
Abstract
Objective
This study aimed to explore how childhood trauma (CT) affects the psychological, clinical and demographic characteristics of migraine patients.
Methods
A sample of subjects with chronic migraine with medication overuse (CM + MO) (n = 192) and episodic migraine (EM) (n = 84) was assessed for CT, psychological profiles (via DSM-5-based clinical interviews and self-report questionnaires) and migraine characteristics.
Results
CT was detected in 40% of the total population, being more prevalent in the CM + MO subgroup (41%) versus the EM subgroup (36%) (p = 0.006). The CT group showed a higher prevalence of personality disorders (PDs), particularly Cluster B (12% vs. 4%) and Cluster C (60% vs. 34%), as well as psychopathologies (94% vs. 75%); p = 0.001). The CT group also exhibited greater anxiety, depression, alexithymia and exposure to current stressful life events (p = 0.001). CT participants were more frequently women, had an earlier migraine onset and a higher intake of acute medications. In the multivariate analysis, only Cluster C PDs (i.e., obsessive–compulsive PD), psychopathologies (i.e., anxiety disorders), stressful life events, difficulty identifying feelings (alexithymia), and female sex remained significant.
Conclusions
CT is associated with psychological comorbidities, an earlier onset of migraine and a higher intake of acute medications, leading to a more complex migraine phenotype
This is a visual representation of the abstract.
Introduction
There is growing interest in the identification of the possible factors involved in migraine development, particularly in its complicated forms, including chronic migraine (CM) and medication overuse headache (MOH). Specifically, CM can be defined by the presence of at least 15 monthly headache days over the previous three months, with at least eight days per month presenting migraine features. 1 When associated with medication overuse, it is classified as CM + MOH and represents the most severe end of the migraine spectrum.1 The biopsychosocial model emphasizes the complex interplay between biological, psychological and psychosocial factors, which influence each other. 2 According to this perspective, the variability in migraine manifestations, encompassing aspects such as severity, duration and impact, arises not only from the individual's biological attributes, but also from the interplay between their psychological well-being and the social environment. 3 Hence, these factors may significantly influence disease perception and response.
In this frame, the existing association between CM + MO and psychopathologies such as anxiety, depression, personality disorders (PDs), dependency-like behaviors and alexithymic traits is well known.4–11 As a matter of fact, the presence of psychopathologies in migraine subjects can increase the frequency of attacks and contribute to the chronification of the disease. Therefore, identifying and treating comorbid mental disorders in these individuals is crucial to prevent the disease from becoming chronic.
However, in addition to commonly investigated psychological vulnerabilities,4–11 there are other factors commonly implicated in chronic pain syndromes that require a comprehensive understanding. Among these, childhood traumas (CTs) is a key area of interest. CT encompasses all adversities experienced during early life and occur before the age of 18 years, including experienced or witnessed violence, abuse or neglect; mental health diagnosis in family members; or instability in the household. 12 These adverse experiences during childhood are not only able to impact health and well-being during that period, but also elevate the likelihood of encountering mental and physical health issues in adulthood.13–15
For example, CTs were shown to increase the risk of subsequent physical disease, particularly chronic pain, which is associated with a higher likelihood of persisting throughout life.16–18 In the field of migraine, CTs have been shown to be associated with increased frequency, severity and chronicity of migraines, representing a risk factor for disability and progression toward more severe forms of disease.19–22
Unfortunately, only a limited number of studies have fully explored this topic. We recently found that the presence of CTs predicted CM + MO 23 and the negative outcome of detoxification therapy 24 or preventive treatment with monoclonal antibodies targeting calcitonin gene-related peptide. 25
However, it remains unclear whether the presence of CTs delineates a specific psychological and clinical profile among migraine sufferers, potentially identifying a distinct subgroup regardless of migraine subtype or severity. Although previous studies have explored the relationship between CTs and pathological personality traits,13–15 most have focused on heterogeneous populations, often overlooking the unique characteristics of individuals with migraine. 23 Emerging evidence suggests that CT might also contribute to the onset and to the persistence of pediatric headache disorders, including migraine, by affecting pain sensitivity and stress reactivity early during development. 21 Although the number of studies on this subject is not yet large, it is possible, for example, to highlight a study by Fuh et al., 21 who studied the presence of maltreatment in childhood in a population of adolescents between the ages of 13 and 15 years. They found that maltreatment is a significant predictor of migraine onset already in this age group and how, likewise, the number of maltreatment episodes was positively correlated with a worse clinical picture in terms of migraine. Furthermore, there is a notable lack of research integrating comprehensive psychological variables–such as PDs, anxiety, depression and alexithymia, with migraine-specific clinical factors such as attack intensity, frequency and treatment response. 26 To conclude, few studies have examined the combined impact of CTs and current stressors on the psychological and clinical profiles of migraine sufferers, leaving a gap in understanding how early life adversities may interact with present-day environmental factors to shape migraine outcomes. 27
To address these gaps, the present study aimed to investigate whether the occurrence of CTs delineates a distinct psychological and clinical profile in a large sample of subjects with either CM + MO or episodic migraine (EM). The choice to include both the CM + MO and the EM groups is dictated by the added value that chronicity provides compared to the episodic form. Indeed, this comparison makes it possible to clarify whether CTs are associated with the presence of migraine in general or whether they represent a specific risk factor for the development of more severe and chronic forms, thus increasing the clinical relevance of the findings.
