
Abstract
Background:
Hip dysplasia is a common condition in active adults with hip pain that can lead to joint degeneration. Periacetabular osteotomy (PAO) is a common surgical treatment for hip dysplasia. The effect of this surgery on pain, function and quality of life (QOL) has not been systematically analysed.
Purpose:
In adults with hip dysplasia: (1) evaluate differences in pain, function and QOL in those undergoing PAO and healthy controls; (2) evaluate pre- to post-PAO changes in pain, function and QOL; (3) evaluate differences in pain, function and QOL in those with mild versus severe dysplasia, undergoing PAO; and (4) evaluate differences in pain, function and QOL in those having primary PAO versus those with previous hip arthroscopy.
Methods:
A comprehensive, reproducible search strategy was performed on 5 different databases. We included studies that assessed pain, function and QOL in adults undergoing PAO for hip dysplasia, using hip-specific patient reported outcomes measures.
Results:
From 5017 titles and abstracts screened, 62 studies were included. Meta-analysis showed PAO patients had worse outcomes pre- and post-PAO compared to healthy participants. Specifically, pain (standardised mean difference [SMD] 95% confidence interval [CI]): −4.05; −4.78 to −3.32), function (−2.81; −3.89 to −1.74), and QOL (−4.10; −4.43 to −3.77) were significantly poorer preoperatively.
Meta-analysis found patients experienced improvements following PAO. Pain improved from pre-surgery to 1-year (standardised paired difference [SPD] 1.35; 95% CI, 1.02–1.67) and 2 years postoperatively (1.35; 1.16–1.54). For function, the activities of daily living scores at 1 year (1.22; 1.09–1.35) and 2 years (1.06; 0.9–1.22) and QOL at 1 year (1.36; 1.22–1.5) and 2 years (1.3; 1.1–1.5) all improved. No difference was found between patients undergoing PAO with mild versus severe dysplasia.
Conclusions:
Before undergoing PAO surgery, adults with hip dysplasia have worse levels of pain, function and QOL compared to healthy participants. These levels improve following PAO, but do not reach the same level as their healthy participants.
Registration:
PROSPERO (CRD42020144748)
Keywords
Introduction
Developmental dysplasia of the hip (DDH) is a term that encompasses a spectrum of abnormal hip morphology involving the acetabulum and the proximal femur.1,2 Current notions describe a resultant instability of the hip joint with subsequent chondral degeneration and secondary osteoarthritis. 3 It is thought that DDH is a risk factor of early-onset osteoarthritis.3,4–8 Amongst patients with mild degenerative change in their hip, those with DDH have almost 3 times the risk of progressing to end-stage osteoarthritis or total hip arthroplasty (THA), compared with normal morphology. 9 In those with Tönnis grade 1 degenerative change, 1 in 3 patients received a THA within 10 years, compared to 1 in 5 shown in those with normal or femoroacetabular impingement (FAI) morphology. 9 This implies that those with DDH are at increased risk of rapid degenerative change of their hip joint, once they develop early degenerative change. 9
The international hip-related pain research network has identified acetabular dysplasia as one of the most common hip conditions in active adults presenting with hip pain. 10 The true prevalence of DDH is difficult to ascertain as the condition can often be asymptomatic and there are inconsistencies regarding the diagnosis in the literature.3,8,11 Prevalence ranges from 1.7% to 20% in the general population.7,11–14 The traditional measure of DDH is the lateral centre-edge angle (LCEA) of Wiberg radiographically assessed from a weight-bearing anterioposterior (AP) pelvic view. A value <20° is defined as dysplasia, between 20° and 25° has been defined as borderline dysplasia, and 25–39° is defined as normal. 15 It is unclear whether radiological severity affects outcomes. As the complex multi-directional nature of DDH has become better understood, the importance of utilising a combination of radiological and clinical findings has been recognised, though not agreed upon.3,16,17
Limited evidence suggests people suffering from DDH may experience pain, physical impairments, sporting limitations, and reduced quality of life (QOL).18–20 Surgical management options include arthroscopy, osteotomy, and THA. 3 Hip arthroscopy is considered controversial and is often cautioned in patients with DDH due to conflicting outcomes, 3 with 1 in 4 failures of hip arthroscopy occurring in patients with DDH as a primary or secondary diagnosis. 21 Despite this, hip arthroscopy is commonly used in patients with DDH, and so requires evaluation. The most common surgical treatment used to address symptomatic DDH is periacetabular osteotomy (PAO).22,23 The procedure aims to preserve the native hip joint and delay the need for THA by medialising the hip joint centre, redistributing the high contact stresses from the acetabular rim to the entire articular surface, and transforming the dysplastic hip’s shear stresses across the articular cartilage into compressive stresses that are more favourable for cartilage longevity.24–27 Successful PAO surgery should not only improve structural abnormalities but also aim to improve pain, physical impairments, sporting limitations, and QOL. Several hip-specific patient-reported outcome measures (PROMs) exist to provide information on hip-related pain, function and QOL. However, there is limited systematic synthesis of PROMs, inhibiting our ability to confidently understand what these patients are experiencing. This affects our clinical approach and management, and our ability to truly appreciate the burden of this condition.
