
Abstract
Introduction
Typical migraine aura is characterized by transient focal neurologic symptoms, visual, sensory, dysphasic or other higher cortical dysfunctions. Their manifestations are multi-faceted, with inter and intra-variability.
Objective
To provide a narrative review describing contributions that assist in achieving a precise phenotypic classification of migraine aura.
Methods
We conducted a comprehensive review of the literature to identify and analyze the full spectrum of migraine aura variables. Based on the findings, we proposed a prospective diary model for systematically recording these elements in clinical or research settings.
Results
Visual symptoms are the most multifaceted with many peculiarities such as quality (26 elementary visual symptoms have been described), colour, intermittence, localization and laterality in visual field and direction of spreading. Sensory and dysphasic symptoms have lower level of complexity. The combinations of symptoms, such as their time relationships or duration, are also extremely variable. Furthermore, headache can have five different patterns of presentation with respect to aura onset/end. Higher cortical dysfunctions need to be further investigated in wider populations. After collecting the full spectrum of migraine aura features, we created a diary which we propose can prospectively record those variables.
Conclusion
The findings of this review show that migraine auras present a wide and multi-faceted spectrum of symptoms, generating hundreds of possible scenarios. Therefore, a detailed aura diary to complete during attacks will be of utmost importance to move toward a precise phenotypic classification.
Introduction
Migraine aura (MA) is a common disorder that affects 8% of the general population (1). MA consists of fully reversible visual, sensory, or language symptoms. More rarely non-dysphasic higher cortical dysfunctions, motor or brainstem symptoms can occur. MA symptoms can present in any combinations (visual alone, visual and sensory, visual and dysphasic, sensory and dysphasic, or visual, sensory and dysphasic). Also, their quality, time relationships, sequences and duration might be extremely variable (2,3). MA usually precedes the appearance of a full migraine. Sometimes a typical aura can be followed by a headache with a paucity of migrainous features or at times not even followed by headache. Moreover, visual symptoms, the most common of the auras (occurring in 99% of cases), are not easy to describe verbally neither by the physicians nor by patients (4). All these variables and their range of clinical expressions generate hundreds of possible scenarios in the presentation of MA.
MA is most likely driven by cortical spreading depression, a transient wave of neuronal depolarization in the cortex (5–7). However, the significant variability in its phenotype remains without a clear pathophysiological explanation. A precise characterization of clinical manifestations, combined with investigative tools such as neuroimaging, is essential for gaining deeper insight into the underlying mechanisms.
More importantly, MA presents significant clinical challenges that necessitate a more detailed characterization of its individual features. MA has been linked to an increased risk of ischemic stroke (8), atrial fibrillation (9), and patent foramen ovale (10). Moreover, distinguishing MA from other conditions, particularly transient ischemic attacks (11) and occipital epilepsy (12,13), often proves clinically challenging. Enhancing the clinical characterization of MA may improve diagnostic accuracy and facilitate the identification of patient subgroups at higher risk of comorbidities.
Aim
To provide a narrative review describing contributions that assist in achieving a precise phenotypic classification of MA. Afterward, to propose a data collection sheet to accurately describe the phenotype of a MA.
Methods
Search strategy
PubMed was searched for English language articles up until December 2024. The search string was (“migraine with aura” [Title/Abstract]) OR (“migraine aura” [Title/Abstract]). The bibliographies of all included studies were also searched as well as literature that was known to be relevant by the authors. Moreover, we considered the bibliography of the International Classification of Headache Disorders, Third Edition (14).
Inclusion criteria were all clinical studies in which the features of MA were described.
From each study we collected all the variables of MA and explored their spectra of presentations.
Results
Aura symptoms and their distribution
What we normally call “aura” can occur within the context of a migrainous headache, other headache types, and also occur independently, without any headache. Typical MA can be characterized by any combination of visual, somatosensory, or speech/language symptoms. Non typical MA such as brainstem aura or hemiplegic migraine, which are classified separately (14), can include also other symptoms such as diplopia and motor weakness respectively. In typical MA, the type discussed in this paper, visual symptoms (VS) occur in 99% of the cases, in 31–54% of cases they can be associated with sensory symptoms (SS) and in the 18–32% with dysphasic symptoms (DS) (2,15). In most attacks (62% of cases (2)) there are only VS, in the remaining cases VS presents alongside SS and/or DS. It is only in about 1% of cases that VS are not present and there are just SS (1%) or SS and DS (<1%) (2).
