
Abstract
Background:
The optimal surgical approach in patients with borderline hip dysplasia (BHD) remains controversial. Both hip arthroscopy and periacetabular osteotomy (PAO) are commonly employed in this patient population. Those who participate in sports want to resume and maintain sports activities after surgery, and the ability to do so plays an important role in the choice of a treatment method. To our knowledge, no previous study has assessed return-to-sports rates and activity levels in patients with BHD after PAO.
Purpose:
To assess return-to-sports rates and postoperative activity levels as measured by the University of California, Los Angeles (UCLA), activity scale as well as patient-reported outcome measures. Also to assess changes in sports activity both qualitatively and quantitatively as well as underlying reasons for these changes.
Study Design:
Case series; Level of evidence, 4.
Methods:
We conducted a retrospective analysis of prospectively collected data from 55 hips in 52 patients with BHD who underwent PAO between January 2015 and June 2017. Return-to-sports rates, UCLA activity scores, International Hip Outcome Tool–12 scores, Subjective Hip Value scores, Hip disability and Osteoarthritis Outcome Score subscores, sports practiced, frequency and duration of sports activity, and postoperative changes as well as underlying reasons were recorded.
Results:
The mean follow-up was 62.8 ± 9.0 months. The return-to-sports rate among preoperatively active patients was 92.5%. Most patients resumed sports activity after 6 months (50%) or after 3 to 6 months (37.5%). The UCLA activity score improved significantly (from 5.2 ± 2.4 to 7.0 ± 1.8; P < .001). The International Hip Outcome Tool-12, Subjective Hip Value, and Hip disability and Osteoarthritis Outcome Score scores also improved significantly (all, P < .001). Changes in sports activity occurred in 34.5% of cases after PAO. Significantly more patients engaged in low-impact sports postoperatively. Participation in high-impact sports did not decrease significantly. Reasons for changes were both hip related and non–hip related. Quantitatively, patients were able to significantly increase both the frequency (P = .007) and duration (P = .007) of sports activity.
Conclusion:
The return-to-sports rate in patients with BHD after PAO was high at over 92%. Most patients returned to sports after a period of 6 months or 3 to 6 months. Overall, activity levels and hip function improved after PAO. A number of patients adjusted their sports activity after PAO. Although more patients engaged in low-impact sports, participation in high-impact sports was maintained postoperatively. The results of this study may help both patients and orthopaedic surgeons in deciding on the best surgical procedure in the setting of BHD.
Keywords
The optimal surgical approach in patients with borderline hip dysplasia (BHD) remains controversial. Both hip arthroscopic surgery and periacetabular osteotomy (PAO) are employed in this patient population in the absence of a standardized diagnostic algorithm and a consensus on a treatment option.4,20,22
Improved patient-reported outcomes and hip function have been reported after both hip arthroscopic surgery and PAO in patients with BHD.4,7,10,20-22,26 However, with isolated hip arthroscopic surgery, as many as 40% of patients experience suboptimal outcomes.8,9,21 These high rates of treatment failure likely stem from the difficulty in differentiating between the underlying primary problem of hip symptoms in patients with BHD. Even though labral abnormalities and coexisting femoroacetabular impingement can be addressed arthroscopically, addressing instability due to acetabular undercoverage requires acetabular reorientation through PAO.15,21
At the time of indication, regardless of the surgical approach chosen, patients are usually young and active with high functional demands. Those who participate in sports want to resume and maintain sports activities after surgery,2,6,13,18,23-25 and the ability to do so plays an important role in the choice of a treatment method.
Although high return-to-sports rates have been reported after hip arthroscopic surgery in patients with BHD,2,13,24 to our knowledge, no study to date has reported on return to sports and activity levels in patients with BHD after PAO. However, this information is essential to be able to counsel active patients in the choice of a surgical management strategy for BHD, as hip arthroscopic surgery and PAO are procedures of different magnitudes, which presumably could have implications in return to sports.
The present study therefore aimed to assess return-to-sports rates and postoperative activity levels as measured by the University of California, Los Angeles (UCLA), activity scale and other patient-reported outcome measures. A second aim was to assess changes in sports activity both qualitatively and quantitatively as well as underlying reasons for these changes. We hypothesized that patients would be able to return to preoperative activity levels as measured using the UCLA activity scale and continue to participate in preoperative sports activities.
