
Abstract
Data on the association of the MTHFR 677C→T and ACE D/I polymorphisms with migraine severity, measured by attack frequency, are scarce. We performed an association study among 24 961 women participating in the Women's Health Study. Migraine, aura status and attack frequency were self-reported. Multinomial logistic regression was used to investigate the genotype–migraine association. Among the 3186 migraineurs with complete genotype and attack frequency data, 1270 reported migraine with aura (MA) (attack frequency 76 ≥ weekly; 219 monthly; 123 every other month; 852 fewer than six times/year) and 1916 migraine without aura (MoA) (attack frequency: 85 ≥ weekly; 414 monthly; 208 every other month; 1209 fewer than six times/year). The MTHFR 677TT genotype was associated with a reduced risk for MA, which only appeared for attacks fewer than six times/year (age-adjusted odds ratio 0.78; 95% confidence interval 0.61, 0.99). We did not find a specific pattern of association of the ACE D/I polymorphism with attack frequency for MA or MoA.
Introduction
Migraine is a common chronic neurological disorder affecting 10–20% of the population, predominantly women (1). Typically, migraine presents with recurrent headache attacks and various combinations of gastrointestinal and autonomic nervous system symptoms (2,3). Up to one-third of migraine patients experience an aura prior to or during the migraine headache characterized by neurological symptoms most often involving the visual field.
Migraine pathophysiology involves both multiple genetic and environmental factors (4). Current concepts view migraine as an inherited disorder of the brain, but vascular mechanisms are clearly implicated (5). Gene variants in the methylenetetrahydrofolate reductase gene (MTHFR 677C→T polymorphism, rs1801133) and in the angiotensin-converting enzyme gene (ACE D/I polymorphism, rs1799752) appear to play important roles in the vascular oxidative stress response (6,7). Oxidative stress may lead to endothelial dysfunction and explain, at least in part, pathological vascular reactivity among migraineurs (8) and the association between migraine and cardiovascular disease (CVD) seen in epidemiological studies (9–11).
However, studies on the association between the MTHFR 677C→T (12–24) and the ACE D/I (24–32) polymorphism and migraine, including aura status, have yielded conflicting results. This may in part be due to the often heterogeneous clinical phenotypes among patients diagnosed with migraine. One attempt to create more homogeneous groups may be to categorize patients according to migraine severity. Migraine attack frequency, in addition to aura status, is considered a marker of migraine severity. Certain gene variants may reveal a differential association with migraine depending on attack frequency, as recently suggested (33).
We have recently reported a modestly reduced risk for migraine with aura (MA) among carriers of the MTHFR 677TT genotype (22) and a lack of association for the ACE D/I polymorphism (31) for both MA and migraine without aura (MoA) in a large cohort of White women participating in the Women's Health Study (WHS). This report presents additional analyses investigating whether our observed patterns of association differ according to migraine attack frequency.
Subjects and methods
We have previously reported on the association between the MTHFR 677C→T (22) and ACE D/I (31) polymorphisms and migraine. For reasons of comprehensiveness we will report the important results again along with the new data. However, these may differ minimally from the original data because we have excluded an additional 40 women with missing attack frequency data for the present analysis.
Study population
The WHS was a randomized trial designed to test the benefits and risks of low-dose aspirin and vitamin E in the primary prevention of CVD and cancer. The design, methods and results have been described in detail previously (34,35). Briefly, a total of 39 876 US female health professionals aged ≥ 45 years at study entry (1992–1995) without a history of CVD, cancer, or other major illnesses were randomly assigned to active aspirin (100 mg on alternate days), active vitamin E (600 IU on alternate days), both active agents, or both placebos. All participants provided written informed consent and the Institutional Review Board of Brigham and Women's Hospital approved the WHS. Baseline information was self-reported and collected by a mailed questionnaire that asked about many cardiovascular risk factors and lifestyle variables.
