
Abstract
Background
Post-traumatic headache (PTH) is typically described as migraine- or tension-type-like and treated based on presentation. However, the actual presentations of PTH are not well characterized. The aim of this study is to provide a phenotypic characterization of persistent PTH and co-occurring neurological symptoms from a previously completed clinical trial and characterize PTH treatment utilization.
Methods
This study is a secondary analysis of veterans (N = 193) recruited to participate in a randomized clinical trial of cognitive-behavioral therapy, cognitive processing therapy, or treatment as usual for PTH. Descriptive statistics were examined across characteristics of PTH, including age, gender, neurobehavioral symptoms, headache-related disability, pain characteristics, pain locations, accompanying symptoms, and aura symptoms and treatment utilization.
Results
The median presentation of PTH in this study was a headache with severe pain, lasting about 4 h, and with about 13 headache episodes per month. About half the participants reported a pulsating quality and/or nausea that accompanied head pain. Most characteristics were uncorrelated to each other. The majority of participants used medication to treat persistent PTH. Neurostimulation was the most common non-pharmacological treatment.
Conclusions
The results of this study show that characteristics associated with migraine are more frequently reported with PTH. Correlations among the migraine characteristics were moderate overall, and there was notable variability among reported characteristics of PTH. Treatment utilization for PTH was not associated with current neurobehavioral symptoms and included both pharmacological and non-pharmacological options.
Trial Registration
ClinicalTrials.gov Identifier: NCT02419131.
This is a visual representation of the abstract.
Introduction
According to the Traumatic Brain Injury (TBI) Center of Excellence, there have been 515,885 reported cases of TBI among U.S. Armed Forces service members between the years 2000–2024 (1). Post-traumatic headache (PTH) is one of the most frequent sequela after a head injury (2). Couch and Stewart reported that sequelae such as headaches can persist with little improvement up to 8 years after a deployment-related head injury (3). According to The International Classification of Headache Disorders-3 (ICHD-3) criteria, persistent headache attributed to traumatic injury to the head includes any headache temporally attributable to a head injury that persists for greater than 3 months (4). There are no phenotypic criteria for PTH provided by the ICHD-3, although it is acknowledged that they often resemble tension-type or migraine headaches.
In a literature review, Ashina and colleagues highlighted this gap and noted that treatment is often based on whether the PTH has a migraine- or tension-type-like presentation (5). However, there is no clear evidence in the extant literature that treatment of PTH based on its nearest resemblance to a primary headache type is an effective approach. More recently, Ihara and Schwedt proposed that PTH is distinct from migraine (6). The current ICHD-3 criteria for PTH indicate that the PTH could be a worsening of a previous headache (e.g., prior migraine) or a new headache altogether attributable to a head injury. In essence, this means that there could be different sub-types (e.g., worsened migraine, worsened tension-type headache, new or mixed phenotype) of PTH that can affect functioning and could differentially respond to a treatment. Unremitting head pain is one such characteristic that is not typically observed with migraine or tension-type headaches.
Active duty military personnel with unremitting head pain due to head injury have been found to be more likely to retire or be medically discharged compared to individuals with episodic PTH (7). The researchers also found a strong association between frequent medication use for PTH and retirement or medical discharge. Finkel and colleagues suggested that headache characteristics, and not primary headache type, are more important regarding separation from service (8). A study of civilians with PTH showed that higher head pain intensity was associated with lower likelihood of returning to work after a head injury (9). Peña et al. found that a model including age, trait anxiety, and headache frequency explained almost half the variability of PTH related disability (10). However, the authors only looked at the phenotypic characteristics of head pain duration, frequency, and intensity.
Post-concussive symptoms after a TBI are associated with higher rates of health service utilization and pain medication use (11). A review by Minen et al., described several medical treatments that have been used for PTH such as non-steroidal anti-inflammatory drugs, triptans, anticonvulsants, antidepressants, prazosin, calcitonin-gene related receptor antagonists, and onabotulinum toxin A injections (12). The authors also noted that research has been conducted on non-pharmacological treatments for PTH such as cognitive behavioral therapy and transcranial magnetic stimulation. In a prior randomized controlled trial of cognitive behavioral therapy for post-traumatic headache (13), medication use reported at baseline was consistent with medications reported by Minen and colleagues (12). However, utilization of other treatments for headache management (e.g., chiropractic, massage, physical therapy, acupuncture) were not previously reported from this dataset.
