
Abstract
Background:
New techniques have been proposed to better address anteromedial rotatory instability in a medial collateral ligament (MCL)–injured knee that require an extra graft and more surgical implants, which might not be feasible in every clinical setting.
Purpose:
To investigate if improved resistance to anteromedial rotatory instability can be achieved by using a single-graft, double-bundle (DB) MCL reconstruction with a proximal fixation more anteriorly on the tibia, in comparison with the gold standard single-bundle (SB) MCL reconstruction.
Study Design:
Controlled laboratory study.
Methods:
Eight fresh-frozen human cadaveric knees were tested using a 6 degrees of freedom robotic simulator in intact knee, superficial MCL/deep MCL–deficient, and reconstruction states. Three different reconstructions were tested: DB MCL no proximal tibial fixation and DB and SB MCL reconstruction with proximal tibial fixation. Knee kinematics were recorded at 0°, 30°, 60°, and 90° of knee flexion for the following measurements: 8 N·m of valgus rotation (VR), 5 N·m of external tibial rotation, 5 N·m of internal tibial rotation, combined 89 N of anterior tibial translation and 5 N·m of external rotation for anteromedial rotation (AMR) and anteromedial translation (AMT). The differences between each state for every measurement were analyzed with VR and AMR/AMT as primary outcomes.
Results:
Cutting the superficial MCL/deep MCL increased VR and AMR/AMT in all knee positions except at 90° for VR (P < .05). All reconstructions restored VR to the intact state except at 90° of knee flexion (P < .05). The DB MCL no proximal tibial fixation reconstruction could not restore intact AMR/AMT kinematics in any knee position (P < .05). Adding an anterior-based proximal tibial fixation restored intact AMR/AMT kinematics at ≥30° of knee flexion except at 90° for AMT (P < .05). The SB MCL reconstruction could not restore intact AMR/AMT kinematics at 0° and 90° of knee flexion (P < .05).
Conclusion:
In this in vitro cadaveric study, a DB MCL reconstruction with anteriorly placed proximal tibial fixation was able to control AMR and AMT better than the gold standard SB MCL reconstruction.
Clinical Relevance:
In patients with anteromedial rotatory instability and valgus instability, a DB MCL reconstruction may be superior to the SB MCL reconstruction, without causing extra surgical morbidity or additional costs.
Keywords
The medial collateral ligament (MCL) is a commonly injured knee structure.14,20,29,35 High-grade MCL injuries can occur alone but are frequently accompanied by an anterior cruciate ligament (ACL) rupture.14,20,29,35 Clinically, patients with an MCL injury will present with valgus and/or rotational laxity in the form of an anteromedial rotatory instability (AMRI).3,4,10,13,27,33 Although the MCL has a good healing capacity, some patients will have residual MCL laxity after nonoperative management.1,18,29 Previous work in our laboratory showed that a partial MCL injury increases the load on the ACL by 127% during external rotation (ER) at 30° of knee flexion compared with an MCL-intact knee. 5 Consequently, when residual laxity is present after a healed MCL injury, the load on the ACL or ACL graft will be increased. This might explain why revision rates after ACL reconstruction (ACLR) in patients with a concomitant nonoperatively managed MCL lesion are higher compared with those in patients with isolated ACL injury.1,29 Following these newer insights and analogous to the reduced ACLR revision rates found after addressing anterolateral rotatory laxity, there is an increased interest in AMRI and its treatment.3 -6,9,22,23,33
AMRI is controlled by both the superficial MCL (sMCL) and the deep MCL (dMCL) in knee extension3,4,33; however, the sMCL becomes more important in knee flexion.3,4,33 Moreover, previous work in our laboratory showed that a partial sMCL injury had an additive effect on anteromedial rotation (AMR) compared with an isolated dMCL injury in knee flexion. 4 Because the sMCL is also the primary restraint to valgus rotation (VR), the main goal of an MCL reconstruction should be to mimic the sMCL behavior.3 -5,10,33
The single-bundle (SB) MCL reconstruction, as described by LaPrade and Wijdicks, 17 is often seen as the gold standard. However, the sMCL is a broad, flat diamond-like structure, and the dMCL is a capsular thickening running in an oblique anteromedial direction. 16 Therefore, an SB graft might not be suitable to fully restore native MCL kinematics.16,17 Recently, the ability of an SB sMCL reconstruction to control AMRI has been questioned.6,22,23 New surgical techniques have been proposed with the aim of controlling AMRI by adding an oblique anteromedial graft to an SB or flat sMCL reconstruction.6,22,23 However, for these combined techniques, there is a need for an extra graft, which can be problematic in multiligament knee reconstructions, especially in surgical settings where there is no access to allografts.6,22,23,28 Furthermore, extra tunnels in the tibia and femur increase the risk of tunnel coalition, and extra surgical steps lead to more potential pitfalls and longer surgical time.6,22,23 Therefore, these techniques may unnecessarily increase the morbidity associated with an MCL reconstruction. To overcome these downfalls, the senior author (A.G.) developed a single-graft, double-bundle (DB) MCL reconstruction with a more anteriorly placed proximal fixation of the anterior bundle on the tibia than that of the gold standard SB MCL reconstruction. The anterior bundle therefore runs more obliquely, which is intended to help control AMRI. This modification on the gold standard SB MCL reconstruction avoids the above-mentioned extra surgical morbidity.
It would be of clinical value if this DB MCL reconstruction showed that it can control AMRI better than the SB MCL reconstruction. The purpose of this study was therefore to investigate the differences in controlling knee joint laxity, especially AMRI, between a DB MCL reconstruction no proximal tibial fixation (NoPF) and an SB and DB MCL reconstruction with proximal tibial fixation. We hypothesized that the single-graft, DB MCL reconstruction restores AMRI better than the gold standard SB MCL reconstruction.