Blood samples were collected in tubes containing ethylenediamine tetraaceticacid (EDTA) from 28 345 participating women prior to randomization. After excluding participants with missing information on migraine and with reported CVD or angina prior to receiving the baseline questionnaire (n = 505), 27 840 women remained in the dataset. We further excluded women with missing information on the MTHFR 677C→T and ACE D/I polymorphisms (n = 1411), non-White women (n = 1428), and those with missing information on attack frequency among active migraineurs (n = 40), leaving 24 961 White women for analyses.
Assessment of migraine
Participants were asked on the baseline questionnaire: ‘Have you ever had migraine headaches?’ and ‘In the past year, have you had migraine headaches?’. From this information, we categorized women into ‘any history of migraine’; ‘active migraine’, which includes women with self-reported migraine during the past year; and ‘prior migraine’, which includes women who reported ever having had a migraine but none in the year prior to completing the questionnaire. In a previous study (11), we have shown good agreement of our classification with the 1988 International Headache Society (IHS) criteria for migraine (36) and have shown excellent agreement between self-reported migraine and the second edition of the International Classification of Headache Disorders (ICHD-II)-based migraine classification in a WHS subcohort (37). Participants who reported active migraine were asked further whether they had an ‘aura or any indication a migraine is coming’. Responses were used to classify those women into active MA and active MoA. In addition, participants with active migraine were asked about the ‘approximate frequency of their migraines’ (daily, weekly, monthly, every other month, fewer than six times per year). We will refer to active migraine with aura as MA and to active migraine without aura as MoA in this report.
Genotype determination of the MTHFR 677C→T (rs1801133) and the ACE D/I (rs1799752) polymorphisms
Genotyping was performed in the context of a multi-marker assay (Roche Molecular Systems, Basel, Switzerland) using an immobilized probe approach, as previously described (38). In brief, each DNA sample was amplified by polymerase chain reaction (PCR) with biotinylated primers. Each PCR product pool was then hybridized to a panel of sequence-specific oligonucleotide probes immobilized in a linear array. The colorimetric detection method was based on the use of streptavidin–horseradish peroxidase conjugate with hydrogen peroxidase and 3,3′,5,5′-tetramethylbenzidine as substrates. Linear array processing was facilitated by the use of the AutoRELI-Mark II (Dynal Biotech, Carlsbad, CA, USA). Genotype assignment was performed using the proprietary
Dietary assessment
At baseline, participants completed a 131-item semiquantitative food frequency questionnaire (39). Nutrient intake was calculated based on the content of the portion sizes multiplied by the frequency of consumption and was adjusted for total energy intake by the residual method (40). In addition, participants were asked to report the type and amount of vitamin supplement use. Intake of folate and B-vitamins from supplements was calculated with a comprehensive multivitamin database.
Homocysteine measurements
The EDTA blood samples were stored in vapour phase liquid nitrogen (−170°C). The concentration of homocysteine was determined using an enzymatic assay on the Hitachi 917 analyser (Roche Diagnostics) using reagents and calibrators from Catch Inc. (Seattle, WA, USA).
Statistics
We compared baseline characteristics of participants with respect to their MTHFR 677C→T and ACE D/I genotype status using the χ2 test for categorical variables and the Kruskal–Wallis test for continuous variables.