Visual symptoms
Quality features
One prospective diary-aided study on 72 patients who recorded three consecutive MAs, found 67 different visual scenarios out of 216 MAs (16). Such visual phenotypes were composed of one or more of 20 elementary visual symptoms (EVS - single/basic visual symptoms that cannot be further subdivided into other ones) in different combinations. A few years later a systematic review of literature of previous prospective and retrospective systematic recordings of visual aura symptoms identified 25 EVSs (17) (Table 1). As previously mentioned, different EVSs can occur during the same MA. In fact, most MA attacks (63%) prospectively recorded with a diary included more than one visual symptom (median 2, IQR 1–3, range 1–4) (2). A more recent study on 215 MA patients, found that the median number of EVS experienced by patients in the whole lifespan was seven (IQR 4–11) (16). A series of images of each EVS depicted on the same background image with the same style (Standardized Migraine Aura Iconography – SMAI 1.0) was created and tested on MA patients in a multicenter international study (16). Almost 80% of 1645 EVSs experienced by patients in their lives were recognized via images of SMAI 1.0, and almost all patients (98.1%) recognized at least one EVS image of SMAI 1.0 as part of their aura. Only one patient reported a new EVS that the authors defined as “curtain phenomena”. Based on the results of the study and patients’ feedback, the authors amended SMAI 1.0, to SMAI 2.0. The 26 images of EVS together with an image of normal vision, of SMAI 2.0 are represented in Figure 1. This figure, which has been named “visual aura table” can be consulted and downloaded from the IHS website (18).

Visual Aura Table. Image n. 0 = normal vision.
List of all elementary visual symptoms (EVS) of migraine aura and their description.
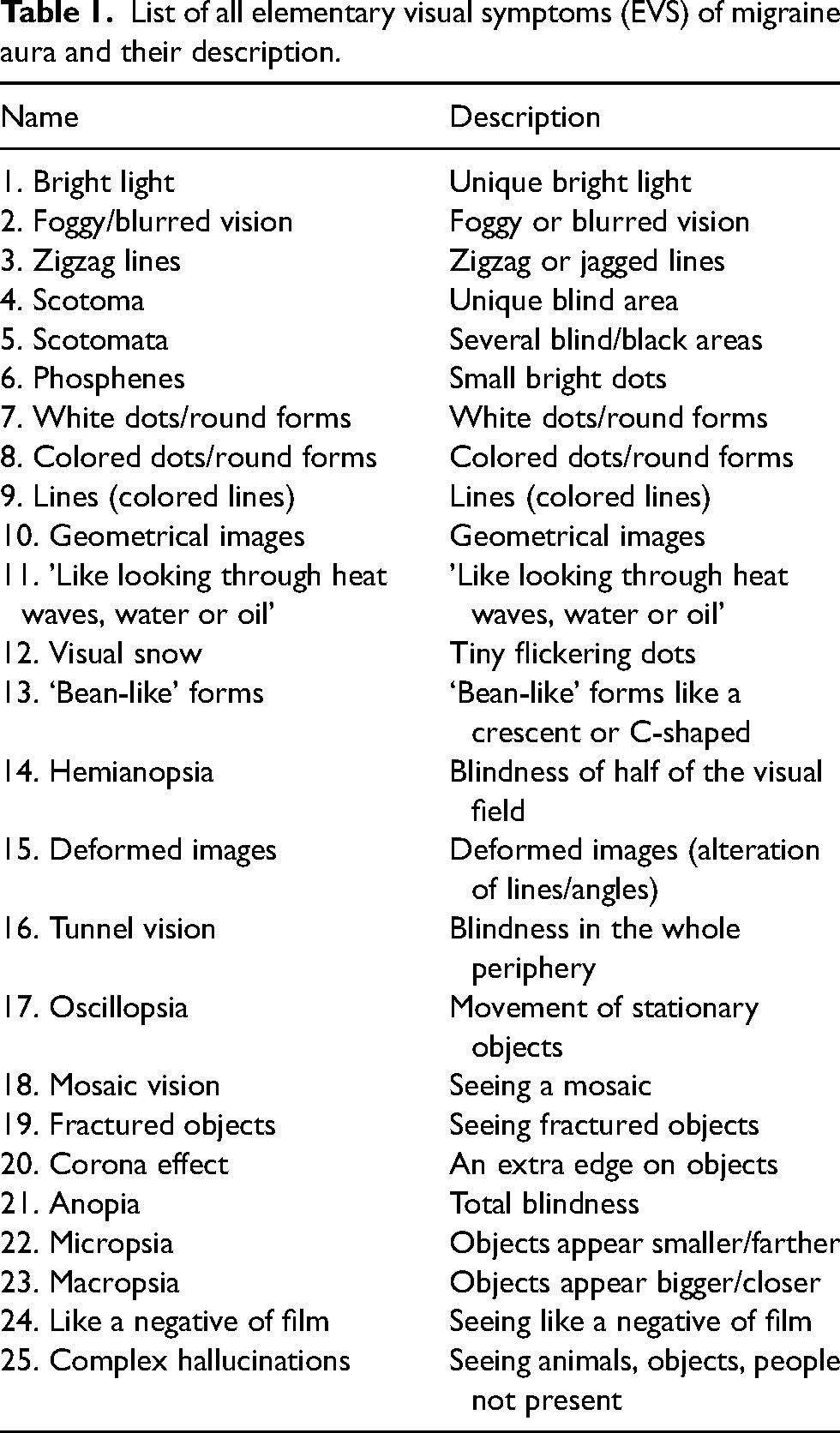
Some EVS, mainly the positive ones (such as zig-zag lines and colored dots) may have also relevant additional features such as colors and intermittent/flickering quality. The frequency of 14 colors and the intermittent/flickering quality have been analyzed in the study by Viana et al. (16).