Methods
Eight fresh-frozen human cadaveric knee specimens (1 pair; 6 male, 2 female) without a history of injury, surgery, osteoarthritis, or meniscal pathology were used for this study. The mean donor age was 63 years (range, 49-67 years), the mean height was 170 cm, the mean weight was 54.8 kg, and the mean body mass index was 18.9. This study was approved by the institutional research ethics board.
Apparatus and Specimen Preparation
A 6 degrees of freedom joint motion simulator was used for the biomechanical testing (VIVO; Advanced Mechanical Technologies Inc). Specimens were thawed at room temperature over a 24-hour period before testing. The proximal femur and distal tibia/fibula were denuded from soft tissues while leaving all tissues within 150 mm of the transepicondylar axis intact. We previously described the potting and mounting technique onto the joint motion simulator.25,31 Two optical motion trackers (Optotrak; Northern Digital) with 0.1-mm/0.3° accuracy were fixed to the femur and tibia. Each specimen’s femur and tibia/fibula were segmented and reconstructed from the computed tomography images (3D Slicer; http://www.slicer.org/), and the models were co-registered to the specimens. The femur was positioned on the joint motion simulator with the aid of a model-guided motion-capture alignment technique, using the co-registered reconstructions of the femur and tibia. The flexion axis of the femur was defined as a line passing through the centers of spheres fitting the posterior femoral condyles. The femur was positioned on the machine such that the midpoint of that line was positioned at the femoral mechanical center of rotation of the machine and was oriented such that the tibia was vertical with the femur in extension and in flexion, which minimized unwanted secondary motions. 34 The tibia was oriented and potted vertically in the coronal and sagittal planes. A purely compressive load (100 N), parallel to the long axis of the tibia, was applied onto the joint with the specimen in full extension, while all other degrees of freedom were unconstrained. The resulting pose was defined as the reference pose; all joint kinematics were measured relative to this pose by the joint motion simulator using Grood and Suntay coordinate conventions. 11
Biomechanical Testing
Before data collection, each specimen was preconditioned by repeating the entire loading sequence for 5 test cycles to reduce tissue hysteresis. Tibiofemoral kinematics were measured with the joint flexion angle fixed at 0°, 30°, 60°, and 90° under a compressive load of 50 N. Valgus laxity was measured using an 8-N·m VR torque. ER and internal rotation (IR) laxities were measured using 5-N·m rotation torques. Anteromedial laxity was measured using the maximal anteromedial translation (AMT) referencing the center of the medial tibial plateau and maximal tibial ER (AMR) after applying a combined anterior-directed force (89 N) and external torque (5 N·m) to the tibia. The middle of the medial tibial plateau, defined on the reconstructed computed tomography images, was the point at 50% of the distance in both the anteroposterior direction and the mediolateral direction on the medial tibial plateau. The loads used were in line with those used in previous studies investigating medial knee biomechanics.3,10,26,33 Each load was applied and removed over an approximately 30-second period. The resulting kinematics were recorded with a camera capturing the femoral and tibial optical motion trackers. The maximal achievable rotation/displacement was measured relative to the specimens’ corresponding neutral position. Each test was repeated sequentially for a total of 5 cycles. The mean of the second, third, and fourth tests was used as the final laxity output. Data from the first and fifth cycles were not used to limit possible beginning- and end-of-cycle behavior effects. The specimen was unmounted once to create the medial-side injury and to drill the bone tunnels; all subsequent surgical steps were done while keeping the specimen mounted on the joint motion simulator to reduce possible repositioning inaccuracies. After DB MCL reconstruction, the graft was preconditioned during another 5 test cycles without data recording to reduce hysteresis of the MCL reconstruction.
Dissection Technique
All surgical procedures were conducted by the same trained orthopaedic sport fellows (W.B., T.V.) supervised by the senior author. The medial side was approached through a longitudinal skin incision. The sartorial fascia was opened, and the hamstring tendons were released from the insertion to visualize the medial structures. The MCL injury was created by releasing the sMCL from its distal tibial insertion, dissected and removed up to its femoral origin. The anterior border was the anteromedial capsule, and the posterior border was the anterior margin of the anterior arm of the posterior oblique ligament (POL). 16 The dMCL was severed by cutting both the meniscofemoral and meniscotibial divisions. 16 The resulting MCL injury was in line with the injury created in previous studies investigating the biomechanics of different MCL reconstructions.6,22,23 Injury to the POL and posteromedial joint capsule can cause a posteromedial instability25,26 and therefore lies outside the scope of this study.
Surgical Technique
Previously obtained peroneus longus soft tissue grafts were used for the MCL reconstructions. The graft properties from a peroneus longus graft and a semitendinosus graft are similar. 21 The diameter of the peroneus longus graft was adapted, if needed, to create consistent bone tunnel diameters that were similar to those used in MCL reconstructions with a semitendinosus tendon graft. The peroneus longus graft was doubled and whipstitched with 2 No. 2 high-strength sutures (Ultrabraid; Smith & Nephew Inc) on each side. The minimal doubled graft length was 14 cm. The tibial and femoral ends had diameters of 6 and 7 mm, respectively. The graft was pretensioned to 60 N over a minimal period of 20 minutes.
Three different MCL reconstructions were created using the same graft. The surgical steps did not allow a randomized testing order. The testing order was (1) DB MCL NoPF, (2) DB MCL, and (3) SB MCL. All 3 reconstructions used the same femoral and tibial tunnels. On the tibia, a tunnel of 6 mm in diameter was created 60 mm below the joint line at the posterior aspect of the sMCL insertion. 17 On the femur, a 2.4-mm eyelet pin was drilled at the level of the femoral MCL insertion referencing 12 mm distal and 8 mm anterior of the adductor tubercle. 17 Isometry was ensured before subsequently drilling a 4.5-mm tunnel to the lateral cortex and a 7-mm socket on the medial cortex. Both exits on the lateral cortex of the tibial and femoral tunnels were denuded from soft tissue to ensure correct deployment of the tensioning device and cortical button (Endobutton; Smith & Nephew Inc), respectively.