This systematic review aimed to, in adults with DDH: (1) evaluate differences in pain, function and QOL in those undergoing PAO and healthy controls; (2) evaluate pre- to postoperative changes in pain, function and QOL following PAO; (3) evaluate differences in pain, function and QOL in those with mild versus severe dysplasia, undergoing PAO; and (4) evaluate differences in pain, function and QOL in those having primary PAO versus those with previous hip arthroscopy.
Methods
Study selection, eligibility criteria, data extraction, and statistical analysis were performed according to the Cochrane Collaboration guidelines. 28 The systematic review was reported according to the preferred reporting guidelines for systematic reviews and meta-analysis (PRISMA) guidelines, 29 and was registered on the Prospero international prospective register of systematic reviews (ID: CRD42020144748).
Search strategy
A comprehensive, reproducible search strategy was performed on the following databases MEDLINE CINAHL, EMBASE, Sports Discuss, and PsychINFO from inception until 05 January 2021.
The search strategy was conducted by 2 reviewers (MO, AS) and using the following concepts:
(1) Humans with DDH aged ⩾15 years
(2) Periacetabular osteotomy
(3) Hip-specific patient-reported outcome measure
Synonyms were searched within concepts using ‘OR’ operator and searched between concepts using ‘AND’ operator.
For search strategy used see Supplemental Appendix 1.
All potential references were imported into Endnote X8 (Thomson Reuters, Carlsbad, CA, USA) and duplicates removed. All included studies were then uploaded into Covidence software (Veritas Health Innovation Ltd, Australia) for screening. Title, abstract and full text screening was conducted by 3 independent reviewers (MO (A–Z), CS (A–M), LR (N–Z). Any disagreements were resolved by a 4th independent reviewer (JK).
Eligibility criteria
Studies were eligible for inclusion if they used a hip-specific patient-reported outcome measure (PROM) and were written in English. All quantitative observational study designs were considered eligible including randomised control trials, non-randomised controlled trials, case series, prospective or retrospective study designs.
Participants/population
People aged 15 years and older with DDH undergoing PAO (based on the mean or median age of the study sample). Studies were ineligible if the PAO was undertaken in people with Cerebral Palsy, Down Syndrome or Charcot-Marie Tooth Disease populations.
Intervention(s), exposure(s)
Studies utilising PAO surgery as primary intervention for DDH. The terms ‘Bernese Osteotomy’ and ‘Ganz Osteotomy’ were considered interchangeable with ‘Periacetabular Osteotomy’. Studies were ineligible if the PAO was reported to be a ‘rotational’ or ‘curved’ procedure as these procedures differ in surgical technique.
Comparator(s)/control
Studies using sham treatment, no treatment or other treatment (e.g. THA or hip arthroscopy surgery) as the comparator/control treatment were included. We also included studies where no comparison group was present if they used 2 time-points (e.g. case series). In this instance, the pre-intervention time-point was considered the ‘comparison’.
Outcomes
Primary outcomes of interest were hip-specific PROMs. These included: Hip disability and Osteoarthritis Outcome Score (HOOS), Western Ontario and McMaster universities osteoarthritis Index (WOMAC), the International Hip Outcome Tool (iHOT), the Copenhagen Hip and Groin Outcome Score (HAGOS), NonArthritic Hip Score (NAHS), and the Oxford Hip Score (OHS).
