
Abstract
Migraine is one of the most disabling diseases worldwide, especially when it transforms into chronic migraine, which is often associated with medication overuse and can become resistant or even refractory to treatments. Molecular, neuroimaging and neurophysiological changes have been described in chronic migraine, some of which might not be fully reversible with preventive treatment. For these reasons, we should aim to prevent this transition, and initiate preventive treatment before disease becomes refractory and burden increases. Preventive migraine treatments are often delayed because of access to care, stigma leading to undertreatment and patients’ reluctance as a result of fear of side effects and, in some cases, fear of being labeled as chronically ill. With the availability of effective and well-tolerated preventive treatments, we must shift our mindset and take advantage of new opportunities to initiate preventive treatment earlier. In this International Headache Society position statement, we propose a migraine preventive strategy under the idea of shifting from reactive treatment once disability is established (prevention of attacks), to proactive, individualized prevention initiated early with safe, effective and tolerable therapies (prevention of disease progression). This approach is based on 1) promoting the early initiation of effective and tolerable preventive therapies, starting from two to four monthly migraine days in line with the majority of current guidelines and recommendations and 2) fostering longitudinal studies to gather more evidence on the potential benefit of early prevention, with the final goal of improving patient outcomes, promoting excellent migraine care, enhancing individual and social well-being, and, ultimately, preventing migraine progression and preserving brain health.
This is a visual representation of the abstract.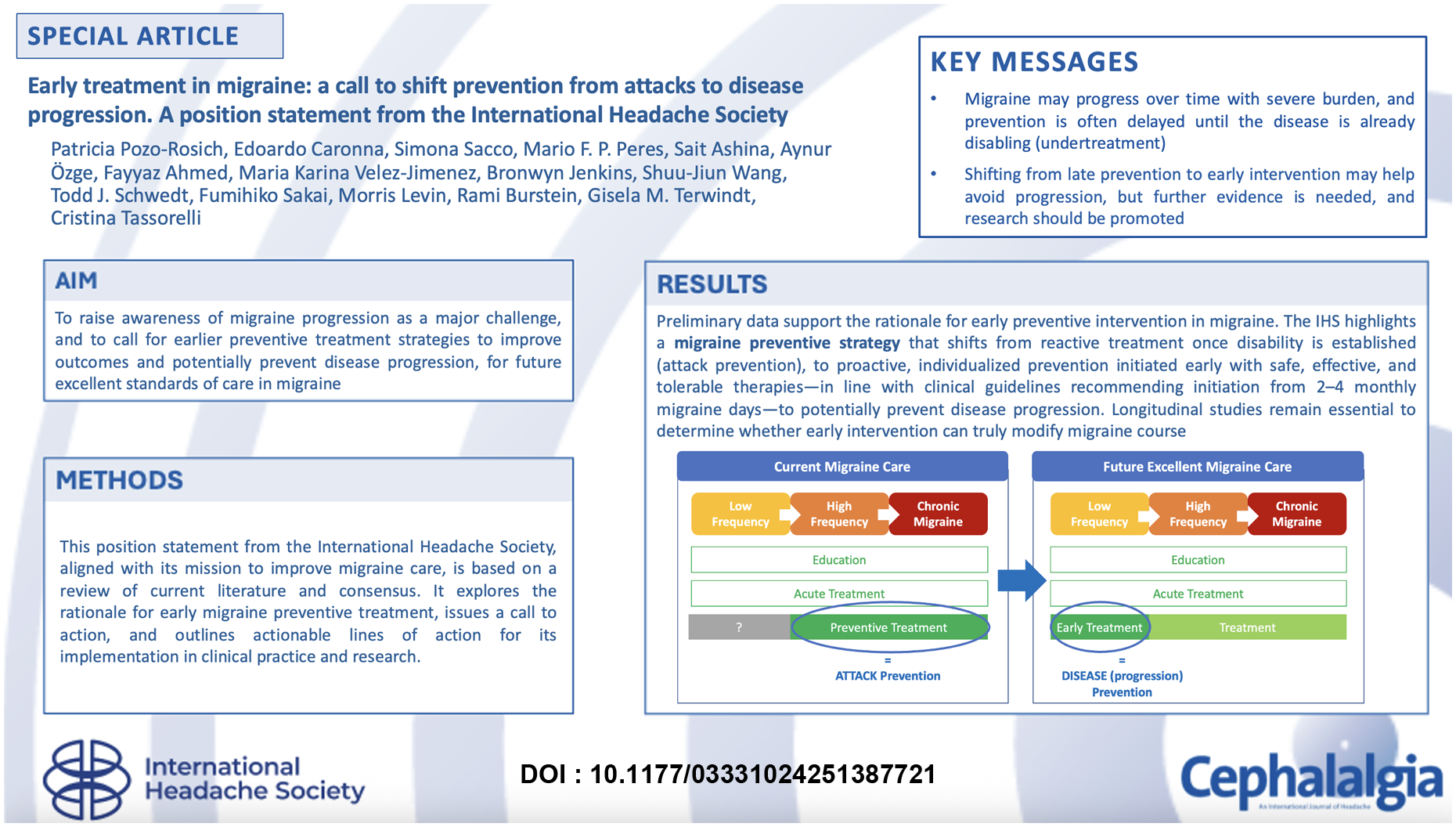
Introduction
Migraine is a complex neurological disease based on the interaction between genetic and environmental factors, affecting around 15% of the population (1). It is considered one of the most disabling diseases worldwide (2), given that, on a migraine day, people cannot function properly. In this context, the most severe form is chronic migraine (CM), which is defined by the current International Classification of Headache Disorders (ICHD-3) as headache occurring on ≥15 days/month for more than three months, which, on at least eight days/month, has the features of migraine (3). The definition of CM is therefore based on the frequency of headache and migraine days, rather than duration of the illness. CM affects 1–2% of the global population (4) and usually represents the progression of a less frequent (episodic) migraine (EM). According to epidemiological studies, the transformation rate from EM to CM is around 3% annually (4). While some individuals with CM may revert to an episodic pattern, a substantial proportion of them evolve and persist in an even more severe clinical condition that includes acute medication overuse, treatment resistance