To our knowledge, no studies have attempted to characterize the varied post-concussive symptoms and treatments used to attenuate PTH symptoms. Thus, the aims of this study are to address these characterization gaps by providing (1) a phenotypic characterization of persistent PTH and co-occurring neurobehavioral symptoms from a previously conducted clinical trial and (2) characterization of headache treatments used within 6 months of study participation. We also hypothesized, a priori, that greater presence of co-occurring neurological symptoms at baseline would be associated with greater treatment utilization for headache (both pharmacological and non-pharmacological), while controlling for headache days per month.
Methods
This study is a secondary, cross-sectional analysis of baseline data from a completed randomized controlled trial of cognitive behavioral therapy for post-traumatic headache (13). Complete details on the research methods, participant demographics, and primary outcomes have been previously published (13,14). The original trial was approved by the Institutional Review Board (IRB) of the University of Texas Health Science Center at San Antonio that served as the single IRB of record for the South Texas Veterans Health Care System, Wake Forest School of Medicine, Duke University Health System, and VA Boston Healthcare System. The United States Army Medical Research and Development Command Human Research Protection Office oversaw all regulatory actions.
Between 2015 and 2019, 193 veterans were enrolled into the original study. For inclusion, participants needed to have at least one deployment to Iraq or Afghanistan. Individuals with clinically significant changes in headache symptoms in the 6 months prior to screening were excluded. Individuals with moderate to severe TBI or headaches attributable to whiplash injury were excluded. Individuals who met criteria for medication overuse headache (MOH) were excluded. Pregnancy was also an exclusion-criteria because pregnancy can alter the presentations of headaches.
To be included in the study, veterans needed to meet ICHD criteria for persistent PTH and the presence of symptoms of post-traumatic stress disorder (PTSD). Diagnostic interviews and confirmation by a physician were done to ensure that criteria were met for persistent headache attributable to mild traumatic brain injury (ICHD-3 5.2.2) (4,15). Participants additionally needed to meet Diagnostic and Statistical Manual of Mental Disorders, 5th Edition PTSD criterion A (exposure to a traumatic event) and B thresholds (at least one intrusion symptom).
The original RCT included three arms consisting of treatment as usual, 8-sessions of cognitive behavioral therapy for PTH, or 12-sessions of cognitive processing therapy (13). Participants assigned to treatment as usual were instructed to follow their routine clinical care, which may have consisted of one or more treatments such as pharmacological treatment, interventional pain management (e.g., onabotulinum toxin A injection), physical therapy, or complementary and integrative health treatments (e.g., acupuncture). Study follow-up periods of 1-, 3-, and 6-months were conducted, but only baseline data were used for this secondary analysis. Independent evaluators blinded to treatment conditions were used to minimize any bias in data collection at baseline and follow-up periods.
Measures
Measures used included the headache impact test (HIT-6),which is a self-report measure of impairment of headaches on daily functioning (higher scores mean greater impairment) (16). The HIT-6 scores range from 36–78 with an item scale that includes “never” (6 points), “rarely” (8 points), “sometimes” (10 points), “very often” (11 points) and “always” (13 points). The HIT-6 has high internal consistency (α between 0.75 and 0.92) (17).
The structured diagnostic interview for headaches (SDIH-revised) was used to assess headache presentations (18). The structured interview captures headache characteristics including numeric pain rating (0–10), pain location(s), pain quality (e.g., pulsating, pressing), frequency, duration, factors that may aggravate head pain (e.g., movement, light, noise), nausea, vomiting, and aura symptoms if present.
The Neurobehavioral Symptoms Inventory (NSI) has 22-items and was used to capture information of co-occurring symptoms that may be present after a TBI (19). The NSI has been tested in veterans and has high internal consistency (α = 0.95) (20). Treatment utilization was defined as a total number of treatments for headache reported at baseline in which each separate pharmacological or non-pharmacological approach (e.g., massage, chiropractor, physical therapy, neurostimulation, cold or heat) implemented within the previous 6 months counted as a treatment.