The first reconstruction, DB MCL NoPF, which restores only the sMCL, was a DB peroneus longus graft without a proximal fixation onto the tibia (Figure 1A). The DB peroneus longus graft was fixed first on the femoral side with an 8 × 25–mm interference screw (Biosure; Smith & Nephew Inc) and backed up with a cortical button on the lateral femoral cortex. The graft was then docked in the tibial tunnel and fixed on a tensioning device using a cortical button. The tensioning device consisted of a 3-dimensional printed custom-made tool that was seated on the lateral tibial cortex, wherein a 50-kg capacity bending-beam load cell (CZL635; Phidgets) with an accuracy of <1 N was fixed and measured applied tension (Figure 2). The graft was tensioned to 60 N with the knee in 30° of flexion, 2 N·m of varus load, and neutral rotation. As previously mentioned, the specimen/reconstruction was again preconditioned by repeating the entire loading sequence to reduce hysteresis of the subsequent MCL reconstructions. The graft was retensioned to 60 N with the knee held in the exact same position as originally, before performing an actual test run.
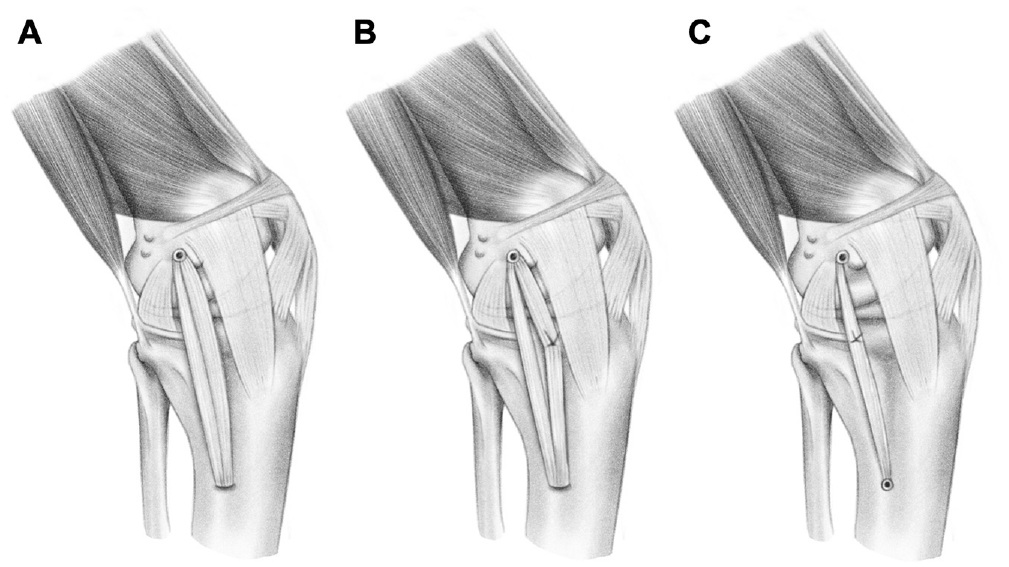
The 3 different medial collateral ligament (MCL) reconstructions are shown using the same femoral and tibial insertion as described by LaPrade and Wijdicks. 17 (A) Shows the double-bundle (DB) MCL no proximal fixation reconstruction. (B) Shows the DB MCL reconstruction. The most anterior bundle is fixed on an anteriorly placed anchor, creating a diamond-like shape. (C) Shows the single-bundle (SB) MCL reconstruction. The SB is fixed to a proximal tibial anchor deployed just anterior from the anterior arm of the semimembranosus tibial attachment. 17 The distance between the 2 proximal anchors is ±10 mm.
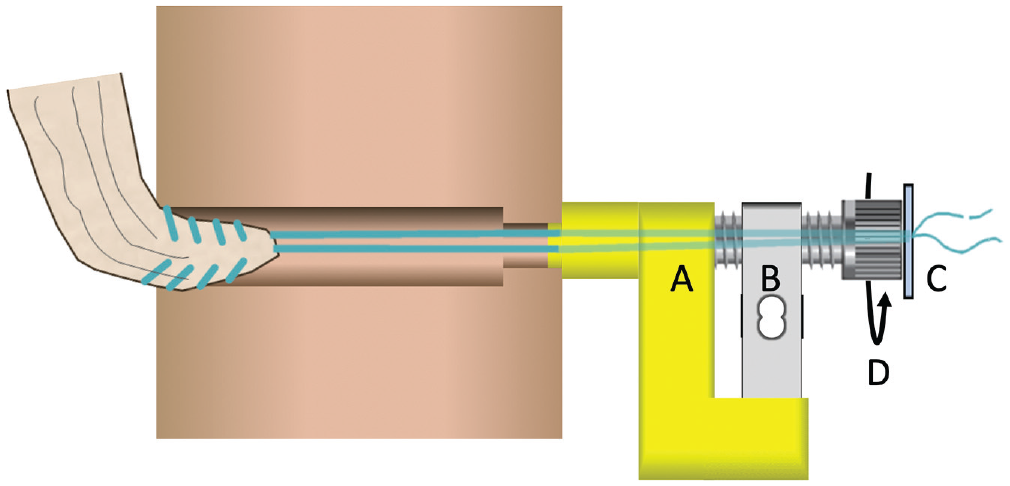
The tensioning device is mounted on the lateral cortex of the tibia, with a 3-dimensional printed custom-made mount (A) for the load cell (B). The mount is tapered down to fit in the exit of the tibial tunnel. The 2 high-strength sutures, which are whipstitched on the tibial side of the graft, are shuttled through the tibial tunnel and tensioning device. They are then tied over a cortical button (C). The load cell is connected with a computer to allow a digital readout of the load applied. A cannulated screw is unscrewed (D), which increases the distance between the cortical button and the tibia, and thus increases the load applied until 60 N tension is achieved.
