
Abstract
Background
There is limited evidence about visceral autonomic symptoms in the different phases of migraine attack. We evaluated the prevalence of these symptoms in migraineurs before, during, and after headache attacks. In addition, the association between migraine characteristics and visceral autonomic symptoms was investigated.
Methods
A total of 605 participants who met the entry criteria were enrolled prospectively in this cross-sectional study. Participants were 18–60 years old and met the ICHD-3 criteria for migraine with or without aura. Information on the migraine symptoms was gathered from all participants in face-to-face interviews. A structured questionnaire was used to evaluate the related symptoms before, during, and after attacks. Migraine features of frequency, duration, and severity were also assessed.
Results
Considering all phases, the most commonly present visceral symptom was nausea (52.9%). About half of participants reported at least one visceral symptom before the onset of attacks. While, during and after attacks, 71% and 36% of participants reported such characteristics, respectively. Notably, the migraine headache in participants with visceral symptoms was longer during attacks compared to participants without them (24.4 ± 29.6 vs. 16.8 ± 19.8; P = 0.008). Additionally, subjects with positive visceral symptoms experienced more severe migraine attacks than participants without symptoms for both the premonitory (8 ± 1.7 vs. 7.6 ± 1.8; P = 0.02) and during-attack (8.01 ± 1.7 vs. 7.09 ± 1.9; P = 0.001) phases.
Conclusion
This study demonstrated that visceral symptoms were common in migraine sufferers not only during attacks but also in the premonitory and postdrome phases. Positive visceral symptoms were also associated with more burdensome headache attacks. Therefore, recognizing the phenotypic presentation of associated symptoms of migraine, especially during the pre-attack phase, could aid in early implementation of optimal management.
Introduction
Migraine is a chronic neurovascular disorder characterized by frequent and recurrent multiphase attacks of disruptive pain (1). Globally, over 1 billion people experience migraine, making it one of the most prevalent neurological disorders, especially among females (2). The peak prevalence of migraine is during the reproductive years; thus, it imposes a substantial burden on individuals and society (3). The most recent report of the Global Burden of Disease Survey ranked migraine first as a cause of disability of those under 50 years of age (4). Migraine is not isolated simply to head pain, its consequences extend far beyond the headache attack to a range of symptoms that exacerbate its debilitating nature (5,6).
The pain and symptoms of migraine have been attributed to involvement of the autonomic nervous system; however, the pathophysiology of migraine and its activation of the autonomic nervous system remain poorly understood (7–10). Cranial autonomic symptoms (CAS) are not limited to trigeminal autonomic cephalgia (TAC), but occur in migraines as well, affecting 27% to 73% of migraineurs (11–15). Because abnormalities of the trigeminovascular system and autonomic disturbances previously have been reported in migraineurs, it is not unreasonable to expect CAS among migraineurs (16,17). Typical CAS symptoms include conjunctival injection, lacrimation, nasal congestion, rhinorrhea, eyelid edema, facial sweating, miosis, and ptosis (14,18). In addition to CAS, visceral autonomic symptoms also are known to occur with migraines (19). However, unlike CAS, visceral symptoms such as nausea, vomiting, diarrhea, bloating, fullness in the stomach, frequent defecation or urination have not been rigorously studied (20–22).
Importantly, the prevalence of reported symptoms differs for every patient and can vary from attack to attack for an individual or in the different phases of the headache (23–26). A migraine attack can consist of up to four phases: premonitory, aura, headache, and postdrome (27). Although the headache phase is generally the most recognizable and debilitating, for some migraineurs, the other phases can be prolonged and even more disabling than the headache (27–29).
