
Abstract
Aim
To identify clinical predictors of cranial autonomic symptoms (CAS) in chronic migraine (CM) and explore the role of cranial parasympathetic outflow.
Methods
We conducted a cross-sectional study using audit data from first consultation letters of 333 patients diagnosed with CM at King's College Hospital London (January 2015 to September 2019). All met the International Classification of Headache Disorders, 3rd edition (ICHD-3) criteria for CM. Predictors included sex, aura, age, pain quality and headache laterality. A generalized linear regression model with a Poisson distribution was used to analyze CAS count predictors.
Results
Of 333 cases, 85.2% were female and 54% reported aura. CAS were present in 75.1%, with 19.8% experiencing unilateral symptoms. CAS count was positively skewed (mode = 0; median = 2). Female sex (β = 0.244; p = 0.036), aura (β = 0.328; p < 0.001) and unilateral CAS (β = 0.317; p < 0.001) were significant positive predictors. Pain quality and age were not significant.
Conclusions
Female sex and aura are linked to increased CAS in CM. Enhanced trigeminal-autonomic reflex activation may represent a protective cerebrovascular mechanism. CAS may contribute to maintaining perfusion or modifying nociceptive input during attacks. Targeted therapies modulating this pathway could benefit females with aura and frequent CAS.
This is a visual representation of the abstract.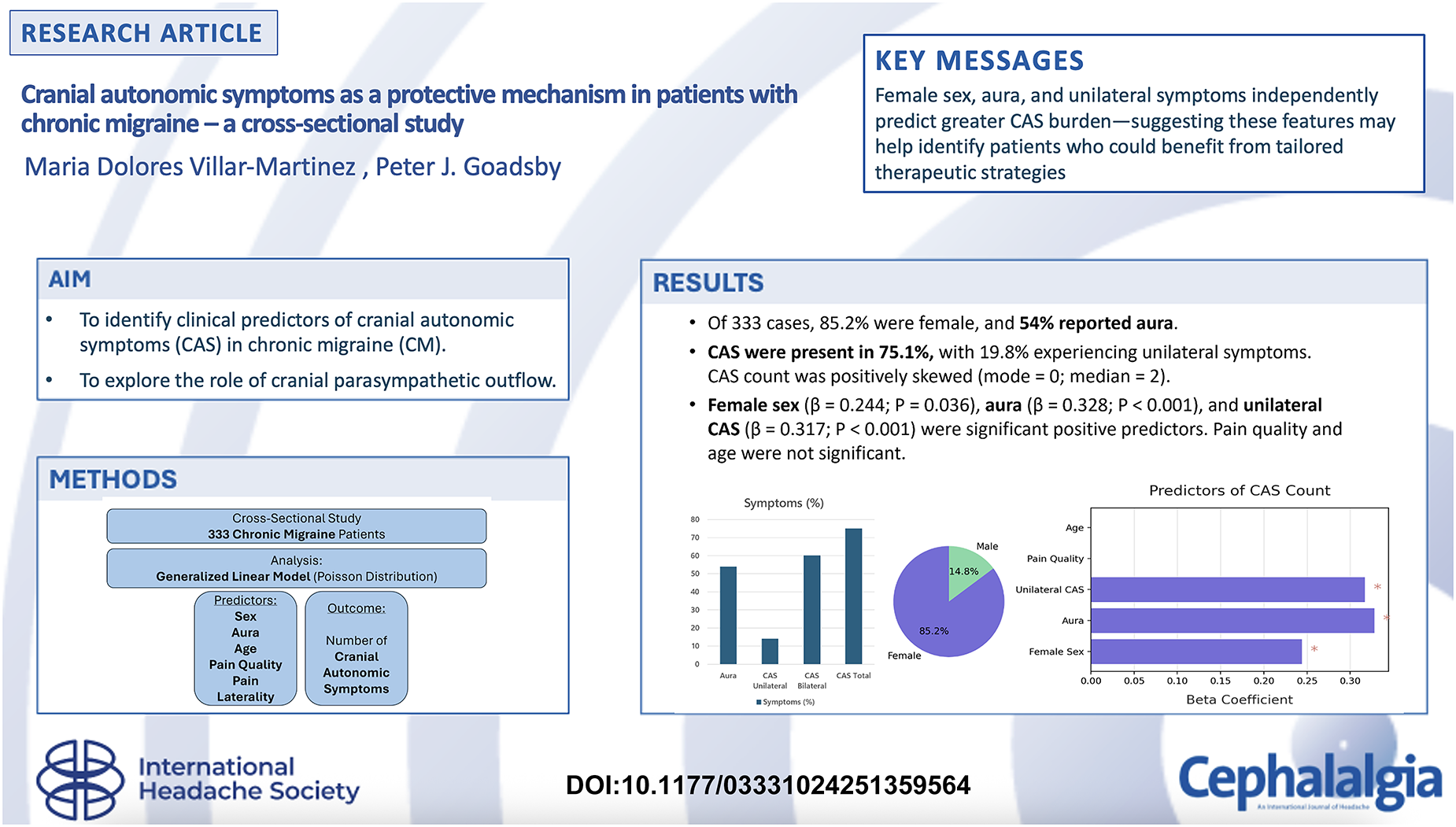
Introduction
The anatomical relationship between the cranial nerves, craniofacial vessels and the central nervous system is implicated in neural influences on the cerebral circulation. 1 In patients with headache disorders, the interaction between the cranial autonomic system and ipsilateral pain is mediated by the trigeminal-autonomic reflex, and is prominent in trigeminal autonomic cephalalgias. 