The second reconstruction, DB MCL, was a DB peroneus longus graft with proximal fixation on the tibia using a double-loaded 3.5-mm suture anchor (Twinfix Ultra Titanium; Smith & Nephew Inc) (Figure 1B). Before anchor placement, the graft was retensioned to 60 N with the knee held in the exact same position as for the previous reconstruction. The anchor was deployed with the knee in neutral rotation and 90° of knee flexion, at a position 12 mm distal from the joint line and 5 mm anterior from the most anterior bundle. The anterior bundle was sutured on the anchor using 2 No. 2 high-strength sutures (Ultrabraid). It was important that the anchor not be moved >5 mm anteriorly on the tibia because this would overconstrain the specimen in ER and AMR compared with intact, as observed in pilot tests (n = 2).
The third reconstruction, SB MCL, was the MCL reconstruction as described by LaPrade and Wijdicks 17 (Figure 1C). The previous anterior anchor was released from the anterior bundle. The graft was retensioned to 60 N at the same position as previously described. A 6 × 20–mm interference screw (Biosure) was inserted into the tibial tunnel. This permitted cutting 1 bundle of the graft without losing tension in the remaining bundle. The SB graft was sutured on a double-loaded 3.5-mm suture anchor (Twinfix Ultra Titanium), deployed with the knee in neutral rotation and 90° of knee flexion, at a position 12 mm distal from the joint line directly anterior to the anterior arm of the semimembranosus tibial attachment. 17 The second anchor was ±10 mm posterior from the first.
Statistical Analysis
Statistical analysis was performed using statistical software (GraphPad Prism 9; Dotmatics). A 2-factor (flexion angle and state) repeated-measures analysis of variance was performed to compare each state with every other state. A post hoc Bonferroni correction was used to correct for multiple comparisons. Based on recent publications on medial-side reconstructions, a 2° change in ER could be detected with 80% power and 95% confidence using 7 specimens.6,22 The results are reported as mean ± SD; in degrees for VR, ER, IR and AMR; and in millimeters for AMT. Statistical significance was set at P < .05 (adjusted P value after Bonferroni correction).
Results
Detailed mean increases ± SD for each state compared with each other state, as well as the exact P values, are listed in the Appendices (available in the online version of this article).
Anteromedial Rotation
The mean AMR of the intact knee ranged from 13.2° to 22.8° between 0° and 90° of flexion (Figure 3). In the MCL-deficient state, there was a significant increase in AMR compared with the intact state in all flexion angles (mean Δ, 3.7°-12.9°; P < .05). In extension, no reconstruction was able to restore intact kinematics (mean Δ with respect to intact state, 4.2°-4.4°; P < .05). Furthermore, the DB MCL NoPF reconstruction showed a significant increase compared with the intact state in flexion (mean Δ, 4.6°-10.7°; P < .05). The DB MCL reconstruction restored the AMR closest to intact kinematics with no significant difference compared with intact kinematics at 30° to 90° and significant decreases compared with the MCL-deficient state at 60° and 90° of knee flexion (mean Δ, –9.0°, P = .023; and −9.1°, P = .005, respectively). At 30° and 60° of knee flexion, the AMR did not differ significantly in the SB MCL reconstruction compared with intact but also did not differ significantly from the MCL-deficient state. At 90° of knee flexion, AMR increased significantly in the SB MCL reconstruction compared with the intact state (mean Δ, 6.5°; P = .021). All reconstructions did not differ significantly from each other, except for the DB MCL reconstruction, which decreased AMR significantly at 90° of knee flexion compared with the DB MCL NoPF reconstruction (mean Δ, –6.9°; P = .006).
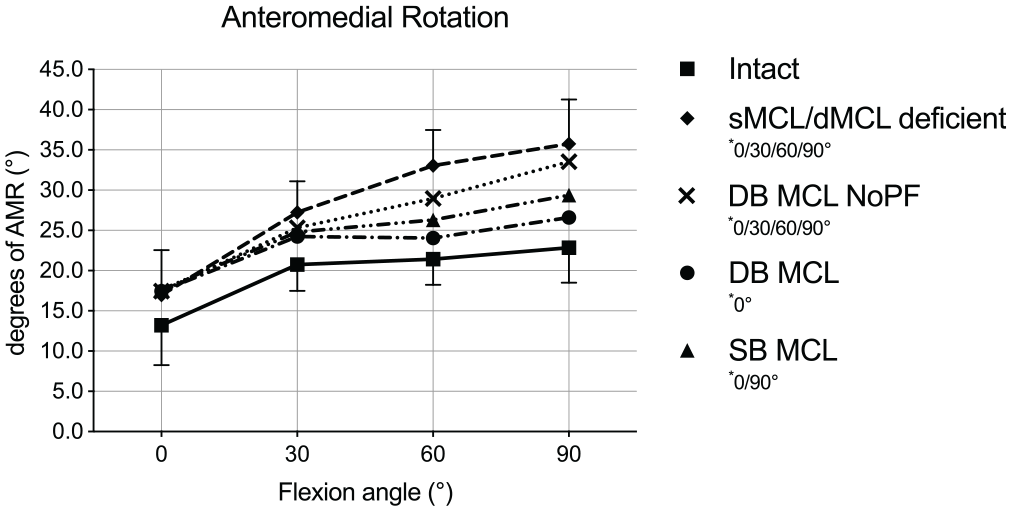
Anteromedial rotation (AMR) in degrees in response to 5 N·m of external rotation torque plus 89 N of anterior tibial translation force for each knee flexion angle in the medial collateral ligament (MCL) intact and deficient states, as well as for all 3 different MCL reconstructions. Results are shown as mean ± SD. The asterisk indicates a significant difference (P < .05) for each state compared with the intact state in the indicated flexion angles. DB, double bundle; dMCL, deep MCL; NoPF, no proximal fixation; SB, single bundle; sMCL, superficial MCL.