Among the EVS reported, where the feature’s color was available, 42% to 66% (geometrical images and colored dots respectively) included at least one color among the following: red, orange, yellow, green, blue, purple, pink, brown (16). In another study on 122 patients, it was reported that 40% of total visual auras included one or more color (19). These results go against the finding from Panayiotopoulos (20) who reported that “Elementary visual hallucinations were described by patients with migraine as predominantly black and white […] whereas in epilepsy they were predominantly multicolor”. It must be noted that this latter study had a small sample size (number of patients with typical MA = 47, number of patients with epilepsy = 20).
Among the EVSs where the feature of intermittence was available, this had a frequency ranging from 54% to 92% of cases (respectively bright light and bean-like form) (16).
Distribution of visual symptoms in the visual field
The area of onset of MA in the visual field (VF) was assessed in five clinical studies, three retrospective and two prospective with different findings (Table 2) (2,19,21–23). Typically, VS have a gradual development (or build-up) with changing of shape/dimension and spreading toward other areas of the VF (21). The direction of spreading can be variable as well. In a study where a single patient recorded the characteristic of 1000 MA attacks over two decades, VS gradually moved in every possible direction within the VF (although with different frequency) (24).
Clinical studies in which data on visual aura with respect area of onset in the visual fields and/or its laterality were reported.
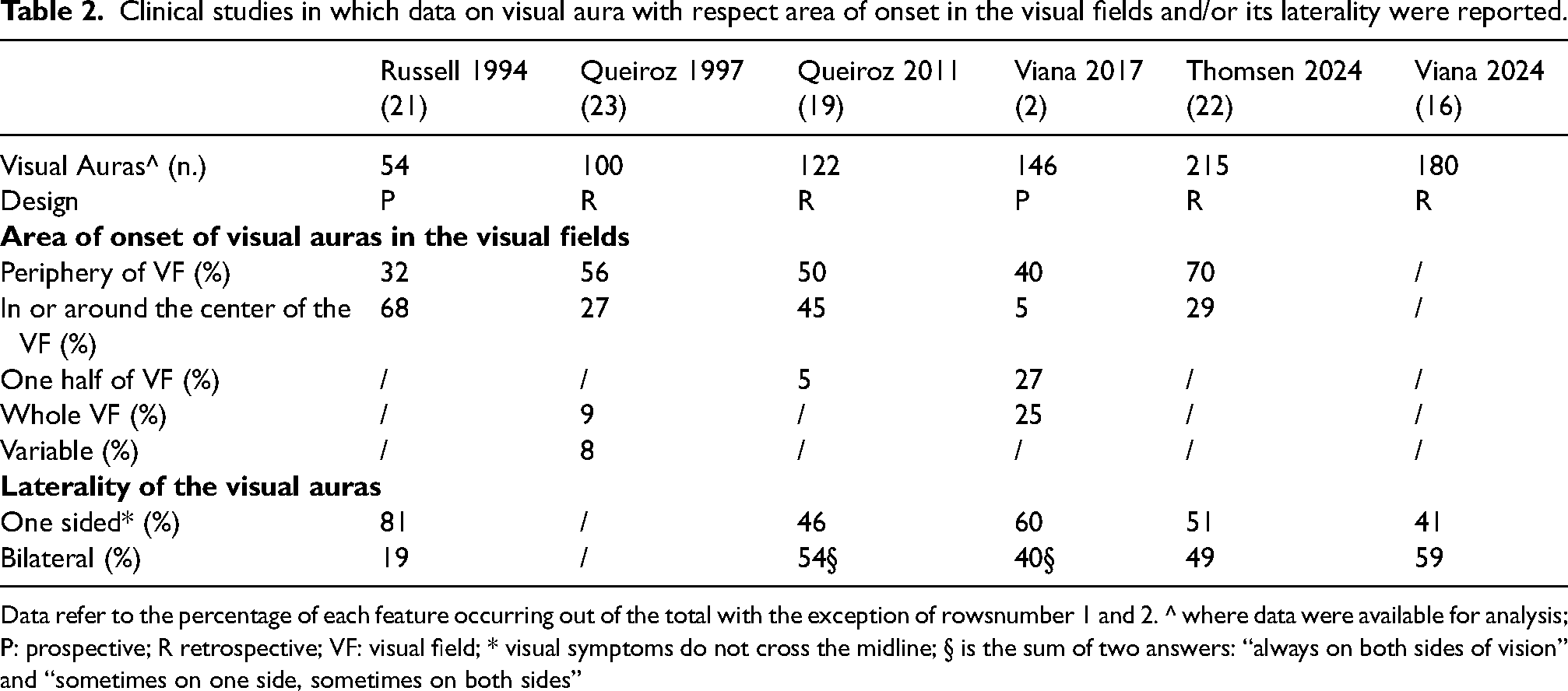
Data refer to the percentage of each feature occurring out of the total with the exception of rowsnumber 1 and 2. ^ where data were available for analysis; P: prospective; R retrospective; VF: visual field; * visual symptoms do not cross the midline; § is the sum of two answers: “always on both sides of vision” and “sometimes on one side, sometimes on both sides”
Laterality of visual symptoms
MA can sometimes be bilateral, meaning that it crosses the midline of the VF. This aspect was reported in six clinical studies, with a prevalence of bilaterality between 19 to 59% of cases (Table 2).
