8% male) undergoing surgery for PHCI. The RTS rate was 98.4%, with 78.1% of the athletes returning to their preinjury level of competition at 6.2 months (SD, 2.5 months). Twelve (19%) patients had returned to sport at an inferior level of competition, and 2 (3.1%) were unable to continue in their preinjury sport. Subgroup analysis revealed variation in RTS based on sport type, with the highest rate of return to preinjury performance found in athletes in handball and sports with splits (fencing, squash, and escalade; 100%) and soccer (95.2%). In the univariate analysis, male sex (hazard ratio [HR], 4.05; 95% CI, 1.45-11.3; P = .008), higher preinjury TAS score (HR, 1.27; 95% CI, 1.06-1.52; P = .011), injury involving the semimembranosus (HR, 4.84; 95% CI, 2.31-10.2; P < .001) or conjoint tendon (HR, 3.12; 95% CI, 1.55-6.25; P = .001), and PHTR (HR, 7.77; 95% CI, 3.54-17.0; P < .001) were significantly associated with a better postoperative level of competition. Multivariate analysis identified 3 favorable predictors of RTS with HRs of 2.91 (95% CI, 1.01-8.35; P = .047) for male sex, 3.86 (95% CI, 1.78-8.37; P < .001) for isolated semimembranosus injury, and 5.18 (95% CI, 2.24-12.0; P < .001) for PHTR. The complication rate was 4.7%.
Conclusion:
Favorable predictors of early RTS were male sex, isolated semimembranosus injury, and PHTR injuries.
Registration:
NCT02906865 (ClinicalTrials.gov identifier).
Keywords
Proximal hamstring complex injuries (PHCIs) are common musculoskeletal problems in professional athletes, with the injury severity ranging from strains to complete proximal hamstring free tendon rupture (PHTR), proximal hamstring tendon avulsion injuries (PHAIs), and proximal hamstring bony avulsion from the insertion at the ischial tuberosity.1,8,10,14,29,30,34 The mechanism of injury generally involves an eccentric contraction of the hamstring muscles due to sudden forceful hyperflexion of the hip while the knee is extended or hyperextended.1,4-6 PHTR generally involves a slow-velocity stretching injury such as in high kicking, splits, and sliding tackles, 7 while other PHAIs and myotendinous injuries involve high-velocity injuries during running, water skiing, or ballet extreme positions.1,4-6 Patients with PHCI have pain, subcutaneous hematoma and a possible palpable defect along the hamstring trajectory.11,28 Additional symptoms include an avoidance of hip flexion when the knee is extended (hurdler position); a lack of hamstring muscle tension (bow stringing sign); and sciatic nerve–related issues, such as motor and sensory deficits, and neuropathic pain.12,15,22,28,38 Several imaging modalities can be used to confirm the diagnosis, such as ultrasound imaging, magnetic resonance imaging (MRI), and standard radiography for bony involvement.2,32,41
Patients with PHAI frequently require surgical treatment, particularly in competitive athletes, to avoid prolonged recovery times that could affect their athletic careers.16,20,24,39 Patients who receive nonoperative management for PHAI experience lower satisfaction rates and reduced strength of the hamstring muscles and are less likely to return to their preinjury level of sports participation. 18 When an athlete has operative treatment, postoperative care should focus on protecting the repair and providing a rapid rehabilitation protocol to allow the earliest return to sport (RTS). 39
There is a lack of clear guidelines on the timing of RTS and the criteria that should be used to determine when an athlete is ready to RTS after surgical treatment of PHAI.5,18 The resumption of high-level sports may be allowed after 16 weeks by some surgeons, whereas others do not allow it before 50 weeks depending on the type of sport and injury.6,7,9,21,24 Most of the available literature targets mixed populations of athletes and nonathletes, which may affect the generalizability of their recommendations. 21 Furthermore, the definition of RTS is different between the studies: a systematic review by Belk et al 9 in 2019 found that most studies defined RTS as a return to any sport while only 1 study defined it as a return to the same sport in which the patient was engaged before the injury. 9 These studies may not be applicable when assessing professional athletes, who often need to return to their preinjury level to maintain their careers.
The primary objective of this study was to evaluate the RTS capabilities of surgically treated professional athletes with PHCI as evaluated using the rate of RTS to the same preinjury level of competition, time delay to RTS, and quality of RTS as measured using the level of performance and progression of scores on activity scales such as the Tegner Activity Scale (TAS) 33 and University of California, Los Angeles (UCLA).3,40
The secondary objectives were to report the complication rates and to investigate any potential predictor correlated with early RTS.
We hypothesized that individual professional athletes with PHCI, upon receiving surgical treatment, would have the potential to return to their specific preinjury level of sports activity. RTS may be associated with potential predictors such as age, chronicity, extent of injury (completeness and type of tendons involved), type of sport, and tendon retraction.
Methods
Study Design
This prospective cohort study was conducted at a specialized sports surgery referral center between January 2002 and May 2022 as part of the Proximal Hamstring Avulsion Surgery Cohort Study (ClinicalTrials.gov identifier NCT02906865).
It included professional athletes with PHCI who were treated surgically. The study defined professional athletes in line with the French Sports Code, Articles L221 and L222: “… toute personne ayant pour activité rémunérée l’exercice d’une activité sportive dans un lien de subordination juridique avec une association sportive ou une société…. Afin d’assurer la protection des sportifs et entraîneurs professionnels et de garantir l’équité des compétitions.” This translates to individuals who engage in a remunerated sports activity in a legal subordination relationship with a sports association or company. These athletes are typically involved in high-level sports that include national or international competitions and require exceptional athletic abilities. Exclusion criteria included revision surgery, <1 year of follow-up, bony PHAI, and refusal to be enrolled in the study.
