
Abstract
We have recently developed an instrument to describe and categorize severity of migraine attacks from patient self-report, the MIGSEV questionnaire. We have now performed a large prospective survey using this tool to evaluate migraine severity in 2979 patients consulting for headache in France, included by 1164 general practitioners, 174 neurologists and 82 gynaecologists. The objective of the study was to determine the prevalence of severity grades in a large population who consults for migraine, to test the concordance between severity calculated from physician-derived and patient-derived data, and to test the relevance of the concept of severity as applied to diagnosis, other measures of the burden of migraine, and to health-related quality of life. Severe attacks were reported in around one-fifth of the sample. Physician- and patient-derived data provided concordant estimates of severity in 71% of cases, the discordant cases representing principally an underestimate by the physician of headache severity. Migraine severity was associated with frequent, long-lasting and treatment-resistant attacks, and with poor quality of life. The MIGSEV questionnaire is proposed as a simple measure of severity for the diagnosis and management of migraineurs, suitable for use both by physicians and patients.
Introduction
It is increasingly recognized that a valid assessment of severity is a prerequisite to optimize the medical management of migraine (1, 2), and to control the economic cost of this chronic condition (3, 4). While the diagnostic criteria developed by the International Headache Society (5) have been widely validated and are now used extensively in epidemiological research, no such tool exists for evaluating severity. Moreover, the concept of migraine severity is rather an imprecise one, and is often used by authors without being clearly defined (6).
To address this shortcoming, we have recently evaluated a number of parameters that could be used to characterize the severity of migraine attacks. These were identified from the clinical literature during expert consensus meetings and tested during patient interviews. From this initial selection, we developed a simple severity scale (the MIGSEV questionnaire) which could be used to assess the severity of individual migraine attacks (7). This uses replies to questions about four of these parameters (intensity of pain, disability in daily activity, tolerability and nausea) to categorize migraine attacks as mild, moderate or severe. The MIGSEV questionnaire was validated in a pilot study of 287 migraineurs, and showed good metrological properties in terms of reliability, reproducibility and sensitivity.
The objective of the present study was to determine migraine severity using the MIGSEV questionnaire in a large population survey of patients consulting for headache, to test the concordance between severity calculated from physician-derived and patient-derived data, and to test the relevance of the concept of severity as applied to diagnosis, other measures of the burden of migraine, and to health-related quality of life.
Methods
The objective of the study was to estimate the distribution of migraine severity grades in a population of patients consulting for migraine, to compare subjective and algorithm-assigned ratings of severity, and to assess the relationship between severity and quality of life. This was a national survey carried out in France from May to December 1999.
A target population of 1566 community physicians (1287 general practitioners, 180 neurologists and 99 gynaecologists) was identified. The DREES (Direction de la Recherche, des Etudes, de l’Evaluation et des Statistiques) national physician registry was used to obtain the total number of physicians by speciality and by the eight administrative regions in France. On this basis, a stratified target population was set for each speciality and for each region. In an initial phase, a sample corresponding to 500% of the target population for each speciality and region was selected from an exhaustive database of practising physicians in France (TVF files) using a stratified random sampling method. This number was set in order to maximize the chances that the targeted number of physicians could be recruited from the same initial stratified sample, and in order to avoid re-sampling. These pre-selected physicians were sent documentation of the aims and methodology of the study and then contacted by telephone in the order in which they appeared on the random list and asked if they wished to participate in the study. This operation was continued until the pre-assigned quota had been achieved for each physician speciality and for each region.
For each participating physician, the following information was collected: name and address, age, gender, medical speciality and size of the community (three possible classes). These data were then compared where possible with national norms for each medical speciality using the 1995 CREDES national physician registry.
Each participating physician was requested to include the next five patients consulting for migraine who fulfilled the inclusion criteria. For inclusion into the study, patients were required to be aged 18 years or more, regularly experience headaches fulfilling IHS criteria for migraine (IHS categories 1.1 or 1.2; Headache Classification Committee of the International Headache Society), and to be seeking treatment from their physician for their headaches. Each patient could only be included once.