The HOOS is a PROM used for patients with reduced hip function with or without hip osteoarthritis, consisting of 5 subscales (pain, symptoms, activities of daily living, sport/recreation and QOL) with a 0–100 score for each, with 100 being the best possible result. 30 In patients undergoing PAO the minimal clinically important difference (MCID) is 10.3 for pain, 10.2 for symptoms, 10.8 for activities of daily living, 12.6 for sport and recreation, and 11.2 for QOL. 31 The HOOS has also shown adequate internal consistency and external validity. 31
The WOMAC is a valid PROM for those with hip pain, consisting of 3 subscales (Pain, Stiffness, Function). 32 Each subscale is summated to a maximum score of 20, 8, and 68, respectively. A lower score indicates a lower level of pain or symptoms. Typically, it has been used in older patients with degenerative joint disease but has also shown to be sensitive in a younger population following PAO. 33 The minimal detectable change (MDC) has been reported as 5.51 for pain, 9.10 for function and 1.96 for stiffness, 31 and the MCID has been reported as 10.8 for pain, 12.9 for stiffness, 10.8 for function, in patients with DDH undergoing PAO. 33
The iHOT-33 is a PROM developed for younger active patients presenting with a variety of hip pathologies. Each score is out of 100, with 100 being the best score. It comprises of 33 questions relating to symptoms and functional limitations, sports and recreation activities, job-related concerns, and social, emotional and lifestyle concerns. The final score is then divided by 33. It has shown excellent validity and reliability with a minimal important change (MIC) of 6 and MDC ranging from 3.3 to 4.9 in those with hip pain.34,35
The HAGOS employs 6 subscales (symptoms, pain, function in daily living, function in sport and recreation, participation in physical activities, and QOL). Each subscale is scored from 0 to 100, with 100 being the best possible score. The HAGOS has also been used in patients following PAO and has been recently recommended one of the most appropriate PROMs to use in young and middle-aged active adults with hip-related pain.36,37
The NAHS was also developed for young active patients with higher demands and expectations. 38 It consists of 20 items distributed in 4 domains of pain, mechanical symptoms, functional symptoms, and activity level. The NAHS has satisfactory reliability and fair validity. 34
The OHS is a 12-question outcome measure assessing the patient’s hip pain and function. 39 It generates a total score ranging from 0 to 48, where 48 indicates best possible result. The MIC for individual patients has been reported as 8, though this was in a population undergoing THA. 40
Certain hip-specific PROMs were not eligible for inclusion in this systematic review due to their reported limitations in this population. The modified Harris Hip Score (mHHS) has been shown to have a lack of content validity and the presence of a ceiling effect.34,41 Similarly, the Hip Outcome Score (HOS) has also shown a ceiling effect and limited responsiveness following hip surgery. 41 Therefore, studies that used the mHHS or the HOS as the primary PROM were not included. Studies using the Merle d’aubigne score, University of California Los Angeles activity-level rating score (UCLA), and visual analogue scale (VAS) were also excluded as these PROMs are not hip-specific. Studies using generic health-related QOL questionnaires were also not included as the purpose of this systematic review was to evaluate hip-specific outcome measures.
Studies were excluded if: (1) no full text was available; (2) the study was an animal study; or (3) the study was written in a language other than English.
Quality evaluation
A modified version of the Downs and Black checklist was used to assess the quality of included studies. This modified version scores 18 potential criteria and has been used in other systematic reviews on hip pain. 42 Studies were considered high quality with a score of >60%. 42 Included studies were rated by 2 independent reviewers (MO, LR). Any disagreements between reviewers were discussed in a consensus meeting and an independent arbitrator (JK) was employed when consensus could not be met. Agreement between rates was determined using Cohen’s Kappa (K).
The Grades of Recommendation, Assessment, Development and Evaluation (GRADE) was applied to assess the quality of evidence for each meta-analysis.43,44 The overall GRADE certainty ratings include ‘very low’, ‘low’, ‘moderate’ and ‘high’. Observational data is initially graded at ‘low’ and can be increased or decreased for various reasons. 45 Certainty can be rated up for (1) large magnitude of effect, (2) dose response gradient, (3) all residual confounding would decrease magnitude of effect. Certainty can be rated down for (1) risk of bias (if mean modified epidemiology appraisal instrument scored <60%), (2) imprecision (if upper or lower confidence interval [CI]) spanned a standardised mean difference [SMD] or standardised paired difference [SPD] of 0.5 in either direction), (3) inconsistency (if I2 was ⩾25%), (4) indirectness (if clinically heterogeneous) and (5) publication bias (for example, small studies that are industry-sponsored).