Our working hypothesis was that migraine patients with CTs would exhibit more complex psychological and clinical profiles compared to those who did not. Specifically, concerning the psychological features, we expected a higher prevalence of personality, mood and anxiety disorders, alexithymia and increased exposure to current stressful life events. Regarding clinical features, we hypothesized that these patients would exhibit more severe migraine manifestations, such as earlier onset, higher attack frequency and increased use of acute medications, indicating a more burdensome and treatment-resistant migraine phenotype.
Methods
Participants
The present cross-sectional study was conducted at the Headache Science Centre and Neurorehabilitation Unit (a tertiary referral center) of the Mondino Foundation in Pavia, Italy. We enrolled consecutive subjects diagnosed with either CM + MO or EM. All participants were screened for a history of CTs using a validated self-report questionnaire23,28 and underwent a thorough evaluation of their psychological and clinical characteristics. PDs were treated as the primary outcome, given the well-established interaction between environmental experiences, personality disorders development, and pain chronicity.29,30 Other psychological vulnerabilities (i.e., mood and anxiety disorders, stressful life events, alexithymia and dependence levels) and clinical characteristics were considered secondary outcomes.
The study was approved by the local Ethics Committee (San Matteo Hospital, Pavia, Italy) and written informed consent was obtained from all participants. Recruitment began in March 2019 and was completed in July 2023. EM participants were enrolled during outpatient visits at the headache clinics, while CM + MO during inpatient detoxification programs.
Participants with CM + MO
Inclusion criteria for participants with CM + MO were: (a) age between 18 and 65 years and (b) diagnosis of CM and MO according to International Classification of Headache Disorders, 3rd edition (ICHD-3) criteria. 31 Exclusion criteria included: (a) dementia; (b) psychosis; and (c) intellectual disability.
EM participants
Inclusion criteria for participants with EM were: (a) age between 18 and 65 years; (b) diagnosis of migraine with or without aura according to ICHD-3 criteria 31 ; and (c) migraine duration of more than 10 years. Exclusion criteria included: (a) history of MO or other chronic headaches (ICHD-3); (b) dementia; (c) psychosis; and (d) intellectual disability.
Inclusion/exclusion criteria were selected to ensure diagnostic clarity and comparability between groups. EM participants were required to have a migraine history >10 years to ensure a stable episodic profile and avoid recent chronification. Participants with dementia, psychosis or intellectual disability were excluded to ensure reliable participation in interviews and self-report measures.
Procedures and materials
A neurologist conducted each consultation, diagnosing headache type, collected socio-demographic data, migraine history and information on the use of medications and/or other substances. Participants completed self-report questionnaires and were evaluated for psychopathologies through clinical interviews.
For the detection of CTs, we used a shorter version of the Childhood Trauma Questionnaire (CTQ),23,28 previously validated in a migraine cohort. 23 This comprises 13 items covering five trauma domains: emotional abuse, emotional neglect, physical abuse, physical neglect and sexual abuse. For each item, participants first indicated whether the trauma had occurred; if endorsed, they were then asked to rate its impact on their quality of life using a five-point Likert scale (mild, moderate, important, serious or very serious).
Participants were classified as having experienced childhood trauma (CT group) if they reported at least one trauma rated as “important” or higher. This threshold was chosen to ensure that only subjectively significant experiences were considered, enhancing both the clinical relevance and interpretability of findings. Although each trauma type was considered for descriptive purposes, no cumulative CT score was calculated, and CT exposure was analyzed as a binary variable (CT vs. without CT (wCT)) for all statistical comparisons.