Methods
Study Design
We performed a retrospective analysis of prospectively collected data from the institutional PAO database of a single orthopaedic university center. Approval from the local ethics committee was obtained before the initiation of the study (EA1/052/21). The present study describes a unique analysis, but some patient data may have been reported in other studies. The study was conducted in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology guidelines. Patients who underwent PAO between January 2015 and June 2017 were included. Inclusion criteria were a primary diagnosis of symptomatic BHD, defined as a lateral center-edge angle of 18° to 25° as measured on standardized anteroposterior standing radiographs; complete preoperative and postoperative data on activity levels as well as the frequency and duration of sports activity at follow-up; completed hip questionnaires on preoperative and postoperative functional status; and signed informed consent forms. Exclusion criteria were PAO for indications other than symptomatic BHD (eg, severe hip dysplasia or acetabular retroversion), Tönnis grade >1 osteoarthritis, incomplete data, or lack of informed consent.
Patients
During the study period, a total of 90 of 202 patients who underwent PAO were treated for a primary diagnosis of symptomatic BHD. Of these, 35 cases were lost to follow-up, resulting in a final cohort of 55 hips in 52 patients. Of these hips, 83.6% were female, and 16.4% were male. PAO was performed on the right hip in 52.7% of cases. PAO was performed through a single-incision less/minimally invasive approach according to the Bernese technique.11,28 Fixation was achieved through K-wire fixation (43.6%) or screw fixation (56.4%). Additional femoral head-neck osteochondroplasty through mini-arthrotomy was performed in 13 cases.
All patients underwent a standardized mobilization regimen with toe-touch partial weightbearing for a period of 6 weeks postoperatively. After week 6, weightbearing was increased to half of the patient's body weight from week 7 to week 10. After week 10, weightbearing was then gradually increased to full weightbearing. No restriction was imposed on the range of motion of the operated hip joint.
The mean age of patients at the time of surgery was 28.9 ± 8.6 years, and the mean body mass index (BMI) was 23.3 ± 4.2. The mean follow-up was 62.8 ± 9.0 months.
Data Collection
Radiographical parameters relevant to BHD (ie, lateral center-edge angle, Tönnis angle, femoral head extrusion index, anterior wall index, and posterior wall index) were measured preoperatively and postoperatively on standardized anteroposterior standing radiographs.
The return-to-sports rate was defined as the proportion of patients who participated in sports activities preoperatively and continued to engage in sports activities postoperatively. Overall sports participation preoperatively and postoperatively was also recorded among the study cohort.
The time to return to sports was recorded as the time between surgery and the resumption of sports activity, recorded in weeks. Patients could categorize themselves as (1) between 1 and 3 months, (2) between 3 and 6 months, (3) after >6 months, or (4) no return to sports. 18
Preoperative and postoperative activity levels and hip function were assessed during a routine examination. The activity level was determined using the UCLA activity scale. 3 Hip function was evaluated using the International Hip Outcome Tool–12 (iHOT-12), 12 the Subjective Hip Value, 16 and the Hip disability and Osteoarthritis Outcome Score (HOOS) with its subscales (Pain, Symptoms, Activities of Daily Living, Sport and Recreation, and Quality of Life), 27 as these have been previously validated and recommended for young, active patients in the context of hip preservation surgery. Patient-reported outcomes and sports activity data were collected at follow-up using a hip-specific questionnaire.
Return-to-sports rates and timing as well as qualitative and quantitative changes in sports activity were recorded using a questionnaire developed specifically for this purpose. For simplification, a list of common sports (cycling, alpine skiing, fitness training, tennis, basketball, soccer, handball, volleyball, hiking, golf, long walks, Nordic walking, running/jogging) was provided. 18 Sports not included in the list were recorded by free-text answers. Furthermore, the option of “no sports” was listed, and multiple choices were possible. Activities were divided into high-impact sports (tennis, soccer, volleyball, alpine skiing, mountaineering, running/jogging, dancing, martial arts) and low-impact sports (cycling, long walks, Nordic walking, hiking, fitness training, swimming, yoga, horseback riding), as previously defined in the literature.14,18 Patients were asked whether they participated in different sports after surgery than before surgery. In the case of a postoperative change in the sports practiced, patients were asked about the reason for this change. The answers were divided into hip-related and non–hip-related reasons.
