
Abstract
Background
Cervicogenic headache is a rare headache disorder which is garnering increasing clinical and research interest, but whose prevalence and clinical phenotype is surrounded by uncertainty. We found it timely to systematically appraise the current literature on prevalence, relative frequency, and clinical features of cervicogenic headache in population- and clinic-based settings.
Methods
PubMed and Embase were searched for observational, population- and clinic-based studies published between 1 January 1942 and 3 September 2024 that reported on the prevalence and relative frequency of cervicogenic headache, diagnosed according to the International Classification of Headache Disorders. The titles, abstracts, and full text-articles were screened by two independent investigators. To estimate prevalence and pooled relative frequency of cervicogenic headache across clinic- and population-based studies, random-effects meta-analyses were conducted. The study was pre-registered on PROSPERO (identifier: CRD42024498128) and reported in accordance with the Guidelines for Meta-Analyses of Observational Studies in Epidemiology.
Results
Three studies met the inclusion criteria from the International Classification of Headache Disorders for diagnosing cervicogenic headache. One was population-based reporting on the prevalence and two were clinic-based reporting on the relative frequency of cervicogenic headache among adult patients who were evaluated for headache in a tertiary care unit. The one population study reported a prevalence of 3.9% with females representing 77.8% of those affected. In the two clinic-based studies, the relative frequency was found to be 3.1% (95%, CI, 2.6–3.8) amongst the adult outpatient population of 3165 patients evaluated for headache, with women representing 80.8% (95%, CI, 71.9–87.4).
Conclusions
Based on this meta-analysis, data on the prevalence and relative frequency of cervicogenic headache are limited. The scarcity of data stresses the need for further research into cervicogenic headache, the diagnostic criteria, and its current position in the International Classification of Headache Disorders.
This is a visual representation of the abstract.
Introduction
Cervicogenic headache is a rare secondary headache disorder attributed to cervical pathology, first described by Ottar Sjaastad in 1983 (1,2). In recent years, cervicogenic headache has gained increasing clinical and research interest (3,–7). However, certain ambiguities surround the frequency of the disorder in part owing to overlaps in the clinical presentation with other headache disorders (5). These ambiguities are even greater in the face of the growing recognition of neck pain and cervical involvement in primary headache disorders, with up to 90% of patients presenting with neck pain (8,–10).
Several studies have investigated the prevalence of cervicogenic headache in population-based cohorts, or the relative frequency in the headache clinics. Nevertheless, these have yielded discrepant estimates, leading to uncertainties about the actual prevalence of cervicogenic headache and its clinical presentation. Multiple factors could potentially contribute to these discrepancies, including evolution of the diagnostic criteria through multiple iterations of the International Classification of Headache Disorders (ICHD), but also confounding with nonstandard diagnostic criteria such as those of the Cervicogenic Headache Study Group (CHSG). The diagnostic boundaries for primary headache disorders with neck symptoms, and other secondary disorders such as persistent post-traumatic headache, likewise create challenges in differential diagnosis (9,11,–14). An overview of the literature is therefore needed to summarize current knowledge on the prevalence and relative frequency of cervicogenic headache. Such an overview might also help identify clinical features that distinguish cervicogenic headache from other headache disorders, thereby creating opportunities for refining clinical diagnosis. Furthermore, it would facilitate further research into cervicogenic headache.
We therefore undertook a systematic review and meta-analysis of existing literature to assess the prevalence and clinical features of cervicogenic headache in the general population as well as the relative frequency in tertiary care centers. Finally, we critically appraised the methodology of included studies.
Methods
Search strategy
We pre-registered the current study on PROSPERO (identifier: CRD42024498128) and reported in accordance with the Guidelines for Meta-Analyses of Observational Studies in Epidemiology (MOOSE). On 4 September 2024, we searched Medline, Cochrane, and Embase databases from 1 January 1942 to 3 September 2024 for population – or clinic-based studies investigating the relative frequency, prevalence, and clinical features of cervicogenic headache. The search string was “cervicogenic headache.” In cases of incomplete reports or unpublished data, we contacted the relevant investigators. The PICO framework was not used, since the review did not assess any interventions.