The CTQ has Cronbach's α = 0.79–0.94 and test–retest reliability r = 0.88,28,32,33 thus demonstrating strong reliability and validity indices.
Psychological characteristics
The psychological evaluation was performed by an experienced psychologist (SB) using the Structured Clinical Interview for DSM-5, Clinical Version (SCID-5-CV) 34 to assess PDs, mood and anxiety disturbances. Interview questions corresponded to each DSM-5 criterion, rated as either present or absent. PDs were categorized into Cluster A (paranoid, schizoid and schizotypal), Cluster B (antisocial, borderline, histrionic and narcissistic) and Cluster C (avoidant, borderline and dependent) PDs. Anxiety disorders included specific phobias, social anxiety disorder and generalized anxiety disorder, as well as panic disorder and agoraphobia. Mood disorders encompassed bipolar disorder, cyclothymia, major depressive disorder, disruptive mood dysregulation disorder, persistent depressive disorder and premenstrual dysphoric disorder. Psychopathologies were considered present if either an anxiety or mood disorder was diagnosed.
Stressful life-events were assessed using a questionnaire from Paykel et al., 35 as previously adapted to the Italian language, 23 listing 58 potential events (e.g., moving, divorce, job loss, etc.). Participants indicated which events had occurred in the past 10 years and rated their impact on a five-point Likert scale (mild to very serious). We recorded the total number of stressful events, their subjective impact, and specifically noted events rated as having an impact of at least “important”. This scale has demonstrated good content and predictive validity and reported test–retest reliability ranges from r = 0.60 to 0.83. 35
Alexithymic traits were measured using the Italian version of the 20-item Toronto Alexithymia Scale (TAS-20). 36 Factor 1 assessed the ability to identify feelings; Factor 2 addressed concrete thinking; and Factor 3 measured the ability to express emotion and fantasy (daydreaming). Scores obtained above the cut-off of 60 indicate a clinically relevant presence of alexithymia. 36 The Italian TAS-20 has Cronbach's α ≈ 0.81 and test–retest reliability r = 0.77.37,38
The Italian version of the Hospital Anxiety and Depression Scale (HADS) 39 was used to assess anxiety and depression symptoms, comprising 14 items (seven each for depression and anxiety) rated on a four-point (0–3) Likert scale. Scores obtained above the cut-off of 11 on either the anxiety or depression subscales indicate a clinically relevant presence of anxiety or depression. The HADS has Cronbach's α ≈ 0.82–0.83 and well-established construct validity. 40
Dependence on migraine medications was evaluated using the Leeds Dependence Questionnaire (LDQ), 41 a 10-item scale evaluating psychological components of dependence. Items are rated on a 0-3 Likert scale, with a total score ranging from 0 to 30. Although no formal cut-off exists, scores of above 21 are typically interpreted as indicating severe psychological dependence. 42 In our analysis, we used the total LDQ score, as a continuous variable, without applying a categorical threshold. The LDQ has Cronbach's α ≈ 0.91–0.94 and high one-week test–retest reliability (r = 0.95), with convergent validity supported by strong correlation with the Severity of Dependence Scale (r = 0.86) 43
Clinical and demographic characteristics
These were collected during the initial neurological consultation, including socio-demographic information (e.g.,age, sex), migraine history (e.g., age at migraine onset, age at CM and MO onset) and monthly migraine days. Medication use was assessed through a structured clinical interview and verified using participants’ headache diaries. We recorded both the number of days per month and the number of doses per month of acute medication intake over the previous three months, in line with ICHD-3 criteria. 1
Primary and secondary outcome measures
The primary outcome was the prevalence of PDs as assessed via SCID-5-CV. Secondary outcomes included other psychological vulnerabilities (mood and anxiety disorders, stressful life events, alexithymia and dependence levels) and clinical-demographic characteristics.
Statistical analysis
Participants were subdivided into two groups: with CTs (CT) and without CT (wCT) on CTQ responses. The sample size calculation was based on the primary outcome: with alpha = 0.05, power = 0.8 and effect size = 0.1, the required sample was 48 participants per group (CT and wCT), totaling 96 subjects.
Data are presented as the mean ± SD for continuous data and as n/% for categorical data. Differences between CT and wCT groups were assessed using chi-squared tests for categorical variables and one-way analysis of variance for continuous variables.