Sensory symptoms
Typically, SS consist of positive symptoms (paresthesia) in 65% of cases. Anesthesia/hypoesthesia may occur in 10% of cases, whereas in 21% of cases paresthesia and anesthesia/hypoesthesia occur simultaneously. In 4% of cases thermic paresthesia may occur (2). SS classically involve one side of the body (85% of cases) (1,2,25). The hand (89–96% of cases) and face (59 to 67%) are the body parts most often affected, whereas the leg (24–25%) and trunk (14–18%) are less commonly involved (1,2). The typical hand–mouth distribution is also called cheiro-oral. Frequently the disturbances have a typical march, moving slowly, starting in the thumb and gradually spreading to the whole hand and the perioral region.
Language symptoms
Paraphasic errors, substitution of one word or sound for the intended word or sound, and other types of impaired language production are the most common speech disturbances during an MA occurring in 76% and 72% of cases, respectively (15). This data has been confirmed by a more recent study (74% of cases) (22). Comprehension errors occur less frequently (38%) (15) (1).
Attention should be paid to the differential diagnosis of the premonitory symptom “difficulty in speech” occurring in 9% of patients (26). This may be the result of differences in frequency of dysphasia among different studies.
Higher cortical dysfunctions
As well as dysphasia, other higher cortical dysfunctions (HCDs) can occur during MA (27). Such symptoms can be divided into three groups: visual HCD (including symptoms such as prosopagnosia, visual agnosia) somatosensory HCD (manual dyspraxia, neglecting hand symptoms, astereognosis); memory HCD (retrograde amnesia, anterograde amnesia, deja vu phenomenon). Unfortunately, it is not possible to estimate the frequency of occurrence of such symptoms, as the studies which investigated them (specifically or among other clinical features) have several methodological limitations (such small sample size, selection bias, retrospective design) (2, 15, 25, 28, 29) . The experience of experts is that such symptoms have a frequency lower than DS.
