
Abstract
Background
The stigma associated with migraine impacts patients’ quality of life, mental health and their willingness to seek treatment. The present study aimed to gain insights into the stigma from the patient's perspective and to assess migraine knowledge among people without the condition.
Methods
This cross-sectional descriptive, quantitative study used two surveys (survey 1, open April 2023 to July 2023; survey 2, September 2023 to November 2023). The surveys were distributed to local patient organisations across 26 European countries and nine countries in South and North America, Asia and Oceania.
Results
Survey 1 received 3712 answers. Most respondents were women (3444; 92.8%), 45–54 years (1090; 29.4%) and experienced severe migraine (2047; 55.1%). Most participants viewed their migraine as disabling (2655; 71.5%) and felt that medical professionals only partially understood (2135; 57.5%). Survey 2 gathered 774 responses, with most of the participants being partners (202; 26.1%), friends (196; 25.3%) or other relatives (110; 14.2%) of individuals with migraine. The significant majority of respondents demonstrated a high understanding of migraine (573; 74.0%) and predominantly recognised migraine as disabling and impacting personal and professional life. Responders felt a high degree of stigma, more from work colleagues and medical professionals than from their social network.
Conclusions
The disabling nature of migraine, combined with the associated stigma, aggravates the challenges faced by patients. There is an urgent need for improved medical education, public awareness campaigns and possible revisions in medical terminology to better support people with migraine and mitigate the stigma they encounter. Importantly, medical professionals need to re-double efforts to check their behaviour to avoid adding to the burden of our patients.
This is a visual representation of the abstract.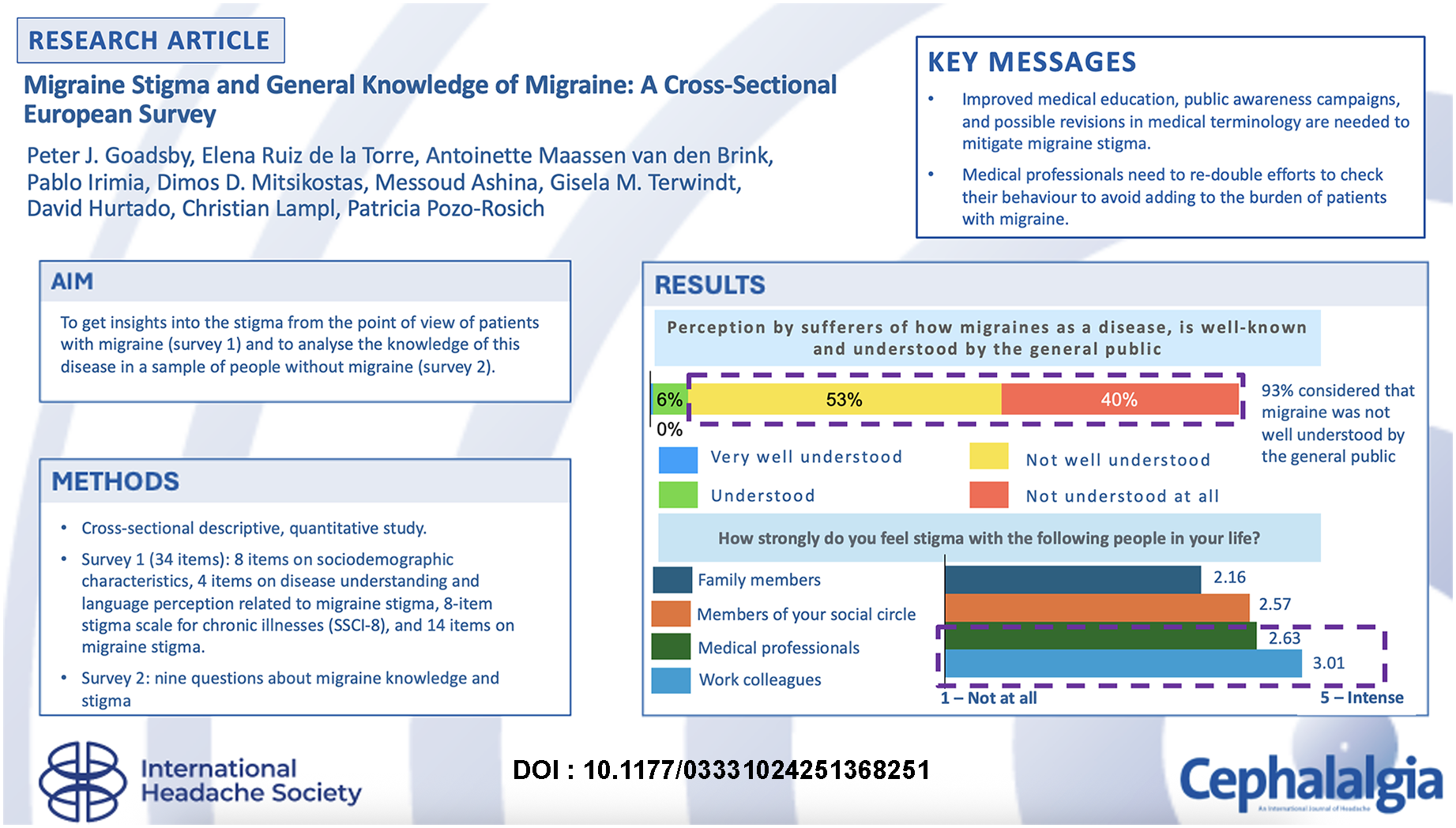
Keywords
Introduction
Migraine is a prevalent and disabling neurological condition characterized by recurrent headaches, often accompanied by nausea, vomiting, and sensitivity to light and sound (1,2-3,4-6,7). However, stigma related to this disorder remains an unexplored, yet particularly relevant, construct.
