
Abstract
Association between mild to moderate hypertension and headache is probably coincidental. Severe sustained hypertension, malignant hypertension and paroxysmal hypertension (sudden rise) are associated with severe headache. Transient hypertension can occur during an attack of migraine or cluster headache. Hypertension may increase the frequency and severity of migraine in migraineurs and may transform an episodic migraine into chronic daily headache. Concomitant treatment of hypertension is important in these patients.
Both hypertension and migraine are very prevalent disorders in the general population, of which approximately 10–20% suffer from each of these disorders. The prevalence of episodic tension-type headache is between 50–70%, whereas chronic tension-type headache occurs in 3% of the population. Because of this very high prevalence of primary headache disorders, it is possible that the same person may have headache and hypertension purely by coincidence. However, presence of hypertension in a migraineur may lead to more frequent and severe headache and will definitely affect the treatment strategies.
Headache and hypertension
Epidemiological studies
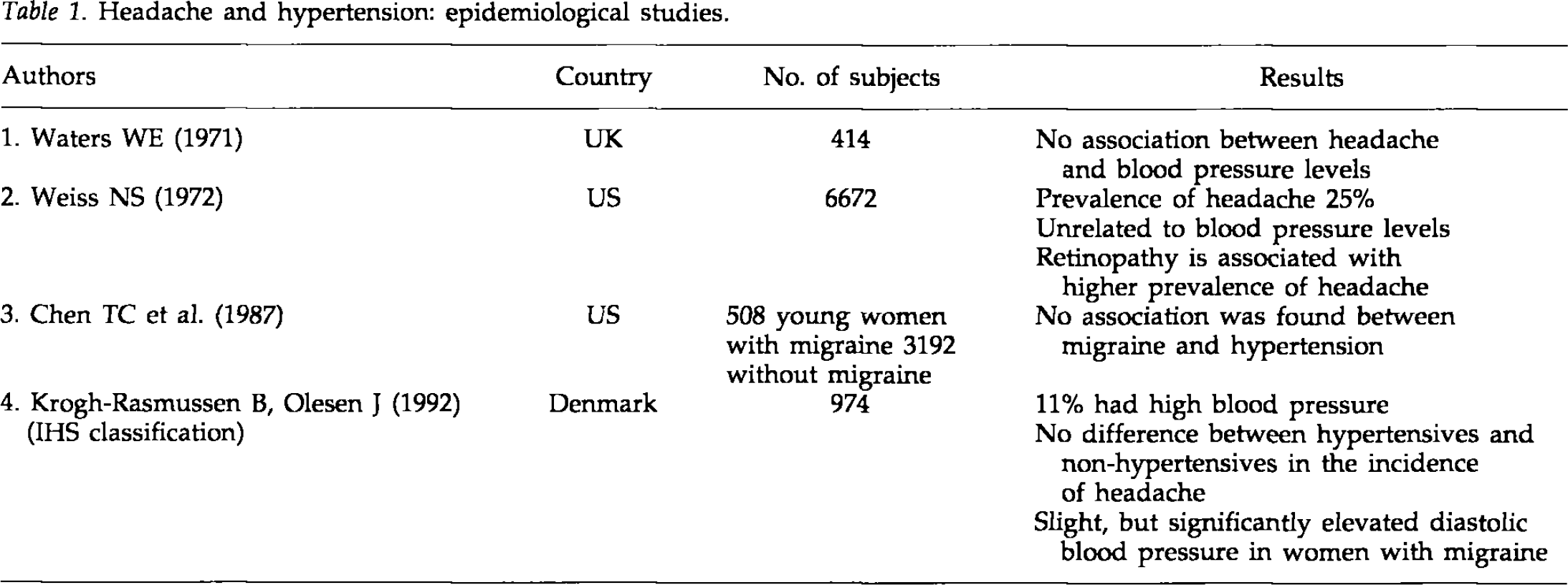
Table 1 summarizes four major studies that looked at the relationship between headache and hypertension. Waters in 1971 (1) surveyed 414 subjects and found no association between headache and blood pressure levels. Weiss in 1972 (2) on surveying 6672 hypertensive patients found the prevalence of headache to be 25% in that population. These headaches were concluded to be unrelated to the level of blood pressure. Retinopathy was found to be associated with a higher prevalence of headache in that series. Chen et al. in 1987 (3) compared 508 young women with migraine and 3902 without migraine. They found no association between migraine and hypertension. The first population survey using IHS criteria for headache classification to study hypertension and headache was done by Krogh-Rasmussen et al. (4) in 1992. Nine hundred and seventy-four subjects were interviewed and examined. Eleven percent had high blood pressure. No difference between hypertensives and nonhypertensives was found in the incidence of headache. Slight, but significantly elevated diastolic blood pressure was found in women with migraine.
Headache and hypertension: epidemiological studies.
Clinical studies
Table 2 summarizes three studies done in clinic settings that examined the relationship between hypertension and headache. Badran et al. in 1970 (5) compared 100 hypertensives with 100 controls and found that prevalence of headache in normotensives was 39%, in patients with mild to moderate hypertension it was 36%, and in patients with severe hypertension (diastolic blood pressure above 130 mm of mercury) it was 50%. It appeared that mild to moderate hypertension was not associated with increased incidence of headache. These authors did not break down the data into migraine or tension-type headache. Bulpitt et al. in 1976 (6) found that 31% of untreated hypertensives complained of headache, whereas the incidence of headache in treated patients and normal controls was only 15%. Cooper et al. in 1989 (7) studied 11 710 hypertensives and concluded that headache was common and was related to blood pressure levels.