Little information has been available thus far on the phenotypic presentation of both cranial and visceral symptoms in the same person during all phases of a migraine (26,30–32). The frequency of migraine-related symptoms also depends on factors that have not been well defined (33,34), although several reports have suggested that some of the non-headache symptoms are associated with poor outcomes and response to treatment (35,36). These facts warrant efforts toward the development of a detailed symptom profile among migraineurs which can contribute to optimal diagnostic and therapeutic success. In this study, our hypothesis is that visceral symptoms are also common among migraine patients and the prevalence of these symptoms is not limited to the attack phase. There may also be an association between the onset of these symptoms and the characteristics of the migraine headache. Therefore, in an attempt to address this hypothesis, we evaluated migraineurs complaints for symptoms occurring before, during, and after headache attacks to determine: (I) the prevalence of different symptoms in migraineurs; (II) their occurrence in relation to an attack phase; and (III) the association between migraine characteristics and visceral autonomic symptoms.
Methods and materials
Patient characteristics
This was a cross-sectional study that prospectively recruited migraine patients who presented at the headache clinic of Sina Hospital from 2018 to 2019. The study was approved by the ethical committee of Tehran University of Medical Sciences. Participation was voluntary and written informed consent was obtained from each subject before initiating data collection. The protocol was developed in accordance with the Helsinki Declaration. Inclusion criteria were 1) willing to participate in the study; 2) diagnosis of migraine according to ICHD-3 criteria, and 3) age between 18–60 years. Exclusion criteria were 1) accompanied other headaches, and 2) having any gastrointestinal disorders.
Clinical evaluation
Information on the migraine-related symptoms was gathered from all participants by means of face-to-face interviews using a structured questionnaire. The first part of the questionnaire addressed demographic factors (age, gender), type of migraine based on neurologist diagnosis according to the ICHD3 classifications, and migraine characteristics. The evaluated migraine features consisted of frequency, duration, and severity of the migraine attacks (based on the numeric rating scale; NRS-11). Participants were asked about their family history of migraine, total duration of their illness, and any relation of migraine attacks with menstruation. All acute and prophylactic migraine medications, prescribed or non-prescribed, that had been used by the participants were recorded. They were also questioned about the average number of acute medications taken per week over the past three months.
The second part of the questionnaire addressed related symptoms before, during, and after attacks as well as the presence of an aura before initiation or during the migraine attacks. Information was also collected regarding any history of liver and kidney disease, thyroid abnormalities, diabetes, hypertension and cardiovascular disease. Possible premonitory and postdrome symptoms were as follows: stomach fullness, bloating, nausea, vomiting, eructing, constipation, diarrhea, frequent defecation, and frequent urination. The symptoms accompanying a headache attack were identified as: tearing (unilateral/bilateral), nose congestion (unilateral/bilateral), rhinorrhea (unilateral bilateral), eye redness (unilateral/bilateral), drooping eyelid (unilateral/bilateral), eyelid edema (unilateral/bilateral), nausea, vomiting, stomach fullness, bloating, eructing, constipation, diarrhea, frequent defecation, and frequent urination. In all phases, the participants were able to add symptoms not included in this list and respond to the questions as well. The following details were asked of participants:
The number of years since the onset of comorbid symptoms. An estimate of the percentage of headache attacks that are accompanied by symptoms. Rating of headache intensity (0 to 10) at times when the symptoms are accompanied by a headache attack.
Addressing potential biases
Because the information collection method was direct interview, the missing data was reduced as much as possible. However, in the case of missing data, we used the listwise deletion. This is the most frequently used method in handling missing data, and thus has become the default option for analysis in most statistical software packages including SPSS. In listwise deletion a case is dropped from an analysis because it has a missing value in at least one of the specified variables. So the analysis was only run on cases which have a complete set of data.
To minimize the bias caused by misdiagnosis of migraine, other types of headache with similar clinical picture were ruled out by the neurologist based on the ICHD-3 diagnostic criteria.
Statistical analysis
The data were analyzed using SPSS software, release 19 (SPSS; IBM; USA). Categorical variables were reported by frequency (%) and quantitative variables were described using mean (standard deviation; SD). Comparisons between the groups with and without visceral symptoms were made using a chi-square test for the categorical data and the independent t-test for the continuous variables. Statistical significance was defined as a p-value <0.05.