Anteromedial Translation
The mean AMT from the intact knee ranged from 7.5 to 12.5 mm between 0° and 90° of flexion (Figure 4). In the MCL-deficient state, there was a significant increase in AMT compared with the intact state in all knee positions (mean Δ, 2.4-8.8 mm; P < .05). In extension and at 90° of knee flexion, no reconstruction was able to restore intact kinematics (P < .05). Furthermore, the DB MCL NoPF reconstruction could not restore intact kinematics at 30° and 60° of knee flexion (mean Δ with respect to intact state, 3.2 mm, P = .030; and 5.3 mm, P = .014, respectively). The DB MCL reconstruction restored the AMT closest to intact kinematics with a significant decrease compared with the MCL-deficient state at 60° and 90° of knee flexion (mean Δ, –5.2 mm, P = .049; and −5.5 mm, P = .011, respectively). The SB MCL did not show any difference compared with the MCL-deficient state in any knee position (P > .05). All reconstructions did not differ significantly from each other except for the DB MCL reconstruction, which decreased AMT significantly at 90° of knee flexion compared with the DB MCL NoPF reconstruction (mean Δ, –4.4 mm; P = .012).
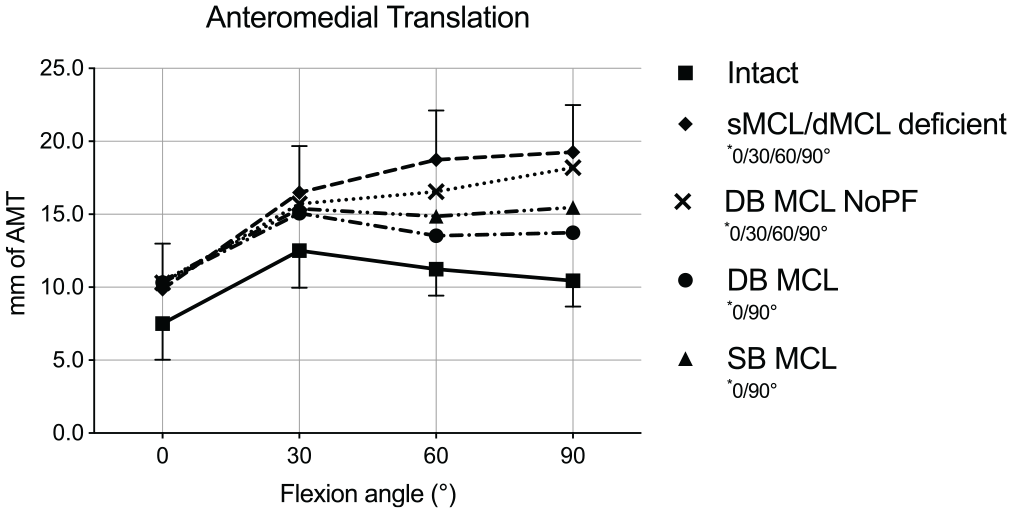
Anteromedial translation (AMT) in millimeters in response to 5 N·m of external rotation torque plus 89 N of anterior tibial translation force as measured from the middle of the medial tibial plateau for each knee flexion angle in the medial collateral ligament (MCL) intact and deficient states, as well as for all 3 different MCL reconstructions. Results are shown as mean ± SD. The asterisk indicates a significant difference (P < .05) for each state compared with the intact state in the indicated flexion angles. DB, double bundle; dMCL, deep MCL; NoPF, no proximal fixation; SB, single bundle; sMCL, superficial MCL.
External Rotation
The mean ER from the intact knee ranged from 13.1° to 24.2° between 0° and 90° of flexion (Figure 5). In the MCL-deficient state, there was a significant increase in ER compared with the intact state at all flexion angles (mean Δ, 3.4°-11.3°; P < .05). In extension, no reconstruction was able to restore intact kinematics (mean Δ with respect to intact state, 3.9°-4.1°; P < .05). Furthermore, the DB MCL NoPF reconstruction showed a significant increase compared with the intact state at 60° and 90° (mean Δ, 6.0°, P = .031; and 8.9°, P = .002, respectively). The DB MCL reconstruction restored the ER closest to intact kinematics with no significant difference compared with intact kinematics at 30° to 90° and a significant decrease compared with the MCL-deficient state at 60° and 90° of knee flexion (mean Δ, –8.8°, P = .011; and −8.1°, P = .004, respectively). At 30° and 60° of knee flexion, the ER did not differ significantly in the SB MCL reconstruction compared with intact, but it also did not differ significantly from the MCL-deficient state. At 90° of knee flexion, ER increased significantly in the SB MCL reconstruction compared with intact state (mean Δ, 5.6°; P = .031). All reconstructions did not differ significantly from each other except for the DB MCL reconstruction, which decreased ER significantly at 90° of knee flexion compared with the DB MCL NoPF reconstruction (mean Δ, –5.8°; P = .008).