Selection criteria
Studies were eligible if using an observational, cross-sectional, prospective, retrospective, clinic-based, or population-based design and reporting on the prevalence, relative frequency, or clinical features of cervicogenic headache amongst adult participants (≥18 years of age), diagnosed according to any iteration of the ICHD (Table 1). Eligible studies had to comprise 10 or more participants (Table 2 for full inclusion and exclusion criteria). Studies which did not adhere to ICHD criteria, or mixed these with non-ICHD criteria, such as those of the CHSG, were excluded (15,16). These criteria are not validated to be equivalent to ICHD criteria, but rather seem to re-diagnose patients who according to the ICHD have other headache disorders (e.g., migraine or tension-type headache), as having cervicogenic headache (17,–19).
Diagnostic criteria for cervicogenic headache.

ICHD: International Classification of Headache Disorders, 1st-3rd editions; CHSG: Cervicogenic Headache Study Group. Diagnostic criteria are from the four iterations of the International Classification of Headache Disorders (ICHD) and ICHD-4a is currently underway. ACriteria not sufficiently validated. BFractures, infections, rheumatoid arthritis, tumors are not sufficiently validated but are accepted as valid causes when demonstrated to be. CClinical signs must have demonstrated validity and reliability. D≥ 90% reduction in pain to a level < 5 on the 100-point visual analog scale. EImaging findings in upper cervical spine are common in patients without headache but are suggestive yet not firm evidence of causation.
Inclusion and exclusion criteria.

ICHD: International Classification of Headache Disorders, 1st-3rd editions; CHSG: Cervicogenic Headache International Study Group.
Study selection and data extraction
Two investigators (C.L.R. and H.M.A) independently screened titles, abstracts, and full texts for eligibility. Discrepancies were resolved by a third investigator (R.H.C.) acting as final arbiter. The same two investigators (C.L.R. and H.M.A) independently extracted data into a pre-designed extraction sheet using Microsoft Excel.
Risk of bias assessment
Two investigators (C.L.R. and H.M.A) assessed risk of bias using the Joanna Briggs Institute Critical Appraisal Checklist for Studies Reporting Prevalence Data, with a third investigator (R.H.C) consulted in case of disagreements (Online Supplemental Table 1) (20). The sample size was calculated based on a previously published formula (see Online Supplemental Table 1 for details) (21). The instrument scores risk of bias from 0 to 100% based on nine domains, where higher scores indicate lower risk of bias. The risk of bias is then graded as high risk (≤49%), moderate risk (50%-69%), or low risk (≥70%) (Online Supplemental Table 3).
Data synthesis and analysis
The co-primary outcomes were the prevalence of cervicogenic headache in the general population, and the relative frequency of cervicogenic headache amongst participants with headache in tertiary care centers. Secondary outcomes included the relative frequencies of clinical features of cervicogenic headache in clinic-based studies. We conducted random effects meta-analysis when ≥ 2 studies were eligible using random intercept logistic regression model on log transformed data. As a post-hoc analysis, we likewise conducted meta-analyses of relative frequency and prevalence of cervicogenic amongst the excluded studies using CSHG criteria. This was done for comparative purposes only.
Between-study variance was calculated with the inverse variance and confidence intervals with the normal approximation method. We quantified between-study heterogeneity with the I2 statistic, regarding values ≤ 25% as low heterogeneity. All statistical analyses were conducted in R version 4.2 (R Foundation for Statistical Computing, Vienna Austria) using the “meta” (version 6.2) and “metafor” (version 4.6) packages.
Results
A total of 3104 articles were initially identified, of which 535 duplicates were eliminated. Subsequently, 2545 articles were excluded following evaluation of their titles and abstracts. The full texts of the remaining 24 articles were screened, leading to the inclusion of three for analysis (Figure 1). Of these, two clinic-based studies (15,16) and one population-based study met the eligibility criteria for inclusion (22). The clinic-based studies were conducted in outpatient clinics associated with a tertiary care center. One clinic-based study was a retrospective, cohort study (16) and the other was cross-sectional (15). The one population-based study was a cross-sectional study (22). All three studies reported on the relative frequency or prevalence of cervicogenic headache (15,16,22).

Preferred reporting items for systematic reviews and meta-analyses (PRISMA) flow diagram.