Stigma has multiple dimensions and can be defined, among other terms, as enacted and internalised stigma. Enacted stigma comprises the negative attitudes expressed by individuals encountered regularly by the person with the disease, such as healthcare professionals, work colleagues or employers. Internalised stigma is characterised by endorsing stereotypes and prejudices, leading to self-discrimination and negative reactions (8-10). Emerging evidence shows that a significant proportion of migraine patients experience stigma often or very often, with prevalence rates ranging from 25.5% among those with fewer than four headache days per month to 47.5% among those with 15 or more headache days. Besides, a higher frequency of stigma is associated with increased disability, greater interictal burden and reduced quality of life (11-14). Studies have shown that stigma is correlated with the degree of job-related disability and the overall impact of migraine on daily life (10,14-15). These efforts are essential in promoting better health outcomes and improving the quality of life for patients with migraine.
Despite the progress in understanding the stigma of migraine, current studies have several limitations. One major drawback is their small sample size, which may not be representative of the broader population of people with migraine (14,19).
Therefore, the European Migraine and Headache Alliance (EMHA), a non-profit organisation representing 34 patient associations across Europe, decided to collect data regarding stigma and knowledge of migraine in a large population through two surveys. The aim of the first survey was to obtain insights into the stigma from the point of view of patients with migraine, and that of the second survey was to analyse the knowledge of this disease in a sample of people without migraine. The data were presented in preliminary form at the 10th Congress of the European Academy of Neurology (29 June to 2 July 2024, Helsinki, Finland) (20).
Methods
Study design and setting
This was a cross-sectional descriptive, quantitative study using two surveys: the first (survey 1) open between April 2023 and July 2023 and the second (survey 2) between September 2023 and November 2023. Survey 1 targeted only patients with migraine and survey 2 only people without migraine. We emailed the surveys to local patient organisations in 26 countries from Europe and nine countries from South and North America, Asia and Oceania. We asked the participants to provide us consent to use their surveyed data for this study before taking the surveys, which were entirely voluntary; and the questionnaires were confidential. We did not take any specific actions to prevent the multiple participation of a single respondent. Spanish charities are not required to obtain ethics committee approvals for this type of research project. We report the results of the surveys in accordance with the Consensus-Based Checklist for Reporting of Survey Studies guidelines (21).