2 Three main structures of the central nervous system, and their connections, are involved in the trigeminal-autonomic reflex. In the brainstem, the trigeminocervical complex, situated in the caudal medulla and upper cervical spinal cord, is connected with the superior salivatory nucleus (SSN) of the facial nerve, situated in the pons, and also projects to, and receives input from, several hypothalamic areas.3,4 The SSN seems to play an important role as an integrating center of autonomic and sensory information from the cranial nerves, at the same time as receiving descending modulatory inputs from the hypothalamic nuclei, cortical and limbic areas. 5 From the SSN, preganglionic parasympathetic fibers join another branch of the facial nerve, the nervus intermedius, and then project through the greater petrosal nerve. These fibers, in conjunction with sympathetic preganglionic fibers, form the nerve of the pterygoid canal. The parasympathetic fibers then synapse in the sphenopalatine ganglion. Postganglionic fibers innervate lacrimal and nasal glands as well as dural vessels. 6 The intricate anatomical interplay between cranial nerves, craniofacial vasculature and central autonomic centers underpins the trigeminal-autonomic reflex, for which activation is important to trigeminal autonomic cephalalgias and contributes to cranial autonomic symptoms (CAS) in migraineurs through its modulatory effects on pain and cerebrovascular dynamics.
Parasympathetic hyperactivity ipsilateral to the symptomatic side can be evoked with known pharmacological migraine triggers such as nitroglycerin, a nitric oxide donor in patients with primary headaches, 7 reinforcing the involvement of autonomic pathways in migraine pathophysiology. The autonomic system of migraineurs may exhibit baseline dysregulation. 8 Compared with individuals without migraine, migraineurs often show altered functions in the sympathetic and parasympathetic tone, and different responses to external stimuli also during the interictal period. 9 This dysregulation of the sympathetic and parasympathetic pathways may contribute to mechanisms aimed at modulating the nociceptive input. The appearance of CAS might not reflect only a pathological byproduct of trigeminal activation but could rather represent a homeostatic or protective mechanism.