Additionally, five other studies were assessed but were not included in the analyses due to non-adherence to the corresponding ICHD criteria or using other criteria such as those of CHSG (19,23,–26). We found no eligible studies reporting mean age or age of onset of individuals with cervicogenic headache. Furthermore, we identified no eligible studies reporting the relative frequencies of clinical features of the headache in terms of laterality, location, pain intensity, character, monthly headache days, or associated symptoms such as photophobia, phonophobia, nausea, or vomiting. To provide a comprehensive overview of the literature, details of these studies are nevertheless reported in Online Supplemental Table 2. The risk of bias was low, moderate, and high for each of the studies assessed (Online Supplemental Table 3).
Prevalence and relative frequency of cervicogenic headache
The only population-based study reported a prevalence of 3.9% amongst 232 adult individuals (22). In the two clinic-based studies, the pooled relative frequency of cervicogenic headache was estimated to be 3.1% (95%, CI, 2.6–3.8) based on 3165 adults being evaluated for headache (Table 3, Figure 2) (15,16). No heterogeneity was noted across these two clinic-based studies (I2 = 0.0%) (15,16).

Forest plot of the relative frequency of cervicogenic headache in clinic-based studies.
Characteristics of the included studies on the relative frequency and prevalence of cervicogenic headache.
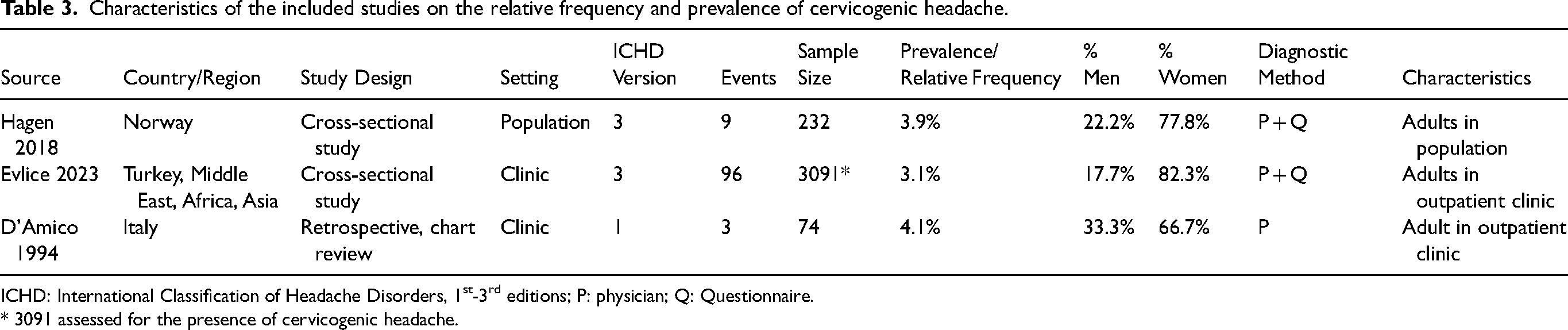
ICHD: International Classification of Headache Disorders, 1st-3rd editions; P: physician; Q: Questionnaire.
* 3091 assessed for the presence of cervicogenic headache.
Clinical characteristics
Amongst the two clinic-based studies, the pooled proportion of individuals with cervicogenic headache who were female was 80.8% (95%, CI, 71.9–87.4%; I2 = 68.4%; τ2 = 0.0) (Figure 3) (15,16). In the population-based study, the proportion of individuals with cervicogenic headache who were female was 77.8% (22).

Forest plot of the proportion of female individuals with cervicogenic headache.
Prevalence and relative frequency in studies applying CSHG criteria
Post-hoc meta-analyses of the excluded studies which used CHSG criteria yielded a pooled prevalence of cervicogenic headache of 1.2% (95%, CI, 0.1–10.3%; I2 = 98.8%; τ2 = 3.87) based on two population-based studies (Onlline Supplemental Figure 1), and a pooled relative frequency of 21.1% (95%, CI, 8.7–42.9%; I2 = 96.2%; τ2 = 0.54) based on two clinic-based studies (Online Supplemental Figure 2).
Discussion
Our meta-analysis revealed a pooled relative frequency of 3.1% for cervicogenic headache amongst adults evaluated for headache, based on just three eligible studies. The only population-based study reported a similar prevalence of 3.9% amongst adults in the general population. The estimates were associated with low, but largely indeterminable, heterogeneity, and should be interpreted with caution. Likewise, no studies reported on characteristics of cervicogenic headache as defined by the ICHD. Overall, our meta-analysis highlights the scarcity of robust clinical data on cervicogenic data, largely due in-adherence to diagnostic criteria of the ICHD.