Results
Figure 1 illustrates the recruiting procedure of participants. A total of 615 migraine patients were screened for the current study. Five patients were not willing to participate and five patients also reported gastrointestinal disorders unrelated to the migraine attacks. Finally, 605 patients who met the entry criteria were enrolled in the current study. Table 1 provides the demographic and baseline data of the participants. The population was 82.7% female and 17.3% male with a mean age of 38.2 ± 11.2 years. A total of 75.9% of participants reported a family history of migraine. The mean duration of illness was 13 ± 9.7 years. Of the participants, 62% were affected by episodic migraine and 38% by chronic migraine. The majority of participants complained of accompanying symptoms during all migraine attacks. The mean intensity of attacks (0 to 10) at the time when the symptoms were accompanied by headache was reported to be 8.09 ± 1.7. On average for the study population who had been experiencing migraine, it had been 11.2 ± 9.3 years since the onset of autonomic symptoms.

Flowchart of participants enrollment.
Baseline characteristics of participants.
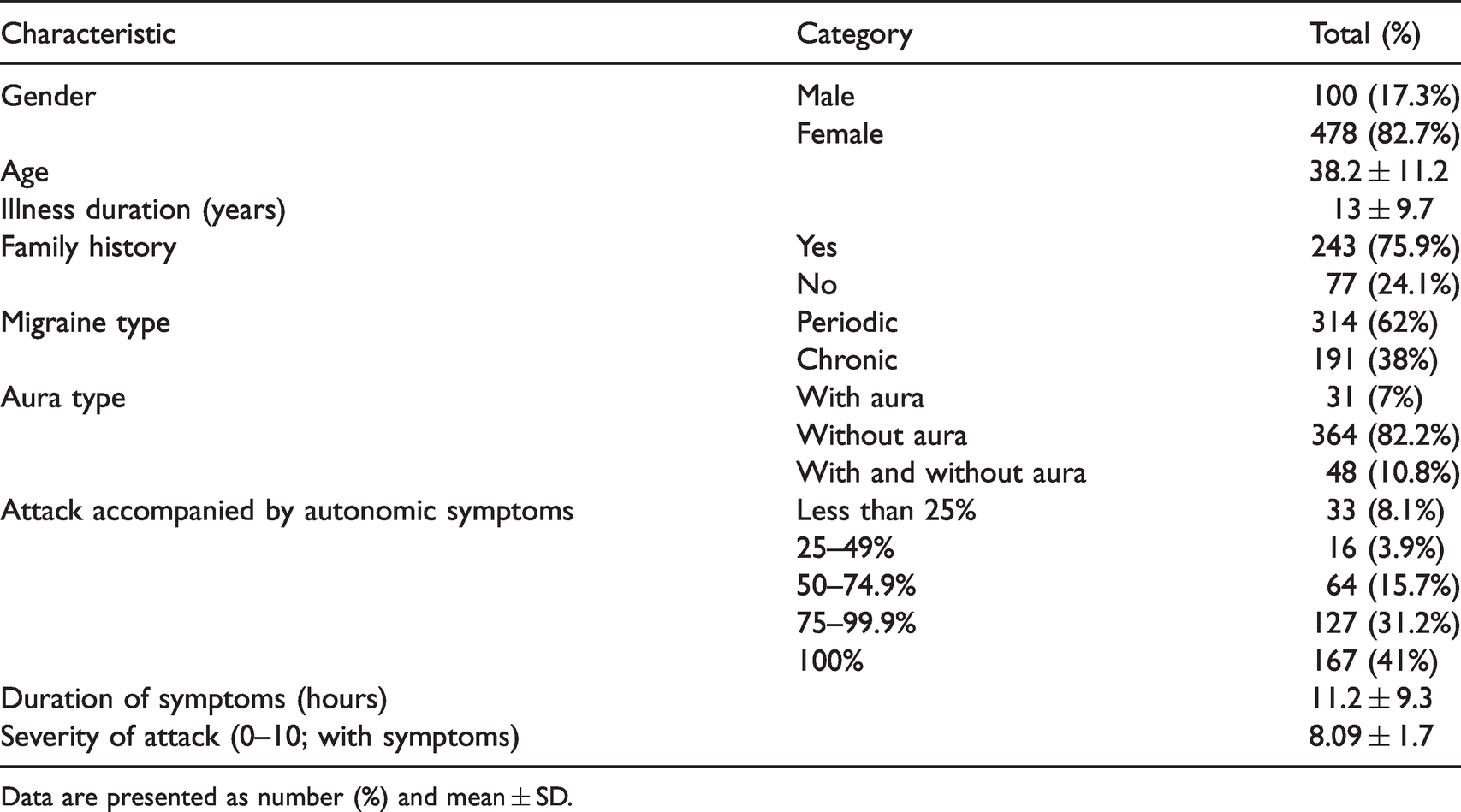
Data are presented as number (%) and mean ± SD.