Based on MRI findings, the study distinguished 2 types of PHCI: PHAI, which included proximal hamstring tendon avulsion from the ischial tuberosity with an empty proximal hamstring footprint (positive dropped ice cream sign 37 ), and PHTR, which involved proximal hamstring ruptures at the free tendon area, leaving a tendon remnant at the corresponding ischial tuberosity footprint (negative dropped ice cream sign).14,30,34
Outcome Measurements
The primary outcome parameters of this study were the capability of professional athletes to RTS, as indicated by the rate of RTS, the length of time to RTS in each sporting profession, and the quality of RTS. The quality of RTS was evaluated based on the progression of the patient’s TAS 33 and UCLA scale scores,3,40 as well as the patients’ subjective impressions of performance at follow-up.
The secondary outcome parameters included the rate of complications and potential predictors of RTS, such as the type of injury (PHAI vs PHTR), type of sport (pivot contact, pivot without contact, or sport without pivot), chronicity of injury (acute injury, defined as an injury to surgery delay of a maximum of 4 weeks, vs chronic injury, defined as an injury to surgery delay of >4 weeks), preinjury and preoperative activity scale scores such as preoperative TAS 33 and UCLA scale scores,3,40 extent of lesion (completeness and type of tendons involved), and degree of MRI retraction.
The TAS is a graded activity scale designed to assess an individual’s level of physical activity, ranging from a sedentary lifestyle to competitive sports. 33 The UCLA scale is a 10-point activity-level rating system, ranging from “wholly inactive” to “regular participation in impact sports.”3,40
To assess potential predictors of RTS, we assessed the quality of RTS by categorizing patients into 2 groups based on their response at the 1-year follow-up:
Data Collection and Follow-up
The collected data included the patients’ information, as well as the previously cited outcomes of interest. The data were collected using Websurvey online software, which was completed by the surgeons for the medical history, physical examination findings, workup, and follow-up and by the patients for questionnaires and scores.
Activity scale scores for each athlete were collected at 3 distinct time points: preinjury (collected retrospectively at the first consultation), preoperatively (collected prospectively), and during various follow-up intervals (prospectively).
Surgical Techniques and Rehabilitation Protocol
All patients were operated on by the same surgeon (N.L.). For surgical treatment, the procedure followed the technique described by Lefèvre et al 24 in 2013. Patients received either spinal or general anesthesia. The procedure was done with the patient in the prone position. The incision was either transverse or longitudinal midline. Each procedure involved the reinsertion of the ruptured tendon to the ischial tuberosity using 2 to 4 suture anchors depending on the extent of injury. The postoperative protocol includes use of an extension-blocking hinged knee brace and initiation of standard rehabilitation after 1 week.
The rehabilitation strategy also closely followed the protocol described by Lefèvre et al. 24 It started with isometric strengthening for both the quadriceps and the hamstring muscles while maintaining knee flexion of 30° to 45°. By the end of the 6th week, the program progressed to dynamic quadriceps exercises in a closed-chain formation and active assisted workouts for the hamstrings. From weeks 12 to 16, patients were allowed to engage in brisk walking and potentially light jogging. During this period, the focus remained on enhancing hamstring strength using isokinetic exercises, eventually transitioning to eccentric workouts. From the 16th to 32nd weeks, athletes were generally able to return to their typical sporting activities.
From a review of the medical records of all patients treated at a specialized sports surgery referral center (Clinique du sport–Paris V), 80 consecutive patients who were professional athletes surgically treated for PHAI were identified for this study. Sixteen of these athletes were excluded from the study: 1 with a bony PHAI, 9 with insufficient follow-up time (<1 year at the time of study), and 6 who did not complete follow-up. Thus, 64 professional athletes met the inclusion criteria and are the basis of this report (Figure 1).
