
Abstract
Introduction: Our study objective was to investigate the mode of occurrence of traumatic head injury in episodic cluster headache and migraine patients.
Methods: We conducted a retrospective study on 400 male patients, 200 with cluster headache (cases) and 200 with migraine (controls). We investigated the frequency and mode of occurrence of traumatic head injury and some lifestyle habits.
Results: The number of traumatic head injuries was significantly higher in cases than in controls (adjusted odds ratio [OR] = 2.0; 95% confidence interval [CI] = 1.5–2.8). Cases were more often responsible for the head traumas (adjusted OR = 2.6; 95% CI = 1.3–4.9) and reported a significantly higher proportion of injuries during scuffles or brawls (OR = 6.5; 95% CI = 2.9–14.8). Compared with other cluster headache patients, cases responsible for traumatic head injuries were more frequently heavy alcohol (p = .000), heavy tobacco (p = .03) and heavy coffee consumers (p = .003).
Conclusions: Cluster headache patients (a) had traumatic head injuries more frequently than migraineurs; and (b) were more often responsible for them, perhaps due to particular behaviours related to their lifestyles.
Introduction
Cluster headache (CH) is a severe, debilitating headache that occurs in about one to three people per 1000 of the general population (1,2).
Several authors have suggested a relation between traumatic head injury (THI) and CH (3–6), but the nature of this relation is still unclear (7). A few case reports indicate a causal relationship between THI and CH, suggesting that functional or organic alterations of intra- or extracranial nervous structures may predispose to CH onset (8).
An alternative hypothesis is that CH sufferers develop distinctive lifestyles (9), perhaps as a result of peculiar personality traits: males with episodic CH seem to be more anxiety-prone, less successfully socialised and with more hostile attitudes toward others than controls (10–12). The high rate of THI may then represent only an epiphenomenon of these individuals’ behaviour, which includes the tendency to overindulge in non-essential consumption habits such as cigarette smoking and heavy alcohol and coffee consumption (4,13). To define the behaviour of episodic CH male patients with respect to THI, we evaluated the frequency and clinical features of THIs, how they occurred and whether the patients themselves were responsible for the situation in which they occurred. We also investigated such patient habits as cigarette smoking and alcohol and coffee consumption.
Patients and methods
We conducted a retrospective case-control study. The case group included 200 male patients with episodic CH consecutively referred to the Headache Centre of the University of Parma Department of Neuroscience from 1 January 2004 through 31 January 2008. The control group consisted of 200 male patients with migraine without aura (MO) referred to our centre over the same period. Controls were matched to cases not only by age at the first visit to our centre (±2 years), but also by age at headache onset (±2 years) to avoid selection bias from differences in disease duration, which could determine differences in behaviour between the two study groups. All diagnoses were made according to the criteria of the International Classification of Headache Disorders, second edition (ICHD-II) (14). Patients with more than one headache subtype were excluded from the study. We did not include female CH patients and chronic CH sufferers in the study because the size of these patient subgroups was too small to draw any significant conclusions. One of our centre’s physicians (GL), blinded to diagnosis, administered a specially designed semistructured questionnaire (filled in by the physician) face-to-face to all patients. The questionnaire asked about the year when THI occurred, how it occurred, who was responsible for the situation in which it occurred and whether there was loss of consciousness. In the event of multiple THIs, this information was repeated for each single injury. For those THIs that did not require a medical visit at a hospital’s emergency department or by a neurologist, we used data from patients’ past medical histories. In all other cases, data were also derived from the medical documentation enclosed with our centre’s patient records (discharge letters, specialists’ reports, X-rays, etc.) or provided by the patients themselves after the interview. The questionnaire also included questions regarding non-essential consumption habits (alcohol and coffee intake, cigarette smoking). In our data analysis, we did not consider THIs separately according to their severity, because this was not relevant to our study purpose. Each patient gave his/her consent to use of personal data for scientific purposes according to Italy’s Decree-Law no. 196 of 30 June 2003.
In the two study groups, we evaluated the following parameters: (a) the number of THI patients with or without loss of consciousness; (b) the number of THIs with or without loss of consciousness; (c) patient’s age at the first THI and the temporal relation between CH onset and THI; (d) patient’s occupation; (e) how THI occurred; and (f) who was responsible for causing the accident that induced THI or for inflicting THI. Based on the most common THI causes described in the literature (15), we recognised five categories for THI etiology: road accidents, household accidents, workplace accidents, sports accidents and other accidents which included all those causes that did not fall within those four categories. For THI from road accidents, we also recorded the type of vehicle (car, motorcycle, bicycle) and whether the patient was driving.