The prevalence of visceral symptoms before, during, and after attacks are depicted in Figure 1. Considering all phases, the most commonly present visceral symptom was nausea (52.9%) and the least common was frequent defecation (1.2%). Based on the participant reports, visceral symptoms occurred most commonly during headache attacks (3.1% to 52.9% for different visceral symptoms), rather than before or after headache attacks. However, the prevalence of several symptoms during two or all three phases of an attack should not be neglected. The frequency of cranial symptoms is presented in Figure 2. The two most frequently reported cranial symptoms were eye redness (about 30%) followed by tearing (about 26%). Regarding laterality, drooping eyelid (13.9%), rhinorrhea (7.4%), nose congestion (11.7%), and tearing (15.4%) were more frequently reported as unilateral, whereas eyelid edema and eye redness were primarily reported as being bilateral (5% and 16.4%, respectively).

Frequencies of visceral symptoms before, during, and after attacks.
For each phase of the attacks, participants were categorized based on the accompanying visceral symptoms. Fifty-two percent of participants reported at least one visceral symptom before the onset of a headache. During and after attacks, 71% and 36% of participants reported such characteristics, respectively. Participants who reported at least one visceral symptom were placed into the “presence” group and those who experienced no symptoms were included in the “absence” group. The negative and positive visceral symptoms groups were compared during all phases of attacks in terms of aura presence, pulsatile nature, pain location, prophylactic medication usage, and comorbidities. Table 2 shows that, in all phases of an attack, the majority of participants in both groups suffered from migraines without aura. Bilateral pain tended to be more prevalent among participants with visceral symptoms during the pre-attack phase.
Characteristics of visceral autonomic symptoms by phase of attack.

Data presented as total (%).
**Chi-square test.
Table 3 shows the effect of visceral autonomic symptoms on migraine characteristics across the three phases of attack. There were significant differences between participants with and without visceral symptoms regarding migraine features and this difference was more pronounced during attacks. In participants who reported at least one visceral symptom, the duration of migraine attacks was significantly longer than in participants without visceral symptoms during attacks (24.4 ± 29.6 vs. 16.8 ± 19.8; p = 0.008). This significant difference was not observed in the pre-attack or postdrome phases. Additionally, participants with positive visceral symptoms experienced significantly more severe migraine attacks than participants without symptoms. This significant difference held true for both the premonitory (8 ± 1.7 vs. 7.6 ± 1.8; p = 0.02) and during-attack (8.01 ± 1.7 vs. 7.09 ± 1.9; p = 0.001) phases. However, we found no significant differences between groups in terms of the frequency of attacks or painkillers usage/week across any phase of migraine attack. Interestingly, in all phases, more than 70% of participants with visceral symptoms reported menses-related attacks. This figure was significantly higher than in the negative visceral symptoms group (Figure 2).
Migraine characteristics with or without visceral autonomic symptoms.