Methodological considerations
Despite great clinical interest in cervicogenic headache, we noted a surprising scarcity of studies evaluating the disorders’ prevalence, relative frequency, or clinical features. This was mainly because only a few studies adhered to ICHD criteria, or mixed these with other, ad-hoc criteria. We also note that the only population-based study reported an unexpectedly high prevalence of 3.9% (22), compared to the lower relative frequency of 3.1% amongst individuals evaluated for headache in tertiary care centers (15,16). Surprisingly, this study did not find a single case of persistent post-traumatic headache, a common differential to cervicogenic headache, amongst the 232 participants (22).
Though we did not identify any heterogeneity in the pooled relative frequency amongst individuals with headache, this was likely due to the low number of studies, which can bias the I2 heterogeneity (27). Several key methodological differences could have contributed to the different estimates. Firstly, the criteria for cervicogenic headache have evolved with the iterations of the ICHD (Table 1). Most notably, the ICHD-2 was more restrictive than either its predecessor or subsequent iterations, requiring the complete abolition of headache with a diagnostic cervical blockade, or clinical signs with demonstrated validity (12,14). Additionally, resolution of pain in < 3 months after treatment of the cervical lesion was added in ICHD-2 then removed in ICHD-3 (11,12). Since no clinical signs have been validated, the diagnostic blockade was effectively a sine qua non for the diagnosis (2). In contrast, diagnostic blockade was not even a polythetic requirement in the ICHD-1, which however required radiological evidence (14). In the latest iteration, the ICHD-3, both diagnostic blockade and radiological evidence are polythetic criteria. However, due to the low number of eligible studies, differences in prevalence and relative frequency between the iterations of ICHD-3 are difficult to evaluate.
Several ineligible studies applied criteria from the CHSG on equal footing with those of the ICHD, hampering harmonization of cervicogenic headache research (19,23,–26). This is problematic, since it is unknown if patients diagnosed using CHSG criteria are comparable to those diagnosed according to the ICHD, and likewise whether they respond similarly to treatments. Ad-hoc criteria also hold the risk of misdiagnosing patients with other headache disorders as having cervicogenic headache. This potentially bars patients from specialized treatments such as onabotulinium toxin A or drugs targeting calcitonin gene related peptide (CGRP) signaling, which are restricted to certain diagnoses (e.g., migraine). This issue is exemplified by the pooled relative frequency of cervicogenic headache being 21.1% in clinic-based studies applying CHSG criteria (with an upper confidence interval of 42.9%), compared to just 3.1% in studies adhering to ICHD criteria.
The discrepancy is likely due to the ICHD requiring clinical or imaging evidence of cervical pathology with a temporal relation to the development or resolution of headache. By comparison, the CHSG criteria only requires signs and symptoms of cervical involvement with either provocation of neck pain by neck movement or pressure, restricted neck range of motion; or ipsilateral shoulder/arm pain (28,29). This can cause confusion, given the high prevalence of neck pain more frequent headache disorders, such as migraine and tension-type headache (10,30). As opposed to the ICHD criteria, the CHSG criteria also requires the headache to be unilateral without side shift and for there to be effect of anesthetic blockade (which is polythetic in the ICHD) (28,29).
Secondly, clinical and sociodemographic differences between the studies might have affected the relative frequency of cervicogenic headache. We observed a slight female preponderance of cervicogenic headache. Little is known about the potential causes for the female predisposition in cervicogenic headache, but similar sex distributions are noted for other headache disorders, such as migraine. One might speculate that this could be related to a higher prevalence and burden of neck pain in women (31), suggesting a disposition towards cervical nociception. It is also possible that sex hormones such as estrogen could affect headache-related structures and signaling pathways (32,–38). Nevertheless, it is important to note that even for migraine the exact mechanisms underlying the female predisposition remain elusive.
Whether cervicogenic headache prevalence differs with age remains unknown but could potentially affect the observed frequencies. Another factor is the presence of other comorbid headache disorders (16,22). This is not only relevant for heterogeneity, but the validity of cervicogenic headache as a separate disorder, especially since co-existent neck pain is frequent across headache disorders (9,10,39,40). Nevertheless, the contribution of each factor remains unknown, since the scarcity of studies prevented meta-regression analysis.