For each included patient, the investigator was expected to fill in a case report form (CRF) which specified the inclusion criteria, the patient's socio-demographical profile, migraine history and characteristics (disease duration, frequency of attacks, existence of aura) and any treatment given. The CRF also documented the last migraine attack using the MIGSEV questionnaire, and the duration of the attack was noted. The MIGSEV questionnaire included four items (nausea, pain intensity, disability in activities of daily living and tolerability) which could each be rated on a three- or four-point scale. The physician provided an assessment of severity (mild/moderate/serious) and of treatment response of this last attack.
At the inclusion and after 3 months, the patient was requested to complete a questionnaire in the waiting room to assess quality of life within the three previous months using the QVM (Qualité de Vie et Migraine) scale (8). The QVM is a questionnaire containing 20 items which are used to generate a global quality of life index (GI), and four specific indices relating to functional quality of life (FI), psychological quality of life index (PI), social quality of life index (SI) and medical quality of life (MI). All five indices have a 100-point range where 100 represents best and 0 poorest quality of life. The different items for the QVM and the scoring system are presented in Appendix 2.
The statistical analysis was mainly descriptive. Qualitative variables are presented as absolute numbers and modal frequencies, and compared using the χ2 test. Ordinal variables are compared with a trend test. Quantitative variables, presented as mean, S.D. and median values are compared with the Wilcoxon test, or the Kruskal–Wallis test as appropriate. To compare the distribution of the various study parameters between MIGSEV severity grades, the χ2 test, Cochrane-Armitage tendency test or Kruskall–Wallis test was used as appropriate. Concordance between measures was assessed using the MacNemar test (2 classes) or a κ coefficient (>2 classes). A probability level of <0.05 was taken as statistically significant. All data were analysed centrally using the SAS software package (version 6.12, SAS Institute, Cary, NC, USA).
Results
Of the 3100 physicians who were contacted and expressed interest in taking part in the study, 1420 actually participated. This population was made up of 1164 general practitioners (81.2%), 174 neurologists (12.1%) and 82 gynaecologists (5.7%). A comparison with national demographic data in the CREDES physician database showed the 1420 participating physicians to be generally representative of the profession, although there were small but statistically significant differences in age (43.8 years vs. 44.3 years nationally) and geographical distribution (slight over-representation of the North and West of France) as compared with national data for the general practitioners. Of the 1420 participating physicians, 36% included the target number of five patients set out in the study protocol before the end of the predetermined inclusion period. After validation of the database, exploitable case report forms were obtained for 3296 patients, and patient questionnaires for 3079.
The socio-demographic characteristics of the patients are presented in Table 1. Their mean age was 40.3 ± 11.6 years (range 18–84 years) and 82% of them were female. The majority (72.7%) of the included patients had a professional activity; these are presented in Table 1.
Socio-demographic characteristics of patients

The mean duration of the disease was 14 years (range 0.1–72 years), the patients treated by a neurologist having a longer duration of disease (17 ± 11 years) as compared with those seeking help from a general practitioner (13 ± 10 years) or a gynaecologist (12.5 ± 10 years). In almost half of the patients (48%), the frequency of attacks ranged from 1 per month and 1 per week; the overall frequency of those experiencing more than one attack per week was 20%. More than one-third of the patients (39%) usually experienced migraine with aura, and their frequency was markedly lower in those consulting neurologists (17%) as compared with GPs (42%) or gynaecologists (43%). The last migraine attack most frequently lasted between 4 and 12 h, but was even longer in 38% of patients. For 48% of patients, the last attack had not responded to treatment.
At the time of the consultation, 22% of patients reported suffering from a health problem other than migraine. The most frequently encountered pathologies were arterial hypertension (17.4% of patients), anxiety/depression (14.6%), back pain (5.8%), asthma (4.1%), elevated blood cholesterol (4.1%), arthritis (3.9%), venous insufficiency (3.4%), colopathy (3.1%) and diabetes (3.1%).