Data presented as total (%) and mean ± SD.
*Independent t-test.
**Chi-square test.
To determine whether there is a tendency for co-occuring of visceral symptoms, we evaluated the correlations within-phases across symptoms. The results of the analysis showed that there was a positive correlation between the symptoms of nausea and vomiting in all three phases. Due to the common co-occurrence of these two symptoms, this correlation is somewhat reasonable and predictable. But there was no correlation between the other symptoms and they seem to have occurred independently.
We also evaluate the frequency of endorsement of various numbers of visceral symptoms in patients. It turns out the majority of patients in the current study had one visceral symptom across all phases. To be precise, during attack phase, 42%, 34.4%, 14%, 5%, 3.4%, 0.5%, 0.5% and 0.2% of patients reported 1 to 8 visceral symptoms, respectively. This superiority in the number of patients with one visceral symptom was even more evident in the premonitory and postdrome phases and the number of patients who had only one visceral symptom was almost double that of subjects who had two symptoms. Therefore, visceral positive patients do not necessarily have multiple visceral symptoms which are almost in line with the independent occurring nature of symptoms in our study.
Regarding the within-person consistency across phases, the majority of the visceral positive patients showed symptoms only during one of the phases, and fewer subjects showed symptoms during two or even less during 3 phases. The symptom in which the highest intra-individual consistency was observed during all phases was constipation (23% of subjects) while, in case of frequent defecation, there was not even one patient involved across all 3 phases.
Discussion
Unlike research on cranial autonomic symptoms, research evaluating the visceral autonomic symptoms before, during, and after headache attacks is scant. Also, previous studies have mostly focused on the prevalence of gastrointestinal symptoms among migraine sufferers. The results of our study showed that visceral symptoms occurred at least once during headache attacks among 71% of participants and by 52% and 36% of participants before and after attacks, respectively (Figure 3).
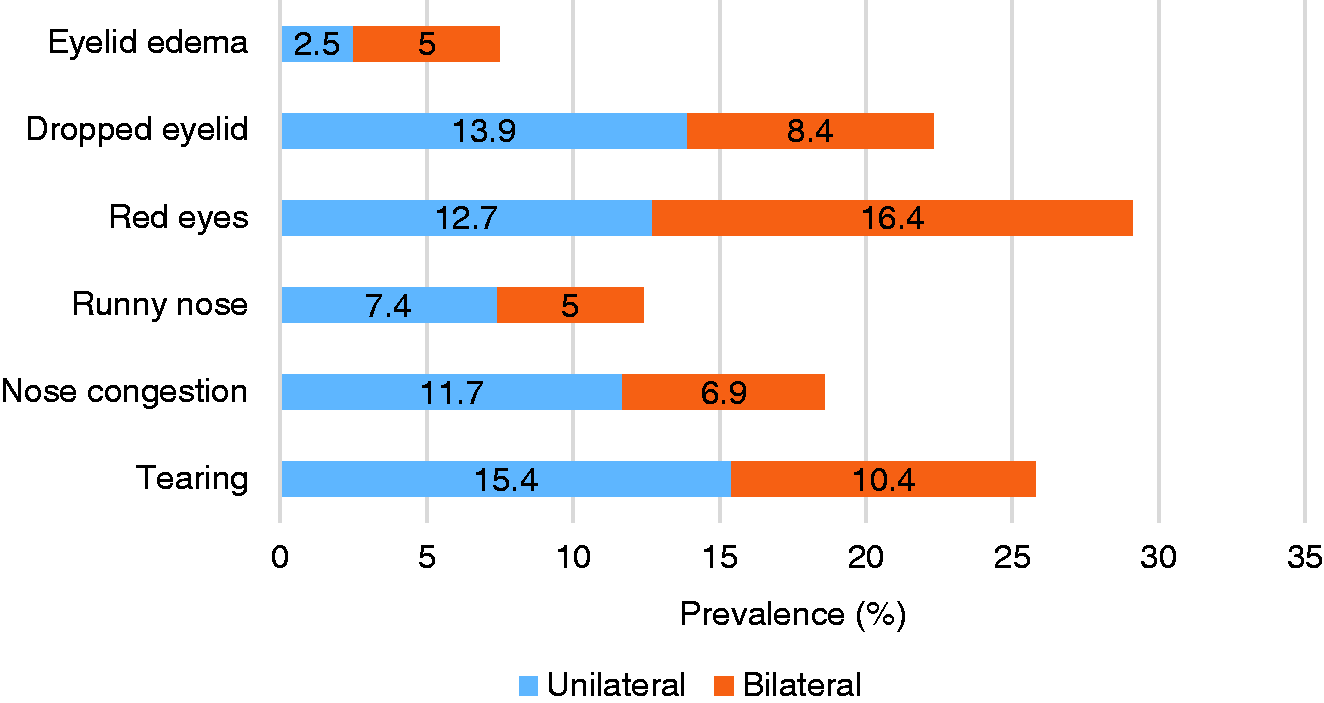
Prevalence of cranial autonomic symptoms based on laterality.