Univariate and multivariate logistic regression (enter method) were performed to further evaluate the association between CTs and participants’ characteristics. Variables significant at univariate analysis (p ≤ 0.05) were entered into the multivariate models. HADS scores were used descriptively; primary analyses were based on data from the SCID-5-CV clinical interview. A significant threshold of 0.05 was applied. SPSS software was used for all analyses. In particular, two logistic regression models were conducted: in the first model, clustered PDs were considered as covariates; in the second, specific PDs were included. The rationale for carrying out these two separate models was to explore the impact of PDs treated globally as Clusters, as well as the specific value of the specific PD. At the same time, in these two models, we considered first grouped psychopathologies, as well as each disorder separately. In both cases, because of the strong associations existing between variables that were statistically significant in the previous analyses, we included in the logistic regression models only those variables that we considered as more representative of the investigated construct.
Results
Participant population
In total, 276 participants were enrolled in the study, 226 females (82%) and 50 males (18%), with a mean ± SD age of 45.2 ± 11.4 years and average migraine onset at 15.4 ± 7.8 years. Participants reported an average of 17.6 ± 10.2 migraine days per month and monthly intake of 26.1 ± 22.7 acute medication doses. One-hundred ninety-two participants were diagnosed with CM + MO (mean ± SD age: 47.4 ± 10.9 years), 84 with EM (mean ± SD age: 40.0 ± 11.1 years)
Based on CTQ responses, 40% (n = 109) were classified as CT and 60% (n = 167) as wCT. Between the CT participants, 72% of them had a diagnosis of CM + MO (n = 78 of 109 participants with CT), whereas 28% had a diagnosis of EM (n = 31 of 109 participants with CT). Trauma types included physical trauma (35%, n = 97), emotional trauma (56%, n = 154) and sexual abuse (5%, n = 13). Among participants classified as CT, 50% (n = 54) reported multiple types of traumas, indicating a substantial proportion of individuals exposed to more than one form of early adversity. To further explore the perceived severity of childhood traumas, we analyzed their distribution across the full sample (Table 1). Almost one-third of participants (28%) reported at least one trauma rated as “important”, which served as the minimum threshold for CT classification. Smaller proportions of participants reported more severe experiences: 13% for “serious” and 8% for “very serious” traumas.
Distribution of participants and trauma events by severity level (CTQ responses).

Note. CTQ = childhood trauma questionnaire.
Comparison of psychological characteristics in CT and wCT groups
PD profiles assessed via SCID-5-CV showed higher prevalence of PDs in the CT group compared to wCT, particularly Cluster B and Cluster C PDs, specifically borderline, avoidant and obsessive–compulsive PDs. CT participants also demonstrated higher prevalence of psychopathologies, anxiety and mood disorders compared to wCT. No other significant differences emerged from the clinical interview (Table 2).
Comparison between subjects with CT and wCT for psychological characteristics as assessed via the clinical interview. Data are expressed as percentages, with corresponding p-values.

Note: CT = childhood trauma; wCT = without childhood trauma. Statistically significant values are indicated in bold.
Self-report questionnaires revealed a higher prevalence of stressful life events with at least an important impact in the CT group than in the wCT. TAS-20 results showed higher Factor 1 scores in CT participants compared to the wCT group, indicating greater difficulty identifying feelings. HADS scores indicated higher anxiety and depression symptoms in CT participants compared to wCT ones. Dependence levels, assessed via LDQ, were also higher in the CT group with respect to the wCT one (Table 3).
Comparison between subjects with CT and wCT for psychological characteristics as assessed via self-report questionnaire (mean ± SD for continuous variables, percentages for prevalence rates) and corresponding p-values.