For CH patients who had responsibility in causing their THI, we compared personal habits with those of other CH patients. In particular, we evaluated: (a) alcohol consumption, measured in alcohol units per day (16) (mild drinkers, <4 units/day; moderate drinkers, 4–8 units/day; heavy drinkers, >8 units/day); (b) cigarette smoking, measured in number of cigarettes per day (mild smokers, 1–15 cigarettes/day; moderate smokers, 16–24 cigarettes/day; heavy smokers, >25 cigarettes/day) (17); and (3) coffee consumption, measured as cups of coffee per day (mild drinkers, 1–3 cups/day; moderate drinkers, 3–6 cups/day; heavy drinkers, >6 cups/day). By this comparison among CH patients, we tried to find out whether there was a behavioural pattern suggesting a possible association between responsibility for THI and the tendency to overindulge in non-essential consumption habits.
Data analysis
We performed our statistical analysis using Student’s t-test for mean comparison and the Chi-square test. For each variable, we calculated the crude odds ratio (OR) and, when applicable, we used the Mantel-Haenszel method to estimate the adjusted odds ratio (AOR) for confounding factors (cigarette smoking and alcohol consumption). For each OR, we calculated the corresponding 95% confidence interval (CI); 95% CIs for AORs were estimated by the Miettinen method. We calculated p values using the two-tailed test (α = .05). For data analysis, we used the Statistical Package for the Social Sciences software (version 15) (SPSS, Chicago, IL, USA).
Results
Traumatic head injury characteristics in cluster headache cases and in migraine without aura controls
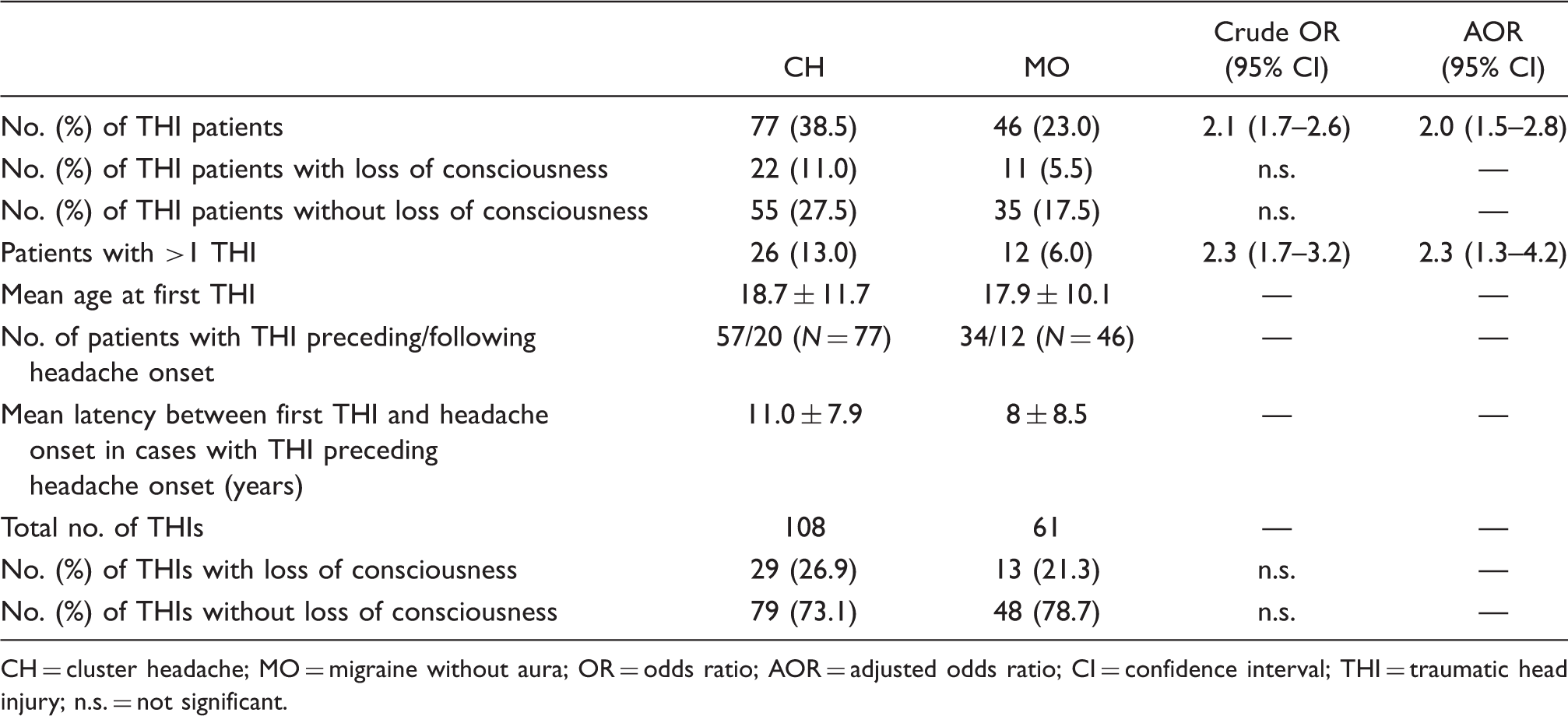
CH = cluster headache; MO = migraine without aura; OR = odds ratio; AOR = adjusted odds ratio; CI = confidence interval; THI = traumatic head injury; n.s. = not significant.