Nausea and vomiting were the most common visceral symptoms reported by the study population. These results are consistent with previous reports indicating a high prevalence of gastrointestinal symptoms, including nausea, vomiting, bloating, constipation, and diarrhea, among migraineurs (19–22). Although these studies have also reported a high prevalence of gastrointestinal symptoms in migraineurs, the occurrence of these symptoms, as in the present study, was not related to the phases of the migraine attack.
In our study, about half of participants reported at least one visceral symptom before the onset of an attack. The examination of the premonitory phase was advantageous and could have clinical implications, since it is the earliest clinical change during a migraine attack. The results of previous studies suggest that early treatment is critical to successful treatment and a long delay can cause the window of opportunity for preventing the migraine to be lost (37,38). Evidence from previous studies have shown that, in selected migraineurs, premonitory symptoms can be considered as reliable predictors of an impending attack and treatment with medication during the premonitory phase has the potential to be beneficial (37,39). In this regard, accurate recognition of the symptoms associated with the premonitory phase can allow early implementation of the best therapeutic approach.
From a clinical point of view, we found that headache attacks in migraineurs with visceral symptoms differed in duration and severity from that of those without visceral symptoms. In fact, the migraine headache was more severe and of longer duration in participants with visceral symptoms than in participants without such symptoms. This finding is compatible with a previous report that linked the associated symptoms with severe migraine attacks.
Kelman et al. (40) investigated the relationship between migraine pain and associated symptoms and indicated that there is a significant correlation between headache intensity and nausea and vomiting. The results of the Head-HUNT study, a large-scale, population-based study indicated that the association between headache and gastrointestinal complaints increased substantially with an increase in headache frequency. The odds ratio for nausea increased more than six-fold for migraineurs with headaches on more than four days/month compared with those without headache (41). However, we did not find significant differences between participants with and without visceral symptoms regarding the frequency of attacks across any phase of a migraine.
A wide range of symptoms and neurological disturbances have been reported by migraineurs over all phases of attack. Disruption of the sensory, cognitive, and autonomic functions could occur suggesting the involvement of multiple neural networks (42). In recent decades, the peripheral and central pathways and relevant neuropeptides, neurotransmitters, and receptors involved have received more attention (43,44). Many of the symptoms associated with migraine, such as nausea, vomiting, and thirst, as well as CAS such as lacrimation, nasal congestion, and rhinorrhea are representative of changes in autonomic function in the central nervous system (45). It has been proposed that alterations in sympathetic and parasympathetic tone can occur from the premonitory phase through to the postdrome phase (46).