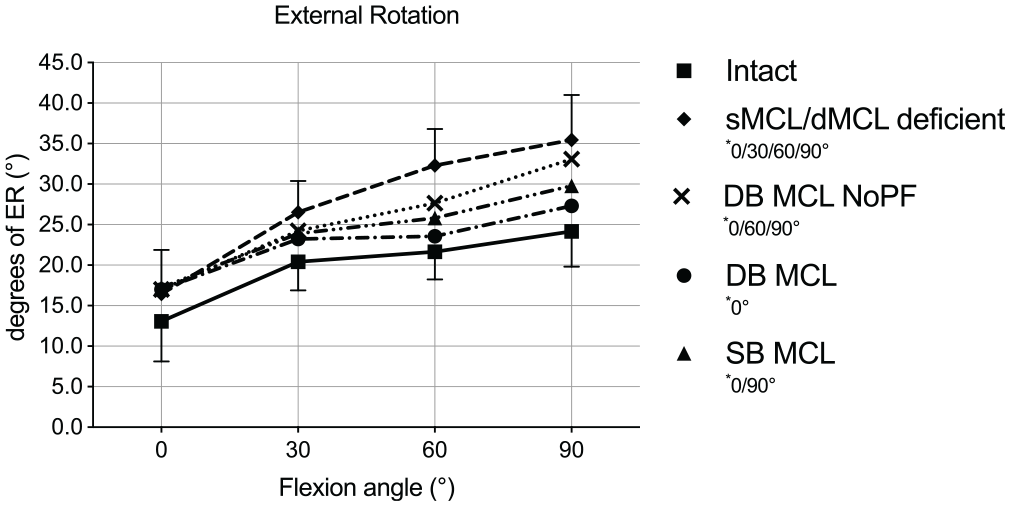
External rotation (ER) in degrees in response to 5 N·m of ER torque for each knee flexion angle in the medial collateral ligament (MCL) intact and deficient states, as well as for all 3 different MCL reconstructions. Results are shown as mean ± SD. The asterisk indicates a significant difference (P < .05) for each state compared with the intact state in the indicated flexion angles. DB, double bundle; dMCL, deep MCL; NoPF, no proximal fixation; SB, single bundle; sMCL, superficial MCL.
Internal Rotation
The mean IR from the intact knee ranged from 11.9° to 20.1° between 0° and 90° of flexion (Figure 6). Despite the smaller changes compared with the other measured kinematics, there were some small significant changes in IR found. In the MCL-deficient state, there was a significant increase in IR compared with intact kinematics at 60° of knee flexion (mean Δ, 1.6°; P = .003). IR increased in the DB MCL NoPF reconstruction at 60° and 90° compared with the intact state (mean Δ, 1.9°, P = .048; and 1.5°, P = .029, respectively). The DB MCL reconstruction showed a significant increase in IR compared with the intact state at 90° of knee flexion (mean Δ, 1.6°; P = .043). In the SB MCL reconstruction, IR increased significantly at 90° of knee flexion compared with the intact state (mean Δ, 1.6°; P = .043). All reconstructions did not differ significantly from each other except for the SB MCL, which decreased IR significantly at 30° of knee flexion compared with the DB MCL NoPF (mean Δ, 3.2°; P = .032).
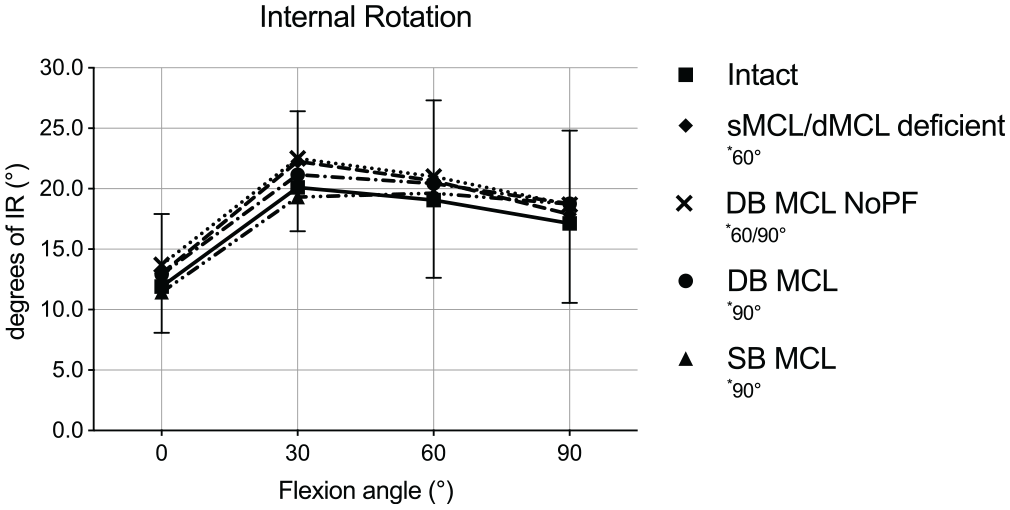
Internal rotation (IR) in degrees in response to 5 N·m of IR torque for each knee flexion angle in the medial collateral ligament (MCL) intact and deficient states, as well as for all 3 different MCL reconstructions. Results are shown as mean ± SD. The asterisk indicates a significant difference (P < .05) for each state compared with the intact state in the indicated flexion angles. DB, double bundle; dMCL, deep MCL; NoPF, no proximal fixation; SB, single bundle; sMCL, superficial MCL.
Valgus Rotation
The mean VR from the intact knee ranged from 2.4° to 4.1° between 0° and 90° of flexion (Figure 7). In the MCL-deficient state, there was a significant increase in VR compared with the intact state at all knee positions except at 90° of knee flexion (mean Δ, 3.9°-6.3°; P < .05). All reconstructions were able to restore intact kinematics at 0° to 60° of knee flexion. At 90° of knee flexion, compared with the intact state, the largest mean increase was seen in the MCL-deficient state (mean Δ, 2.8°; P = .30); However, the increase was only statistically significant between all the reconstructions and the intact state (mean Δ, 1.9°-2.3°; P < .05).