Multinomial logistic regression models were used to evaluate the association between MTHFR 677C→T and ACE D/I genotypes and migraine. We calculated odds ratios (ORs) and 95% confidence intervals (CIs) for MA and MoA as well as for frequency categories (≥ weekly, monthly, every other month, fewer than six times per year). We built additive, dominant and recessive models. The additive model assumes that the risk for migraine among carriers of the heterozygous genotype (MTHFR 677CT; ACE DI) is half way between carriers of the homozygous wild-type (MTHFR 677CC; ACE DD) and the homozygous mutant genotype (MTHFR 677TT; ACE II). The dominant model assumes that carriers of the heterozygous (MTHFR 677CT; ACE DI) and homozygous mutant (MTHFR 677TT; ACE II) genotypes have the same risk for migraine compared with carriers of the homozygous wild-type genotype (MTHFR 677CC; ACE DD). The recessive model assumes that carrying the homozygous mutant genotype (MTHFR 677TT; ACE II) is necessary to alter the risk for migraine compared with carriers of the heterozygous (MTHFR 677CT; ACE DI) and homozygous wild-type (MTHFR 677CC; ACE DD) genotypes. We built age-adjusted and multivariable-adjusted models. In the multivariable-adjusted model investigating the ACE D/I polymorphism we included the following covariates: age (continuous), body mass index (continuous), exercise (never, < 1/week, 1–3/week, ≥ 4/week), postmenopausal hormone use (never, past, current), history of oral contraceptive use (yes, no, not sure), history of hypertension (yes, no), history of diabetes (yes, no), alcohol consumption (never, 1–3 drinks/month, 1–6 drinks/week, ≥ 1 drinks/day), smoking (never, past, current < 15 cigarettes/day, current ≥ 15 cigarettes/day), and family history of myocardial infarction prior to age 60 (yes, no). In the multivariable-adjusted model investigating the MTHFR 677C→T polymorphism we additionally included serum homocysteine levels (continuous), folate intake (continuous), vitamin B2 intake (continuous), vitamin B6 intake (continuous) and vitamin B12 intake (continuous). We incorporated a missing value indicator if the number of women with missing information on covariates was ≥ 100 or imputed a value otherwise.
All analyses were performed using
Results
Baseline characteristics of participants in the Women's Health Study according to MTHFR 677C→T and ACE D/I genotypes (n = 24 961)*

Proportions may not add up to 100 because of rounding or missing values.
Data are expressed as percentages unless otherwise stated.
P-values for χ2 test for categorical variables, and Kruskal–Wallis test for continuous variables.
IQR, interquartile range; MI, myocardial infarction.
At baseline, 4537 (18.2%) women reported any history of migraine; 3186 of those reported active migraine. Among the 1270 women with MA (39.9% of active migraineurs), 76 reported an attack frequency ≥ weekly, 219 of monthly, 123 of every other month and 852 of fewer than six times/year. Among the 1916 women with MoA, the numbers were: 85 (attack frequency ≥ weekly), 414 (monthly), 208 (every other month) and 1209 (fewer than six times/year).
The genotype distribution for MTHFR 677C→T was in Hardy–Weinberg equilibrium among women with and without any history of migraine (χ2 with 1 degree of freedom: P = 0.38 and P = 0.06, respectively). The genotype distribution for the ACE D/I polymorphism deviated from Hardy–Weinberg equilibrium for women with and without history of migraine (χ2 with 1 degree of freedom: both P < 0.0001).
Genotype and allele distribution for the MTHFR 677C→T and ACE D/I polymorphisms among women with and without migraine in the Women's Health Study (n = 24 961)

Genotype frequencies are in %, allele frequencies in decimals. Numbers are in parentheses.
Frequencies for any history of migraine comprise those for migraine with and without aura as well as prior migraine.
P-value from χ2 test (2 d.f.) comparing each of the migraine categories with women with no history of migraine.
P-value from χ2 test (1 d.f.) comparing each of the migraine categories with women with no history of migraine.
Results from the age-adjusted and multivariable-adjusted models were very similar for both genotypes, thus we only report results from the age-adjusted models.