The frequency of CAS during attacks in our study population ranged from 7.5% to 29.1%. The two most frequently reported cranial symptoms were eye redness and tearing. Lai et al. (18) compared the characteristics of CAS in migraines with those in cluster headaches in a cross-sectional study. They found that, in patients with migraine, 56% had at least one CAS. In a Japanese study aimed at evaluating the clinical characteristics of CAS in patients with migraine, 42.4% had at least one CAS (47). The lower prevalence of CAS in our study was likely because the present data are based on participant recall of a typical attack while, in some previous studies, the data gathered was prospectively linked to a specific attack. The results indicated that the prevalence of CAS was associated with the participant characteristics, including illness history, attack frequency, severity, and duration. More severe attacks could result in more symptoms being reported by participants. Therefore, differences in migraine characteristics could be part of the difference observed in the prevalence of CAS between studies.
It has been suggested that CAS result from activation of the trigeminal-autonomic reflex, as demonstrated by an increase in calcitonin gene-related peptides and vasoactive intestinal peptides during attacks (48). This reflex pathway comprises functional connections between the trigeminal nerve and facial parasympathetic outflow which exit the brainstem via the seventh cranial nerve (CN VII) (49). The activation of the trigeminal autonomic reflex contributes to the stimulation of periaqueductal gray and dorsal raphe nuclei and a few fibers directly activate the ipsilateral and contralateral superior salivatory nucleus. Efferent fibers from the superior salivatory nucleus are involved in CAS ipsilateral to pain (48).
We found that bilateral pain tended to be more prevalent among visceral positive participants. However, there was a significant difference between groups only during the pre-attack phase. More than 70% of participants who had visceral symptoms reported menses-related attacks, before, during, and after migraine attacks. The association of menstruation with the presence of autonomic symptoms has not been well clarified in migraineurs. However, it has been proposed that ovarian hormones affect the autonomic nervous system (ANS) (50). In our study, menses-related attacks were more common in participants with visceral autonomic symptoms, which supports the hypothesis that menstruation-related hormonal factors could be triggering the trigeminal autonomic reflex pathway (50).
Because most previous studies have focused on cranial symptoms, the major strength of the current study has been an evaluation of the visceral symptoms during all phases of an attack and detailed analysis of the clinical characterization of these autonomic symptoms in migraine. However, this study has several potential limitations. First, our findings cannot be directly extrapolated to the general migraine population, as participants were recruited from tertiary referral centers and were selected according to specific inclusion/exclusion criteria. Therefore, interpretation and generalization of our findings should be done with caution. Second, there is the possibility that some migraine attacks may have been stopped or relieved by medication before the complete phenotype could be expressed. This may have caused a reduction in the frequency of some symptoms. Another methodological issue of this study was the risk of recall bias because all information was gathered interictally. Furthermore, we did not separately evaluate and compare visceral symptoms during different phases of attacks in periodic and chronic migraine, as well as accompanying medication overuse headache (MOH). Even though we had a relatively good number of participants, the presence of a larger sample size could provide higher statistical power for comparing the frequency of visceral symptoms in different subtypes of migraine.
Conclusion
Although a large body of evidence exists about cranial autonomic symptoms among migraineurs, little information is available on the phenotypic profile of visceral symptoms during all phases of migraine attacks. This study demonstrates that visceral symptoms are common in migraineurs not only during attacks but also in the premonitory and postdrome phases. In the current study, about half of the participants reported visceral autonomic symptoms before the onset of the attacks, which may have clinical implications.
Identification of the symptoms associated with the pre-attack phase could aid in early implementation of optimal management. Among our study population, migraine headaches were more severe and lasted longer in participants with visceral symptoms than in those without them. However, the question that remains to be determined is whether or not the pathophysiological mechanisms and therapeutic responses in migraineurs with visceral symptoms differ. We suggest further prospective clinical studies for the deeper pathophysiological understanding of visceral autonomic symptoms among migraineurs.
Article Highlights
About half of participants reported at least one visceral symptom before the onset of attacks Visceral symptoms occurred most commonly during the headache attack Migraine headache was more severe and longer in participants with visceral symptoms than in participants without them
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.