Differential diagnosis
In a clinical setting, several headache disorders may resemble cervicogenic headache and give rise to misdiagnosis. The notes of the ICHD describe cervicogenic headache as typically being a side-locked, unilateral headache, which can be provoked by palpation of cervical structures (11). It is noted that it is less frequently accompanied by nausea, photophobia, and phonophobia than is the case for migraine. Surprisingly, our comprehensive evaluation of the literature did not find any data supporting these or other clinical features of cervicogenic headache, as defined according to the ICHD. At this stage, diagnosis should therefore solely be guided by the ICHD criteria irrespective of the clinical presentation. Whether cervicogenic headache differs from other headache disorders in terms of treatment responses, e.g., to certain types of physical therapy, largely remains an open question (41). It is theoretically possible that responses to treatments other than diagnostic blockade could help distinguish cervicogenic headache, though further research is needed.
The estimated prevalence and relative frequency suggest that cervicogenic headache is a rare headache disorder, even in specialized headache centers. This stresses the need to carefully consider more frequent differentials, such as migraine or tension-type headache, in making the proper diagnosis. It also highlights that resources allocated to diagnose and treat the disorder should be proportional to its relative rarity. Diagnostic training should be not only sensitive to cases of cervicogenic headache, but also specific enough to exclude when this is not the likely diagnosis. To avoid overdiagnosis, clinicians should keep in mind that cervicogenic headache is a rare secondary disorder requiring evidence of a cervical pathology that is causally related to the headache; in most cases this would at current require imaging evidence of a lesion.
Migraine
Migraine represents a frequent differential to cervicogenic headache owing to its high prevalence and common association with neck pain (8,42,43). Individuals with migraine consistently report higher prevalence of neck pain and greater neck pain related disability than both healthy controls and those with tension-type headache (10,30). Furthermore, while blockades of cervical nerves and structures serve diagnostic purposes in cervicogenic headache, both migraine and other headache disorders can also respond to greater occipital nerve blockade (44). Given that no studies investigated the relative frequency of migraine associated symptoms such as nausea, vomiting, photophobia, and phonophobia in cervicogenic headache, these symptoms cannot be used to differentiate the disorders. Further studies are required to investigate similarities and differences in clinical characteristics of the two headache disorders. Likewise, it is important to investigate whether individuals with cervicogenic headache might experience migraine-like exacerbations similar to what is seen in post-traumatic headache (45).
Tension-type headache
Another clinically important differential diagnosis is tension-type headache. This is in part due to the high prevalence of tension-type headache (42). Furthermore, the pathogenesis of tension-type headache is suspected to involve muscular and cervical structures, including activation of nociceptive trigeminal and upper cervical fibers that innervate cranial muscles (46). Upper cervicogenic afferents also supply cervical musculature, before converging with headache-generating trigeminal input within the brainstem (47). Another important overlap in tension-type headache is the presence of pericranial tenderness upon palpation (11). Since this tenderness is described within both occipital and cervical regions, such tenderness might be confused for the clinical evidence of cervical pathology necessary to diagnose cervicogenic headache (48,49). Indeed, the notes to the ICHD specifies that cervical myofascial pain should “probably” produce a diagnosis of tension-type headache rather than cervicogenic headache (11). Just as for migraine, it is important to note that the clinical characterization of cervicogenic headache is too insufficient to differentiate it from that of tension-type headache.
Persistent post-traumatic headache
Another crucial differential for cervicogenic headache is persistent post-traumatic headache. While cervicogenic headache is characterized by headache due to a cervical pathology, persistent post-traumatic headache is defined as either developing after traumatic brain injury or a whiplash injury of the neck (11). A recent meta-analysis has shown that 38% of individuals who had experienced whiplash injuries still reported neck pain and post-traumatic headache one year after the injury (50). It can be difficult to differentiate clinical evidence for cervical pathology from whiplash injury, especially since both conditions are likely driven by pathological activation of cervical nociceptive afferents (51). The clinical presentation likewise remains largely unelucidated for both cervicogenic and post-traumatic headache following whiplash injury. Finally, there is a need for greater clarity in the ICHD to help distinguish persistent post-traumatic headache due to whiplash injury from cervicogenic headache. It seems reasonable that headache developing after trauma should yield a diagnosis of persistent post-traumatic headache as opposed to cervicogenic headache.