Data collection
EMHA prepared a draft version of the questionnaires by taking into consideration migraine questions that were deemed more relevant and critical for patients. We prepared the questionnaire using Microsoft Forms. The draft versions were submitted to a Steering Committee formed by representatives from EMHA, pharmaceutical companies and key opinion leaders in the migraine field. The final version of the questionnaire was then made available in 17 different languages. The surveys were available through social media channels (Facebook, Twitter, Instagram and LinkedIn) and the EMHA internal newsletter (https://www.emhalliance.org/about-emha/#all-members). Survey 1 was composed of four sections with a total of 34 items: (i) eight items on sociodemographic characteristics; (ii) four items on understanding the disease and language perception related to migraine stigma; (iii) the 8-item Stigma Scale for Chronic Illnesses (SSCI-8) (8); and (iv) 14 items on migraine stigma (see supplementary material, Doc. S1). Survey 2 comprised a single section mixing nine questions about migraine knowledge and stigma. For the SSCI-8, we considered questions 1, 2, 4, 5 and 8 as enacted stigma, questions 6 and 7 as internalised stigma, and question 3 as both enacted and internalised (8).
Migraine severity and treatment refractoriness were self-reported by survey respondents according to the questions “How would you describe most of your migraine attacks (>60%) according to the following parameters? In terms of severity (mild, moderate, or severe) and in terms of response to treatment with medicines (my medicines usually resolve the episodes, I need to take medicines for several days, or episodes persist even if taking my medicines)” (see supplementary material, Doc. S1). For answers requiring a rating scale, we used a five-point Likert item (22), always ranging from one as the lowest to five as the highest score, except for categorising mental and neurological diseases-related stigma, where the scale was inverted (1 for the highest stigma and 5 for the lowest stigma). For survey 1, we only selected participants with migraine using convenience sampling. For survey 2, we only considered participants without migraine.
Statistical analysis
A Prescient Healthcare Group (https://prescienthg.com) consulting team conducted data analysis. We presented categorical data as absolute numbers and percentages and continuous variables as the mean ± SD. For missing data, we extrapolated a percentage from the answers of the global population. We analysed answers by country of residence and did not apply any cut-off; all answers were considered. The data was checked for quality, including evaluating response patterns and inconsistencies.
Results
Sociodemographic characteristics (survey 1)
In total, 3712 answers were received for survey 1. The vast majority of respondents were women (3444; 92.8%) between 45 and 54 years old (1090; 29.4%) with severe migraine (2047; 55.1%). Out of the respondents who were employed part-time (670; 18.0%) or unemployed (309; 8.3%) (Table 1), 758 (77.4%) considered that their employment status was somewhat affected by their migraine. Most patients with severe migraine (2047; 55.1%) reported ≥15 days of migraine per month (899; 43.9%), but a non-negligible part reported 8–14 days (567; 27.7%) or 4–7 days of migraine per month (406; 19.8%). Although 568 (15.3%) of respondents had 0–3 migraine attacks per month, only 123 (3.3%) considered their disease as mild. The vast majority of those with 0–3 days of migraine per month considered their attacks disabling (329; 57.9%) or with some impact on their daily activity (215; 37.9%). The most common countries of residence of most respondents to survey 1 were Spain (807; 21.7%), France (508; 13.7%), Italy (429; 11.6%) and Germany (371; 10.0%) (Figure 1).

Country of residence of participants in survey 1.
Sociodemographic characteristics of study participants with migraine (survey 1).

Migraine stigma: patient perspective (survey 1)
Migraine attacks had some degree of impact on almost all survey respondents, with the majority (2655; 71.5%) considering them disabling. In addition, many respondents felt they were refractory to migraine treatment (1460; 39.3%) (Table 2). Most patients with migraine considered that their disease was not well understood (1978; 53.3%) or not understood at all (1496; 40.3%) by the general public. Patients with severe migraine showed the highest SSCI-8 score (mean = 20.20; SD = 0.59). Notably, mean values stratified by severity showed high uniformity since their SD values were small (0.28 for mild migraine and 0.51 for moderate migraine). Survey participants showed higher degrees of internalised stigma (mean = 2.59; SD = 0.30) than enacted stigma (mean = 2.09; SD = 0.57). As migraine severity increased, patients felt less comfortable discussing their attacks with family and saw their relationships with others more affected (Table 3).