Quantitative sports activity was measured by the frequency of sports participation as 0, 1, 2, 3, 4, or >4 times per week. In addition, the duration of sports activity was recorded in minutes. Patients could rate their sports activity on a scale of 0 to 15, 16 to 30, 31 to 60, 61 to 120, or >120 minutes per session. 18
The subjective influence of PAO on athletic ability was also recorded. Patients could choose between (1) improved, (2) worsened, and (3) no influence. Qualitative and quantitative aspects were collected at the time of follow-up using the previously mentioned questionnaire. 18
Statistical Analysis
The frequency, proportion, mean, standard deviation, and range were used to describe basic patient characteristics. A normal distribution was examined using the Shapiro-Wilk test. The t test was used to determine significant differences between continuous data, and the chi-square test was used for categorical data. For nonparametric data, the Wilcoxon test was used. A P value of <.05 was considered statistically significant. Excel (Version 16.16.2; Microsoft) was used to document the collected data. The collected data were analyzed using SPSS (Version 25; IBM).
Results
Radiographical Findings
The relevant radiographical parameters significantly improved from preoperatively to postoperatively. The lateral center-edge angle increased from 20.9°± 2.5° preoperatively to 31.9°± 5.3° postoperatively (P < .001), the Tönnis angle decreased from 9.8°± 4.8° preoperatively to 1.0°± 7.4° postoperatively (P < .001), and the femoral head extrusion index decreased from 19.5% ± 5.6% preoperatively to 6.9% ± 6.5% postoperatively (P < .001). The anterior wall index increased from 0.44 ± 0.15 preoperatively to 0.49 ± 0.14 postoperatively (P = .031), and the posterior wall index decreased from 0.86 ± 0.15 preoperatively to 0.77 ± 0.23 postoperatively (P = .013).
Patient-Reported Outcomes and Hip Function
Hip function, as measured by the iHOT-12 (P < .001) and Subjective Hip Value (P < .001), improved significantly from preoperatively to postoperatively. The HOOS subscores also improved significantly (P < .001). For a detailed overview of patient-reported outcomes, see Table 1.
Preoperative and Postoperative Patient-Reported Outcomes a
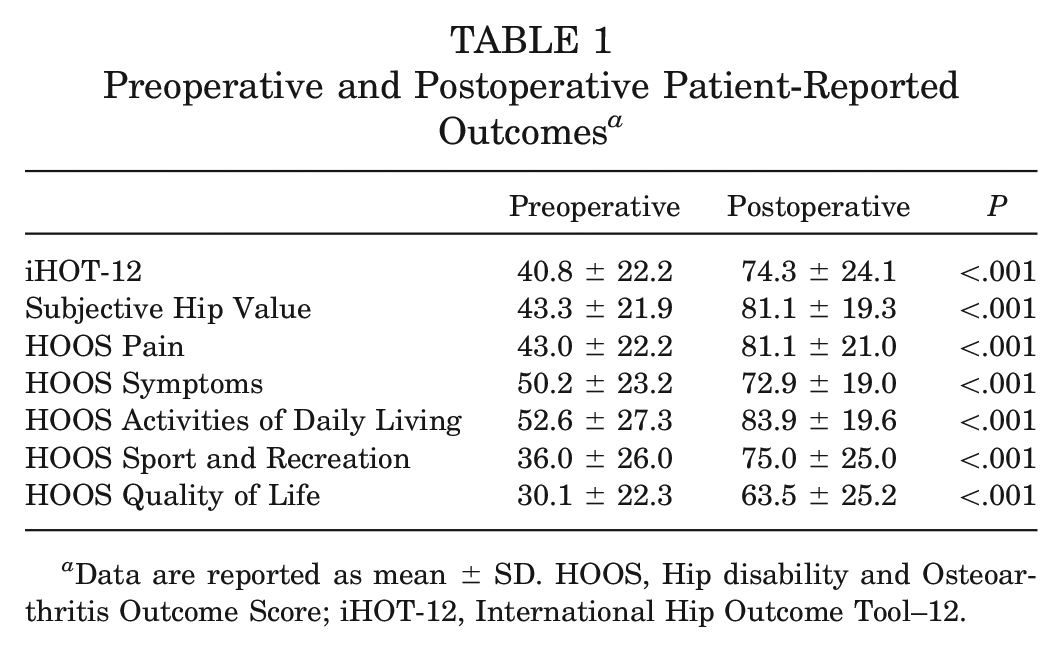
Data are reported as mean ± SD. HOOS, Hip disability and Osteoarthritis Outcome Score; iHOT-12, International Hip Outcome Tool–12.