Data extraction, synthesis and analyses
Data were extracted by 2 independent reviewers (MO, LR) into customised excel worksheets. The following data was extracted: author, year, country of origin, number of participants, demographic characteristics of participants (age, gender, body mass index [BMI], type of PAO), PROM scores, length of follow-up, and a summary of the findings was collated. Any discrepancies in data extraction were resolved by an independent reviewer (JK). A hierarchy of the different PROMs was decided on between authors to prioritise data extraction where more than one had been used, as recommended in the Cochrane guidelines. 28 The order of the hierarchy was based on the established level of validity and reliability of the PROM for young people with hip pain, and applicability to people with DDH undergoing PAO. In order of selection, the hierarchy was HOOS, WOMAC, IHOT, HAGOS, NAHS, OHS. Where data was insufficient, authors were contacted and asked to provide missing data.
Studies were grouped according to design including: (1) between-group studies or (2) paired-data studies assessing change between pre- and post-PAO. If studies used a similar subscale, such as pain or QOL, at similar time-points then we performed meta-analysis using the random effects model. For between-group results this was done using Review Manager (RevMan) (Version 5.4.1 The Cochrane Collaboration, 2020), with a SMD and 95% CI for continuous data. The SMD is a summary statistic used to combine results from different studies that have measured similar outcomes but with different scales. 28 For analysis of paired-data studies, a standardised paired difference (SPD) was calculated using R statistical software (version 4.0.4, Metafor package version 3.0-2). The SPD and 95% CI were calculated from the sample size, mean and SD of the difference between time-points. SMDs and SPDs of 0.2, 0.5 and 0.8 were interpreted as small, moderate and large effect sizes, respectively. 46 Subgroup analyses were performed for specific time-points. Statistical heterogeneity across the pooled data was assessed using an I2 statistic, with 25% considered low, 50% moderate and 75% as high levels of heterogeneity. 47
Where mean and SDs were not presented, we approximated mean scores from the median scores and SD from the range scores. 48 Studies that only included total scores for outcomes that require subgroup scores, were not included in meta-analysis. Where patients had undergone 2 PAO surgeries, data was taken only for the first PAO. Participants were also excluded if it was easily identifiable that they had significant concomitant pathologies (e.g. Down syndrome, Charcot Marie Tooth Disease, septic arthritis). If postoperative data were not provided but change scores were, then the postoperative mean was calculated as the difference between the preoperative score and the change score. The preoperative standard deviation [SD] score was used as the postoperative SD score if this was unable to be imputed, as per the Cochrane guidelines.33,49,50
Where individual studies were not sufficiently homogenous to be included in a meta-analysis, a best evidence synthesis was used to provide an overall rating for the body of evidence. 51 Grading of the best evidence synthesis was completed using previously published criteria.42,52 They were graded as strong (⩾2 studies with low risk of bias and ⩾75% agreement), moderate (⩾2 studies including at least 1 low risk of bias and ⩾75% agreement), limited (⩾1 moderate/high risk of bias studies, with ⩾75% agreement, or 1 low risk of bias study), conflicting (inconsistent findings <75% agreement), or no evidence.
Results
Search strategy
The search yielded 5017 titles and abstracts for screening. 124 full-text studies were screened, and 62 studies were excluded. 62 studies fulfilled the inclusion criteria and were included in this systematic review. An overview of the study identification process is provided in Figure 1.
Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) flow diagram.
Methodological quality
Supplemental Appendix 2 contains the results of risk of bias assessment using the modified Downs & Black checklist. Initial agreement between quality assessors was moderate (K = 0.546). 53 The methodological quality scores ranged from 39% to 94%,54,55 with an overall mean (SD) rating of 71% (11.6%). Of the included studies, 61 (98%) clearly described their aims or hypothesis and 60 (97%) outlined their main outcomes in the introduction or methods section. 17 studies (27%) stated if the main outcome measures used were valid and reliable, and only 8 studies (13%) provided characteristics of patients lost to follow-up.