or even total refractoriness to acute and preventive treatments, and the development of psychiatric comorbidities, and also correlates with social and working limitations (5,6). Hence, migraine progression is not simply the transition from a lower frequency to a higher frequency of migraine attacks (chronification), but also involves the accumulation of complexity and severity which complicates the disease and makes it increasingly debilitating (Figure 1) (7,8).

Migraine progression. Migraine progression is often referred to as the transition from episodic to chronic migraine, in other terms, as a synonym of migraine chronification. However, not only an increase of frequency, but also the duration and severity of the attacks can be seen as migraine progression and can lead to certain disease complications such as an increase in acute medication intake (medication overuse) or resistance to acute and preventive treatments (including refractoriness when all available treatments have failed). These complications, on the one hand, can be seen as the indirect expression of a disease that is progressing and is becoming more severe and uncontrolled. On the other hand, they may represent risk factors that are able to further worsen the migraine disorder progression
At present, migraine cannot be cured, but it can be treated. A recommended treatment strategy for people with migraine consists of (behavioral) education coupled with adequate acute and preventive treatments (9,10). However, the precision of the term prevention is, in reality, questionable, when, either because of the severity or the frequency of attacks, the disease has already become resistant or even refractory.
The International Headache Society (IHS) has the mission to improve migraine care worldwide. In line with this mission, recent IHS papers have emphasized the recognition of migraine as one of the most disabling neurological diseases – first among children and adolescents and second in adults (2) – the need for a higher standard of care (11), and the development of practical, implementable treatment recommendations to improve prevention (10). Building on these priorities and, grounded in clinical and translational literature, as well as consensus-based expert opinion, the present position statement highlights migraine progression as a critical challenge and underscores the urgent need for preventive strategies. We advance the hypothesis that, for some people, early initiation of preventive treatment may reduce the risk of migraine progression. Although more work is required to determine whether current preventive drugs are truly disease-modifying – given the strong genetic determinants and other factors influencing chronification (12) – this position statement from the IHS is intended as a call to action to place stronger emphasis on early treatment strategies, this is when the frequency is lower, with the goal of not only improving treatment effectiveness and reducing unnecessary suffering, but also preventing disease progression and, ultimately, achieving excellent standards of care (11).