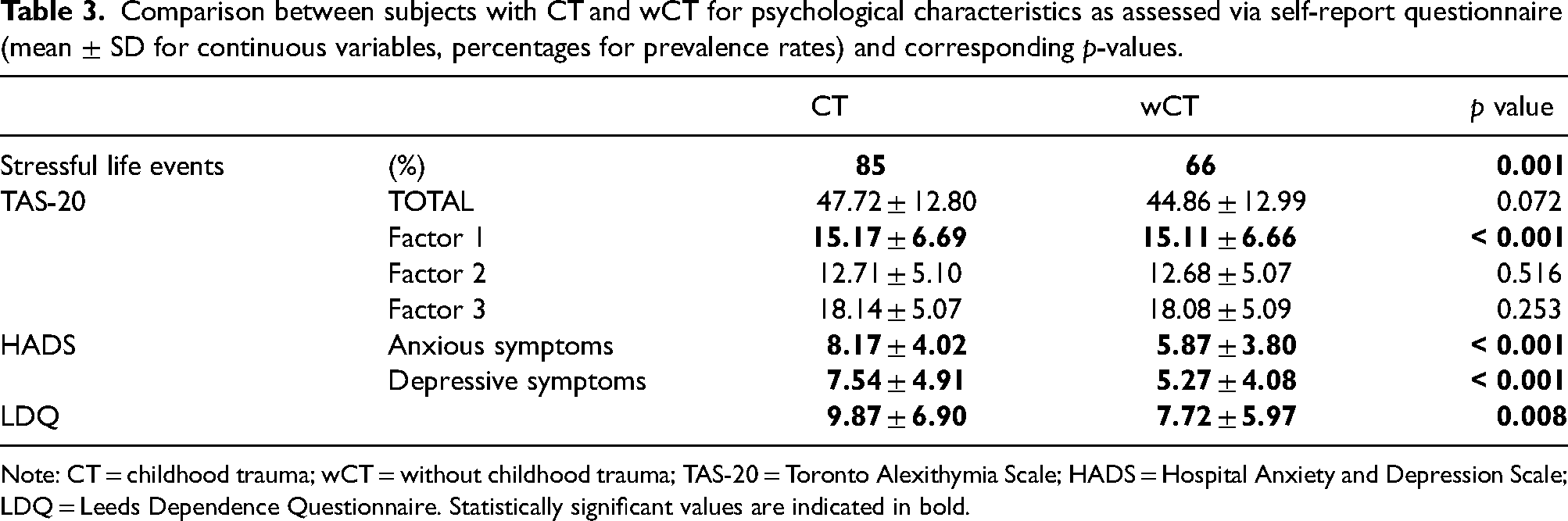
Note: CT = childhood trauma; wCT = without childhood trauma; TAS-20 = Toronto Alexithymia Scale; HADS = Hospital Anxiety and Depression Scale; LDQ = Leeds Dependence Questionnaire. Statistically significant values are indicated in bold.
Comparison of clinical and demographic characteristics in CT and wCT groups
When comparing demographic and clinical features between these two groups, we observed a higher prevalence of females, younger age at migraine onset and higher number of doses of acute medication per month in CT participants compared to those wCT. No other difference resulted between the two groups (Table 4).
Comparison between subjects CT and wCT for clinical and demographic characteristics (mean ± SD for continuous variables, percentages for prevalence rates) and corresponding p-values.

Note: CT = childhood trauma; wCT = without childhood trauma; CM = chronic migraine; MO = medication overuse. Statistically significant values are indicated in bold.
Factors associated to the presence of CTs
In the first multivariate analysis (Table 5) considering clustered PDs (i.e., Cluster B and Cluster C) as covariate, the factors that emerged as associated with CTs were: presence of Cluster C PDs, presence of psychopathologies, presence of at least important current stressful life events, high score at the Factor 1 subscale of TAS-20 and female sex. This logistic regression model was statistically significant, χ 2 = 49.45, df = 8, p < 0.001 and it explained 24.5% (Nagelkerke R2) of the variance of CT and correctly classified 69.5% of cases.
First model of multivariate analysis–Clustered PDs as covariate.

Note: CT = childhood trauma; wCT = without childhood trauma; PDs = personality disorders; Cluster B = antisocial, borderline, histrionic, narcissistic PDs; Cluster C = avoidant, dependent, obsessive–compulsive PDs; TAS-20 = Toronto Alexithymia Scale; LDQ = Leeds Dependence Questionnaire; OR = odds ratio; CI = confidence interval. Values in bold indicate statistically significant results in the multivariate logistic regression analysis, i.e., p-values < 0.05.
In the second multivariate analysis (Table 6) that considered specific PDs (i.e., borderline disorder and obsessive–compulsive disorder) as covariate, the factors that emerged as associated with CTs were: presence of obsessive–compulsive PD, presence of anxiety disorders, presence of at least important current stressful life events and female sex. This logistic regression model was statistically significant, χ 2 = 57.16, df = 9, p < 0.001 and it explained 27.8% (Nagelkerke R2) of the variance of CT and correctly classified 70.4% of cases.
Second multivariate analysis model, with specific PD as covariate.