Participants
The 62 studies included 8222 participants, with 6852 of these participants undergoing PAO. A proportion of these participants represent data-points that were published on multiple occasions. Sample sizes of the PAO groups ranged from 16 patients to 599 patients.56,57 The mean (SD) ages for patients in the included studies ranged from 17 years to 45 years.58,59 26 studies were single cohort studies which assessed PROM preoperatively and postoperatively, 29,30,32,35,48,58,60–80 3 studies compared those having PAO as a first-time surgery with those who have had previous arthroscopy,81–83 and 3 studies compared those having PAO with healthy controls.19,84,85
Outcome measures
17 studies used the HOOS, 33 studies used the WOMAC, 5 studies used the iHOT, 4 studies used the HAGOS, 3 studies used the NAHS, and no studies used the OHS. Study details are contained in Table 1. When a study used more than 1 of these questionnaires, only data from the highest-ranking PROM in our hierarchy was used.
Summary of included studies.
ACEA, anterior centre-edge angle; ADL, activities of daily living; AP, anteroposterior; CEA, centre-edge angle; CSI, corticosteroid injections; DDH, developmental dysplasia of the hip; FAI, femoroacetabular impingement; HAGOS, Copenhagen Hip and Groin Outcome Score; HOOS, Hip disability and Osteoarthritis Outcome Score; iHOT, International Hip Outcome Tool; IR, internal rotation; LCEA, lateral centre-edge angle; LCPE, Legg-Calvé-Perthes disease; MRI, magnetic resonance imaging; MRA, magnetic resonance arthrography; NA, not applicable; NAHS, Non-arthritic Hip Score; NR, not reported; NSAIDs, nonsteroidal anti-inflammatory drugs; PROM, patient-reported outcome measure; QOL, quality of life; ROM, range of motion; SCFE, slipped capital femoral epiphysis; UCLA, University of California Los Angeles; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
Result also included in meta-analyses.
Result not included in meta-analyses for one of the following reasons: single study for a particular outcome or timepoint, same cohort as another study, incomplete data provided.
PAO versus healthy controls
2 studies compared outcomes pre-operatively and postoperatively, between PAO patients and healthy controls, 1 high-quality prospective cohort study, and 1 high quality cross-sectional study.19,84 An additional high-quality cross-sectional study also compared the pain subscale only, between patients with DDH and healthy controls, preoperatively. 85 Meta-analysis of the preoperative time-point showed significantly worse pain (SMD [95% CI]: −4.05; −4.78 to −3.32) (Figure 2), activities of daily living (−2.81; −3.89 to −1.74) (Figure 3), QOL (−4.10; −4.43 to −3.77) (Figure 4), symptoms (−3.84; −4.36 to −3.29) (Supplemental Appendix 3), and sport & recreation (−3.47; −3.79 to −3.16) (Supplemental Appendix 4), for those undergoing PAO versus controls. Despite the large magnitude of effect found, the GRADE level of certainty of these pre-operative difference between PAO patients and healthy controls is low. This is due to inconsistency in data and risk of bias. 45
Forest plot comparing
Forest plot comparing
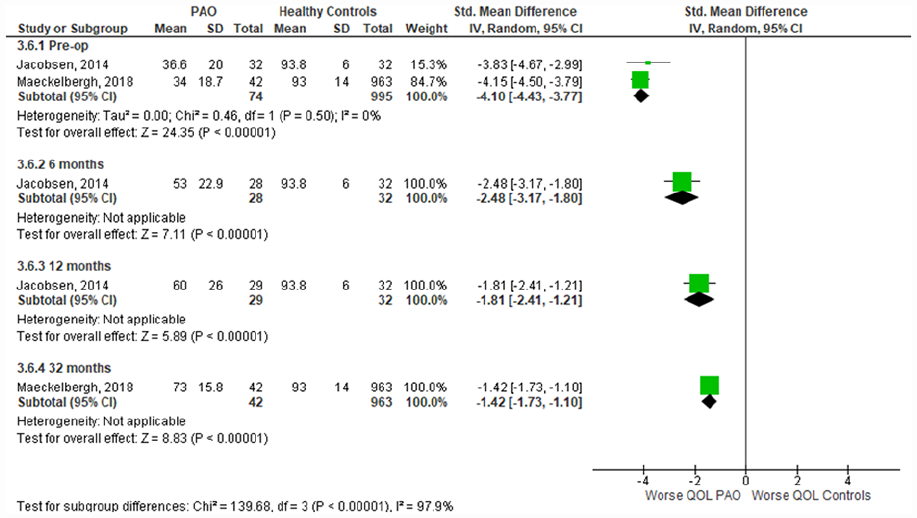
Forest plot comparing
Data were unable to be pooled for the postoperative time points as the studies used different follow-up time periods. Jacobsen et al. 19 reported follow-up data at 6 months and 12 months postoperatively, and Maeckelbergh et al. 84 reported 32 months postoperative data. Across all subgroups the PAO group had significantly worse outcomes than the healthy controls, at every time point. The magnitude of difference between healthy controls and those undergoing PAO has significantly reduced with time following PAO (p < 0.001).