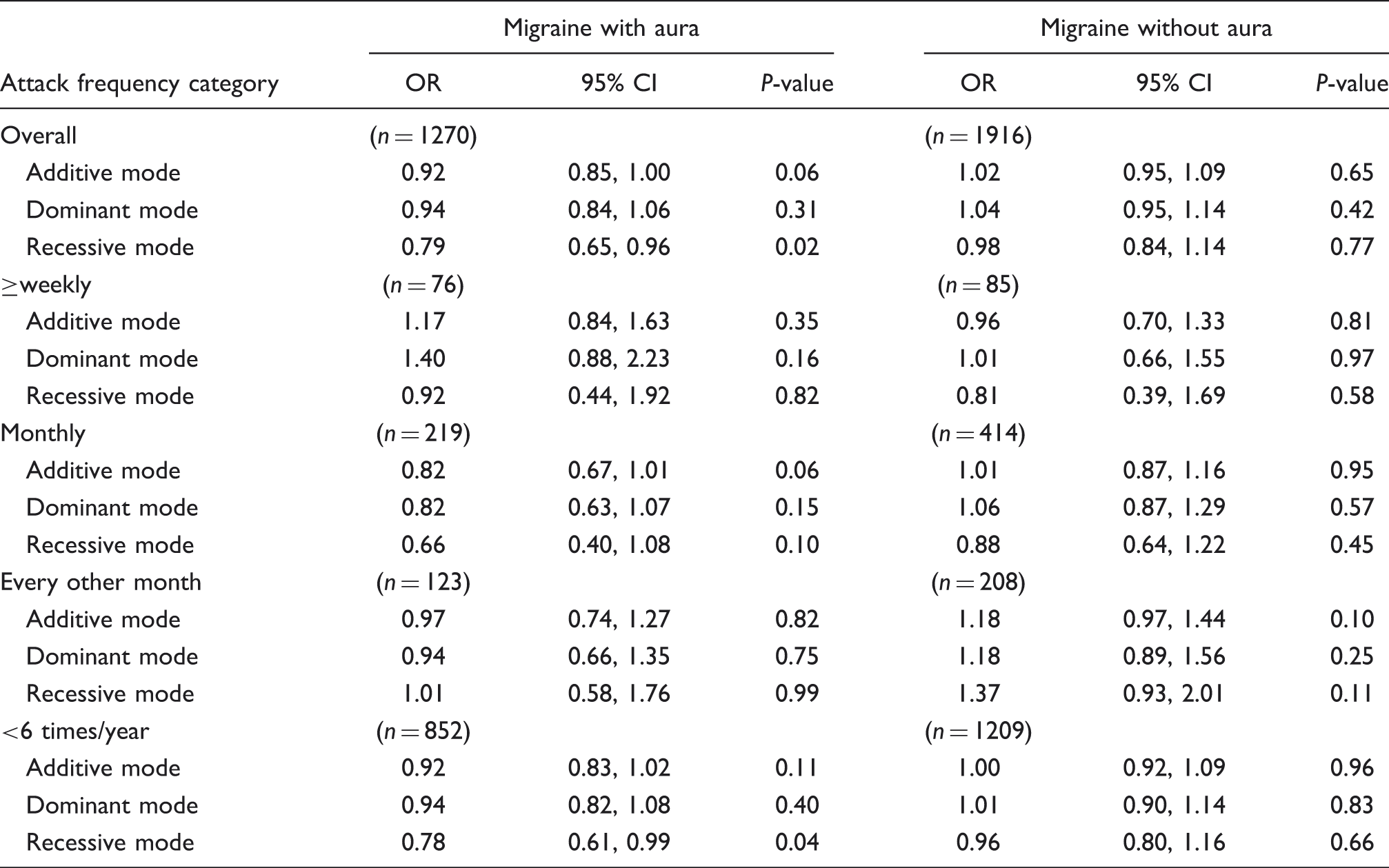
Age-adjusted odds ratios (OR) and 95% confidence intervals (95% CI) for migraine attack frequency according to MTHFR 677C→T polymorphism (n = 24 961). Women with no history of migraine (n = 20 424) serve as the reference group
Age-adjusted odds ratios (OR) and 95% confidence intervals (95% CI) for migraine and attack frequency according to ACE D/I polymorphism (n = 24 961). Women with