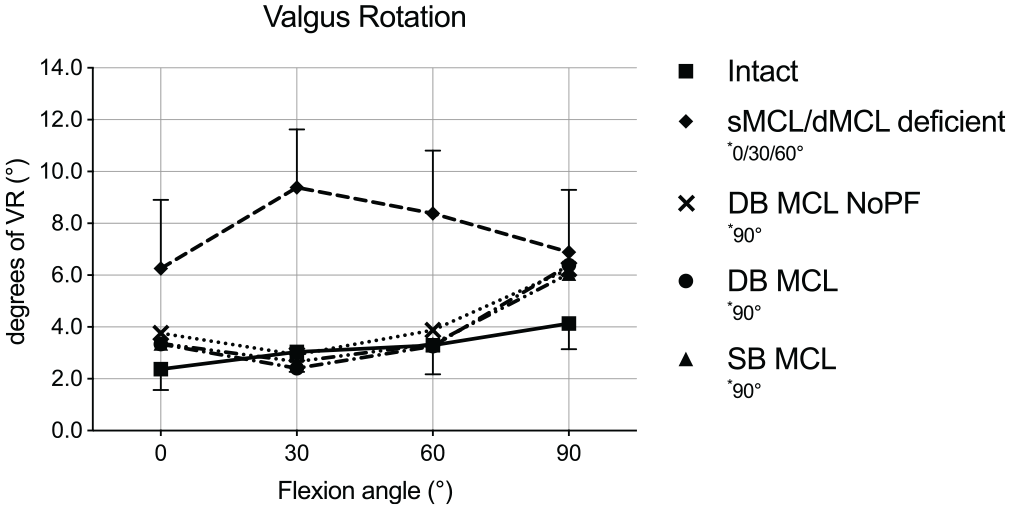
Valgus rotation (VR) in degrees in response to 8 N·m of VR torque for each knee flexion angle in the medial collateral ligament (MCL) intact and deficient states, as well as for all 3 different MCL reconstructions. Results are shown as mean ± SD. The asterisk indicates a significant difference (P < .05) for each state compared with the intact state in the indicated flexion angles. DB, double bundle; dMCL, deep MCL; NoPF, no proximal fixation; SB, single bundle; sMCL, superficial MCL.
Discussion
The most important finding of this in vitro cadaveric biomechanical study was that a single-graft, DB MCL reconstruction with an anteriorly placed proximal tibial fixation controlled AMRI better than the gold standard SB MCL reconstruction, particularly at 60° and 90° of knee flexion. The proximal fixation on the tibia was found to be important to reduce AMRI in both reconstructions but did not influence VR. Moving the proximal fixation more anteriorly on the tibia further reduced AMRI. In extension, however, AMRI was not controlled to the same extent as the intact knee in any of the tested reconstructions.
The SB anatomic MCL reconstruction, which has long been seen as the gold standard, has recently been discussed as being unsuitable to control AMRI.3,6,17,22,33 Two independent biomechanical studies showed that an SB MCL reconstruction was not able to restore intact kinematics in AMR or AMT in all flexion angles except in knee extension.6,23 In contrast, the results of this study showed that the SB MCL reconstruction was able to control AMRI better in knee flexion than what has been reported in the recent literature; however, it could not restore intact kinematics at 0° and 90° of knee flexion. The difference could be related to small changes in surgical technique (femoral/tibial tunnel position or use of suture tape instead of soft tissue graft) compared with the original description by the above-named studies, which may affect control of the AMRI.6,17,23
New surgical techniques have been proposed to improve the restoration of native AMR kinematics in MCL reconstructions.6,22 Behrendt et al 6 found that a combination of an SB MCL reconstruction and an extra, more oblique running graft, the so-called anteromedial reconstruction, restored the kinematics to intact in all knee positions. In agreement, Miyaji et al 22 found that AMRI could be well controlled with their combined anteromedial and SB MCL reconstruction. Alternative to these 2-graft techniques, our DB MCL reconstruction with an anterior-based proximal tibial fixation restored AMR/AMT to intact kinematics in ≥30° of knee flexion except for AMT at 90° of flexion. Compared with the study by Behrendt et al, the mean differences in AMT between the intact state and the DB MCL reconstruction or their SB MCL plus anteromedial reconstruction at ≥30° of knee flexion were similar; however, their proposed flat sMCL plus anteromedial reconstruction does slightly better. 6 The mean difference in AMR between the intact state and the DB MCL reconstruction was smaller at ≥60° and similar at 30° of knee flexion compared with the 2-graft reconstruction of Miyaji et al. 22 Their results for AMT were better than those found in this study; however, the overall increase in AMT after MCL injury was low. 22 AMT is difficult to compare between studies, as the reference point to measure the anterior tibial translation is either the middle of the knee joint or the middle of the medial tibia plateau.6,22,33 Furthermore, the method to define the middle of the medial plateau is not standardized. 33 The further the reference point is away from the knee center, the larger the increase in AMT. This might explain the low AMT measurements found in some studies.6,22 Additionally, a different anterior tibial translation force might influence the measurements.6,22 That said, the results of these studies show that in ≥30° of knee flexion, the DB MCL reconstruction controls AMRI similarly, in comparison with the recently described 2-graft techniques.