Return to Sports
The overall return-to-sports rate among preoperatively active patients was 92.5% (37/40). Compared with preoperatively, more patients participated in sports after PAO (72.7% [40/55 hips] vs 87.3% [48/55 hips], respectively; P = .056). Most patients resumed sports activity after 6 months (50.0% [24/48]) or after 3 to 6 months (37.5% [18/48]); 12.5% (6/48) reported resuming sports after 1 to 3 months. All of the patients who reported returning to sports between 1 and 3 months participated in low-impact sports (cycling, swimming, long walks, fitness training, yoga).
Changes in Sports Activity
Activity levels, as measured by the UCLA activity scale, improved significantly from preoperatively to follow-up (from 5.2 ± 2.4 to 7.0 ± 1.8; P < .001). For a graphic representation of preoperative to postoperative changes in activity levels, see Figure 1.
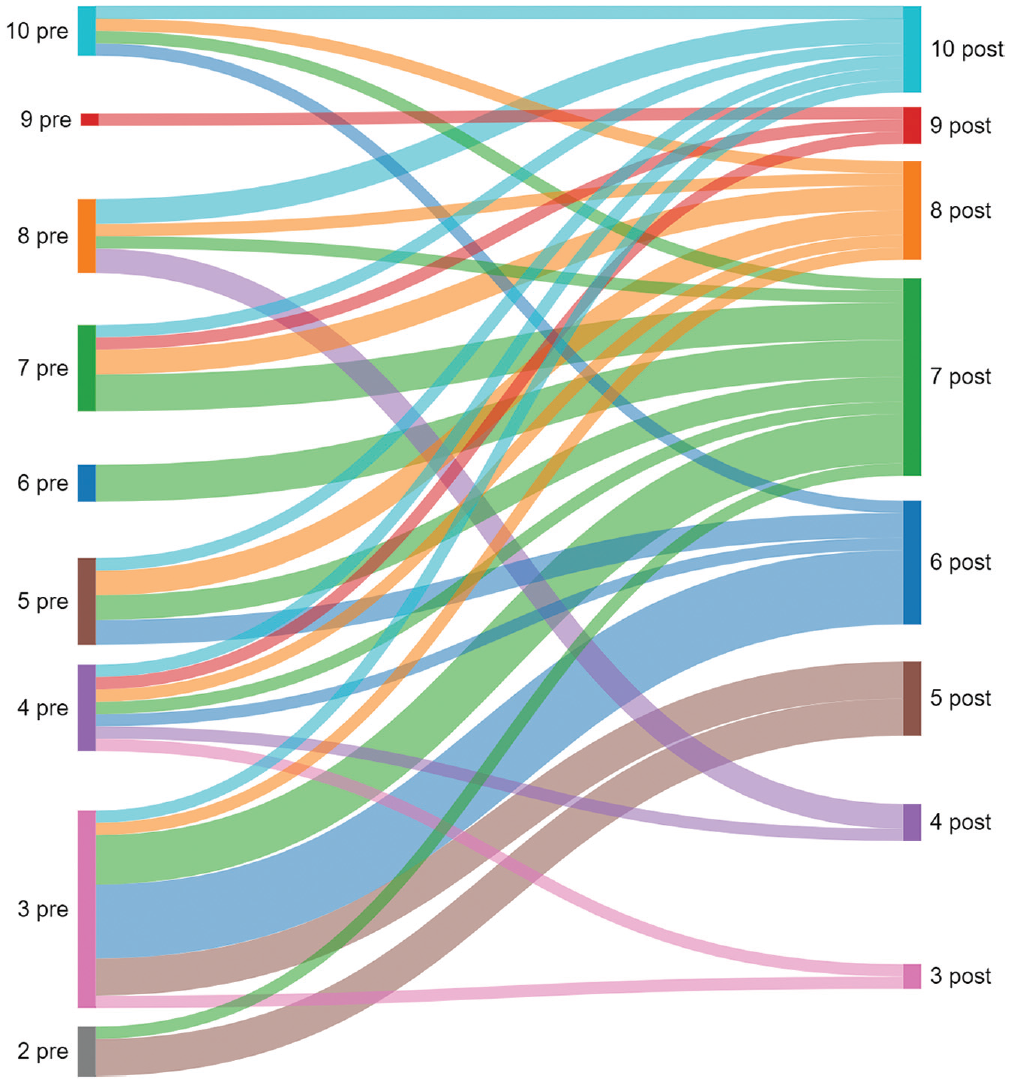
Sankey plot illustrating the preoperative (pre; left) to postoperative (post; right) changes in sports activity levels as measured by the University of California, Los Angeles, activity scale.