Analytic strategy
The present study characterized phenotypic features of PTH, and headache management treatments used within 6 months of study enrollment. This was a secondary analysis of this study. Because the sample size for this study was based on the available data from the original randomized controlled trial, we did not conduct an a priori power analysis. The analyses, which were conducted using R software, are both exploratory and hypothesis driven. Descriptive statistics were examined for characteristics of post-traumatic headache and treatment utilization. Tests of normality were conducted to make sure assumptions of normality are met and nonparametric test statistics were used when appropriate.
Correlations were conducted to determine relatedness between phenotypic features of PTH and headache disability. Tetrachoric correlations were calculated for dichotomous versus dichotomous variables. Point bi-serial correlation coefficients were used for dichotomous versus continuous variables. Kendall's Tau rank correlation coefficients were used for continuous versus continuous variables. Correlations were calculated using pair-wise deletion and two-tailed testing with a cutoff of < .05 for statistical significance. For the hypothesis that co-occurring neurological symptoms would be positively correlated with greater treatment utilization, a nonparametric partial correlation using a general matrix formula was calculated using the ‘ppcor’ package in R. Missingness was <1% across the baseline data and no adjustments for missing data were made.
Results
No imputations or other methods were used to adjust for missing data; therefore, some results are based on 192 of the 193 total study participants. Participants in this study were mostly male (167/192; 87.0%) with a mean age of 39.7 years (SD = 8.4). Basic descriptives, including counts and percentages, are presented in Table 1. The median presentation of PTH was a headache with severe pain, lasting approximately 4 h, and with about 13 headache episodes per month. The “years at same frequency” means that these individuals reported experiencing these headaches at the same rate for a median of 7 years without any significant change (per self-report during the SDIH-R interview). Head pain located in the frontotemporal and vertex regions was commonly reported. Half the participants (96/192; 50.0%) reported a pulsating quality with the head pain. About half of the participants (103/193; 53.4%) reported nausea with typical head pain episodes and nearly 4 out of 5 (153/193; 79.3%) reported photophobia associated with the head pain. Nearly three-fourths of participants (141/192; 73.4%) reported bilateral pain. Of the 59 individuals that reported aura symptoms, scotoma, vertigo, tinnitus, and dysarthria were most prevalent.
Variable characteristics.

NSI = Neuropsychological Symptoms Inventory;
HIT-6= Headache Impact Test-6 Item;
Freq = Frequency of Headaches.
Correlations between several phenotypic variables of PTH can be found in Table 2. Most correlations among variables did not reach statistical significance (p < 0.05). Of the correlated variables, mostly low to moderate correlations were found. Pain severity was weakly correlated with 10 other phenotypic variables and vomiting was correlated with 9 other phenotypic variables. Photophobia, phonophobia, nausea, vomiting, aura symptoms, and movement worsening the head pain had several moderate correlations among them.
Correlations among headache variables.