A positive history of THI was reported by a significantly higher number of cases than by controls (38.5% vs. 23.0%; OR = 2.1, 95% CI = 1.7–2.6; AOR = 2, 95% CI = 1.5–2.8; p = .019). The difference between the two groups was observed also for those with multiple THIs (OR = 2.3; 95% CI = 1.7–3.2; AOR: 2.3; 95% CI = 1.3–4.2; p = .04). The number of THIs was also higher in cases than in controls. The mean latency between the first THI and headache onset in cases with THI preceding CH headache onset was 11 years ±7.9 (Table 1).
Traumatic head injury etiology in cluster headache cases and in migraine without aura controls

CH = cluster headache; MO = migraine without aura; OR = odds ratio; CI = confidence interval; THI = traumatic head injury; n.s. = not significant. *The adjusted OR for the “scuffle/brawl” variable was not calculated because the number of subjects was too small.
Responsibility for mode of occurrence of traumatic head injuries in cluster headache cases and migraine without aura controls

CH = cluster headache; MO = migraine without aura; OR = odds ratio; CI = confidence interval; THI = traumatic head injury; n.s. = not significant.
Non-essential consumption habits in cluster headache cases and migraine without aura controls

CH = cluster headache; MO = migraine without aura; OR = odds ratio; CI = confidence interval; THI = traumatic head injury; n.s. = not significant. *“Other CH patients” includes CH subjects not responsible for THI and CH subjects without THI.
Again, more CH patients than controls drank alcohol (149 vs. 113, 74.5% vs. 56.5%, p = .000); in this case, too, they were more frequently moderate (p = .002) or heavy (p = .03) drinkers. No significant differences were observed for coffee consumption between the two groups (Table 4).
When we investigated the association between patients' responsibility for THI and non-essential personal habits, we found that 26.7% of cases responsible for al least one THI (N = 12/45) were heavy alcohol drinkers, 44.4% (N = 20/45) were heavy smokers and 22.2% (N = 10/45) were heavy coffee drinkers. The difference in behaviour from that of the other CH patients in the case group was statistically significant: of the latter, only 5.1% (N = 8/155; OR = 7.2; 95% CI = 2.9–18.2; p = .000) were heavy alcohol drinkers, 26.5% (N = 41/155; OR = 2.2, 95% CI = 1.6–3.1; p = 0.03) were heavy smokers, and 5.8% (N = 9/155; OR = 5; 95%, CI = 3.1–8.1; p = .003) were heavy coffee drinkers (Table 4).
Discussion
The purpose of our study was to describe THI occurrence and causal responsibility in a clinical population of CH compared to MO male patients. To our knowledge, no similar study has ever been published in the literature.
The study was conducted on two homogeneous groups matched by age at headache onset, type of job (data not shown), and number of patients driving a vehicle when a road accident was involved.
We found that CH patients were more likely to incur THI than MO controls. This finding corroborates evidence from an Italian cooperative study (5), which revealed a history of THI in 30.8% of CH patients (N = 120) versus 15.8% of healthy controls (N = 120) (OR = 2.50, 95% CI = 1.28–4.88) and confirmed the results obtained by Manzoni et al. in another Parma University Headache Centre case series in the late 1990s (6). The latency between head trauma and subsequent onset of CH makes a causal relation between the two occurrences rather unlikely, except for rare cases of post-traumatic CH (18).
Our study indicates that CH patients exhibit distinctive THI-related features compared with MO controls, namely: (a) they are more likely to incur a THI; (b) they have a higher rate of multiple THIs; (c) they have a higher rate of THI incurred during scuffles or brawls; (d) they are more frequently responsible for their THI, especially when incurred during scuffles or brawls, and the number of THIs for which they are responsible is also higher; and (e) they are more frequently cigarette smokers and alcohol drinkers. We found that the number of heavy smokers and heavy alcohol and coffee drinkers was significantly higher among CH patients who were responsible for their THI than among the other CH patients.