There was a significant negative correlation between postoperative activity levels as measured by the UCLA activity scale and BMI (rs = −0.31) and postoperative pain levels (rs = −0.38), indicating that patients with a higher BMI and pain level had lower activity levels. There was a significant positive correlation between activity levels and postoperative hip function as measured by the iHOT-12 (rs = 0.49) and Subjective Hip Value (rs = 0.49). Among patients who participated in sports preoperatively and did not return to sports postoperatively, there was a significant negative correlation with postoperative hip function as measured by the iHOT-12 (rs = −0.39) and Subjective Hip Value (rs = −0.31) as well as a significant positive correlation with postoperative pain levels (rs = 0.36), indicating that poorer hip function and higher pain levels were associated with not returning to sports.
Overall, 19 cases (34.5%) had changes in sports activities after PAO. A total of 12 cases (21.8%) reported that they had stopped their previously practiced sports after surgery, whereas 9 (16.4%) reported that they had started new sports. Of the cases that stopped participating in sports postoperatively, 2 (3.6%) reported doing so for reasons unrelated to surgery, 8 (14.5%) indicated lower tolerance/pain as the reason, and 2 (3.6%) stopped sports on the advice of their physician. Of those that started new sports postoperatively, 5 (9.1%) reported that they started new sports that were not possible preoperatively because of hip pain, while 4 (7.3%) reported that they started new sports to improve hip function.
The proportion of cases that participated in low-impact sports increased significantly from preoperatively (29.1% [16/55]) to postoperatively (47.3% [26/55]) (P < .049). The proportion of cases that participated in high-impact sports did not decrease significantly from preoperatively (43.6% [24/55]) to postoperatively (40.0% [22/55]) (P = .699). Among the high-impact sports listed, soccer stood out as a sport that involved fast running as well as stop-and-go and cutting activities. The number of patients who played soccer decreased from preoperatively (10/55 [18.2%]) to follow-up (4/55 [7.3%]) (P = .086), resulting in a return-to-sports rate of 40.0% for soccer. These changes were not significant. For a detailed overview of the sports practiced and preoperative to postoperative changes, see Figure 2.