Migraine perception (survey 1).

Migraine stigma (survey 1).

The 8-items/questions on the Stigma Scale for Chronic Illness (SSCI) were rated on a five-point Likert item from 1, never (lowest stigma) to 5, always (highest stigma).
Most patients considered that medical professionals understood their condition only to a certain extent (2135; 57.5%). When asked to rate from one (not at all) to five (intense) the strength of stigma they felt, mean values showed it was more perceived around work colleagues (mean = 3.01, SD = 1.37, median = 3) and medical professionals (mean = 2.63, SD = 1.27, median = 3) than around members of their social circle (mean = 2.57, SD = 1.21, median = 2) or family (mean = 2.15, SD = 1.26, median = 2).
Regarding work-related stigma, most patients with migraine (2938; 79.1%) had experienced difficulties in completing work tasks or their careers were affected negatively by their condition. Those with severe migraine considered that their disease affected how their value to the company was assessed more often than those with moderate or mild migraine (Figure 2).

Answer to the question “how do you feel your condition affects the way in which your direct manager assesses your value to the company?” according to migraine severity (survey 1).
When asked about potential steps to reduce stigma, most patients answered that the education on migraine should be broadened (1347; 36.3%) and advocacy for patients increased (1039; 28.2%). A non-negligible portion of them (646; 17.4%) considered a change in wording/lexicon used to describe migraine as an interesting step towards understanding the disease's impact by the general public.
On a scale of 1 to 5, patients with migraine classified their own disease as the one with the lowest stigma (mean = 2.70) among other mental disorders (the highest was depression; mean = 2.52), but was more stigmatising, according to them, than other disorders, such as multiple sclerosis (mean = 2.97) or epilepsy (mean = 2.97) (see supplementary material, Figure S1).
Migraine knowledge of people without migraine (survey 2)
In total, 774 answers were received for survey 2. Most of the participants were partners (202; 26.1%), friends (196; 25.3%) or other relatives (110; 14.2%) of patients with migraine, and 100 (12.9%) had no relationship with someone with migraine (Figure 3).

Relationship of non-migraine participants with patients with migraine in survey 2 (n = 774).
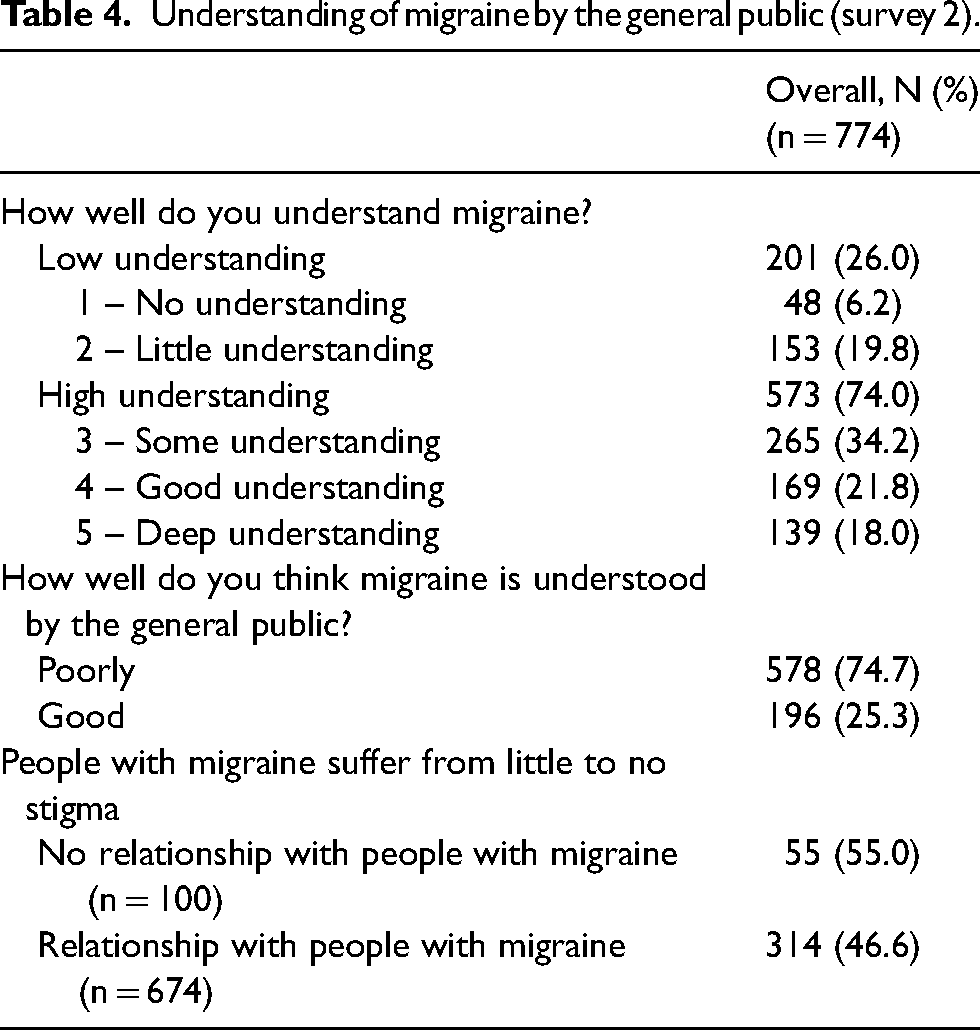
The vast majority of respondents were considered to have a high understanding of migraine (573; 74.0%) and mostly evaluated the general public as having a poor understanding of the disease (578; 74.7%) (Table 4).
Understanding of migraine by the general public (survey 2).