no history of migraine (n = 20 424) serve as the reference group
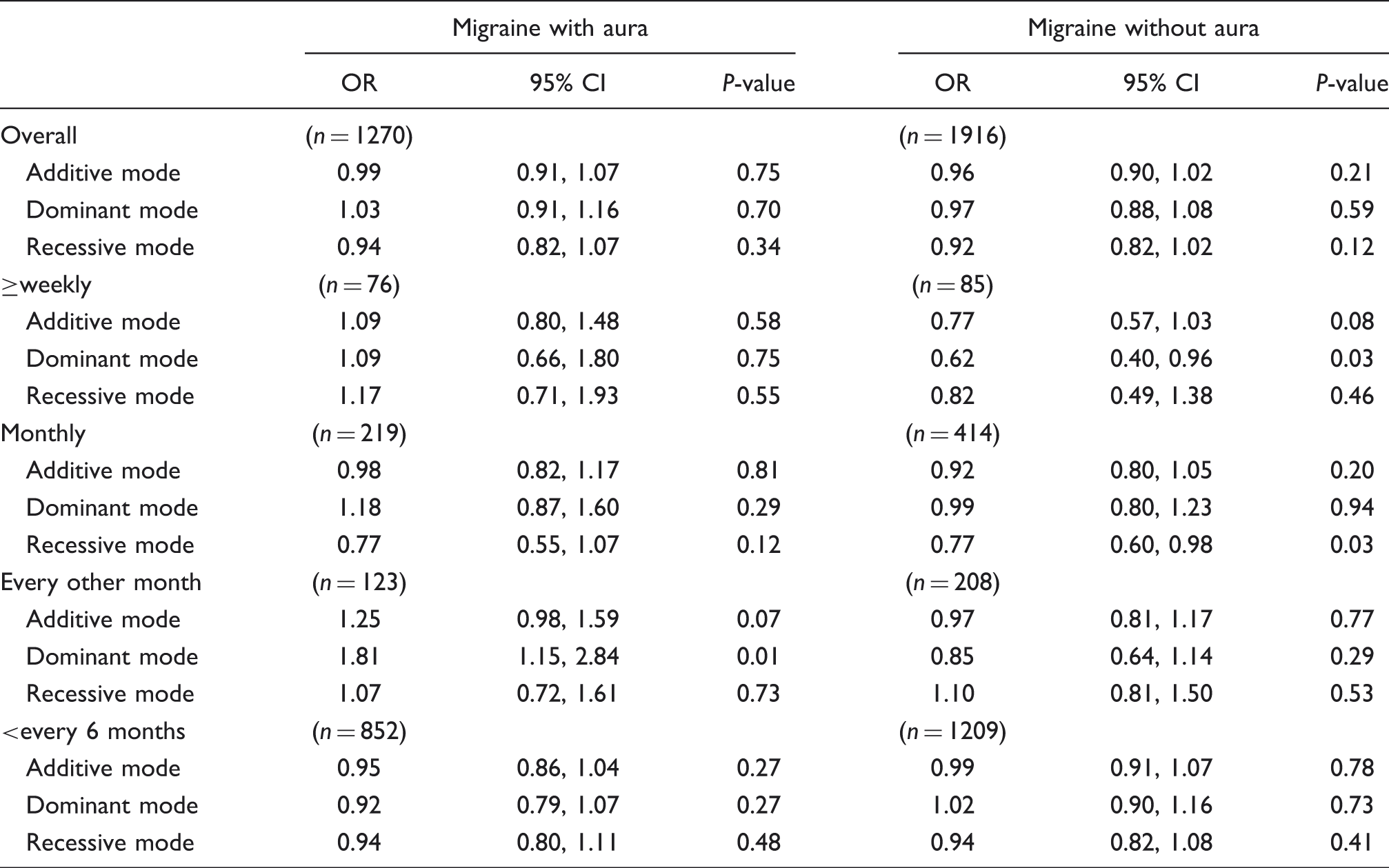
Taken together, our results indicate that the MTHFR 677TT genotype reduces the risk for active MA, which only appears in women with attacks fewer than six times/year. In contrast, with regard to the ACE D/I polymorphism, the results do not show a specific pattern of association with frequency categories for MA or MoA.