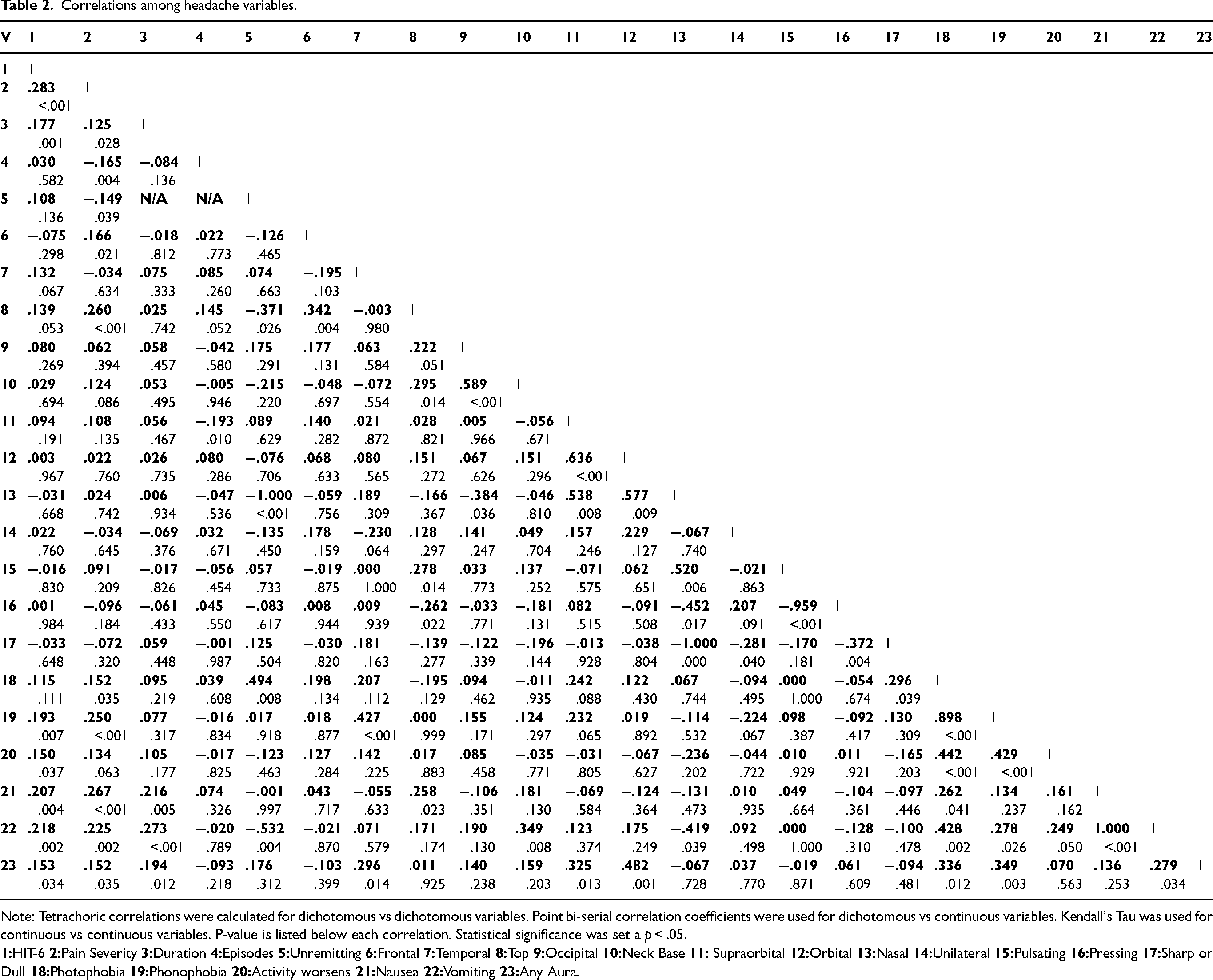
Note: Tetrachoric correlations were calculated for dichotomous vs dichotomous variables. Point bi-serial correlation coefficients were used for dichotomous vs continuous variables. Kendall's Tau was used for continuous vs continuous variables. P-value is listed below each correlation. Statistical significance was set a p < .05.
Treatments used for PTH pain in the 6 months prior to the baseline assessment of the study are listed in Table 3 (excluding oral headache medications) and in Figure 1. Treatment patterns are described based on participant report, but do not provide information about the efficacy of the treatments used. The majority of individuals (150/193; 77%) used an oral medication for headache management. Of the individuals who used a treatment not including oral medications (n = 107), neurostimulation was the most common non-pharmacological treatment used. Onabotulinum toxin A injections, physical therapy, and chiropractic services were less frequently used for headache management. “Other” treatments for headache management included heat, cold, massage therapy, transcutaneous electrical stimulation, magnesium supplementation, power breathing, meditation, sunglasses, occupational therapy, and low-level laser therapy. “Other injections” included steroid, triptan, or vitamin B12 injections. Of 115 individuals for which detailed oral headache medication usage information was available (see Figure 1), non-steroidal anti-inflammatory drugs (NSAIDs) were most commonly used (71%), followed by acetaminophen (37%), triptans (32%), and opioids (10%). Less than half of the participants (48/115; 42%) used more than one headache medication at baseline.

Oral medication use at baseline (N = 115 for detailed medication use). Note: Med = Medication; NSAID = Non-steroidal anti-inflammatory drug; Aceto = Acetaminophen.