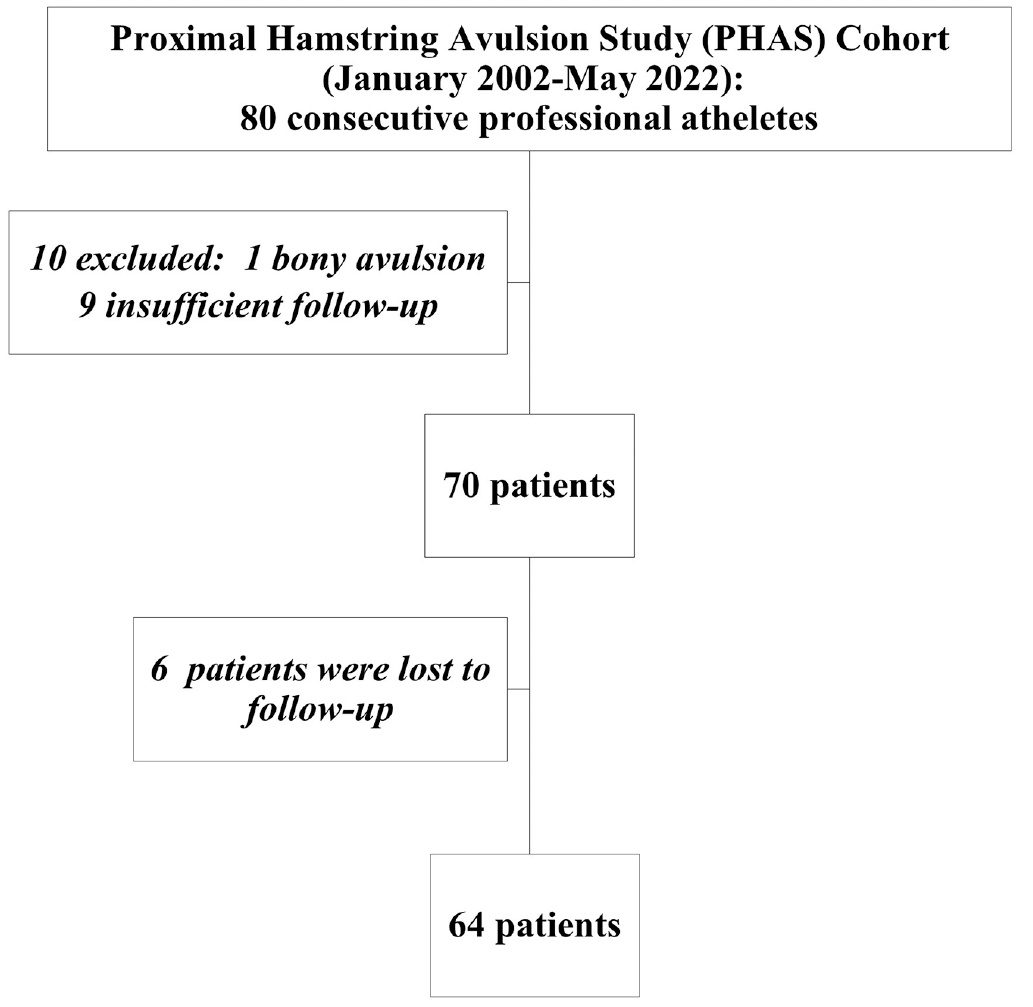
Study flow diagram.
Ethics Approval and Patient Consent
This study was approved by the institutional ethics review board. Patient consent was obtained at the first medical visit.
Statistical Analysis
To describe quantitative variables, we used the mean and standard deviation, as well as median and interquartile range, unless otherwise mentioned. To describe dichotomous variables, we used their frequencies and percentages. Qualitative variables were compared using either the Pearson chi-square test or the Fisher exact test, depending on the group sizes, whereas quantitative data were compared using the appropriate statistical tests between the Student t test and Wilcoxon Rank-Sum test.
A multivariate Cox proportional hazards model was done to estimate the hazard ratios (HRs) and 95% CIs of the risk factors associated with the outcome of interest. Univariate Cox regression analyses were conducted before fitting the multivariate model, to identify potential confounding variables with a significant association to the outcome at a P value of <.05. We used a backward stepwise method to eliminate nonsignificant variables from the model, using a threshold of P < .05 for retention in the model. The final multivariate model included only the variables that were significantly associated with the outcome. The proportional hazards assumption was tested using the Schoenfeld residuals and found to be valid.
All statistical analyses were carried out using the R software (Version 4.2; R Foundation for Statistical Computing).
Results
A total of 64 consecutive professional athletes who underwent surgical treatment for PHCIs at our center (Clinique du sport–Paris V) between January 1, 2002, and May 31, 2022, were analyzed. All patients (64/64; 100%) completed the 1-year follow-up. The mean duration for subsequent follow-ups was 4.2 years (SD, 3.9 years).
Patient Characteristics
The mean age at the time of surgery was 27.3 years (SD, 8.9 years), and most of the participants were male (53; 82.8%). Most participants were engaged in pivot contact sports (47; 73.4%) such as soccer, rugby, and basketball. The mean baseline TAS score was 8.9 (SD, 1.9), dropping to 2.9 (SD, 2.1) after injury. A similar pattern was seen with the UCLA scale score, where it dropped from 9.7 (SD, 1.2) preinjury to 3.9 (SD, 1.9) preoperatively. The predominant mechanism of injury was stretching injuries such as high kicking, shooting, and splits (40; 62.5%), followed by sudden acceleration injuries (24; 37.5%) (Table 1). A total of 25 (39.1%) participants had complete injuries. Most of the injuries were PHAIs (49; 76.6%), with a median delay from injury to surgery of 12 days (interquartile range, 8.0-36.0 days) (Table 1). All patients, being professional athletes, were closely monitored and showed high compliance with the standardized rehabilitation protocol.