Our previous studies have demonstrated that an isolated dMCL injury increases the load on the ACL by 168% during AMR in knee extension. 5 If this is the case in the clinical scenario, then it might be important to further decrease AMR closer to extension. Because the dMCL plays the most important role of controlling AMRI in knee extension, an additional anteromedial graft might help to mimic the dMCL kinematics and thereby improve AMRI close to extension.3,33 A possibility is to add an extra graft in the femoral tunnel for the anteromedial reconstruction in the proposed DB MCL reconstruction. Alternatively, a second femoral tunnel can be made for the anteromedial reconstruction.22,23 In the current study, we piloted (n = 2) an anteromedial reconstruction using the anatomic landmarks as described in the past literature,22,23 but 2 important problems were encountered. First, given the close proximity of the centers of the femoral tunnels (8.6 mm), the bone bridge between the tunnels was very small, which led to failed fixation due to tunnel coalition during interference screw insertion. Even in a young active adult, a 1.6- or 2.6-mm bone bridge is at high risk for tunnel coalition. 24 Second, because the anteromedial bundle is an extra anatomic reconstruction, the anterior insertion of the anteromedial reconstruction on the tibia is not well defined. Inserting it too anterior on the tibia can lead to overconstraint of the knee joint. In the literature, the anteromedial bundle is only tensioned to 20 or 40 N to overcome potential overconstraint.6,22,23 A too posterior tibial insertion might, however, miss the goal of the extra reconstruction. Similarly, in the presented DB MCL reconstruction, it was difficult to exactly define the position of the proximal anterior anchor based on anatomic landmarks. AMRI was overconstrained in knee flexion when moving the insertion more than 5 mm anterior to the anterior bundle of the graft (2 pilot study specimens). It is therefore important to further investigate the ideal tibial positioning of the proximal tibial fixation for anteromedial reconstruction based on anatomic or radiographic landmarks to make these reconstructions more reproducible. 2
The native MCL has different length change characteristics depending on the location of the examined fibers. 15 The more posterior MCL fibers become tighter in extension and slacken in flexion. 15 The SB MCL reconstruction proposed by LaPrade and Wijdicks 17 has similar characteristics to the posterior MCL fibers.8,15 Consequently, a slight slackening of the reconstruction can be expected at 90° of flexion.8,15 In the current study, valgus laxity was not restored to intact kinematics at 90° of knee flexion in all tested reconstructions. With all reconstructions being performed equally, a proximal fixation did not have an important influence on VR. In contrast to this study, Behrendt et al 6 found that an SB MCL reconstruction could not control VR in 30° to 90° of knee flexion. However, the femoral tunnel was slightly different compared with the originally described technique.6,17 Furthermore, a flat sMCL with or without anteromedial reconstruction or an SB MCL with anteromedial reconstruction did restore intact VR kinematics. 6 However, several other biomechanical studies have shown that the SB MCL reconstruction could restore VR to intact.7,30,32,36 These studies all included a POL reconstruction as well, which could have influenced their results.7,30,32,36 However, because the POL mainly controls VR in extension and not in flexion, it may be interpreted that these studies’ SB MCL reconstruction was responsible for controlling VR in deep flexion.3,10,33 Although isometry was controlled in the current study, the results did show differently. In clinical practice, the isometric point can sometimes be difficult to identify, particularly because the femoral insertion is very sensitive to positional changes. 15 If isometry is difficult to achieve, it is better that the MCL slackens slightly in flexion than vice versa. 19 Furthermore, many sports or activities at risk are performed in low flexion angles. Therefore, restoring VR in 90° of knee flexion might be less important than close to extension.
The dMCL is discussed as a secondary stabilizer for knee IR. 25 As long as the POL or posterior cruciate ligament is intact, the effect on IR of transecting the dMCL and sMCL might therefore be minimal. 25 In agreement, the mean differences in IR were small between the intact and deficient states in the current study. Reconstructing the MCL did not seem to have an important effect on IR either. It is unknown what the performance would be of the different MCL reconstructions in controlling IR in a knee with concomitant dMCL/sMCL and POL injury. However, this lies outside the scope of this study.
Despite the DB MCL reconstruction not being able to fully mimic intact MCL kinematics in all knee positions, the technique has technical advantages. It is easy to adapt from the gold standard technique as it uses the same femoral and tibial tunnel positions. 17 There is only a need for 1 graft, which can be especially important in multiligament reconstructions or in hospitals with reduced access to allograft tissue. 28 Furthermore, there is no need for extra implants, which avoids extra costs. In the clinical setting, the senior author uses an adjustable loop suspensory fixation at the level of the femur, which allows retensioning of the graft after cycling of the knee joint. 8 This technique was previously published; however, in the currently proposed technique, the proximal fixation is more anterior than that in the initial publication. 8
The present study is not without limitations. First, the surgical steps did not allow for randomized testing order, which could potentially induce bias due to graft creep and increases in joint laxity after multiple tests. To mitigate this, the joint was first preconditioned by executing the entire test sequence, allowing the graft to potentially creep without recording any data. Furthermore, a digital tensioning tool allowed retensioning of the graft so that the tension was the same at the beginning of each test cycle. The risk that the testing order affected the results might be limited as the second reconstruction tested was tighter than the first. Second, the medial hamstring muscles are dynamic stabilizers of AMRI and were not loaded in this in vitro study 12 ; however, this simplification equally influences all testing stages and should not invalidate comparisons between reconstructions. Third, although ACL injury and ACLR are discussed, an ACL injury and subsequent ACLR were not studied. This approach was chosen to reduce confounding variability related to ACLR, which could make the interpretations of the results more difficult. Moreover, other recent studies on MCL reconstructions also chose not to perform an ACLR.6,7,22,23
Conclusion
In an in vitro cadaveric study, a DB MCL reconstruction with a proximal tibial fixation of the anterior bundle placed more anteriorly on the tibia was able to control AMR and AMT better than the gold standard SB MCL reconstruction. The reconstruction uses the same anatomic landmarks and tunnel positions as the SB technique; however, it does not require an extra graft or additional implants, which makes it a viable alternative when addressing combined AMR and valgus instability.
Supplemental Material
sj-pdf-1-ajs-10.1177_03635465241251463 – Supplemental material for Double-Bundle Medial Collateral Ligament Reconstruction Improves Anteromedial Rotatory Instability
Supplemental material, sj-pdf-1-ajs-10.1177_03635465241251463 for Double-Bundle Medial Collateral Ligament Reconstruction Improves Anteromedial Rotatory Instability by Wouter Beel, Thiago Vivacqua, Ryan Willing and Alan Getgood in The American Journal of Sports Medicine
Footnotes
Submitted July 29, 2023; accepted February 14, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: Support was received from Smith & Nephew Inc in the form of a research grant that funded the presented research; Ossur Inc in the form of an educational grant for the authors’ research fellowship position; the Natural Sciences and Engineering Research Council (NSERC) Discovery: RGPIN-2018-05693; the Ontario Early Researcher Award ER18-14-197; and the Canadian Foundation for Innovation JELF and Ontario Research Fund—Research Infrastructure: 38141. A.G. has received consulting fees from Smith & Nephew; is on the advisory board of and holds stock in Spring Loaded Technologies; and holds stock in OS LinkX Robotics and Ostesys Robotics. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.