Rationale for early treatment
The concept of treating people earlier is not new in the neurological field and is based on the scientific progress made in understanding how the brain changes if not treated on time. This knowledge has come from the development and use of biomarkers and the launch of disease-specific therapies, allowing the disclosure of the benefit of a targeted, precise and timely care (Table 1) (13–48). Although the underlying pathophysiological mechanisms differ across neurological disorders, this approach consistently highlights the value of precise, personalized and early intervention, providing a relevant model for migraine.
Examples of neurological disorders and their biomarkers
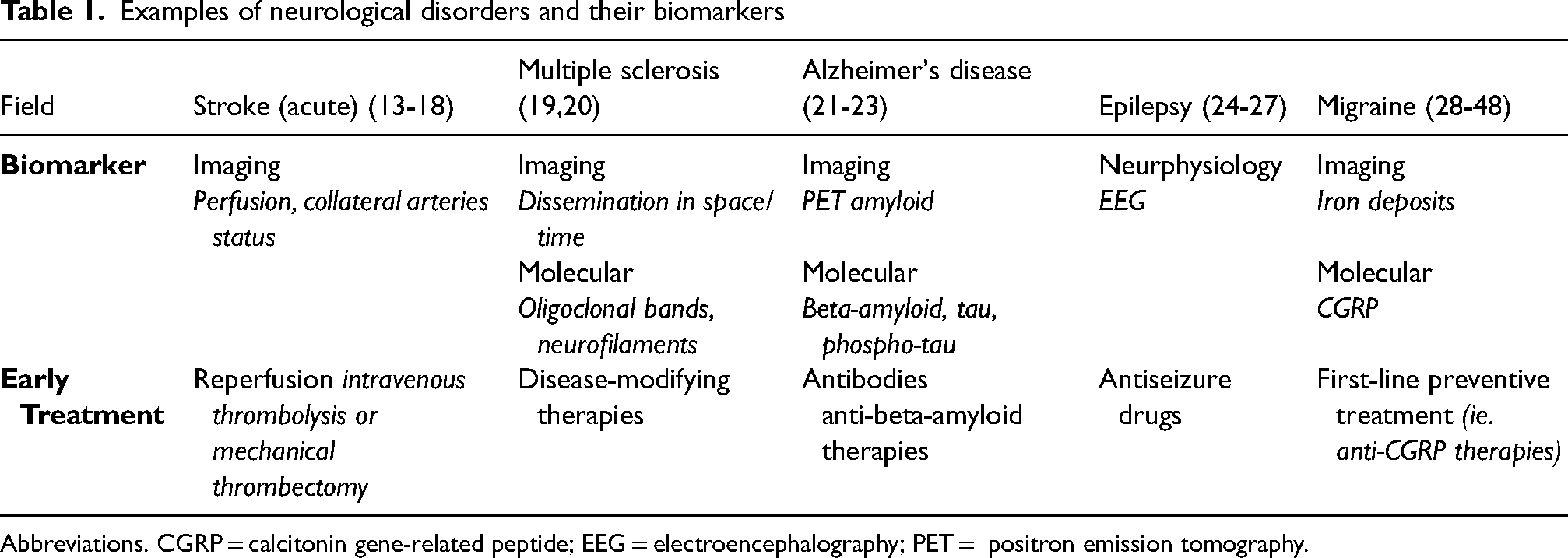
Abbreviations. CGRP = calcitonin gene-related peptide; EEG = electroencephalography; PET = positron emission tomography.
Emerging imaging, neurophysiological and neurochemical techniques have the potential to identify biomarkers for migraine as well, which would be helpful in diagnosing it, understanding prognosis and predicting responsiveness to treatments. Specifically, understanding migraine trajectories, the chronification process, and its risk and complications is fundamental to deliver timely and precise medical care (28), before less reversable changes in pathophysiology occur.