Characteristics of the 64 Professional Athletes Who Received Surgical Treatment of Their PHCIs a
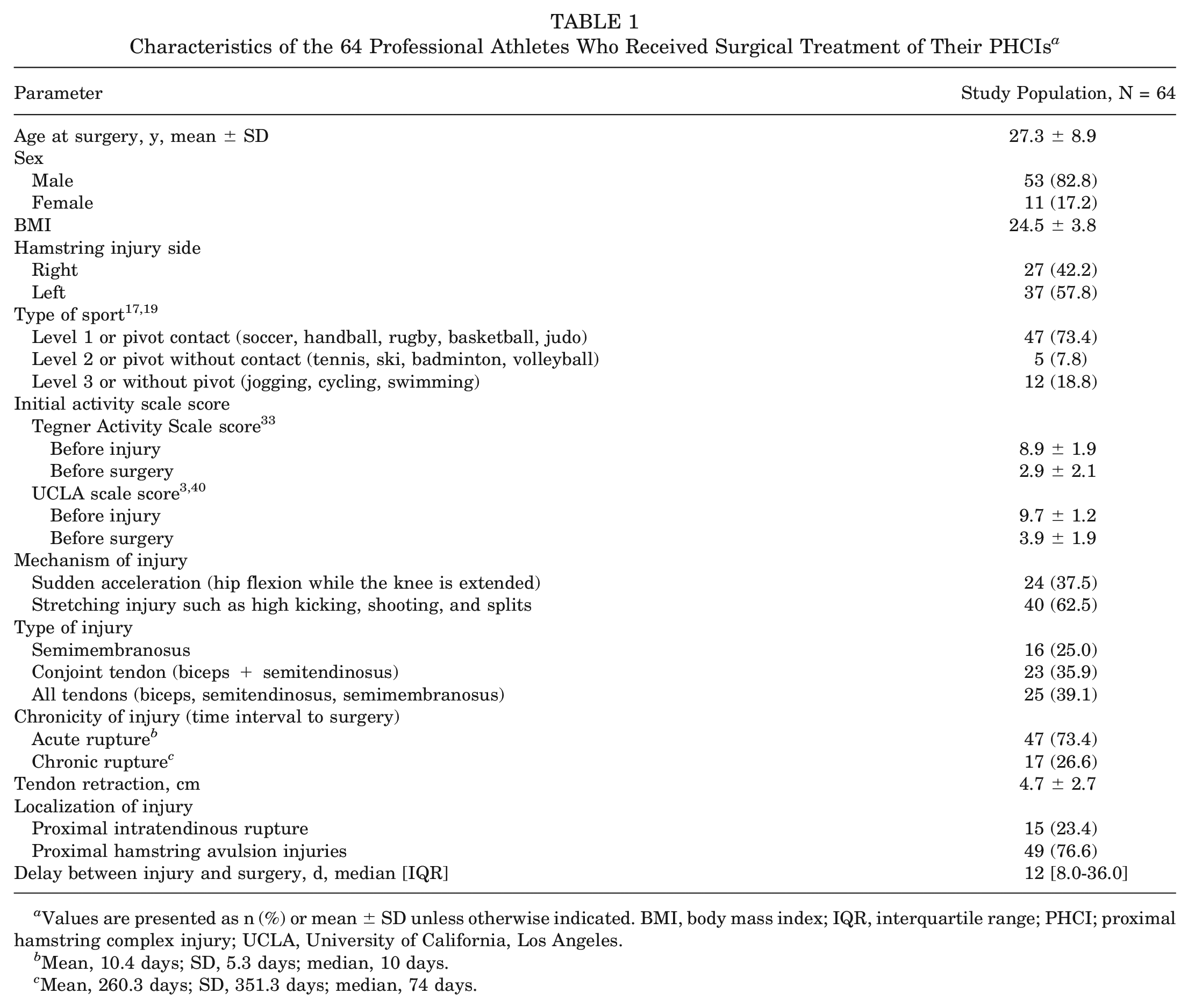
Values are presented as n (%) or mean ± SD unless otherwise indicated. BMI, body mass index; IQR, interquartile range; PHCI; proximal hamstring complex injury; UCLA, University of California, Los Angeles.
Mean, 10.4 days; SD, 5.3 days; median, 10 days.
Mean, 260.3 days; SD, 351.3 days; median, 74 days.
RTS Capabilities After PHCI
The mean time delay to RTS was 6.2 months (SD, 2.5 months). Most patients (63; 98.4%) returned to sports, and 62 (96.9%) of the athletes returned to their preinjury sport: 50 (78.1%) at their preinjury level of competition (maintained performance group) and 12 (18.8%) at an inferior level of performance. Two (3.1%) athletes were unable to continue in their preinjury sport. There was a significant improvement in activity scale scores at 1 year postoperatively, with TAS scores increasing from 2.9 (SD, 2.1) preoperatively to 8.5 (SD, 2.4) postoperatively (P < .0001). Similarly, UCLA scale scores significantly improved from 3.9 (SD, 1.9) preoperatively to 9.7 (SD, 0.8) postoperatively (P < .0001) (Table 2).