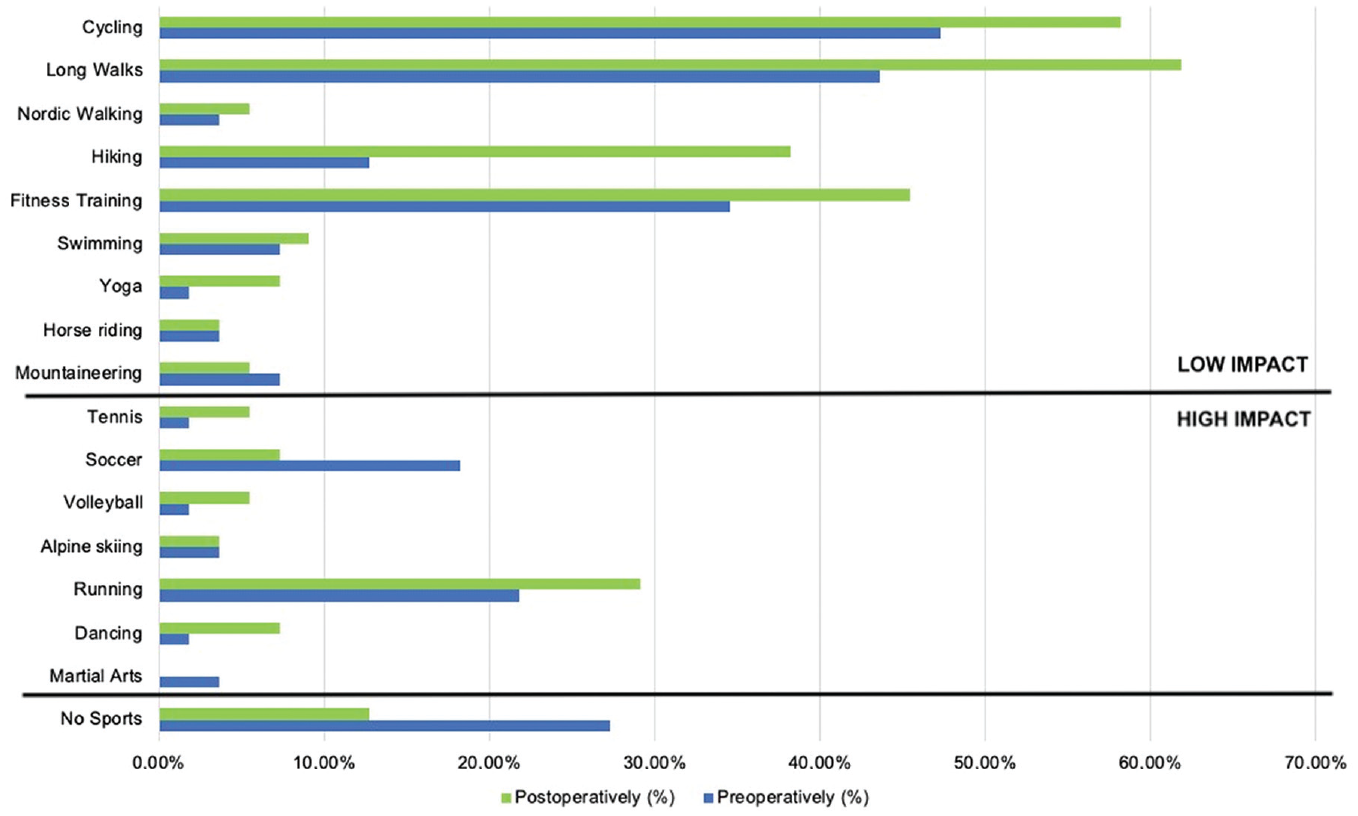
Preoperatively and postoperatively practiced sports divided into high- and low-impact sports. Multiple answers were possible.
Frequency and Duration of Sports Activity
Quantitatively, patients were able to increase sports activity postoperatively. At follow-up, the frequency of sports activity in times per week was significantly higher (P = .007). For a graphic illustration of the frequency of sports activity, see Figure 3.