Studies have described brain structural (29–33) and functional (28,34,35) as well as molecular (36–38) changes in chronic migraine. While there is ongoing debate about whether these alterations reflect predisposing brain traits, it is also likely that at least part of these changes are acquired as consequences of the progression of the disease (39). This aligns with the complex nature of migraine, where genetics and the exposome interact. Genetic studies may offer further insight. So far, GWAS (i.e. genome-wide association studies) (12) have not identified any genetic variant specifically linked to chronic migraine, a fact that may suggest a more prominent role of environmental/acquired factors and epigenetic modulation (40) in migraine progression. Similar changes have been described in patients with complications such as medication overuse (8,41,42) or refractory migraine (7,43–45), but it remains uncertain whether these represent predisposition, disease-related adaptations, or both.
Overall, the central issue is whether such changes are reversible. Some studies have demonstrated “normalization” of certain brain functions associated with migraine preventive treatment response (46). However, for example, iron depositions in brain areas are not reversible, and higher deposits, especially in the periaqueductal gray matter and red nucleus, have been suggested to be associated with poorer responses to onabotulinumtoxinA and erenumab (47,48). Yet, further evidence is warrented and there is a need for longitudinal biomarker studies in migraine, specially starting before or as soon as disease manifests (49).
Growing evidence from both clinical trials and real-world experience (RWE) reinforces the rationale for early intervention. Clinical data are coming especially from anti-calcitonin gene-related peptide (CGRP) drugs because data are lacking on conventional non-specific preventives (e.g. amitriptyline, propranolol, topiramate) and non-pharmacological interventions. The APPRAISE prospective, multicenter, open-label international trial showed that those individuals who are not resistant to different previous therapies and who have less headache frequency per month at baseline respond better to erenumab, a monoclonal antibody targeting the CGRP-receptor (50). This line is also supported by the main finding of the recent largest RWE European EUREkA Consortium study, with 5818 people with migraine included, which found that the likelihood of being a 50% responder or more to treatment with anti-CGRP monoclonal antibodies was higher in individuals who had fewer monthly migraine days (51). Further insight comes from onabotulinumtoxinA, where in a study initiating treatment within the first 12 months after CM diagnosis was associated with a better response (52). While attack frequency was already high in these cases, the finding favours the earlier intervention when the shift in frequency is recent. These observations align with the pathophysiological hypothesis that earlier intervention may help prevent, among other mechanisms, central sensitization, which has been associated with reduced responsiveness to anti-CGRP therapy (53).
Taken together, insights from other neurological fields where earlier intervention is increasingly prioritized, evidence of brain changes associated with migraine progression and emerging clinical experience with preventive therapies – particularly migraine-specific drugs – showing better outcomes in those treated earlier, converge to support the rationale for early preventive treatment strategies.
A call for early treatment
Shifting the concept of migraine prevention from attack to disease
In the past, preventive treatments were often delayed until migraine was perceived as substantially disabling, due to the limited efficacy and tolerability of available treatment options. However, there has been ongoing debate about whether preventive treatment should be started as soon as migraine manifests. With the availability of highly effective and well-tolerated treatments like anti-CGRP drugs, it is time to shift the mindset of patients, treating physicians, and health technology assessment (i.e. HTA) bodies and start treatment earlier with the hope of avoiding high-frequent and chronic migraine, both of which are highly disabling, burdensome and associated to high costs (54,55).
The current controversy in migraine is focused on whether migraine preventive treatments are disease-modifying, and if so, if only migraine-specific preventive treatment (e.g. CGRP-targeting therapies) are disease-modifying, or if all migraine preventive medications are. Unless we start treating early within disease evolution, we will not be able to assess whether treatments could avoid and prevent chronic migraine and modify migraine course , shifting from just giving a treatment (prevention of attacks) to the thought of prevention of the evolution towards a chronic refractory-to-treatment disease (prevention of disease progression) (Figures 2 and 3). This may also mean treating not only the burden, but also the disease itself.