Return to Sport Capabilities After PHCI a
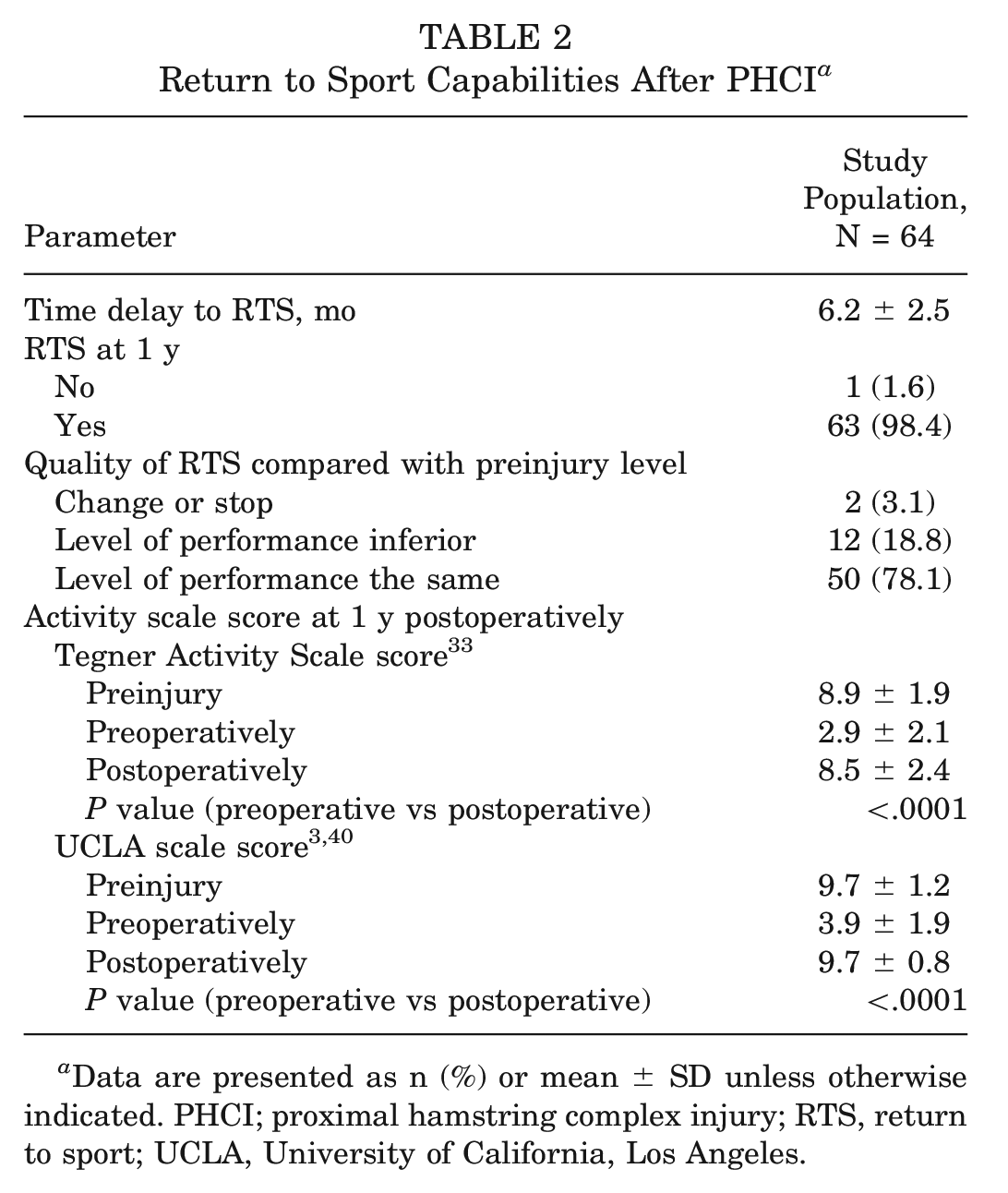
Data are presented as n (%) or mean ± SD unless otherwise indicated. PHCI; proximal hamstring complex injury; RTS, return to sport; UCLA, University of California, Los Angeles.
A subgroup analysis by type of sport showed variations of the mechanism of injury. Stretching injuries were more common in soccer and sprint athletics, while sudden acceleration injuries dominated in rugby, handball, combat sports, sports with splits, gymnastics, and others (Table 3). The quality of RTS also varied, with the highest performance (return to same preinjury level) in handball (3; 100%), sports with splits (3; 100%), and soccer (20/21; 95.2%). It was the lowest in the dance profession. Neither of the 2 dancers returned to their preinjury performance. One reported decreased performance, while the other discontinued her professional dancing career. In terms of RTS timing, the shortest mean time was seen in gymnastics (5.2 months; SD, 1.9 months) and the longest in combat sports (8.9 months; SD, 2.8 months). Players in most sports categories were capable of returning to sport at 1 year postoperatively, except for military personnel, where only 1 patient of 3 patients had returned to sport (Table 3).
RTS Capabilities After Proximal Hamstring Complex Injury by Professional Sports a
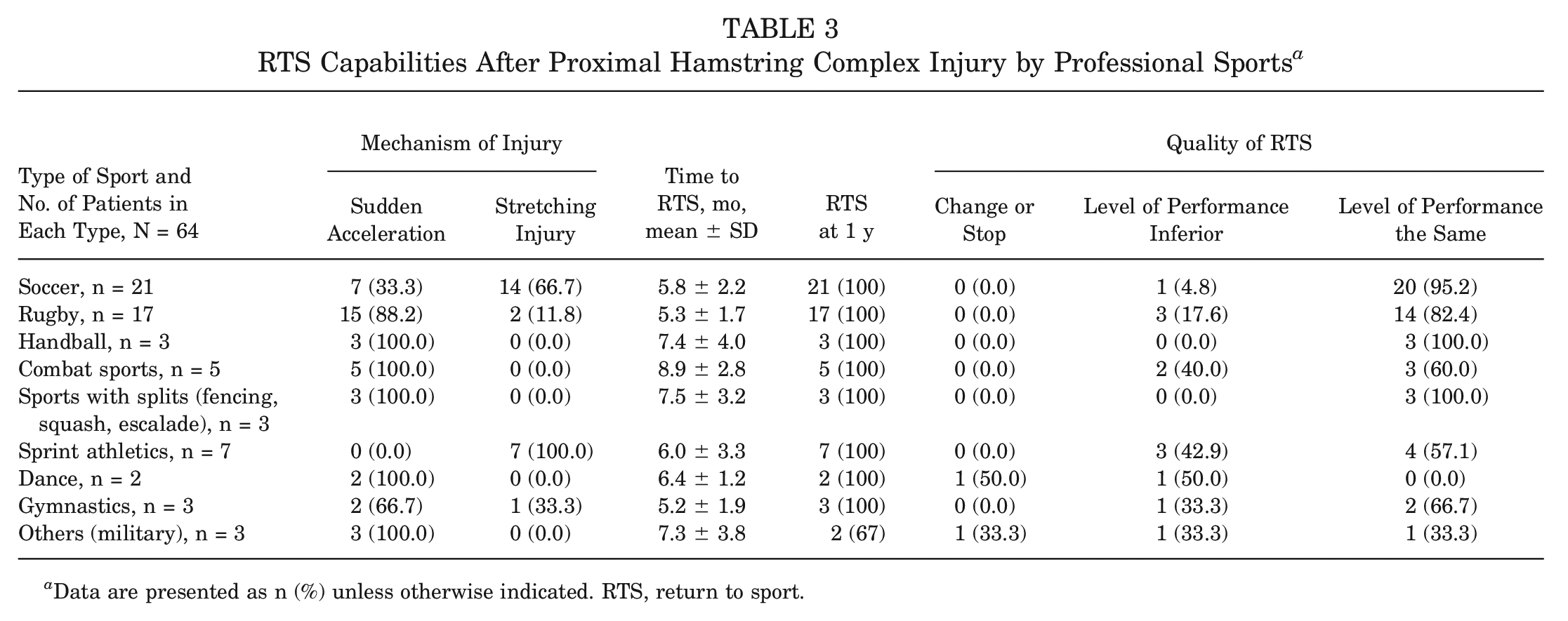
Data are presented as n (%) unless otherwise indicated. RTS, return to sport.