The severity of the last migraine attack was evaluated with the MIGSEV questionnaire, and classified into one of three grades. Of these attacks, 47% were rated as mild, 35% as moderate and 19% as severe. Attacks were more frequently categorized as severe in patients consulting neurologists than in those consulting general practitioners or gynaecologists (P < 0.001; χ2 test; Table 2). There was also a gender difference in the distribution of severity grades, with severe attacks accounting for 19.9% of all attacks in females, and 14.6% in males (P < 0.05). Separate analysis of the four component factors of the MIGSEV scale showed that the distribution of each was well correlated with the aggregate score (Table 3).
Distribution of migraine severity grades by medical speciality
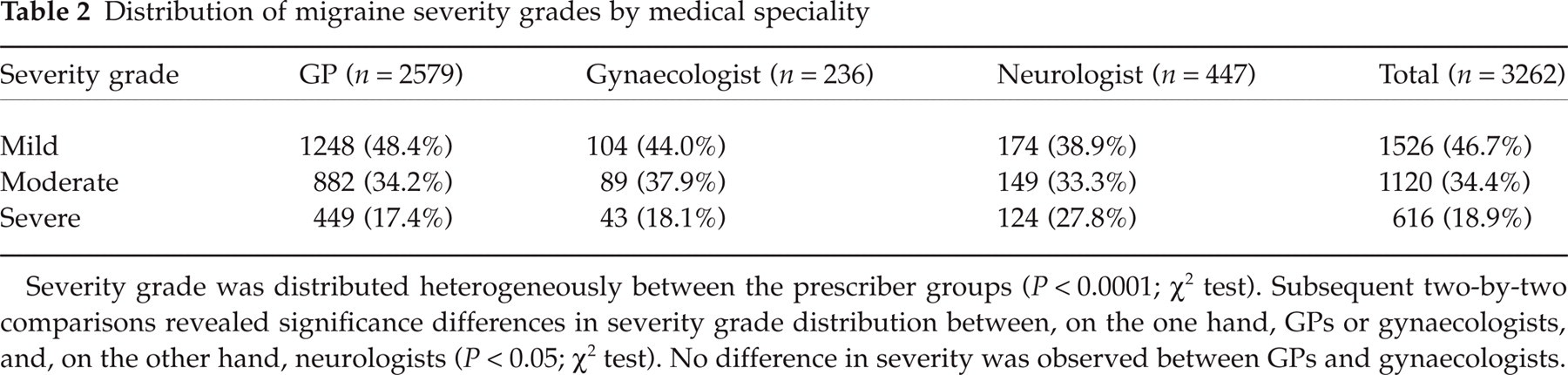
Severity grade was distributed heterogeneously between the prescriber groups (P < 0.0001; χ2 test). Subsequent two-by-two comparisons revealed significance differences in severity grade distribution between, on the one hand, GPs or gynaecologists, and, on the other hand, neurologists (P < 0.05; χ2 test). No difference in severity was observed between GPs and gynaecologists.
Distribution of component scores according to severity grade

∗The asterisks indicate that the variable was distributed heterogeneously between the three severity grades (P < 0.0001; χ2 test). Subsequent two-by-two comparisons revealed significance differences in all the variables between mild and moderate, between mild and severe, and between moderate and severe headaches (P < 0.01; χ2 test).
Moreover, when the severity of the migraine attack was determined from the patient's response to the questionnaire, there was a close relationship to the assessment made from the information supplied by the physician (Table 4). Overall, an identical severity category was assigned in 71.4% of cases. The discordant cases most frequently represented an underestimation of the severity items by the physician compared with the patient (21.8% of all cases), the remaining 6.8% representing overestimates by the physician compared with the patient. The overall coefficient of concordance (κ) was 0.62. When responses to the individual components of the scale were examined, the highest concordance was found for the nausea item, and the lowest for the pain intensity item (Table 5). The level of agreement between severity assignment from physician and patient evaluations varied according to the degree of severity, with greater agreement observed for the extremes of mild and severe (for the physicians) attacks than for attacks of moderate severity (Fig. 1).