The main aim of the present study was to characterize the clinical features associated with a higher burden of CAS in patients with chronic migraine (CM). We hypothesized that CAS may be more common in patients with aura, potentially reflecting the activity of pathways involved in cerebral vasodilation in the absence of increased metabolic demand, consisting with the concept of neural influence on the cerebral circulation. 10
Methods
We performed a cross-sectional study based on audit data from the detailed letters of the first consultation and clinical interview with patients diagnosed with CM, as defined by the third edition of the International Classification Headache Disorders (ICHD-3), seen by neurology headache specialists at a tertiary headache centre at King's College Hospital London, from January 2015 to September 2019. Patients with strictly unilateral headache and CAS had been unresponsive to either oral or intramuscular indomethacin test. Cranial autonomic symptoms could be occasional, necessarily appearing in every headache attack.
We selected the total number of CAS as a dependent variable. The presence of CAS elicited during the headache anamnesis include those in ICHD-3; namely, lacrimation, conjunctival injection, nasal congestion, rhinorrhoea, facial flushing or pallor, eyelid oedema and ptosis. 11 In addition, other CAS such as aural fullness, eye grittiness and throat swelling, which have been described in migraineurs were included. 12 Given that these parameters are a count result, we used a generalized linear regression model with Poisson and log link function. Although CAS are mediated by both parasympathetic and sympathetic pathways, we considered the total CAS burden as a clinical measure of cranial autonomic involvement, with sympathetic features interpreted as resulting from parasympathetic-driven inhibitory interaction with the sympathetic chain. 13 As predictors, we selected biological sex, the presence of any type of current or past aura, age at clinic interview, quality of pain (pulsatile, not pulsatile) and unilaterality of the headache. Recall and observer biases were minimized by following a semi-structured first clinical interview that was subsequently transcribed into a clinical letter. Confirmation bias was also reduced by having a different clinician, often not the one who conducted the original assessment, review the clinical letters and extract the data. Patients with missing data were removed from the analysis.
CAS are count data. A generalized linear regression model with a Poisson distribution and log link function was used to analyze CAS data predictors (R, version 4.3.2 (R Foundation, Vienna, Austria) and RStudio 2024.12.0 (Posit, Boston, MA, USA)).
Results
Three hundred and thirty-three cases were used for the analysis. Fifteen were excluded because of missing data. Female patients accounted for 85.2% of cases. The quality of pain was exclusively throbbing in 42.1% of cases, non-throbbing in 20.8% and of variable quality, including throbbing, in the remaining 37.1%. The pain was unilateral in 23.2%, bilateral in 46.7% and either unilateral or bilateral in 30.1% of our cohort. Fifty-four percent of cases reported some type of aura, and 48.4% had at least two types of aura. The most common type of aura was visual in 83.7%, followed by sensory in 55.9%, dysphasic in 10.7% brainstem in 8.7% and motor in 14.6%. CAS were reported by 75.1% of patients with migraine and were lateralized in 19.8%. The number of CAS followed a positive skewed distribution (skewness 1.038) (Figure 1), with mode = 0, median = 2 of total number of CAS, and the most commonly described were lacrimation, nasal congestion and aural fullness (Figure 2). Mean (SD) age was 43.11 (15.06) years. The model was well-fitted (likelihood ratio χ2 = 41.04, df = 6, p < 0.001).