Univariate Regression Analysis for Potential Predictors of RTS
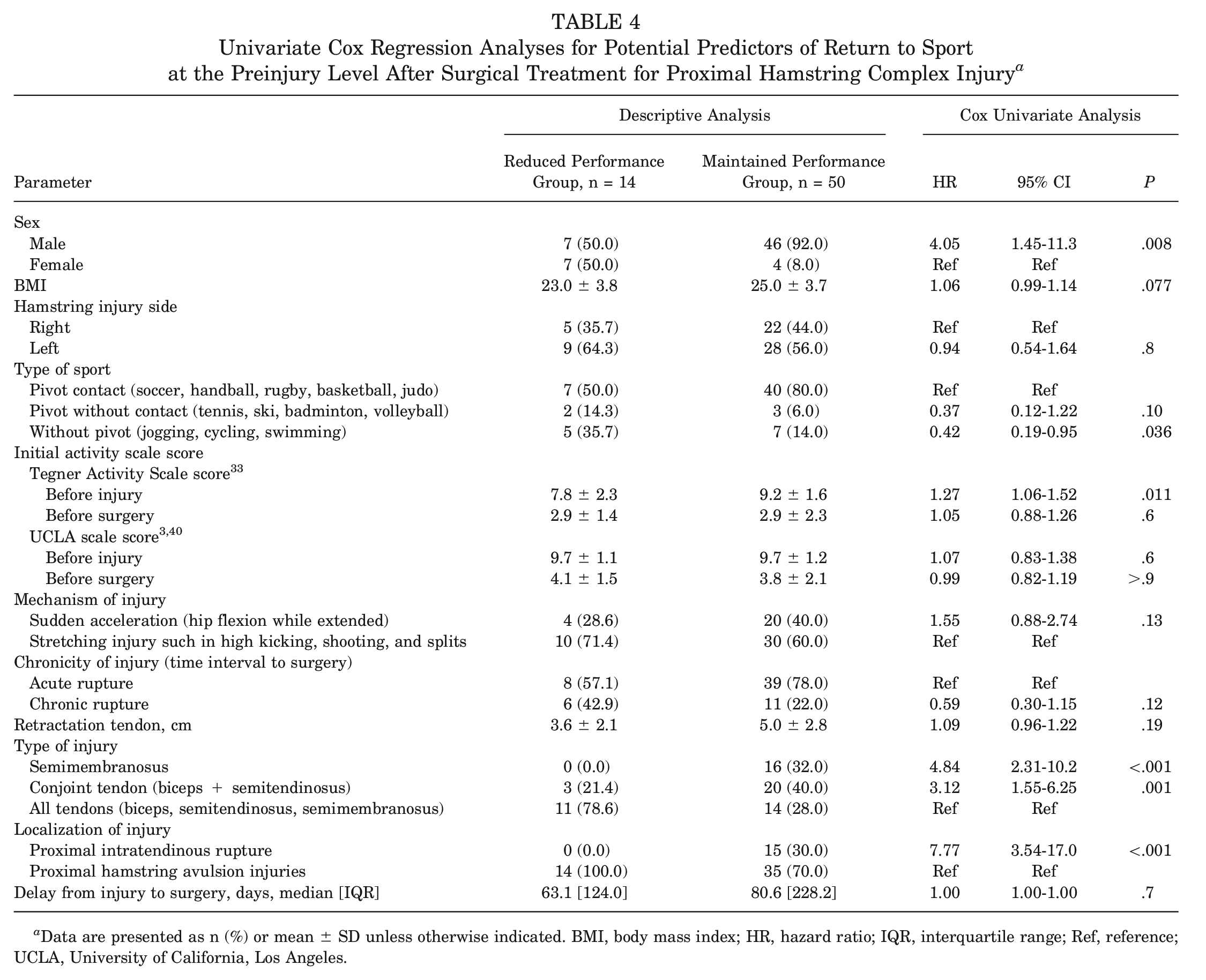
Age at surgery had a significant influence on the likelihood of returning to sport at the preinjury level (HR, 0.94; 95% CI, 0.91-0.98; P = .003), with older individuals less likely to return. Men showed a higher return likelihood than women (HR, 4.05; 95% CI, 1.45-11.3; P = .008). Body mass index and injury side did not significantly affect return likelihood (P = .077 and P = .8, respectively). Type of sport was a significant predictor, with nonpivot sports (jogging, bicycling, and swimming) athletes less likely to return than those in pivot contact sports (soccer, handball, rugby, basketball, and judo) (HR, 0.42; 95% CI, 0.19-0.95; P = .036). TAS score before injury was a significant predictor (HR, 1.27; 95% CI, 1.06-1.52; P = .011), but scores before surgery and UCLA scale scores were not significant predictors. Compared with an isolated semimembranosus injury, complete PHCI significantly decreased the likelihood of return (HR, 4.84; 95% CI, 2.31-10.2; P < .001). PHTR significantly increased return likelihood (HR, 7.77; 95% CI, 3.54-17.0; P < .001) compared with proximal hamstring avulsion injuries. Delay between injury and surgery was not a significant predictor (P = .7) (Table 4).