Headache treatments excluding oral medications (n = 107).

Note: Within 6-months of baseline. Some individuals used more than one treatment.
The internal consistency for the NSI was α = 0.92. The hypothesis that greater presence of co-occurring neurological symptoms at baseline will be associated with greater treatment utilization for headache (both pharmacological and non-pharmacological), while controlling for headache days per month was not supported (partial correlation was r = .030, p = .539).
Discussion
The main findings of this study support that the phenotypic presentations of PTH vary widely. Post-traumatic headache (PTH) in treatment-seeking veterans tends to present with migraine-like characteristics such as high pain severity, duration, pulsating quality, photophobia, phonophobia, nausea, and head pain aggravated by movement. Bilaterality of head pain presentation was more common in the present sample, which differs from the typical presentation of migraine. The more frequently observed migraine characteristics in this sample may explain the high headache related disability scores at baseline assessment.
Both pain severity and headache related disability scores had weak to moderate correlations with several of the characteristics typically associated with migraine. This may suggest that PTH phenotypes are not truly migraine; however, the definition of PTH allows for either a new headache or worsening of a prior headache due to head injury. In this study, there was no variable collected to distinguish between new versus worsening of a prior existing headache. Thus, the weak to moderate correlations among characteristics of migraine may reflect PTH that was a worsening of a previously existing primary headache. An area for further study is to determine whether there are differences between PTH that is a worsening of a prior existing headache (e.g., prior migraine, prior tension-type headache) compared to PTH that is a never previously experienced head pain attributable solely to TBI.
The nature of the head injury may influence PTH phenotype. Previous study of this sample showed that 66% of the individuals were exposed to a blast injury prior to the subsequent development of PTH (blast head injury only (48%), blunt head injury only (34%), and both blast and blunt head injury in the same event (17%)) (21). Civilians, on the other hand, are not typically exposed to blast injuries and may differ in PTH phenotypes. A study of 100 civilians, mostly female, had PTH with primary migraine-like characteristics (22). Individuals in the present study had symptoms of post-traumatic stress which may influence PTH presentations. Further study of persistent PTH in active-duty military personnel is needed to confirm whether the characteristics presented in this study are observed at similar rates.
The head pain characteristics assessed in this sample were for individuals who had PTH episodes at the same rate for 1 to 39 years, with a median of 7 years. The time between head injury related to the PTH and baseline assessment for this study was 8.3 years on average,(21) which indicates that the frequency of headaches episodes tends to be stable over time for this population with persistent PTH. While it is possible for headache presentations to change over time, it is unknown if the presentations captured in this study (i.e., for bilaterality) are representative of the initial acute phase presentations. Rather we suggest that the phenotype presented in this study is representative of persistent PTH attributable to mild TBI in veterans with PTSD symptoms. Pharmacological treatment of PTH is often based on the nearest resembling phenotype (i.e., migraine or tension-type) and there is no evidence that this approach is effective (23).
Treatment utilization in this study was primarily pharmacological even though there are no clear pharmacological guidelines for treatment of PTH. Individuals using oral medications primarily used NSAIDs, acetaminophen, or triptans. This may reflect the easier accessibility of NSAIDs and acetaminophen compared to prescription drugs. Medication overuse headache was an exclusion criterion for this study; however frequent use of pain medications, even when used for other pain conditions, can lead to MOH. Considering a median of 13 head pain episodes per month found in this study, use of medications for pain episodes could increase risk for development of MOH. Practitioners working with individuals with PTH may want to regularly review pain medication usage to determine if an additional MOH is present. A significant proportion (40%) were also using a neurostimulation device for headache management, although the efficacy of these devices for PTH management is unknown. Treatment utilization was not correlated with presence of neuropsychological symptoms.
The sample size in this study is large for an interventional trial of PTH and provides detailed information about characteristics of persistent PTH in veterans and treatment utilization. The correlations found between PTH characteristics do not allow for causal inferences which is a limitation of this study, although the weak correlations among variables do support that there may not be a single, clear, categorical phenotype of persistent PTH. Further research is needed to determine the generalizability of these findings across populations including civilians, active duty military personnel, and veterans without PTSD symptoms.