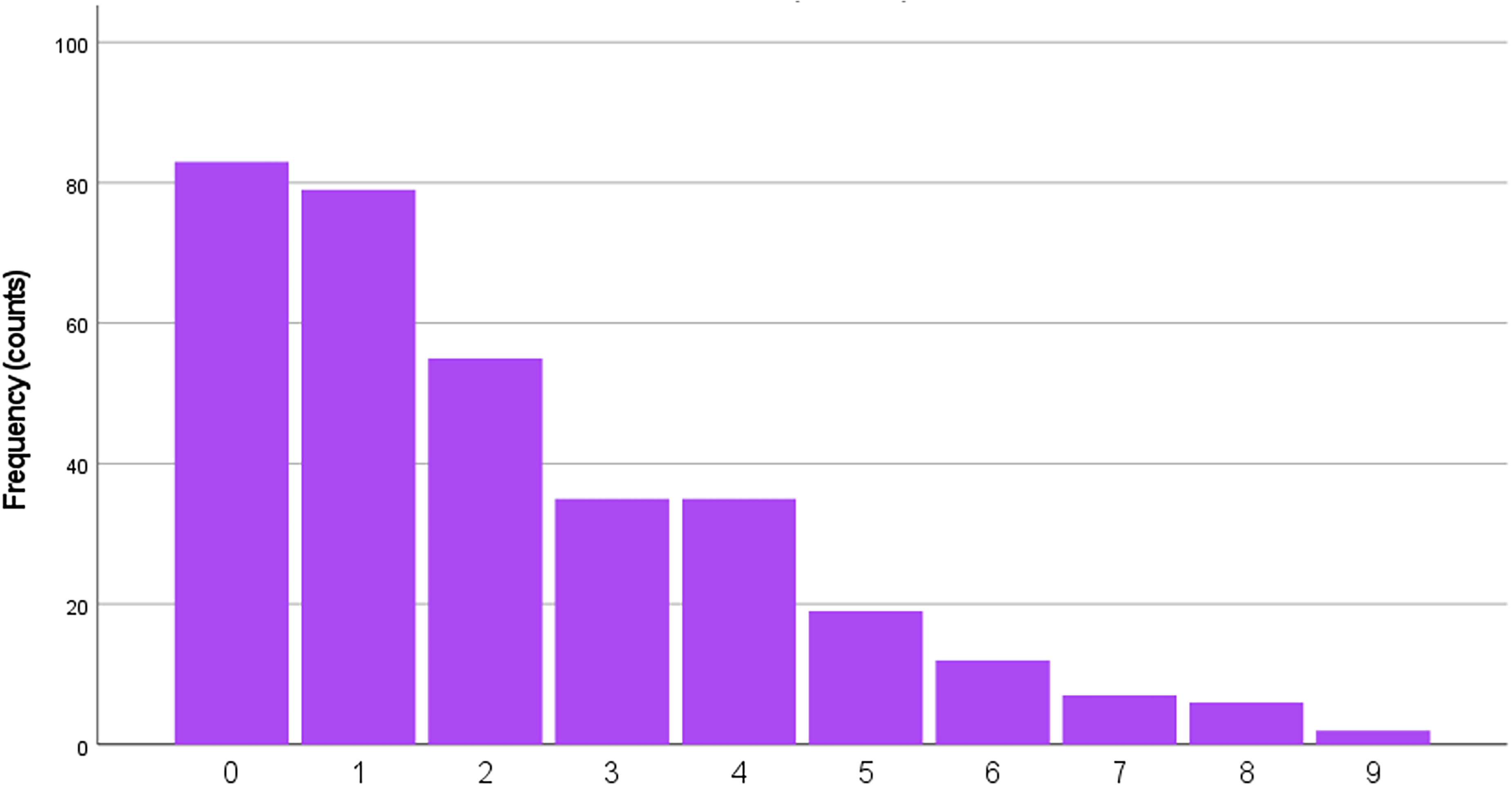
Total number of cranial autonomic symptoms reported by patients with chronic migraine.

Cranial autonomic symptoms (CAS) reported by chronic migraine patients.
Positive predictors of the model included sex (β = 0.244 for females, 95% CI = 0.015–0.472, p = 0.036), presence of aura (β = 0.328, 95% CI = 0.174–0.481, p < 0.001) and unilaterality of CAS (β = 0.317, 95% CI = 0.144–0.491, p < 0.001). Quality of pain and age at clinic appointment were not significant predictors of the total number of CAS.