As CH male patients are more frequently responsible for their THI and they are more likely to engage in risky behaviour prone to THI than MO controls, it is reasonable to assume that the higher THI rate in these patients is a result of their behaviour, which could be correlated to their particular lifestyle. Literature data indicate that CH patients tend to indulge more in certain habits than do healthy subjects or patients with other types of primary headache (10,13,19): in a case series of 246 CH patients, Schürks et al. reported that more than 80% were alcohol drinkers and 65.9% were smokers (20). Our results, too, show that CH patients are more inclined than controls to smoke cigarettes and drink alcohol. We also found that the rate of tobacco-use cessation in current smokers was higher in the migraine group than in the CH group. This finding might corroborate the hypothesis that in CH patients smoking could represent a personality-/lifestyle-related phenomenon and not just a non-essential consumption habit; that would also be the reason why only a tiny proportion of them would quit smoking. In agreement with our hypotheses, Levi et al. suggested that addictive behaviour regarding cigarette smoking in CH patients might reflect certain personality characteristics (21). To determine whether there is an association between responsibility for THI and lifestyle of CH patients, we compared CH patients responsible for their THI with the other CH patients in terms of the tendency to indulge in such habits as cigarette smoking and alcohol and coffee consumption. The results of this comparison indicated that CH patients who caused themselves at least one THI were more frequently heavy smokers and heavy alcohol and coffee drinkers.
Our findings support the hypothesis of a distinctive lifestyle for some CH patients, which is characterized not only by overindulging in some non-essential consumption habits, but also by the tendency to adopt certain kinds of behaviour, which lead to THI. Our hypothesis seems to be confirmed also by Sjöstrand et al. who in a recent study of 23 families with 42 CH sufferers and 41 non-affected first- and/or second-degree relatives found a significantly higher number of THI sufferers, alcohol drinkers and coffee drinkers among CH patients than controls. Other than a personality-/lifestyle-related phenomenon, these findings might represent a gene-environment interaction in affected CH patients or a combination of these mechanisms (22). On the other hand, cigarette smoking is thought by some authors to have a prominent role in CH pathophysiology (23).
However, it cannot be excluded that the high THI rate in CH patients is related to the psychoactive effect of their substance abuse. Literature data indicate that chronic as well as occasional heavy alcohol drinkers are more likely to incur traumatic injuries (24,25) and are more often involved in episodes of interpersonal violence, probably because of a reduction of their cognitive ability to assess risk and to make rational decisions (26). A few studies have demonstrated that cigarette smokers, too, tend to engage in more risky behaviour when they are driving vehicles and therefore are more prone to incur road accidents (27). Having adjusted the crude OR for these confounding factors, we can state that being a CH sufferer is an independent factor for THI.
Our study does have a few methodological limitations: (a) Data were gathered by evaluating THI retrospectively, so our findings merely suggest an association between CH and THI; on the other hand, this approach enabled us to recruit a larger sample of CH patients than would otherwise be possible through a prospective study, given the low prevalence of CH in the general population (1,2). (b) There was a recall bias problem: patients with headache are more inclined to recall a past traumatic head injury as a way to find an explanation for their headache. Probably, due to the extremely severe pain they suffer, CH patients are more likely to remember previous head traumas than do migraine patients who experience a less severe headache. (c) Control subjects were not healthy individuals, but migraineurs; it cannot be excluded, then, that the differences found were due to the fact that migraineurs are described by some authors as perfectionist, strict and inflexible, and therefore have a lifestyle that makes them less prone to incur THI (28,29). Although not supported by statistical analysis, some observations allow us to assume that in terms of lifestyle, migraineurs do not appear to be different from the general population. When we compared the percentage of daily smokers and alcohol drinkers in migraine patients with data from the Italian general population, we didn’t find any remarkable difference (17,30); moreover, no study in the literature has ever demonstrated that migraineurs suffer fewer THIs than the general population or tend to be less violent. The choice of a “clinical” control group was dictated by practical reasons: the patient sample size was so large that it was not possible to establish a control group of healthy individuals. THI concern only moderate-to-severe injuries that had repercussions on the health condition of the injured individuals or led to emergency department admissions (31,32). By contrast, in our case series we considered all THIs, including those that did not require a medical visit.
In conclusion, our study suggests that CH male subjects not only tend to overindulge in some non-essential consumption habits, but also are more prone to cause themselves THI compared with migraine patients. CH patients' being prone to dangerous behaviours could be a consequence of their particular lifestyle, which could partly explain the association between CH and THI.
To corroborate our results, further studies are needed to investigate the frequency and mode of occurrence of non-head traumas in CH patients versus non–headache controls and to define the personality profile of CH patients as a possible predisposing factor to their distinctive lifestyle.