Concordance rates between severity calculated from physician-derived and patient-derived data. For each severity grade assigned from physician-derived data (left) and from patient-derived data (right), the proportion (%) of concordant assignments between patient and physician is presented.
Concordance between severity calculated from physician-derived and patient-derived data

The percentages relate to the 2874 patients for whom a complete data set was available.
Concordance between severity calculated from physician-derived and patient-derived data expressed as kappa coefficients for each item

The relationship between the other clinical features of migraine with severity as determined with the MIGSEV scale was investigated. The length of illness was significantly longer in patients with more severe attacks, and the frequency of attacks higher (Table 6). The proportion of patients with aura was also significantly higher in patients whose last attack was rated as severe (48%) than in those rated as moderate (41%) or mild (33%). The duration of attack and its resistance to treatment was also high in those patients whose attacks were rated as severe (Table 6), the relationship of the last parameter to severity grade being particularly pronounced. For all these parameters, the distribution of the variable between the three severity grades was significantly heterogeneous (P < 0.0001).
Distribution of migraine features according to migraine severity grade

The asterisks indicate that the variable was distributed heterogeneously between the three severity grades
(∗P < 0.0001; χ2 test
∗∗P < 0.0001; Cochrane-Armitage tendency test). Subsequent two-by-two comparisons revealed significance differences in all the variables between mild and moderate, between mild and severe, and between moderate and severe headaches (P < 0.01; χ2 test;), with the exception of disease duration between mild and moderate, and of frequency of migraine between moderate and severe headaches, which were not significantly different.
The global quality of life score (GI) of the entire patient cohort was 59.3. Quality of life was somewhat poorer in patients consulting neurologists than in those consulting general practitioners, both on the global index and on the component subscales (Table 7). There was a clear relationship between the quality of life score on the QVM, and the severity of the last migraine attack measured on the MIGSEV scale, with those patients reporting more severe headaches having poorer quality of life (Fig. 2). This difference according to severity was observed for all the subscales of the QVM, and was in all cases statistically significant (QDV scores are heterogeneously distributed between the three severity grades: P < 0.01; Kruskall–Wallis test). Subsequent two-by-two comparisons identified significant differences between mild and moderate MIGSEV grades, and between moderate and severe grades.