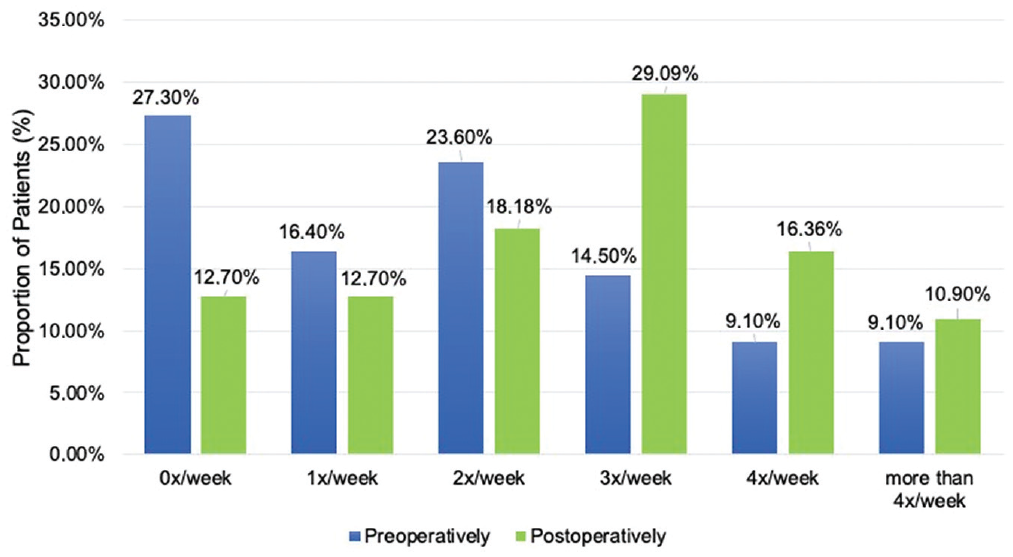
Preoperative and postoperative frequency of sports activity (times/week). Overall, sports frequency increased significantly (P = .007) at follow-up.
There were differences in sports frequency before and after surgery in 72.7% of the cases. In 47.3% of cases, sports frequency was higher postoperatively than preoperatively, while it was lower postoperatively in 25.5% of cases.
The duration of sports activity in minutes per session also increased significantly (P = .007). For a graphic illustration of the duration of sports activity, see Figure 4.
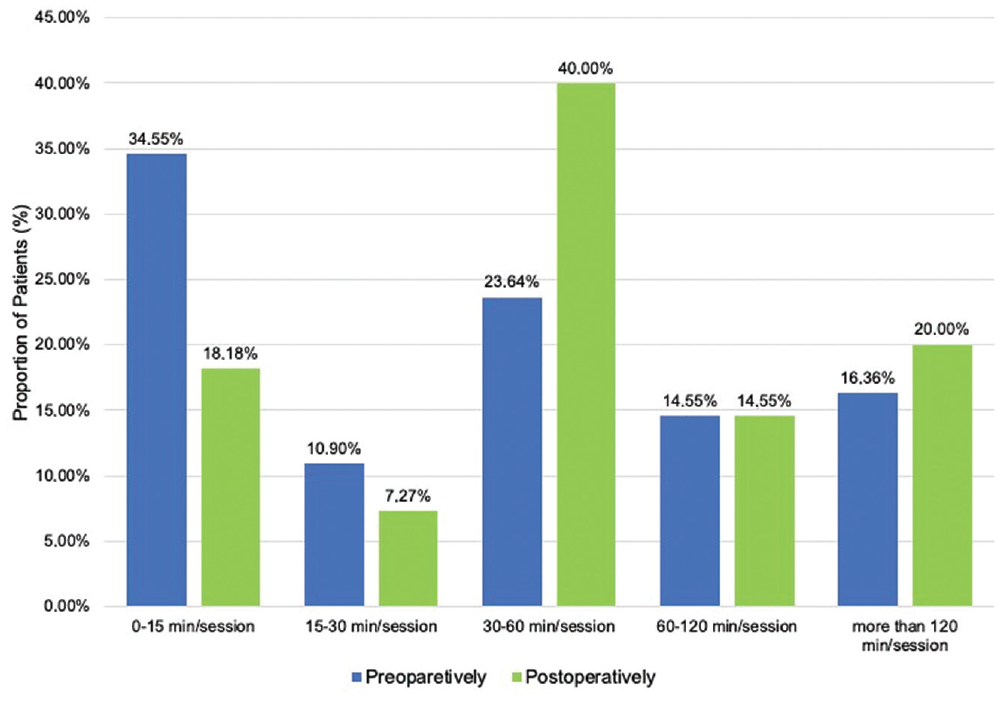
Preoperative and postoperative duration of sports activity (minutes/session). Across the study population, sports duration increased significantly (P = .007).
Subjective Influence on Sports Ability
Regarding the subjective impact of PAO on sports ability, of 53 cases in which patients answered the question, 33 (62.3%) indicated that the procedure subjectively improved their sports ability, 11 (20.8%) indicated that the procedure subjectively decreased their sports ability, and 9 (17.0%) indicated that the procedure did not subjectively affect their sports ability.