Discussion
The results of this large study of White women indicate that the reduced likelihood of having MA among carriers of the MTHFR 677TT genotype (22) appears only among those with infrequent attacks fewer than six times/year. In contrast, none of the ACE D/I genotypes were associated with migraine irrespective of migraine aura status. Further investigation of frequency categories also revealed no specific pattern of association.
The association between migraine, in particular MA, and CVD is consistent in several studies (9–11,41). Alterations in the oxidative vascular stress response are important aspects in the development of CVD, that may also explain in part pathological vascular reactivity seen in young migraineurs (8). The MTHFR 677C→T and the ACE D/I polymorphism have been implicated in the vascular oxidative stress response in CVD and, hence, may also be important in migraine (6,7). However, results on the association between both the MTHFR 677C→T (12–24) and the ACE D/I (24–32) polymorphism and migraine, including aura status, are conflicting. The heterogeneous phenotype of migraine is probably an important reason for this. Migraine severity may be a useful parameter to sub-classify migraine patients further into more homogeneous categories and can, for example, be measured by attack frequency, in addition to aura status. This is supported by recent publications suggesting that migraine behaves differently depending on attack frequency. First, the association between migraine and CVD varies by migraine frequency, specifically in women with MA (42). Second, a study investigating markers of endothelial dysfunction among migraineurs found that the ACE DD genotype is associated with a higher attack frequency (33), which agrees with results of an earlier study on MoA (30).
Our analyses, however, do not suggest that any of the ACE D/I genotypes is associated with MA or MoA (31) or a higher attack frequency (present analysis). Reasons for our different results may include that our cohort was population-based with a lower migraine attack frequency compared with the clinic-based studies with participants reporting more frequent attacks (30,33).
We have previously shown that MA is associated with an about twofold increased risk for CVD, including ischaemic stroke and myocardial infarction (11). This association differs by migraine attack frequency (42). Whereas a high attack frequency (≥ weekly) is associated only with ischaemic stroke, a low attack frequency (< monthly) is associated with any vascular event, including ischaemic stroke, myocardial infarction, etc. Certain gene variants further add to this complexity. For example, the MTHFR 677TT genotype is associated with a modestly reduced likelihood for having MA (22); our present analysis suggests that this appears only among women with infrequent attacks fewer than six times/year. In contrast, co-occurrence of MA and MTHFR 677TTgenotype appears to increase further the risk for ischaemic stroke, but not other vascular ischaemic events (22). This apparent contradiction may be explained in light of the complex migraine pathophysiology involving both neuronal and vascular dysfunctions (5). Migraine aura is probably determined by many gene variants, of which MTHFR 677C→T is just one. We may speculate that while the TT genotype may reduce the risk for migraine aura, migraine attack frequency may further modify the interaction with other tissue-specific gene variants and/or epigenetic effects. This may cause different effects in brain neurons and vascular endothelial cells. This hypothesis also agrees with the concept of a differential pathophysiology between ischaemic stroke and myocardial infarction, which may also be true among migraineurs.
Homocysteine is elevated in carriers of the MTHFR 677TT genotype, as also seen in our data. However, homocysteine is unlikely to be involved in the MTHFR–MA association, as serum levels have shown no association with migraine, migraine aura status, or attack frequency in our cohort (43). Hence, the biology underlying the MTHFR–migraine association remains to be unveiled.