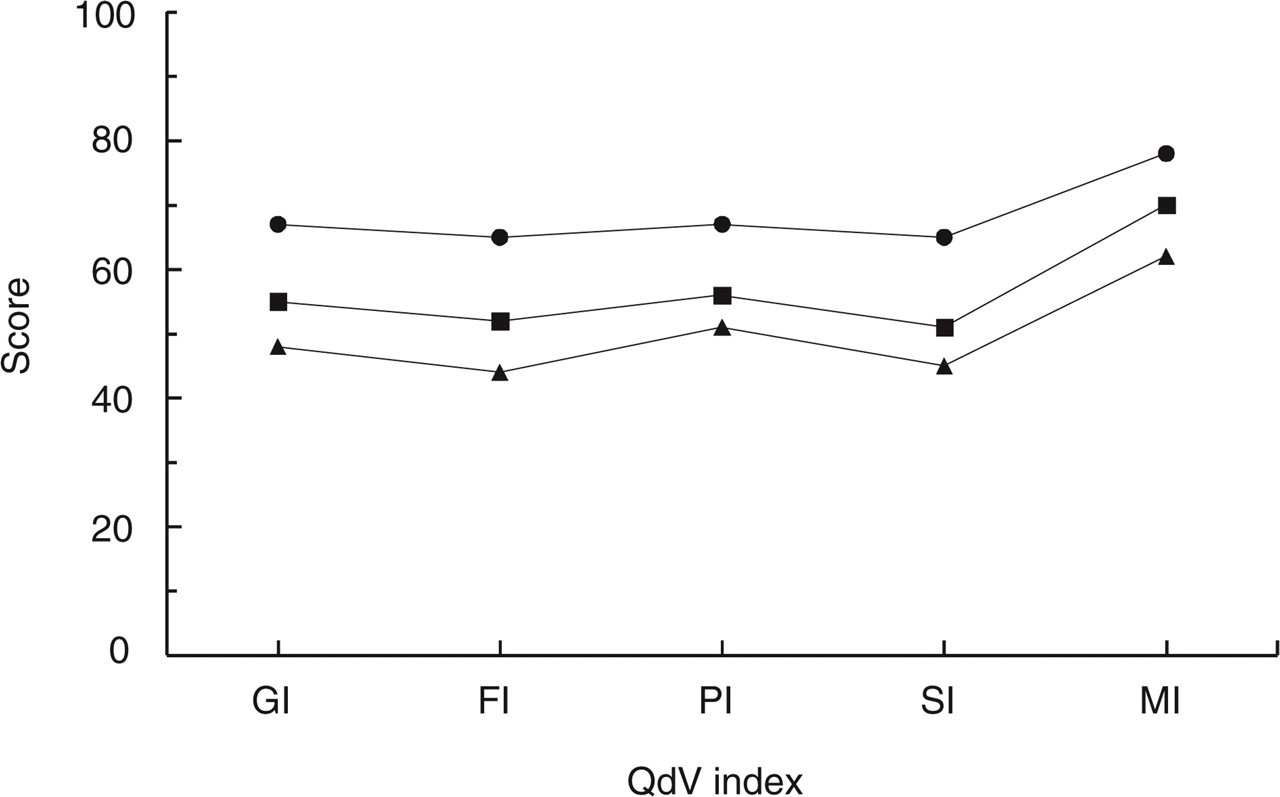
Relationship between self-assessed quality of life and migraine severity. The five items represent the global quality of life scale (GI) and the functional (FI), psychological (PI), social (SI) and medical (MI) subscales. Data are reported for QDV scores for patients reporting headaches as mild (•), moderate (▪) or severe (▴) on the MIGSEV scale. The QVM scores were heterogeneously distributed between the three severity classes (P < 0.001; Kruskall–Wallis test). Subsequent two-by-two comparisons revealed significant differences in all QVM scores between mild and moderate, between mild and severe, and between moderate and severe headaches.
Quality of life scores by medical speciality

Data are presented as mean [S.D.]. All scores were distributed heterogeneously between the three prescriber groups (P < 0.0001; χ2 test). Subsequent two-by-two comparisons revealed significance differences between general practitioners (GPs) and neurologists
(∗) or between gynaecologists and neurologists
(†) or between GPs and gynaecologists
(‡)(P < 0.01; χ2 test).
Discussion
According to a recent editorial, ‘choices about the selection and sequence of drug treatments are at the core of everyday clinical care of patients with migraine but have been largely ignored in clinical research to date’ (9). Although there is sufficient evidence that assessing severity represents a crucial prerequisite to optimize the strategies of care of migraine (2), doctors and patients do not effectively communicate about migraine severity (1) and a review of available literature reveals a surprising lack of consensual data on the assessment of this parameter. It is likely that severity is a composite notion, integrating a variety of different parameters, such as pain, nausea, emotional distress, and functional impairment. Both for clinical practice and for clinical trials, there is a need for a simple tool to measure migraine severity and help the clinician interpret symptomatology from patient self-report, and thus to decide the most appropriate treatment.
In a previous study (7), we identified a number of parameters that could be used to characterize the severity of migraine attacks, and developed a severity scale (the MIGSEV questionnaire) which uses four of these (intensity of pain, disability in daily activity, tolerability and nausea) to categorize migraine attacks as mild, moderate or severe. This scale has now been used to assess severity in a larger population of 3262 migraineurs consulting a random sample of French physicians for headache, and to investigate the relationship between severity and other aspects of migraine, including quality of life.