Shifting from attack prevention to disease prevention (early treatment). The current migraine care model is based on educating individuals, offering adequate acute treatments and then migraine prevention only when the disease is already highly disabling and, in some cases, potentially irreversible such as in chronic migraine. The future proposal is to engage prevention earlier. In this model, ongoing education and proper acute treatments to all individuals would continue but with the added imperative of offering effective and tolerable preventive treatments at earlier disease stages in the hope that this will control or prevent progression

Time-to-treatment in migraine care: the journey of people with migraine. Time-to-effective and tolerable (E-T) migraine preventive treatment refers to the duration from disease onset to the initiation of a E-T migraine preventive treatment. (A) In current migraine care, time-to- E-T preventive treatment is often prolonged due to barriers that limit access to care. The time to initiating migraine-specific preventive medications is even longer. (B) Shift in the approach to migraine prevention. Earlier treatment (when migraine frequency is low) with E-T preventive medications is encouraged. Under this approach, time-to-E-T preventive migraine treatment is reduced (this is, migraine preventive treatment is started earlier in the disease course). Emerging data suggest that this strategy could lead to better outcomes. (C) For migraine care excellence, it will be important to understand disease trajectories and investigate whether E-T preventive treatment initiated not only when frequency is still low, but also earlier in life when it is able to impact migraine course. This proactive approach may positively influence and modify disease progression, although evidence is needed. The International Headache Society wants to ensure in the future that we can offer the right treatment to the right patient at the right time. The right treatment may include pharmacological and non-pharmacological therapies as well as multidisciplinary approaches (physiotherapy, psychological support, lifestyle modifications etc.). Note: While earlier treatment with E-T therapies can potentially involve any available preventive therapy with demonstrated effectiveness and acceptable side effects for patients, the better tolerability and efficacy profile of current migraine-specific medications now makes it more feasible to shift the treatment paradigm toward earlier intervention
Despite new target-driven therapies for migraine, there is still a long-way to go to ensuring access for all who need them. This paradigm shift should extend beyond regions with access to new treatments. Early preventive strategies, irrespective of the use of anti-CGRP therapies, should be embraced, primarily to reduce suffering in the many millions of patients affected, in addition to reducing excessive use of acute medications, as well as in the justifiable hope that disease progression may be controlled or prevented (56).
The major barrier to this new approach is that migraine is still widely underdiagnosed and undertreated. In other terms, even individuals with an already disabling disease are not receiving (appropriate) acute and/or preventive treatments (57). Following migraine onset, people with migraine often have a long journey before they obtain access to adequate treatments. In this scenario, pursuing an early treatment when not even basic care is provided can be challenging (Figure 3). Resistance to care can come not only from healthcare providers. but also from patients. For some individuals, it can be difficult to acknowledge the need for treatment at an earlier stage of the disease before it gets uncontrolled, and many are reluctant to recognize migraine as an illness, but instead continue to seek care and hope not to have any more migraine attacks in the future (58). This will require a change in the awareness of society, coupled with clinical and research efforts to provide scientific longitudinal data showing that early treatment can indeed change the course of migraine evolution. In the future, pragmatic clinical trials may be applied for this pro-active approach of migraine prevention, as well as validating migraine disease biomarkers (59). The economic sustainability of early treatment with migraine preventive drugs might be a major limitation to adopting this approach, highlighting the need for pharmaco-economic studies. However, given the high (in)direct costs associated with migraine for society (60), especially in those who are undertreated (61), preliminary data suggest that migraine-specific treatments may offer a favorable cost-benefit ratio (62).
Actions for early treatment
In line with our call of action, we propose two implementable lines of action for the headache community.
Line of action #1: clinical practice
Starting effective and tolerable preventive treatments from two to four monthly migraine days
In line with Global Practice Recommendations on Preventive Pharmacological Treatment based on several national society recommendations (10) and the Consensus Statement endorsed by the European Headache Federation and the European Academy of Neurology (9), the IHS defines early treatment as the initiation of preventive therapy when migraine frequency is still relatively low—starting from two to four monthly migraine days. Because, in clinical practice, usually preventive treatment is initiated with higher frequency (63), with this position paper, the IHS emphasizes the importance of implementing preventive therapy earlier in the disease course. Effective and tolerable therapies can potentially involve any available preventive treatment with demonstrated effectiveness and acceptable side effects for patients (64).
Line of action #2: research
Conducting longitudinal studies
Despite progress, major knowledge gaps remain. While some individuals may live for years with low-frequency migraine without experiencing progression, others are at greater risk – yet we currently lack the tools to identify who is most vulnerable and when this risk increases across the lifespan.