Univariate Cox Regression Analyses for Potential Predictors of Return to Sport at the Preinjury Level After Surgical Treatment for Proximal Hamstring Complex Injury a
Data are presented as n (%) or mean ± SD unless otherwise indicated. BMI, body mass index; HR, hazard ratio; IQR, interquartile range; Ref, reference; UCLA, University of California, Los Angeles.
Multivariate Regression Analysis for Potential Predictors of RTS
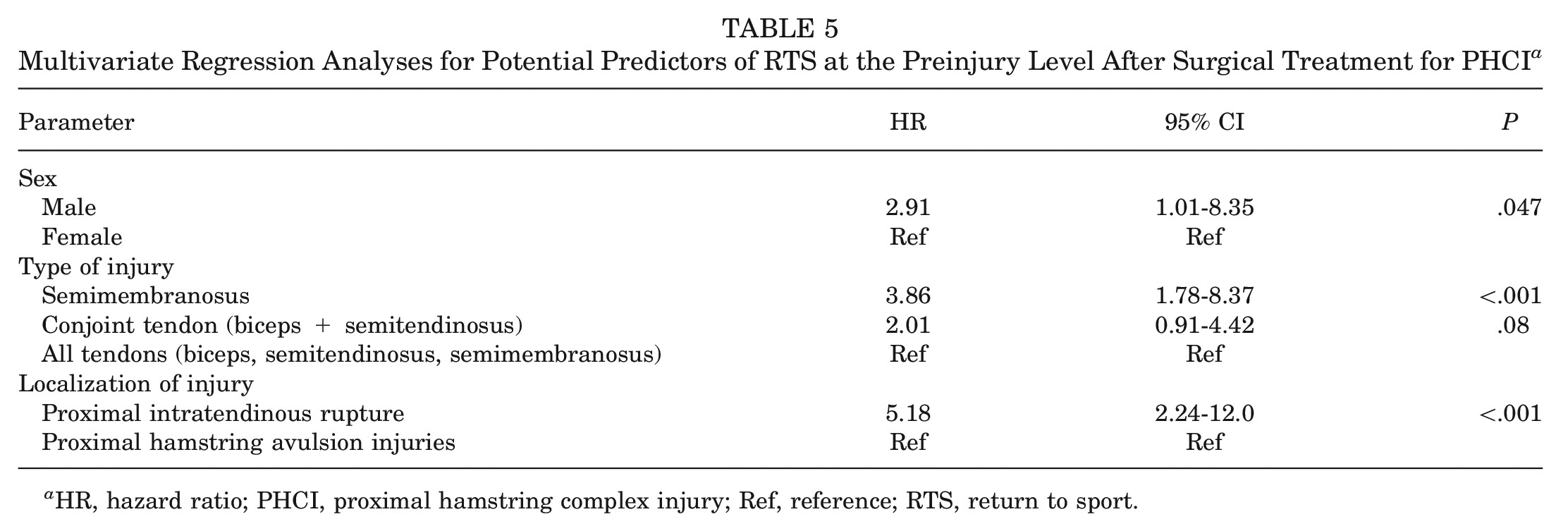
Sex, type of tendon injury, and location of injury were the only significant favorable predictors of RTS on the multivariable analysis. Men were 2.91 times more likely to return to their preinjury sports level than were women (HR, 2.91; 95% CI, 1.01-8.35; P = .047). Patients who had isolated semimembranosus injury were more likely to return to their preinjury sports level than those with complete PHCI (HR, 3.86; 95% CI, 1.78-8.37; P < .001). Furthermore, patients with a PHTR were 5.18 times more likely to return to their preinjury sports level than were those with a PHAI (95% CI, 2.24-12.0; P < .001) (Table 5).
Multivariate Regression Analyses for Potential Predictors of RTS at the Preinjury Level After Surgical Treatment for PHCI a
HR, hazard ratio; PHCI, proximal hamstring complex injury; Ref, reference; RTS, return to sport.
Complications
Three complications were reported, making up 4.7% of the population. These included 1 (1.6%) case of a superficial infection and 2 (3.1%) cases of rerupture.
Discussion
The main finding of our study was that most professional athletes surgically treated for PHCI demonstrated a high rate of RTS (78.1% returned to the same preinjury level in our study) before 1 year postoperatively, with the likelihood of successful RTS significantly influenced by, male sex, PHTR, and incomplete injuries (isolated semimembranosus injury).