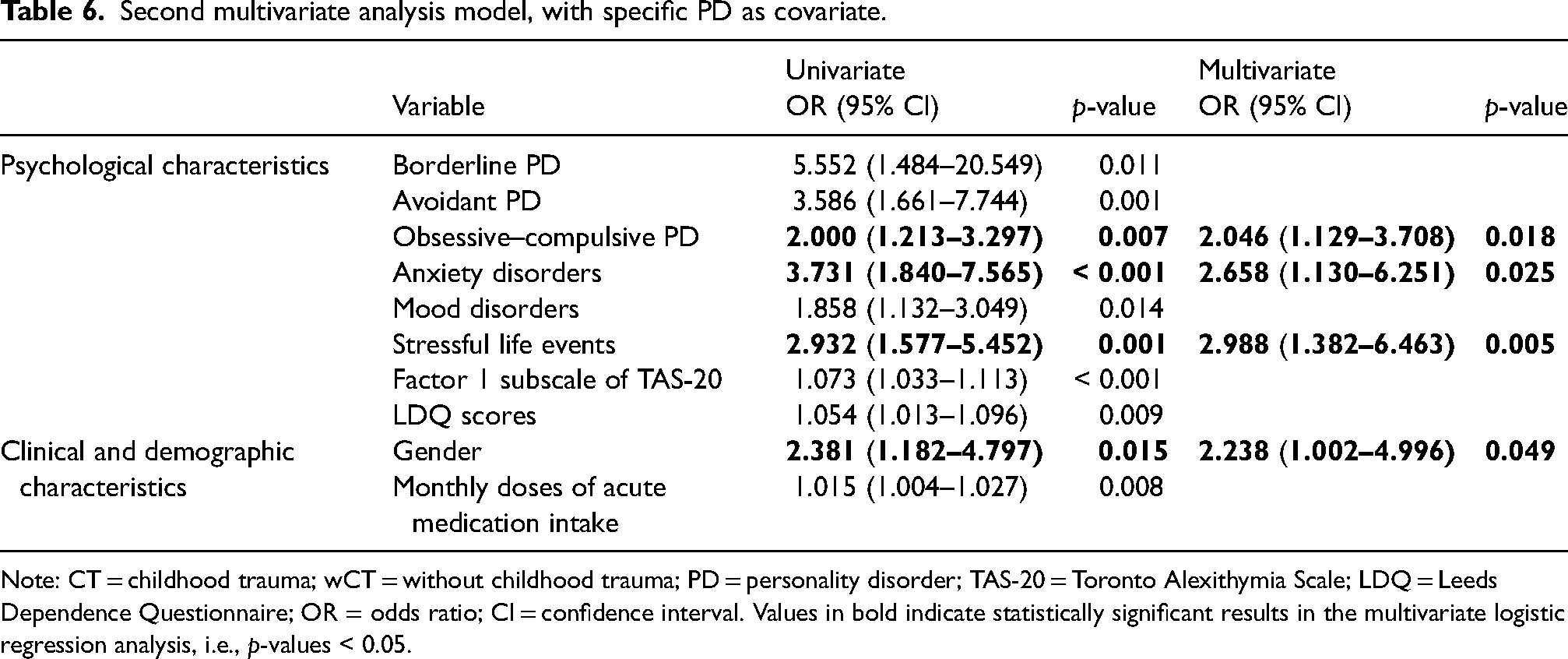
Note: CT = childhood trauma; wCT = without childhood trauma; PD = personality disorder; TAS-20 = Toronto Alexithymia Scale; LDQ = Leeds Dependence Questionnaire; OR = odds ratio; CI = confidence interval. Values in bold indicate statistically significant results in the multivariate logistic regression analysis, i.e., p-values < 0.05.
Discussion
The present study aimed to bridge the gap in the literature regarding the association between CTs and the psychological and clinical profiles in migraine. Specifically, we investigated the impact of CTs on PDs, psychopathologies (anxiety and depression), alexithymia, exposure to stressful events and clinical-demographic characteristics in a large migraine sample. The findings revealed a 41% prevalence of CTs in CM + MO (n = 78 out of 192 participants with CM + MO), aligning with prior research,20,23,44,45 whereas a slightly lower yet substantial prevalence was observed in EM patients (36%, n = 31 out of 84 participants with EM), suggesting that early life adversity may influence migraine vulnerability across its clinical spectrum.