Clinical implications
Post-traumatic headache in treatment seeking veterans tends to present with migraine-like characteristics and over the counter pain medications for PTH are primarily taken, although efficacy of these medications is unknown.
Further research is needed to provide guidance of medication management of PTH and due to the chronic nature (> 15 headache days per month) observed for nearly half the individuals in this study.
Practitioners may want to consider periodically discussing over the counter pain medication use when working with patients with persistent PTH.
Footnotes
Abbreviations
Author note
Disclaimer: The views expressed herein are solely those of the authors and do not reflect an endorsement by or the official policy or position of the U.S. Army, the U.S. Air Force, the Department of Defense, the Department of Veterans Affairs, or the U.S. Government.
Acknowledgments
The authors acknowledge Julie Collins for the research support on this project.
Author contributions
Study concept and design: Paul S. Nabity, Cindy A. McGeary, Blessen C. Eapen, Timothy T. Houle, Patricia A. Resick, John C. Moring, David E. Reed II, Carlos A. Jaramillo, Donald B. Penzien, Terence M. Keane, Stacey Young-McCaughan, Alan L. Peterson, and Donald D. McGeary. Analytic planning and/or analyses: Paul S. Nabity and Timothy T. Houle. Interpretation and discussion of results: Paul S. Nabity, David E. Reed II, Cindy A. McGeary, Patricia A. Resick, Brett T. Litz, and Donald D. McGeary. Drafting the Manuscript: Paul S. Nabity, Cindy A. McGeary, Patricia A. Resick, John C. Moring, David E. Reed II, Timothy T. Houle, Dr Alan L. Peterson, and Donald D. McGeary. Revisions for intellectual content and final approval of completed manuscript: All authors were involved in the revision process and final approval.
Consent to participate
Not applicable, secondary study.
Consent for publishing
Yes.
Data availability statement
The data used for this article may be obtained from the authors with a reasonable request.
Declaration of conflicting interests
Paul S. Nabity reports research funding from the Department of Defense (DoD), the Department of Veterans Affairs (VA), The National Institutes of Health (NIH). David E. Reed reports research funding from the DoD, VA, and NIH. Cindy A. McGeary reports research funding from the DoD, VA, and NIH. Blessen C. Eapen reports research funding from the DoD and VA. Timothy T. Houle reports research funding from the DoD and NIH and serving on the editorial boards of the American Society of Anesthesiology and the American Headache Society. Carlos A. Jaramillo reports research funding from the DoD and VA. Patricia A. Resick reports receiving consultation support from the NIH, royalties from therapist manuals, paid honoraria for lectures, and training workshops. Donald B. Penzien reports research funding from the DoD, VA, NIH, and Salisbury Foundation for Research and Education. Brett T. Litz reports research funding from the DoD, VA, and NIH. Terence M. Keane reports research funding from the DoD, VA, and NIH. Stacey Young-McCaughan reports research funding from the DoD, VA, and NIH. Alan L. Peterson reports research funding from the DoD, VA, NIH, the Bob Woodruff Foundation (BWF), the Texas Veterans and Family Alliance (TV&FA), and the Navy SEAL Foundation. Donald D. McGeary reports research funding from the DoD, VA, and NIH.
Ethical considerations
The original trial was approved by the institutional review board (IRB) of the University of Texas Health Science Center at San Antonio that served as the single IRB of record for the South Texas Veterans Health Care System, Wake Forest School of Medicine, Duke University Health System, and VA Boston Healthcare System. The United States Army Medical Research and Development Command Human Research Protection Office oversaw all regulatory actions.
Funding
This research was supported by Consortium to Alleviate PTSD (CAP) award numbers W81XWH-13-2-0065 from the U.S. Department of Defense, Defense Health Program, Psychological Health and Traumatic Brain Injury Research Program (PH/TBI RP), and I01CX001136-01 from the U.S. Department of Veterans Affairs, Office of Research & Development, Clinical Science Research & Development Service. Additional funding was provided by the U.S. Department of Defense Traumatic Brain Injury and Psychological Health Research Program award HT9425-24-1021 and HT9425-23-1-1046.
Open practices
Not applicable.