When asked to define migraine, a higher percentage of those with a high understanding of the disease gave positive responses (disabling, affecting personal and professional life). On the other hand, those with a low understanding of migraine had a higher percentage of answers in the negative responses (depending on patients’ behaviour, a strong headache, mental health issue, an excuse, not a disease) (Figure 4).

Migraine definition according to people without migraine with high (blue) and low understanding (red) of the condition (survey 2). The level of understanding of migraine was evaluated in a separate survey question.
Discussion
In the present study, we analysed two surveys: one examining migraine stigma from the patient's perspective and another assessing the general public's understanding of this condition. Survey 1 revealed that migraine affected employment status, and the disease was not understood by those without migraine, especially work colleagues and medical professionals. Migraine severity was correlated with an increasing SSCI-8 score and lower consideration by work supervisors. Survey 2, analysing data on people without migraine, showed striking differences regarding knowledge of the condition and stigma awareness between those in contact with a patient with migraine and those who did not know anyone with migraine.
As expected, nearly all respondents to survey 1 were women older than 25 years, which is in line with a previous survey with similar characteristics(23). Our surveyed sample was constituted mainly of patients with a high number of migraine days per month, as found in a previous survey (23). We identified a disparity between the number and proportion of patients reporting 0–3 migraine days per month (15.3%) and those considering their disease as mild (3.3%). However, when analysing the impact of migraine attacks on their daily activity, most respondents felt their disease was disabling or had a non-negligible impact. This finding would suggest that migraine severity should take into account a multiparameter perspective (including pain severity, associated symptoms, variability in treatment response and associated comorbidities) beyond the sole frequency aspect, as has already been suggested (24-26).
In addition, the proportions of the different employment statuses in the present study were similar to those previously reported (23). However, among part-time employees and those unemployed, the high percentage (77.4%) who considered that migraine affected their status was striking and had not been previously described. The proportion of participants who considered themselves refractory to migraine treatment (39.3%) was in agreement with a previous study (between 28.9% and 46%) surveying physicians with interest in headache care (27). Regarding stigma self-reported with the SSCI 8-item and according to mean values, migraine, in our sample, was considered more stigmatising (18.48), especially by severe migraine patients (20.20), than other conditions, such as rheumatoid arthritis (17.85) (28-9,29).