Change from pre-op to post-PAO
9 studies measured change in pain in their respective cohorts following PAO (Supplemental Appendix 5). Meta-analysis of 3 studies reported an improvement at the 1-year time-point (SPD 1.35; 95% CI, 1.02–1.67; I2 = 80%). This included a prospective observational study, 31 a high-quality retrospective case series study, 85 and a high-quality prospective case series study. 36
A similar result was found at the 2-year timepoint (1.35; 1.16–1.54; I2 = 64%) with meta-analysis of 4 studies. A prospective observational study, 31 and 3 respective cohort studies, 33 2 of which were high-quality.30,72 Other included studies also reported improvement in pain at different timepoints, but meta-analysis was not possible at these timepoints as only single studies assessed the timepoint as shown in Supplemental Appendix 5.
Changes in activities of daily living (ADL) following PAO was measured in 5 studies (Supplemental Appendix 6). Meta-analysis of a prospective observational cohort study and a high-quality prospective case series showed improvement at the 1-year time-point (1.22; 1.09–1.35; I2 = 0%).31,36 This was also shown at the 2-year time-point (1.06; 0.90–1.22; I2 = 53%) with meta-analysis of 3 studies, 2 high-quality retrospective cohort studies and a prospective observational study. A single study also showed improvement at the 1.5 year timepoint (1.63; 1.23–2.02).
Improvements following surgery were also observed for QOL at 1-year (1.36; 1.22–1.5; I2 = 0%) and 2-year (1.3; 1.1–1.5; I2 = 65%) time-points (Supplemental Appendix 7), sport and recreation at 1-year (1.29; 1.01–1.57; I2 = 68%) and 2-year (1.24; 0.92–1.57; I2 = 87%) time-points (Supplemental Appendix 8), and symptoms at 1-year (1.16; 1.01–1.32; I2 = 16%) and 2-year (1.02; 0.79–1.25; I2 = 77%) time-points (Supplemental Appendix 9).
The improvements found across all subgroups from pre- to post- PAO surgery provide low level certainty that pain, ADL, QOL, sport and recreation, and symptoms improve following surgery. Despite the large magnitude of effect found, risk of bias of studies and inconsistency in data means the GRADE certainty rating remains at low. 45
Primary PAO versus PAO following arthroscopy
3 high-quality studies compared outcomes between those having a PAO as their first hip surgery, and those having a PAO following a previous arthroscopy.81–83 We were able to perform meta-analyses of 2 studies.81,82 The observational methodology of the studies means these results provide low level certainty that there was no significant difference preoperatively between both groups in pain (SMD 0.15; 95% CI, −0.38 to 0.68) (Supplemental Appendix 10), stiffness (−0.29; −1.10 to 0.52) (Supplemental Appendix 11) and function (−0.03; 0.90 to 0.84) (Supplemental Appendix 12).
1 study provided limited evidence showing despite similar baseline values (0.17; −0.31 to 0.65), those with previous arthroscopy had significantly worse outcomes at 6 months (1.08; 0.43 to 1.74) and 1 year (0.83; 0.22 to 1.44) post PAO compared to those who had not had previous arthroscopy, as measured by the iHOT-33. 83
Mild versus severe dysplasia
2 high-quality studies dichotomised their groups by their lateral centre-edge angle (LCEA) measurement.99,101 We were unable to pool the data from these studies because of differences in outcome measures used, and differences in the LCEA used to define both groups. Ricciardi et al. 83 compared those with a LCEA of 18–25° to those with LCEA of ⩽17° using the iHOT-33 at preoperative (−0.06; −0.57 to 0.45), 6-month (0.10 (−0.47 to 0.66) and 1-year time-points 0.05 (−0.64 to 0.73). 101 Møse et al. 99 compared those with a LCEA of 20–25° to those with a LCEA of <20° using the WOMAC Pain subscale preoperatively (0.20; −0.23 to 0.63) and at 2 years postoperative (0.00; −0.43 to 0.48).
This limited evidence shows no significant difference between groups with DDH pre-operatively or following surgery when dichotomised using LCEA.