Longitudinal studies are urgently needed 1) to clarify whether early initiation of preventive therapy can meaningfully alter long-term disease progression and 2) to determine whether a lower threshold for starting therapy should be established. Future research must also include benefit–risk analyses, assessing the number needed to treat (i.e. NNT) against the number needed to harm (i.e. NNH), aiming to guide more evidence-based decisions.
Conclusions
The international headache community must move beyond simply mitigating attacks and instead aim to change the course of migraine itself. This requires a shift in perspective – from reactive treatment once disability is established, to proactive, individualized prevention initiated early with safe, effective and tolerable therapies. A new mindset is needed across patients, clinicians and health systems alike: prevention should no longer wait until migraine becomes severely disabling. Early and effective intervention must be embraced as both realistic and essential. Coupled with continued research and equitable access to care, this migraine preventive strategy can improve quality of life, enhance standards of care and, ultimately, alter the natural history of migraine and preserve brain health.
Footnotes
Data availability
The data used for this article may be obtained from the authors upon reasonable request.
Declaration of conflicting interests
PPR has received, in the last three years, honoraria as a consultant and speaker from AbbVie, Amgen, Dr Reddy's, Eli Lilly, Lundbeck, Medscape, Novartis, Organon, Pfizer and Teva Pharmaceuticals. Her research group has received research grants from AbbVie, AGAUR, EraNet Neuron, FEDER RIS3CAT, Instituto Investigación Carlos III, MICINN, Novartis and Teva Pharmaceuticals, and has received funding for clinical trials from AbbVie, Amgen, Biohaven, Eli Lilly, Lundbeck, Novartis, Pfizer and Teva Pharmaceuticals. She is the Honorary Secretary of the International Headache Society. Currently, she serves as an associate editor for Cephalalgia and Neurologia. She is a member of the Clinical Trials Guidelines Committee of the International Headache Society. She has edited the Guidelines for the Diagnosis and Treatment of Headache of the Spanish Neurological Society. She is the founder of ![]() .
.
EC has received honoraria from Novartis, Chiesi, Lundbeck, MedScape, Lilly, TEVA, Organon and Dr Reddy's; his salary has been partially funded by Río Hortega grant Acción Estratégica en Salud 2017–2020 from Instituto de Salud Carlos III (CM20/00217) and Juan Rodés fellowship, Subprograma Estatal de Incorporación de la Acción Estratégica en Salud 2023 (JR23/00065). He is a junior editor for Cephalalgia.
SS reports consultant, speaker, or advisory board fees from Abbott, Allergan/Abbvie, AstraZeneca, Bayer, Bristol Myers Squibb, Daiichi-Sankyo, Eli Lilly, Medscape, Medtronic, Novartis, Pfizer, Starmed, Teva and Uriach
MP accepted honoraria for lectures, presentations, speakers bureaus, manuscript writing and educational events from Pfizer, Teva, AbbVie-Allergan and Lundbeck. He has accepted travel support from Teva. Participated in advisory boards, AbbVie-Allergan, Eli Lilly, Pfizer, Kenvue, Eurofarma and Sanofi-Aventis. Mario Peres is president of ABRACES.
SA has served as a consultant or on advisory board for Abbvie, Eli Lilly, Linpharma, Lundbeck, Satsuma, Teva, Theranica, Percept, Pfizer and Impel NeuroPharma.
AO has received honoraria from Pfizer, Lilly, AbbVie, Organon, Abdi İbrahim, TEVA and İlko Pharmacy. AO is one of the board members of IHS, the current president of the Global Migraine and Pain Society together with MENAHeadache Society.
FA: Treasurer of the international headache society, received honorarium for being on the ad board of Abbvie, TEVA, Lundbeck, Pfizer and Dr Reddy.