Psychological characteristics
The occurrence of CT was associated with a higher prevalence of both Cluster B and Cluster C personality disorders, particularly borderline and obsessive–compulsive PDs: these findings were consistent across both descriptive and multivariate analyses. Existing literature suggests that CTs can influence personality development through neurobiological, psychological and relational pathways.29,30,46–48
Neurobiologically, CTs affect amygdala and prefrontal cortex development, increasing emotional reactivity and reducing impulse control, which are typical traits of borderline disorder. 49
A review conducted by Thomason and Marusak 50 explains how early traumatic experiences predispose to cognitive-behavioral, emotional and somatic problems and are strong predictors of psychiatric illnesses, highlighting alterations in neurological structure and function. These alterations predominantly involve the neural pathways of stress, emotion processing and regulation, as well as the pathways related to cognitive control, selective attention and reward processing. CT can dysregulate the hypothalamic-pituitary-adrenal axis and affect the hippocampus, which is associated with memory consolidation and stress response. The limbic emotion-regulation network, including the prefrontal cortex, anterior cingulate cortex and amygdala, is particularly affected. The amygdala, central to threat processing, shows heightened reactivity to emotional stimuli. Reward pathways, involving the ventral striatum, also appear altered, resulting in reduced reward sensitivity and diminished positive affect. Neural connection architecture is found to be altered, with changes in the amygdala-ventromedial prefrontal cortex regulatory pathway and in the organization of the default mode and salience networks, suggesting possible changes in information processing or perception. These neurobiological disruptions may underlie the link between early adversity and later emotional psychopathology.
Experiences of abuse and neglect impair self-image and emotional regulation, fostering dysfunctional coping strategies such as avoidance, self-harm or aggression. 51 Relationally, CTs may foster insecure attachment patterns, contributing to persistent interpersonal difficulties. 52
These factors may help account for the strong association between CTs and Cluster B disorders, particularly borderline PD, 53 which has also been linked to migraine through shared mechanisms of emotional dysregulation and central sensitization 54 Furthermore, physical and sexual abuse, which are core components of CTs, are known risk factors for the development of borderline traits, fostering a hostile worldview and impulsive or aggressive responses. 48
In parallel, our results also highlight a significant link between CTs and Cluster C PDs. This is supported by a meta-analysis by Crișan et al., 55 which demonstrated that CTs may promote dysfunctional cognitive-affective patterns related to self and others, fostering traits such as dependency and perfectionism. In particular, negative emotionality and emotional neglect are frequently linked to obsessive–compulsive PD, often manifesting as chronic anxiety and perfectionistic tendencies. 48
Beyond PDs, in line with our findings, CTs increase vulnerability to a broader range of psychopathologies by impairing emotional regulation and inducing chronic hyperactivation of the nervous system. 49 This results in hypervigilance and a persistent sense of threat, a core feature of anxiety disorders, reinforced by negative cognitive schemas marked by distrust and insecurity. Emotional dysregulation can channel distress into anxiety, 56 being identified as significant risk factor for the progression from EM to CM, as demonstrated for example by Buse et al., 57 reinforcing a vicious cycle. 56 Moreover, CTs contribute to the development of depression by undermining personality functioning, leading to a fragile sense of self, unstable relationships and poor coping strategies. These factors may sustain depressive symptoms even in the absence of current trauma. 58 Both anxiety and depression are more prevalent in individuals with CTs and are well-established risk factors for migraine chronification, supporting the higher prevalence of CTs observed in our CM cohort.
Moreover, we observed more severe stressful life events in the CT group compared to the wCT. 35 Consistent with our previous findings, 23 CTs increase vulnerability to encountering new adversities later in life, perpetuating a risk exposure cycle. This association particularly involves events related to health, interpersonal relationships, work and finances. The heightened exposure to subsequent stress likely reflects the long-term impact of CT on psychological adaptation and coping abilities, predisposing individuals to unstable living conditions and maintaining elevated levels of chronic stress in adulthood. This mechanism is particularly relevant for subjects with migraine because the interaction between CTs, chronic stress and psychological vulnerability may exacerbate the frequency and severity of migraine attacks. 26 In this sense, continuous exposure to stressful events acts as an aggravating factor for migraine.
Finally, we found higher TAS-20 Factor 1 (difficulty identifying feelings) scores in the CT group compared to the wCT. This result is consistent with previous studies59–66 and aligns with our prior findings, 23 where we demonstrated higher alexithymic levels in individuals with CTs, particularly in the dimension related to difficulty identifying feelings. CTs appear to hinder the development of basic emotional competence, such as the ability to recognize and differentiate emotions from bodily sensations. This deficit represents a psychological vulnerability that, when combined with later stress, may contribute to chronic pain conditions, such as CM + MO, and complicate their management.