Discussion
Our systematic review aimed to evaluate pain, function, and QOL in adults with DDH undergoing PAO, as assessed by PROMs. We found low level evidence that those with DDH undergoing PAO had significantly worse PROMs (pain, symptoms, activities of daily living, sport & recreation, and quality of life) preoperatively compared with healthy participants. Patients do improve following PAO surgery, and these improvements appear to be maintained for the 7 years of data we have available. Despite these improvements, post-operatively patients do not return to the same level of pain, function, and QOL as healthy participants for the 3-year period following surgery.
We dichotomised results for patients with DDH based on their LCEA, into mild versus severe dysplasia. There is growing recognition that the diagnosis of DDH is more complex than just examining the LCEA, and probably involves multiple variables in the pattern of dysplastic morphology. 3 The Ottawa classification system, as an example, identifies a proportion of dysplastic patients who have no lateral acetabular deficiency. 16 There is also a greater recognition that variations in hip morphology are common in those who do not have symptoms,108,109 implying that while morphology is a factor potentially influencing the severity of a patient’s symptoms, it may not be the primary driver of pain.
Surgical complications are known to affect pain and activity in these patients but was not evaluated in this systematic review.26,27 Though the PAO is considered a safe procedure with low levels of complications,106,110 a recent study reported bony non-union as the most common major surgical complication at 12%, with 26% of these patients being symptomatic requiring open reduction and internal fixation. 110
There are a number of orthobiologic products utilised in other surgeries that have been shown to enhance bone grafts and provide higher rates of fusion in spinal orthopaedic surgery. 111 However, it is unknown whether these are effective in PAO surgery or improve outcomes such as pain or QOL. There has also been no synthesis of the evidence in relation to PAO surgery. Understanding complications that potentially affect long-term pain and activity and possible solutions for such complications warrants further investigation.
We only investigated differences in patient-reported outcomes, between patients with DDH undergoing PAO and healthy participants in this systematic review. However, similar deficits have been shown in this cohort in individual studies investigating physical impairments.5,15,26,31,32,34,60 A synthesis of the evidence relating to physical impairments would provide greater understanding of how these patients present physically. Understanding physical impairments may also help inform pre- and postoperative rehabilitation by allowing clinicians to target these impairments in rehabilitation programs. These young adults may wish, and should be encouraged, to return to sport and physical activity. 10 While this was not investigated in our review, future studies should explore this important domain.
This review contains several limitations that should be acknowledged. Firstly, there were no randomised controlled trials, and a large proportion of retrospective studies, which have implications for introducing selection, performance and detection bias. Included studies demonstrated considerable variability in the risk of bias, outcomes reported, and post-operative assessment timepoints, which limited opportunities for meta-analysis. Included studies had poor transparency in describing characteristics of patients lost to follow-up, and a lack of validity and reliability for main outcome measures. The above factors rendered it impossible to obtain findings with ‘high’ level evidence and certainty ratings. 43 Longitudinal studies are critical to investigate potential causality and better understand the relationships between pain, function and QOL in patients with DDH undergoing PAO.
Adults with DDH undergoing PAO have more pain and worse function and QOL scores compared to healthy participants. Patients do improve following PAO surgery, and maintain this improvement, but they do not to the same level as their healthy participants. Our findings are important to patients and clinicians when considering PAO surgery, to appropriately manage expectations of recovery, thus enhancing the shared decision-making process, weighing up benefits of surgery against risks.
Supplemental Material
sj-pdf-1-hpi-10.1177_11207000231179610 – Supplemental material for Pain, function and quality of life are impaired in adults undergoing periacetabular osteotomy (PAO) for hip dysplasia: a systematic review and meta-analysis
Supplemental material, sj-pdf-1-hpi-10.1177_11207000231179610 for Pain, function and quality of life are impaired in adults undergoing periacetabular osteotomy (PAO) for hip dysplasia: a systematic review and meta-analysis by Michael JM O’Brien, Adam I Semciw, Inger Mechlenburg, Lisa CU Tønning, Chris JW Stewart and Joanne L Kemp in HIP International
Footnotes
Acknowledgements
The authors would like to acknowledge the following people for providing additional information from their included study to assist our data analysis: Robert Cates, D.O.; Line Borreskov Dahl; Lea Franken; Jitendra Balakumar; and Julie Jacobsen.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.