Temporal features
Duration of aura
According to ICHD-3 the duration of individual aura symptoms (AS) should last between 5 and 60 min (14). A clinical prospective study with a diary to complete during MA attack (reporting time of onset and end of each AS) indicated the duration of 296 AS as follows: median 30 min, IQR 20–45 min. Results also showed that AS lasted for more than 1 h in 15% of cases and for more than 4 h in 5% of cases (2).
In the same study the median duration of the whole aura with two ASs was 45 (IQR 30–103 min) and auras with three ASs was 120 min (IQR 78–160 min) (unpublished results) (2).
ICHD-3 claim also that “when three symptoms occur during an aura, the acceptable maximal duration is 3 × 60 min” (14). In the latter study out of a total of 65 auras with two ASs, 13 auras (20%) lasted for more than 120 min, and a total of 14 auras with three ASs (21%) lasted for more than 180 min (3).
Succession of aura symptoms: Time relationship
ICHD-III states “aura symptoms of different types usually follow one another in succession”(14). Findings from prospective diary-aided study on aura symptoms shows that there could be four scenarios of time relationship between aura symptom B in relationship to aura symptom A as follows: Scenario 1: B starts simultaneously with A; Scenario 2: B starts during A; Scenario 3: B starts when A stopped; Scenario 4: B starts after a free interval of time after the end of A (Figure 2) (3). The frequency of occurrence of each scenario, respectively between 2nd and 1st symptoms and 3rd and 2nd symptom are as follows: Scenario 1: 33% and 14%; Scenario 2: 39% and 43%; Scenario 3: 9% and 7%, Scenario 4: 19% and 36% (3).

Different scenarios of time relationship between aura symptom B in relationship to aura symptom A. Scenario 1: B starts simultaneously with A; scenario 2: B starts during A; scenario 3: B starts when A stopped; scenario 4: B starts after a free interval of time after the end of A. Images taken from: Standardized Migraine Aura Iconography 2.0 (16) and www.pexels.com (free from copyright).
Succession of aura symptoms: Sequence
Auras with multiple symptoms usually have the following sequence: visual, sensory and dysphasic. This happens in 81% of auras with two symptoms (VS – SS) and in 55% of auras with three symptoms (VS – SS – DS). Yet symptoms may occur in different sequences. In auras with two symptoms: VS-DS (13%), SS – VS (2%), DS – SS (2%). In auras with three symptoms: SS-VS-DS (18%), VS-DS-SS (27%) (2).
Headache
Ninety-one percent of 216 auras of the study by Viana et al. (2) was associated with headache. Of the 157 where data related to the onset time of headache were available: in 15 (12%) headache started before aura; in 19 (10%) headache started simultaneously with aura; in 45 (28%) headache started during aura; in 19 (12%) headache started when aura stopped; and in 59 (37%) headache started after a free interval of time after the end of aura (Figure 3). In this last case, the gap between the end of the visual auras and the beginning of the headache has a median of 12 min (IQR 5–30 min). Only in three cases out of 59 (5%) the gap lasted more than 60 min (2). In a multicenter cross-sectional study (25), out of 197 patients with migraine with aura whose data were available, 95 (48.2%) reported greater pain intensity during headache attacks following aura compared to those without aura. In contrast, 14 patients (7.1%) experienced less intense pain, while 88 (44.7%) noted no significant difference in pain intensity. During headache episodes following aura, a variety of accompanying symptoms were reported, with the most common being photophobia/phonophobia (55.1%), nausea/vomiting (55.9%), and vertigo (12.5%) (25).

Different scenarios of time relationship between headache in relationship to the aura. Scenario 1: headache started before aura; Scenario 2: headache started simultaneously with aura; Scenario 3: headache started during aura; Scenario 4: headache started when aura stopped; Scenario 5: headache started after a free interval of time after the end of aura. Images taken from: Standardized Migraine Aura Iconography 2.0 (16) and www.pexels.com (free of copyright).
Attack frequency
In two studies, the attack frequency of MA within the last year was as follows: no attacks in 31–34% of patients; one to six attacks in 48–53%; seven to 12 attacks in 8%; 13–24 attacks in 5–7%; 25–36 attacks in 0–2%, > 36 attacks in 0–4% (26,27).