RTS Capabilities
The high rates of RTS to the same preinjury level in our study may be attributable to the study’s focus on professional athletes, who may have greater motivation and readiness to RTS. Furthermore, our subgroup analysis showed that soccer and handball players exhibited the highest performance, with 95.2% to 100% of patients in the maintained performance group. This underlines the importance of considering the target population in assessing the outcomes of surgical treatment for PHCI. According to Belk et al, 9 the time to RTS after PHCI ranges from 4 to 11 months, with a weighted mean of 5.7 months. Their systematic review also found that 83.5% of patients were able to return to their preinjury activity level. Interestingly, 93.8% of the analyzed studies in their systematic review defined RTS as return to any sport, while we defined RTS by the preinjury level and activity scale scores (TAS and UCLA scale). van der Made et al 35 reported a lower rate of RTS seen in 20 of 26 (76.9%) patients, with a time to RTS ranging from 5 to 8.3 months. However, it is important to note that their study had a limited follow-up period of 1 year and a small proportion of professional athletes (8%), compared with recreational (50%) and competitive (38%) athletes.
Our data demonstrated significant improvement in UCLA scale and TAS scores. These findings are in line with most data from the literature. Kurowicki et al 23 showed a 3-point increase in the UCLA scale score in their series of endoscopic proximal hamstring repairs. Nevertheless, Lefèvre et al 25 demonstrated in their paper a return of both TAS and UCLA scale scores to their preinjury level after surgical repair.
Potential Predictors
Concerning the correlation with the completeness of injury, our results diverge from those of Belk et al, 9 who found no correlation with the timing of RTS. In contrast, we found that the extent of the injury significantly influenced the timing and quality of RTS, with complete injuries leading to longer recovery times and affecting the athlete’s postrecovery activity level and performance.
Lempainen et al 26 proposed that injuries to the biceps femoris, semimembranosus, and semitendinosus tendons should not be regarded equally and that a more nuanced approach is necessary to understand individual muscle-tendon injury in athletes. They suggested that each tendon should be addressed specifically, as different tendons may have different outcomes. Our results support this assertion, where we found that isolated semimembranosus injuries exhibited the best chance of RTS at the same preinjury level (HR, 3.86). Furthermore, our study highlighted the distinct nature of PHTR, which exhibited the best chance of RTS at the same preinjury level (HR, 5.18). Notably, outcomes of surgical repair of this entity are scarcely reported in the literature. This underscores the importance of our findings, as they shed light on an injury type that might be overlooked but has significant implications for recovery and RTS. It is noteworthy that the PHAI classification of Wood et al 39 did not include the distinct entity of PHTR. Pollock et al 30 investigated hamstring injuries in elite track and field athletes using the British Athletics Muscle Injury Classification based on MRI scans. They found that injuries extending into the free tendon (“c” classification) had a significantly longer recovery time and higher recurrence rate when treated nonoperatively. Our study provides insights into the potential benefits of surgical intervention for such injuries, suggesting a favorable prognosis with this approach. Comin et al 14 investigated hamstring injuries, specifically focusing on the central tendon. They found that patients in their study with a central tendon treated mainly nonoperatively (25% were surgically treated) had a significantly longer recovery period compared with those with muscle or musculotendinous injuries.
Complications
The rate of complications reported in our article is relatively low at 4.7%. Complications after PHCI such as rerupture, deep wound infection, neurogenic pain, weakness, general pain at the surgical site, and pain with sitting were all mentioned in the literature.13,18,36 Bodendorfer et al, 13 in their systematic review, reported a higher complication rate of 23.17%. They found that chronic repairs had more complications than acute repairs. In addition, they determined that repairing 1 or 2 tendons was associated with fewer complications when compared with complete repair. Similar results were reported by van der Made et al. 36
The originality of this study lies in its targeted population of professional athletes with PHCI. The percentage of professional athletes in previously published studies is highly variable, with the mean percentage being only 12.2% according to a systematic review by Jokela et al 21 in 2022. Mansour et al 27 were the only ones to report the outcomes in a study sample only formed of professional athletes with PHAI, with a reported RTS of 90%. However, it was limited by the small sample size (10 patients). Subbu et al 31 had a high percentage of professional athletes, at 56.3% (63/112 patients), with a RTS rate of 96.4%. Nonetheless, our study adds to the current literature by focusing solely on professional athletes with PHCI, with a larger sample size and a more comprehensive evaluation of RTS.
Limitations of the Study
Our study had limitations that need to be acknowledged. First, the sample size was limited because of the rarity of the pathology compared with other sports injuries. Although all patients in our study were professional athletes, the type of sport was very heterogeneous regarding the level of pivot and contact. We tried to mitigate these limitations by conducting subgroup analysis and multivariate Cox analysis to control for confounding variables. Other limitations included the lack of a control group and the monocentricity of the study. Another important consideration is that the determination of return to the previous level of performance was based predominantly on activity scale scores and the patients’ subjective impressions rather than on objective performance metrics such as minutes played, goals and assists, and so forth. Additionally, our study did not document the durability of RTS and performance, such as the longevity of an athlete’s career after his or her return. Despite these limitations, our study is one of the first of its kind to target only professional athletes with PHCI, and it provides important insights into the timing and quality of RTS in this category of patients as well as other outcomes.
Conclusion
Most professional athletes with PHCI were capable of returning to sport before 1 year postoperatively, with a high rate of RTS at their preinjury level, especially in soccer, handball, and sports with splits. The time to RTS differed significantly according to the level of competition and pivot in each sport. Our study found that male athletes, those with isolated semimembranosus injuries, and those with PHTR had a higher likelihood of returning to sport earlier after surgery.
Data Accessibility Statement
Data are available upon reasonable request.
Footnotes
Submitted June 2, 2023; accepted December 4, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: N.L. has received consulting fees from Websurvey Society. A.H. has received consulting fees from Arthrex and DePuy. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.