MKVJ: Society Leadership/Board position: AMCEMIG (Mexican Migraine and Headache Association); ASOLAC (Latinamerican Headache Society). Professional membership: American Headache Society, American Academy of Neurology, AMCEMIG, Mexican Academy of Neurology, Psychiatry Society of Mexico. Relationship with scientific journals: Neurology. Personal fees: Allergan-Abbvie, Pfizer, Abott and Weser pharma. Data safety monitoring/Advisory board: Advisory board-Allergan-Abbvie, Pfizer and Weser pharma. Commercial interests: None
BJ has received honoraria from advisory boards for Novartis, Teva, Lilly, AbbVie and Pfizer, as well as honoraria for invited lectures from Care Pharmacy, Healthed, and General Practice Conference and Exhibition. She is a HMO at Royal North Shore Hospital and an Associate Editor for Cephalalgia. Bronwyn is on development and leadership, ethics and education subcommittees of the International Headache Society (IHS) and is the immediate-past president of the Australia and New Zealand Headache Society.
SJW has received honoraria as a moderator from AbbVie, Biogen, Eli-Lilly, Hava Biopharma and Pfizer, has received consulting fees from AbbVie, Eli-Lilly Taiwan, Percept Co. and Pfizer Taiwan, and has been the PI in trials sponsored by Eli-Lilly, Lundbeck and Novartis. He has received research grants from Taiwan branches of Eli Lilly, Novartis, and Orient Europharma.
TJS, within the prior two years, has received compensation for consulting from AbbVie, Amgen, Linpharma, Lundbeck, Salvia and Scilex, and royalties from UpToDate. He has stock options in Allevalux and Nocira. His institution has received research grants on his behalf from American Heart Association, Flinn Foundation, Henry Jackson Foundation, National Headache Foundation, National Institutes of Health, Patient Centered Outcomes Research Institute, Pfizer, Spark Neuro and United States Department of Defense.
FS has received honoraria as a consultant and speaker from AbbVie, Eli Lilly, Otsuka, Amgen and Daiichi-Sankyo Pharmaceuticals.
ML has received honoraria for consulting for AbbVie, Amneal, Axsome, Eli Lilly, Linpharma and Vectura. He has received royalty payments for published books from Oxford University Press and Anadem. He holds no stocks or options in medical companies, and is on no speaker boards.
RB: Research support from the NIH, AbbVie, Modulight, Eli Lilly and Teva. Reviewer for NINDS, and holds stock options in AllayLamp and Percept. Serves as consultant, advisory board member or has received honoraria from Allergan, Amgen, Biohaven, Brise Mutual, CGRP diagnostic, Dr Reddy's Laboratory, ElectroCore, Eli Lilly, Escient, Johnson & Johnson, Merck, NeuroRays, Pernix, Theranica, Teva and Ventus. CME fees from Healthlogix, Medlogix and WebMD/Medscape, and Patents 9061025, 11732265.1, 10806890, US2021-0015908, WO21007165, US2021-0128724, WO21005497 and 18/036,455. Patents: 9061025: methods for selecting headache patients responsive to botulinum toxin therapy; 11732265.1: Method and compositions for the treatment of migraine headaches, endothelial dysfunction and muscle tenderness with statin and vitamin D; US 10,766,952 B2: Methods for selecting a headache patient responsive to treatment with an anti-CGRP antibody and for reducing headache frequency in the selected patients comprising administering an anti-CGRP antibody; 10806890: Method and apparatus for managing photophobia and migraine photophobia; US2021-0015908: Methods for treating and for inhibiting progression of seizures; WO21007165: Methods for treating and for inhibiting progression of seizures; US2021-0128724: CGRP antagonists and clostridial derivatives for the treatment of cortisol spreading depression associated disorders; WO21005497: CGRP antagonists and clostridial derivatives for the treatment of cortical spreading depression associated disorders; US Patent Application No. 18/036,455 : Systems and methods for improving sleep and other indications, including treating anxiety.
GMT has received research grants and/or consultation fees from Abbvie, Lilly, Lundbeck, Novartis, Organon, Pfizer and Teva, and independent support from the Dutch Research Council, European Community, Dutch Heart Foundation, and Dutch Brain Foundation, Dioraphte, and the Clayco foundation.
CT received personal fees for participating in advisory or for speaking at scientific events from AbbVie, Allergan, Biohaven, Dompé, Eli Lilly, Lundbeck, Novartis and Teva. CT has received research funding from the European Commission, the Italian Ministry of Health and Migraine Research Foundation.