Although the rate of physician response in the study was only 57%, there is no reason to believe that the patients recruited into the study may be unrepresentative of French migraineurs consulting for headache in general. The demographic characteristics of the sample are consistent with data reported in surveys of the epidemiology of migraine in France (10–12). In particular, there was a large female predominance, and a median age in early middle age. In addition, the mean duration of illness and the frequency distribution of headache attacks were very similar to those reported in a recent large epidemiological survey of migraine in the French general population (12). The frequency of aura was surprisingly high in patients evaluated by general practitioners and by gynaecologists, but not in those consulting neurologists, and this may reflect difficulty of unfamiliarity with the diagnosis in non-specialists in migraine.
In our previous pilot study, a good agreement between rating of items making up the MIGSEV scale by physicians and by patients was observed. This finding was borne out in the present study, where an overall concordance in the final score of 71.4% was obtained, discordance being essentially attributable to an underestimate of severity by the physician compared with the patient. This phenomenon of underestimation by physicians has been described for other pain syndromes, including cancer pain and post-operative pain, by comparison of visual analogue scale ratings for pain intensity provided by, on the one hand, patients, and on the other hand, by physicians or nurses (13–16). This presumably reflects the difficulty that the physician has in assessing a subjective symptomatology, as well as the difficulty for the patient in communicating symptom severity. This discordance between patient and physician implies that the MIGSEV scale should be used primarily as a patient autoevaluation questionnaire, as subjective self-report by patients is well recognized as a valid method of data collection for the assessment of pain symptoms. However, the κ coefficient obtained for the concordance between physician and patient ratings lies between 0.6 and 0.8, which is considered to indicate substantial agreement between two measures (17). This implies that the MIGSEV scale could also be useful for collecting data from physicians, which is relevant as it is the physician's assessment of severity that is important in orienting treatment choices. Moreover, the use of the questionnaire may foster a creative dialogue between patient and physician.
The distribution of severity grades in the sample was skewed towards low severity, with 19% of patients presenting severe attacks, 34% moderate attacks and 47% mild attacks. It is difficult to transpose this finding to the general migraineur population, as patients with more severe migraine attacks are more likely to seek medical help, and therefore may be over-represented in our sample. On average, neurologists tended to see more severe cases than general practitioners, with the proportion of patients consulting neurologists reporting severe attacks (27.8%) being higher than in those who consult general practitioners (17.4%). A general population study will be required to determine the true distribution of severity grades in French migraineurs.
Severe migraine attacks were reported more frequently by females, by patients with a longer disease history, in those with more frequent attacks and in those reporting aura. Moreover, for individual attacks, there was a positive correlation between MIGSEV grade and headache duration and resistance to treatment. The finding of a close correlation between the MIGSEV score and quality of life measured with the QVM is also important, with patients with more severe migraine attacks reporting more deteriorated quality of life. This suggests that the MIGSEV questionnaire measures items that are relevant to the patient's subjective perception of well-being and quality of life. This correlation was observed in all dimensions of the QVM.
It has been suggested that the choice of treatment strategies for migraine should take into account disease severity (2). Indeed, recent American guidelines have proposed that a measure of disability with the MIDAS scale be used to stratify migraine treatment according to severity (18). In this context, the MIGSEV scale could be useful in identifying those patients with severe attacks who could then benefit from the most appropriate treatment.
In conclusion, this large prospective survey has evaluated migraine severity with the MIGSEV scale in patients consulting for headache in France. Severe attacks were reported in around one-fifth of the sample. Migraine severity was associated with frequent, long-lasting and treatment-resistant attacks, and with poor quality of life. The MIGSEV questionnaire is proposed as a simple measure of severity for the diagnosis and management of migraineurs, suitable for use both by physicians and patients.