Discussion
To our knowledge, this is the first study to report return-to-sports rates and changes in sports activity in patients with BHD after PAO. The most important finding is that >92% of athletically active patients with BHD returned to sports after PAO. Most of them returned to sports after a period of 6 months or 3 to 6 months. Overall, activity levels increased postoperatively, while patient-reported outcomes also increased significantly. A relevant proportion of patients adapted their sports activities postoperatively for hip-related and non–hip-related reasons. Although more patients engaged in low-impact sports postoperatively, those who engaged in high-impact sports were able to continue to do so after surgery.
The optimal surgical approach in patients with BHD remains a topic of debate, and both hip arthroscopic surgery and PAO are commonly employed. To date, few studies exist that directly compare the 2 techniques in patients with BHD. Nepple et al 22 reported on 113 cases of BHD, of which 42% were treated with PAO and 58% with hip arthroscopic surgery. The authors found significant improvements in patient-reported outcomes and hip function in both groups, with comparable improvements and failure rates for both procedures. However, significant differences in patient characteristics were found in the studied population, making a direct comparison difficult. In addition, with a minimum follow-up of 2 years, no long-term conclusions could be drawn, and return to sports was not investigated. 22
In the only systematic review to date comparing hip arthroscopic surgery and PAO in patients with BHD, Murata et al 20 compared the outcomes of 10 studies after hip arthroscopic surgery with 2 studies after PAO. Although, overall, cohorts were heterogeneous and different patient-reported outcome measures were used, significant postoperative improvements were found across all studies. Considering the few studies with a long-term follow-up, patients with BHD treated with hip arthroscopic surgery showed survivorship of 76% to 79%5,17 after 10 years, whereas survivorship after 10 years with PAO was >91% in systematic reviews, although the latter also included higher grade hip dysplasia. 1 It seems plausible that the inability of hip arthroscopic surgery to improve the biomechanics of the joint by better coverage may play a role in this context.
To date, the literature on outcomes after PAO in patients with BHD is scarce. Thus far, only a few studies have reported on functional outcomes after PAO.4,19,21 Even though all of these studies reported improvements in radiographical parameters and patient-reported outcomes, none included an analysis of sports activity. Andronic et al 4 described significantly improved Tegner activity scores after PAO in a cohort of 53 hips in 42 patients. However, no detailed information on return to sports and changes in physical activity was found in that study. Our results also showed an improvement in activity levels as measured by the UCLA activity scale and a high return-to-sports rate of >92% after 6 months or after 3 to 6 months in most cases.
Comparing our results with the literature on patients who underwent hip arthroscopic surgery for BHD, our study showed a higher rate of return to sports after PAO. Jimenez et al 13 studied 54 patients with BHD who underwent isolated hip arthroscopic surgery with capsular plication and labral preservation and found a return-to-sports rate of 80.7%. However, in comparison with the present study, it should be noted that in that cohort, mainly high-level athletes were examined.
Limitations
The present study has inherent limitations. Overall, the preoperative activity level as measured by the UCLA activity scale was relatively low, which makes conclusions for high-level athletes difficult. However, patients were able to improve their activity level postoperatively to one previously defined in the literature as athletic, with a UCLA score of 7.0.6,18,23,25 Other limitations include the retrospective study design and that the cohort was relatively small, with 55 hips. Furthermore, 61.1% (55/90) of the cases were available for follow-up, leading to the possibility of transfer bias. However, in the present study, we were able to report on return-to-sports rates and changes in sports activity in patients with BHD after PAO for the first time in the literature.
Conclusion
The return-to-sports rate in patients with BHD after PAO was high at >92%. Most patients returned to sports after a period of 6 months or 3 to 6 months. Overall, activity levels and hip function improved after PAO in this patient population. A number of patients adjusted their sports activity after PAO. Although more patients engaged in low-impact sports, participation in high-impact sports was maintained postoperatively. The results of this study may help both patients and orthopaedic surgeons in deciding on the best surgical procedure in the setting of BHD.
Footnotes
Submitted July 30, 2023; accepted October 6, 2023.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.