Intravariability of aura attacks
In 1986 it had been already reported that, while in some patients MA phenotype is stereotyped, other patients never experience identical attacks (30). This aspect has been evaluated in a prospective study over three consecutives MA attacks. Considering just three variables together (i. the visual features, ii. the combination of aura symptoms, iii. the succession of subsequent symptoms), 40 out of 71 patients (56%) did not report a stereotyped aura on the three attacks (2).
In a more recent retrospective study on 215 patients, 38% reported different phenotypes with respect to VSs (over a lifetime span) (16).
A proposal for an aura diary
Although hundreds of studies investigated the preclinical aspect of MA, very few focused on clinical aspects (2,3,22), and many of those have methodologic limitations such as recall bias. This issue must be overcome not just with a prospective design but also with a specific diary to complete during MA attack. In Figure 4 all the variables that should be described during an attack are included. This would empower a deep and reliable phenotyping of MA attacks, fundamental for research purposes. The methodological limitation of this diary could mainly be the inability to control the accuracy of the recording of some data (i.e., time) or the possibility of the patient inserting or modifying some parameters later. However, by properly educating the patient, these problems, which are present with any paper diary, can be minimized. Another issue is that we will have more detailed data on VSs, giving the patient the possibility to record their shape and position in VS every 2–3 min. Yet, we should add at least one or two sheets just for this aspect. In order to overcome such limitations, a further step could be the collection of all these data during the attacks with a mobile application.

Proposed diary to fulfill during aura. ^ patients should close one eye and check whether there is the disturbance in the other one and later do the opposite * Visual symptoms: Visual disturbance overcome median line of visual field? Sensory Symptoms: the disturbance involves both limbs (or part of them) and/or crosses the midline of face (passing through nose), or both side of trunk? EVS: Elementary Visual Symptoms: the numbers are explained in the Visual Aura Table (Figure 1).
Implications for public health
Migraine with aura has critical public health implications. A broader dissemination of the aura iconography by public campaigns exposing the images to the general population, is essential to reduce underdiagnosis, ensuring that individuals receive timely and tailored care. In addition, expanding data collection to diverse clinical settings would also broaden the spectrum of known aura phenomenology, capturing variations that may be missed in traditional neurological contexts. This comprehensive approach could inform future research, refine diagnostic criteria, and shape public health strategies, ultimately improving quality of life and reducing the burden of undiagnosed and poorly managed migraine with aura.
Accurate identification particularly among psychiatrists, cardiologists, and gynecologists, given its intersection with conditions managed by these specialists, can enhance patient outcomes by guiding appropriate interventions, such as cardiovascular risk management in cardiology, hormonal considerations in gynecology, and opportunity to treat migraine comorbidity among psychiatric disorders.
Conclusions
MA is a multi-faceted phenomenon with several different features and a wide spectrum of presentations. The review of all clinical studies on MA shows the possibility of having hundreds of scenarios. This is particularly true for visual symptoms, the combinations of symptoms and their temporal features. These aspects can change from patient to patient but also in the same patient. With that in mind, we propose a diary to record the feature of each MA aspect during an attack. This tool could improve MA management in daily practice such as differential diagnosis from other serious neurological disorders (i.e., transient ischemic attacks or epilepsy), monitoring aura evolution over time, management of cardiovascular risk, contraceptive use, smoking cessation. It could also be of utmost importance for basic research (i.e., pairing of various preclinical data with the spectrum of clinical manifestation) and clinical research (i.e., patient subdivisions in endophenotypes in populations undergoing functional images studies). Better awareness of migraine aura is key to improving better management and quality of life.
Clinical implication
Typical migraine aura is characterized by transient focal neurologic symptoms such as visual, sensory, dysphasic and other higher cortical dysfunctions.
Their manifestations are multi-faceted, with both inter- and intra-variability, generating hundreds of possible scenarios.
This is particularly true for visual symptoms, the combinations of symptoms and their temporal features.
The optimal knowledge of the entire spectrum of clinical phenotypes is very important for both everyday clinical practice and for basic and clinical research.
The diary proposed here is to prospectively record migraine aura features, which takes a step forward toward a precise phenotypic classification, of utmost significance for medical doctors and researchers.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.