Future perspectives
Several key aspects remain to be elucidated to determine the prevalence of cervicogenic headache. The current diagnostic criteria in the ICHD-3 are currently too ambiguous for reliable clinical application (11), and there is a need for studies confirming their diagnostic reliability and validity. The necessary criterion for clinical or imaging evidence of cervical pathology known to cause headache is ephemeral, in that the notes for cervicogenic headache take no firm stance on what constitutes “causative” evidence. Future studies should validate which cervical pathologies cause headache, to determine when they should reasonably warrant a cervicogenic headache diagnosis. More data are required to identify a distinct phenotypical presentation of cervicogenic headache that might guide diagnosis. Pending further investigation of the validity of the current diagnostic criteria, it should be considered whether the diagnosis belongs in the appendix of the ICHD. The appendix was specifically intended to contain diagnoses where more research is required to substantiate their validity. Notwithstanding these issues, future research efforts should apply and further investigate ICHD criteria, to standardize research, or as a minimum report separately which patients were diagnosed according to the ICHD.
Limitations
Our meta-analysis is barred by the low number of studies meeting inclusion criteria, as well as the methodological differences, which included variations in iterations of the ICHD applied. We cannot exclude publication bias, in that investigators who did find any cases of cervicogenic headache might not publish the negative finding. Furthermore, we choose to exclude studies which did not adhere to ICHD criteria, to follow the internationally accepted consensus and to form a uniform and homogenous data basis for the estimates. We note that amongst the excluded studies not adhering to ICHD criteria, the prevalence or relative frequency of cervicogenic headache varied greatly, from between 0.17% to 31.6% (19,23).
Conclusions
Our meta-analysis found that cervicogenic headache was present in 3.1% of patients evaluated for headache, and in 3.9% in the only study of the general population. We found no eligible data on clinical characteristics of the disorder. Our findings highlight the scarcity of data on cervicogenic headache and prompts future research and critical appraisal of the disorder's position in the ICHD.
Key findings
In meta-analysis, the frequency of cervicogenic headache was 3.9% in the general population and 3.1% in headache clinics. This was based on only three eligible studies following ICHD criteria.
Females accounted for 80.8% of individuals with cervicogenic headache. No eligible studies reported specific clinical features of cervicogenic headache.
There is a considerable scarcity of data on cervicogenic headache, despite growing clinical interest. This underlines the need for further research into cervicogenic headache and the current diagnostic criteria.
Supplemental Material
sj-docx-1-cep-10.1177_03331024251322446 - Supplemental material for Prevalence and relative frequency of cervicogenic headache in population- and clinic-based studies: A systematic review and meta-analysis
Supplemental material, sj-docx-1-cep-10.1177_03331024251322446 for Prevalence and relative frequency of cervicogenic headache in population- and clinic-based studies: A systematic review and meta-analysis by Christopher L. Robinson, Rune H. Christensen, Haidar M. Al-Khazali, Faisal Mohammad Amin, Ailing Yang, Richard B. Lipton and Sait Ashina in Cephalalgia
Footnotes
Author contributions
C.L.R., R.H.C., H.M.A., F.M.A., A.Y., R.B.L., and S.A. conceived, designed, wrote, and revised the review. C.L.R. did the literature search with H.M.A. S.A. and R.B.L. are the primary investigators.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: C.L.R., R.H.C., H.M.A., F.M.A., A.Y. declare no competing interests. S.A. provided consulting and teaching services for Allergan/Abbvie, Eli Lilly and Company, Impel NeuroPharma, Linpharma, Lundbeck, Satsuma, Percept, Pfizer, Teva, and Theranica. R.B.L. has received research support from the National Institutes of Health, the FDA, and the National Headache Foundation. He serves as consultant, advisory board member, or has received honoraria or research support from AbbVie/Allergan, Aeon, Amgen, Biohaven, Dr Reddy's Laboratories (Promius), electroCore, Eli Lilly and Company, GlaxoSmithKline, Lilly, Lundbeck, Merck, Novartis, Pfizer, Teva, Vector, and Vedanta Research. He receives royalties from Wolff's Headache, 8th edition (Oxford University Press, 2009) and Informa. He holds stock/options in Axon, Biohaven, CoolTech, and Mainistee.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.