A significant concern from our study was that most patients felt that medical professionals only partially understood their condition and were among the groups from whom they felt the highest stigma. This perception may be correlated with the low or moderate confidence among physicians in managing resistant or refractory migraine (27), especially given the high number of self-reported patients with refractory migraine in our survey. Notably, the environment where patients perceived the most stigma was among work colleagues, contrasting with a previous study that reported a moderate degree of support by work colleagues (63.1%), although over half of those surveyed (55.4%) did not feel supported by their company (30). These discrepancies could be due to differences in study methodology or varying proportions of survey respondents from each participating country.
The substantial burden that migraine and related disorders such as cluster headache place on individuals has been extensively demonstrated, with a high impact on the professional, private and social domains of patient's life and substantiated impact on productivity due to unemployment, absenteeism, presenteeism and early retirement of people living with these conditions (31,32-30). Although no data regarding the migraine severity of study participants was described for that study, we could assume that the selection bias towards patients with severe migraine in our study could have influenced this result.
Interestingly, beyond the typical actions suggested by patients to alleviate stigma, including improving education and awareness and increasing patient advocacy (12,33), condition rebranding was also proposed by our surveyed patients with migraine. Terminology can significantly influence public perception and understanding of medical conditions. For example, renaming a condition to reflect better its severity and impact can lead to increased empathy and support from the public and medical professionals. This approach has been suggested, among other areas, in schizophrenia or post-traumatic stress disorder and holds the potential for reducing migraine stigma (34,35). Future research should explore the effectiveness of such interventions in changing public attitudes and improving the quality of life for patients with migraine.
Concerning survey 2, the general public confirmed that migraine is poorly understood and that those without personal connections to patients with migraine tended to be less empathetic. This lack of understanding can lead to social isolation, reduced support, and increased psychological distress for patients with migraine. As described in detail in the literature, migraine is a spectrum of experiences ranging from mild intermittent attacks with little impact on daily life to completely disabling and uncontrolled headache worsening. Educating the general public to foster empathy and understanding is a key step, promoted by advocacy patient groups, towards eliminating stigma for this condition (15,33).
Limitations
The generalisability of our study may be limited since most of our respondents lived in Southern or Western Europe and had severe migraine. In addition, our study was limited by the self-report nature of the survey, which might reduce accuracy. Although the sample size of people with migraine could not be considered small, other survey studies on migraine have been undertaken in larger populations (31). This could also imply that, in Europe, a continent with a large population, the representativeness of our sample could be limited. Finally, as already mentioned, the selection bias of participants coming mainly from patients’ organisations should be borne in mind when interpreting the results. Members of migraine patient organisations tend to have moderately to highly active conditions, thus neglecting patients with mild migraine.
Conclusions
Our first survey highlighted the significant impact of migraine on employment status, societal understanding and interactions with medical professionals and the general public. The disabling nature of migraine, coupled with the stigma associated with the condition, exacerbates the challenges faced by patients. Responses from our second survey underscored an urgent need for improved medical education, public awareness campaigns and potential changes in medical terminology to support patients with migraine better and reduce the stigma they encounter. Future research should continue to explore these areas to develop effective interventions that enhance the quality of life for individuals with migraine.
Clinical implications
All patients with migraine perceived stigma, but those with severe migraine showed the highest SSCI-8 score.
Most patients considered that medical professionals only partially understood their condition and were among the groups from whom they felt the highest stigma.
Migraine is poorly understood and can lead to social isolation, reduced support and increased psychological distress.