Headache and hypertension: clinic studies.

Clinical experience
There are very few studies that clearly elucidate the relationship between migraine and hypertension. Common clinical observations can be summarized as follows (8, 9). In mild or moderate hypertension, there is no significant correlation of the degree of headache and level of blood pressure. In persistent uncontrolled hypertension or malignant hypertension, headache is at least partially related to the degree of hypertension. A sudden rise in blood pressure, as in the case of pheochromocytoma, is invariably associated with severe headache.
In hypertensive migraineurs, hypertension may increase the frequency and severity of migraine. Hypertension has been indicated as one of the factors that can transform episodic migraine into chronic daily headache (10, 11). Clinical experience also tells us that coexistent hypertension in a migraine patient should be treated adequately.
Reactive rise in blood pressure during severe headache
During migraine and cluster headache attacks, blood pressure may become elevated. Usually such elevation is transient and is partly attributable to the anxiety associated with attacks. It is important to measure blood pressure outside the migraine attack to determine whether the patient is hypertensive or not.
Pathophysiology of hypertensive headache
The pathophysiology of hypertensive headache is assumed to be predominantly vascular, although tension-type headache seems to occur in such patients partly because of the anxiety about and awareness of elevated blood pressure. Hypertensive dilatation or stretching of resistance blood vessels of the brain is extended as an explanation for severe headache occurring with rapid rise in blood pressure. Failure of cerebral autoregulation may occur at extreme levels of blood pressure, which may result in brain edema and subsequent intracranial hypertension. This scenario is evident in hypertensive encephalopathy, which is invariably associated with severe headache.
Paroxysmal hypertensive headaches
The most dramatic concurrence of hypertension and headache occurs in disorders associated with paroxysmal rise in blood pressure to very high levels. These are listed in Table 3. In these conditions, particularly in pheochromocytoma, eclampsia and pre-eclampsia, there is a rapid rise in blood pressure. In malignant hypertension, a hypertensive crisis can occur, with neurological symptoms such as extreme dizziness, seizures and alteration in consciousness.
Paroxysmal hypertension and headache.
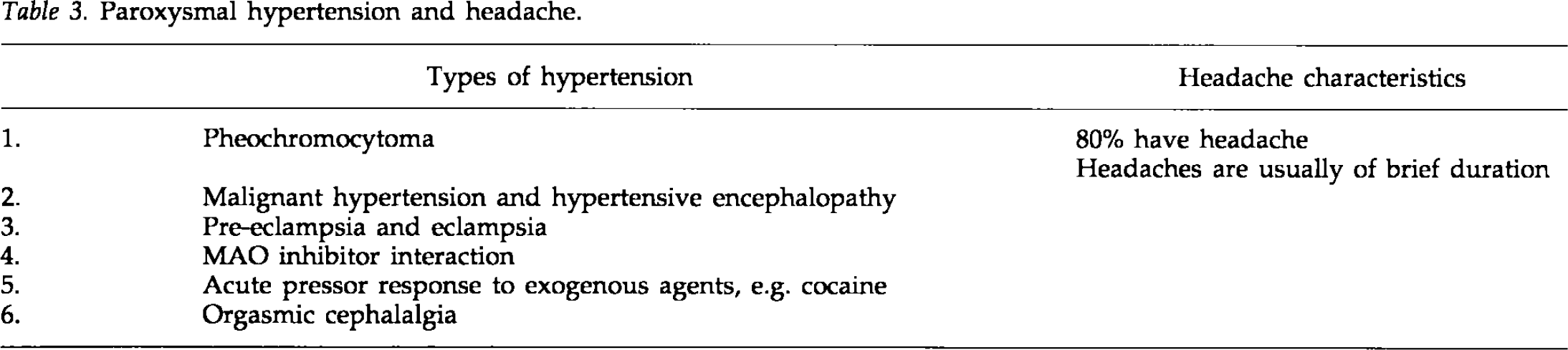
Sudden rise in blood pressure during sexual intercourse may be a pathogenic mechanism of at least some orgasmic cephalalgia patients.
Antihypertensive causing headache
It is well known that certain antihypertensives produce headache as a side effect. These include reserpine, which depletes central and platelet serotonin, vasodilator drugs such as hydralazine, and calcium channel blocking agents like nifedipine. It is advisable to avoid such drugs in patients with migraine in treating their hypertension.
Conclusion
Although there are no major population studies, from clinical experience and reports from the literature, the following can safely be concluded:
Association between mild to moderate hypertension and headache is probably coincidental.
Severe sustained hypertension, malignant hypertension and paroxysmal hypertension (sudden rise) are associated with severe headache.
Transient hypertension can occur during an attack of migraine or cluster headache.
Hypertension may increase the frequency and severity of migraine in migraineurs and may transform episodic migraine into chronic daily headache.
Concomitant treatment of hypertension is important in these patients.