Our study has several strengths, including the large number of participants and women with migraine. Furthermore, we collected information on a large number of baseline characteristics, including medical conditions and lifestyle habits, and the homogeneous nature of the cohort may reduce confounding. However, several limitations should be considered. First, migraine, migraine aura and attack frequency were self-reported and migraine could not be classified according to strict IHS criteria. Thus, misclassification of migraine, migraine aura and attack frequency is possible. However, our prevalence of migraine (18.2%) and migraine aura (39.9%) is similar to those seen in other large population-based studies in the USA (44) and the Netherlands (45), although the data acquisition method was different. Furthermore, we have shown good agreement of our classification (11) with the 1988 IHS criteria for migraine (36) and excellent agreement between self-reported migraine and ICHD-II-based migraine classification in the WHS (37). Second, the genotype distribution for the ACE D/I polymorphism deviated from Hardy–Weinberg equilibrium. This occurred for both women with migraine and women without migraine, thus it is an unlikely indication for genotype-based differential survival. In addition, genotyping error is unlikely given our stringent genotyping protocol. However, this stringency together with the fact that participants were all White female health professionals age ≥ 45 years, not representing all White women, probably accounts for the deviation from Hardy–Weinberg equilibrium. Thus, generalizability may be limited, which may be one reason for the differing results between our study and previous studies on the MTHFR 677C→T and ACE D/I polymorphism and migraine. Third, we had only coarse categorical data on migraine attack frequency and most women reported infrequent attacks. Thus, in contrast to clinic-based studies, which allow more accurate determination of the number of headache days per month, we were not able to investigate potential differences within the group of women reporting monthly and weekly attacks. Fourth, interaction between the ACE D/I and MTHFR 677C→T polymorphisms with regard to migraine risk has been suggested previously (6,28). However, when we grouped women according to genotype status the numbers in some of the cells were too small to run meaningful analyses. Thus, we cannot exclude interactions between these polymorphisms or with other gene variants not in linkage disequilibrium with the variants tested, as well as epigenetic effects. Finally, genetic association studies cannot indicate whether an association is causal or not. Thus, the MTHFR 677TT genotype may be in linkage disequilibrium with other causative genetic variants in nearby genes and may only be a marker for having less frequent attacks among migraineurs.
Future studies investigating the association between the MTHFR 677C→T and ACE D/I polymorphism and migraine severity are warranted. Detailed information on attack frequency, aura status and aura frequency may be important in addition to ICHD-II criteria for migraine. Further, investigation in a non-White population may yield different results.
Footnotes
Competing interests
M. S. has received within the last 5 years investigator-initiated research funds from the Deutsche Forschungsgemeinschaft and honoraria from L. E. K. Consulting for telephone surveys. R. Y. L. Z. has received within the last 5 years research support from the National Heart, Lung, and Blood Institute, the Doris Duke Charitable Foundation, the Leducq Foundation, the Donald W. Reynolds Foundation, and Roche. J. E. B. has received within the last 5 years investigator-initiated research funding and support as Principal Investigator from the National Institutes of Health and Dow Corning Corporation; research support for pills and/or packaging from Bayer Heath Care and the Natural Source Vitamin E Association; and honoraria from Bayer for speaking engagements. T. K. has received within the last 5 years investigator-initiated research funding from the National Institutes of Health, McNeil Consumer & Specialty Pharmaceuticals, Merck, and Wyeth Consumer Healthcare; he is a consultant to i3 Drug Safety and World Health Information Science Consultants, LLC, and has received honoraria from Genzyme, Merck, and Pfizer for educational lectures.
Acknowledgements
The Women's Health Study is supported by grants from the National Heart, Lung, and Blood Institute (HL-43851 and HL-080467), and the National Cancer Institute (CA-47988). The research for this work was supported by grants from the Donald W. Reynolds Foundation, the Leducq Foundation, and the Doris Duke Charitable Foundation. The authors also thank F. Hoffmann La-Roche and Roche Molecular Systems, Inc. for supporting the genotype determination financially and with in-kind contribution of reagents and consumables. The authors are indebted to the participants in the Women's Health Study for their outstanding commitment and cooperation, and to the entire Women's Health Study staff for their expert and unfailing assistance.