Supplemental Material
sj-docx-1-cep-10.1177_03331024251368251 - Supplemental material for Migraine stigma and general knowledge of migraine: A cross-sectional European survey
Supplemental material, sj-docx-1-cep-10.1177_03331024251368251 for Migraine stigma and general knowledge of migraine: A cross-sectional European survey by Peter J. Goadsby, Elena Ruiz de la Torre, Antoinette Maassen van den Brink, Pablo Irimia, Dimos D. Mitsikostas, Messoud Ashina, Gisela M. Terwindt, David Hurtado, Christian Lampl and Patricia Pozo-Rosich in Cephalalgia
Supplemental Material
sj-jpg-2-cep-10.1177_03331024251368251 - Supplemental material for Migraine stigma and general knowledge of migraine: A cross-sectional European survey
Supplemental material, sj-jpg-2-cep-10.1177_03331024251368251 for Migraine stigma and general knowledge of migraine: A cross-sectional European survey by Peter J. Goadsby, Elena Ruiz de la Torre, Antoinette Maassen van den Brink, Pablo Irimia, Dimos D. Mitsikostas, Messoud Ashina, Gisela M. Terwindt, David Hurtado, Christian Lampl and Patricia Pozo-Rosich in Cephalalgia
Footnotes
Acknowledgements
We thank all participants in the two surveys for making this study possible. The medical writing support provided by Matías Rey-Carrizo, PhD, at BCN Medical Writing was funded by EMHA Alliance.
Data availability statement
The data underlying this article will be shared upon reasonable request to the corresponding author.
Declaration of conflict of interests
PJG reports personal fees for consulting from Aeon Biopharma, AbbVie, Aurene, CoolTech LLC, Dr Reddy's, Eli Lilly and Company, Epalex, Kallyope, Linpharma, Lundbeck, Pfizer, PureTech Health LLC, Satsuma, Shiratronics, Teva Pharmaceuticals, Tremeau and Vial; personal fees for advice through Gerson Lehrman Group, Guidepoint, SAI Med Partners and Vector Metric; fees for educational materials from CME Outfitters and WebMD; and publishing royalties or fees from Massachusetts Medical Society, Oxford University Press, UptoDate and Wolters Kluwer. PI reports personal fees for consultancy and participation as a speaker in educational activities from Eli Lilly, Novartis, Teva Pharmaceuticals, AbbVie, Lundbeck, Organon and Pfizer. DDM has received fees and travel grants from Allergan, Amgen, Bayer, Biogen, Cefaly, electroCore, Eli Lilly, Genesis Pharma, Merck Serono, Merz, Mylan, Novartis, Orion Pharma, Roche, Sanofi Genzyme, Pfizer and Teva Pharmaceuticals; has participated in clinical trials for Amgen, Eli Lily, Lundberg, Novartis, Pfizer and Teva Pharmaceuticals, as principal investigator; is president of the Hellenic Headache Society; is a member of the Management Group of the Headache Scientific Panel of the European Academy of Neurology; and a past-President of the European Headache Federation. MA is a consultant, speaker or scientific advisor for AbbVie, Amgen, Astra Zeneca, Eli Lilly, GlaxoSmithKline, Lundbeck, Novartis, Pfizer and Teva; a primary investigator for ongoing AbbVie and Pfizer trials; and is the past president of the International Headache Society; he is supported through the Lundbeck Foundation institutional grant (R310-2018-3711) and serves as associate editor of the Journal of Headache and Pain, and associate editor of Brain. PP-R has received honoraria as a consultant and speaker from AbbVie, Amgen, Dr Reddy's, Eli Lilly, Lundbeck, Medscape, Novartis, Organon, Pfizer and Teva Pharmaceuticals. Her research group has received research grants from AbbVie, AGAUR, EraNet Neuron, FEDER RIS3CAT, Instituto Investigación Carlos III, MICINN, Novartis and Teva Pharmaceuticals, and has received funding for clinical trials from AbbVie, Amgen, Biohaven, Eli Lilly, Lundbeck, Novartis, Pfizer and Teva Pharmaceuticals. She is the Honorary Secretary of the International Headache Society and is an associate editor for Cephalalgia and Neurologia. She is a member of the Clinical Trials Guidelines Committee of the International Headache Society. She has edited the Guidelines for the Diagnosis and Treatment of Headache of the Spanish Neurological Society. She is the founder of ![]() . All other authors declare no conflict of interest with the present study.
. All other authors declare no conflict of interest with the present study.
Ethical statement
Spanish charities are not required to obtain ethics committee approvals for this type of research project.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.