Clinical and demographic characteristics
CT patients exhibited a higher proportion of females, consistent with literature indicating that women report significantly higher levels of all forms of child abuse and neglect compared to males. Specifically, females are more frequently exposed to emotional, physical and sexual abuse, 56 as well as emotional and physical neglect, with almost half reporting experiences of all five forms of maltreatment, compared to just over one-quarter of males. This discrepancy may reflect both greater objective exposure and sex-related differences in the perception and reporting of traumatic experiences.62,67
Furthermore, we observed an earlier onset of migraine and a higher monthly intake of acute migraine medication in CT individuals compared to wCT. These findings are consistent with previous studies.62–66 The earlier onset may be explained by the neurobiological alterations induced by CTs, which increase brain sensitivity to painful stimuli and may also facilitate the progression from episodic to chronic migraine. Additionally, alexithymic traits, particularly difficulties in recognizing and distinguishing emotions from bodily sensations, appear to contribute to an amplified perception of pain and impaired migraine management. 23 The increased medication intake may reflect impaired emotional regulation skills, with patients more likely to use medication not only to alleviate physical pain, but also as a dysfunctional coping strategy to manage emotional distress. 24
Study limitations and clinical implications
Despite the relevance and strengths of the present study, some limitations should be acknowledged. A potential limitation is the use of the CTQ, a self-report measure, to assess CTs. Retrospective identification of CTs presents inherent challenges, 68 including childhood amnesia, 69 memory biases 70 and mood-state-dependent recall. 71 The “seven sins of memory” 72 further emphasize risks of memory transience, misattribution and suggestibility, including typical distortions such as forgetting over time, misattributing information and being influenced by suggestion or current beliefs, all of which may reduce the reliability of retrospective trauma reports. Additionally, the recruitment from a clinical setting may limit the generalizability of these findings because the sample includes individuals already seeking specialized care, potentially introducing selection bias. We recognize as an additional limitation that we did not properly collect some information at baseline, specifically regarding migraine preventive treatments. Future longitudinal studies and community-based samples may help to further validate and generalize these findings.
Despite these limitations, the strength and consistency of the observed associations emphasize the clinical relevance of addressing CTs in migraine care, possibly already during childhood or adolescence, to prevent a possible negative evolution. Elevated CTQ scores may indicate underlying personality pathology and psychological vulnerabilities that could complicate management. Crucially, this study challenges the view of migraine as a purely somatic condition.73–77 The observed association between CTs, personality disorders and psychological comorbidities supports the reconceptualization of migraine within a broader psychopathological framework, where affective, relational and neurobiological factors converge.78–80 We mainly focused on PDs, although the aim of the present study was to consider the predictive value of all the psychological, clinical and demographic characteristics together. By adopting a comprehensive approach that integrates psychological, clinical and demographic variables, 81 the present study highlights the existence of a distinct migraine phenotype shaped by early trauma and its lasting impact on emotional and behavioral regulation. Overall, the present study aims to address an area that is still lacking in the literature, namely the link between traumatic events experienced during childhood and the clinical manifestations of migraine in adulthood. Our findings suggest that childhood traumatic experiences not only increase the likelihood of developing migraine, but also affect its frequency and severity, as well as its associated psychological profile, supporting the view of migraine as a biobehavioral disorder.
To conclude, our results advocate a paradigm shift: effective migraine management requires moving beyond symptom control to embrace holistic, individualized interventions that address the interplay between mind and body. Early identification of CT exposure may serve as a key step toward more targeted, multidisciplinary care, ultimately improving outcomes for this complex patient population.
57
Forty percent of patients reported CT, which was more frequent in CM + MO (41%) than in EM (36%). CTs are associated with more personality disorders, especially Clusters B and C. More anxiety, depression, alexithymia and stressful events in the CT group. CT more present in females, related to early migraine onset and increased medication use.
Footnotes
ORCID iDs
Ethical considerations
The study was approved by the local Ethics Committee (San Matteo Hospital, Pavia, Italy) and written informed consent was obtained from all participants.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was funded by the Italian Ministry of Health to the IRCCS Mondino Foundation (Ricerca Corrente).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Data availability statement
The dataset generated and analyzed during the current study is available in the Zenodo repository, with the DOI: 10.5281zenodo.15130614. The dataset is available from the corresponding author on reasonable request.