Discussion
Pre-clinical models have shown that increased cerebral vasoconstriction could potentiate a trigeminal reflex response, mediated mainly by calcitonin gene-related peptide, to restore normal vascular diameter. 14 Although a higher burden of CAS may reflect a more genetically susceptible migraine phenotype, 15 it is also plausible that greater CAS expression could act as a protective or modulatory mechanism. Our study indicates that female patients and those experiencing any type of aura are independently associated with a higher likelihood of experiencing CAS in individuals with CM. These findings highlight the important role of the cranial parasympathetic outflow pathway and its potential protective effects in the cerebrovascular system, possibly through enhanced activation during the aura phase. An increased activation of the trigeminal-autonomic reflex in these specific migraine phenotypes suggests a complex relationship between cortical and brainstem processes. Cortical changes occurring during the aura phase could be interpreted and modulated in brainstem regions involved in the trigeminal-autonomic reflex pathways. The data offer insights into the underlying normal physiological pathways that are entrained when the oligemic phase of aura threatens the brain.
In comparison with other cohorts, 16 our percentage of patients presenting migraine with aura was higher, and aural fullness was the third most reported CAS (Figure 2). Aural fullness was the most prevalent CAS, in almost one-third of paediatric patients studied by Gelfand et al. 17 Interestingly, in children, sex and the presence of aura were not associated with an increased likelihood of having CAS, which were present in 62% of participants in a paediatric cohort of 125 patients (mean (SD); range: 13.1 (3.4); 4–17). The second most prevalent symptom was either facial flushing or sweating and lacrimation, in one-fourth of the sample.
Laterality of the symptoms as a predictor could reflect a more localized and intense activation of the trigeminocervical complex and its connections with parasympathetic pathways. This focused activity might amplify the cascade of autonomic responses in the affected side. Unilateral CAS were reported in 26.9% out of 841 participants with migraine according to questionnaire studies. The most frequently reported symptoms were ocular, and, among them, the most frequently reported was lacrimation (40.3%), followed by conjunctival injection (25.2%) and either miosis or ptosis (19.5%). 18 This prevalence was similar in another study, at 32%, but when strict unilaterality was not a criteria, the prevalence of CAS in migraineurs almost tripled, at 73.1%, and the side of headache was not influential in the appearance of CAS. 19 Both studies were conducted under previous ICHD classification criteria.
Previous studies have reported a positive prediction of triptan responsiveness in patients with unilateral CAS. 20 Triptan ineffectiveness might account for chronification of migraine, as in our cohort, the percentage of lateralized CAS was lower. Patients with CAS have been reported to have a more severe and disabling migraine attack. 16 Therefore, females with aura may benefit from therapies that also target the cranial autonomic pathway. This study's external validity is limited by its single-center design. As a cross-sectional audit using a semi-structured clinical interview, it cannot establish causality, and variability in clinician documentation may influence findings.
Conclusions
Females with migraine and any type of aura are more likely to experience CAS during a migraine attack. The cranial parasympathetic outflow pathway is considered to play a role in cerebrovascular regulation, potentially contributing to the higher number of dysautonomic manifestations observed in our cohort. However, its exact involvement in the mechanisms underlying CAS and its interaction with aura remain to be fully understood. The data suggests this group of patients could benefit more from therapies targeting the cranial autonomic pathway.
Clinical implications
CAS were reported in 75.1% of CM patients, with significant predictors including female sex, aura presence and unilateral symptoms.
The cranial parasympathetic pathway may play a cerebrovascular protective role, especially in patients with aura.
Therapeutic strategies targeting this pathway could improve outcomes in specific migraine phenotypes.
Footnotes
Acknowledgements
We sincerely thank Karthik Nagaraj for his exceptional dedication and hard work. We also extend our heartfelt gratitude to the nurses, Steffy and Fiona, for their outstanding support and professionalism throughout.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical statement
This study was conducted as a clinical audit and did not require ethical approval. All data were collected and analyzed in accordance with institutional guidelines for service evaluation.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.