
Abstract
Background
The present study aimed to investigate the prevalence and impact of primary headache among students aged 8–12 years in the city of Douala (Cameroon).
Methods
From January to May 2022, a cross-sectional study was conducted in 52 primary schools randomly selected from five districts in the city of Douala. The study population consisted of primary school students in level III classes. The diagnosis of primary headache was made according to the International Classification of Headache Disorders, 3rd ed (ICHD-3) criteria and the paediatric version of the HARDSHIP questionnaire was used for recruitment.
Results
In total, 2056 students participated of whom 55.9% (n = 1149) were female, with a median age of 11 years. The prevalence of headache in the last 12 months was 85.7% (n = 1762), that of migraine was 26.1% (n = 536) and that of tension-type headache (TTH) was 15.1% (n = 311). Regarding the impact of primary headaches, 176 (32.8%) migraineurs reported absenteeism from school compared to 70 (22.5%) students with TTH (p = 0.03) and 309 (57.6%) migraineurs had a break in their activities compared to 147 (47.3%) students with TTH (p < 0.01).
Conclusions
Primary headaches are common among students aged 8–12 years in the city of Douala. They are responsible for a considerable impact on children and their family, particularly for migraineurs.
This is a visual representation of the abstract.
Introduction
Headache is a pain located in the head, above the orbitomeatal line and/or the nuchal crest (1). The main groups of headaches are primary headaches, secondary headaches, painful neuropathy, other facial pain and other headaches (1). Primary headaches are neither caused by nor attributed to an underlying disease. They can be distinguished from secondary headaches, which may have the same phenotypic characteristics but still meet the causal criteria of another disorder. Primary headache disorders are subdivided into four subtypes: migraine, tension-type headache (TTH), trigeminal-autonomic cephalalgias, and other primary headache disorders (1). Primary headaches are common in childhood, with migraine and TTH being the most frequent (2). Reported primary headaches are rare in children under aged <4 years. However, the prevalence of these conditions increases with age. A prevalence of 5.9–37.7% in pre-school age, 38–50% in school age and 75% in adolescence have been reported (3). Other studies report an estimated prevalence ranging from 3–8% at 3 years, up to 57–82% from 7–15 years (4–6). Balottin et al. (3) suggest that environmental and psychological factors play an important role in idiopathic headache with onset in pre-school age, and thus the diagnostic-therapeutic approach must take these factors into account (3). In Africa, studies on the prevalence and impact of primary headache disorders in children are rare (7–9). In Cameroon, Mapoure et al. (10) reported a prevalence of headache of 54.1% among the students of Garoua with an average of school absence of 2.1 days per month. Few data are available on primary headaches disorders epidemiology and impact in school-age children in Sub-Saharan African countries. The present study aimed to investigate the prevalence and impact of primary headache among students aged 8–12 years in the city of Douala (Cameroon).
Methods
This was a cross-sectional study conducted over a period of 5 months, from 1 January to 31 May 2022. Our study took place in primary schools of the five health districts of Douala (Cameroon), with an estimated general population of 3,049,034.
Our study population consisted of students regularly enrolled in level III classes (grade 5–6) in a primary school in the city of Douala. Children aged 6–7 years in this setting were not able to read, understand and fill the questionnaire. We then decided to recruit those aged 8–12 years, and they were included regardless of sex, ethnicity or socioeconomic conditions. We contacted 55 primary schools and 48 of these agreed to take part, resulting in a total of 65 classes being interviewed. Students who were unable to participate in the study (i.e. unable to read or write) or who did not provide the consent of a parent or guardian were excluded.
We carried out a cluster sampling of schools and then sampling of classes in the selected schools. For cluster sampling, we first obtained a distribution of primary schools in the city of Douala by district and then drew lots, resulting in a total of 60 schools to be surveyed. Within each school, a cluster of class to surveyed was performed and then we worked with pupils who met the criteria for inclusion. We used the Headache-Attributed Restriction Disability Social Handicap and Impaired Participation (HARDSHIP), a questionnaire tested and validated by the International Headache Society based on the ICHD-3 criteria in its version for children (11,12). This scale comprises 44 questions divided into four sections:
Socio-demographic characteristics: age, sex, class, school Clinical features of the headache (duration, type, intensity, location, aggravating factors, associated signs). Impact of headaches (assessed in terms of school absenteeism, loss of leisure time, loss of parental working time, children's emotional state during attacks and their quality of life, etc.) Quality of life. Cut-off of the HARDSHIP score on the quality-of-life score was calculated for each participant (ranging from 12 to 48) by summing the values (never: 1; sometimes: 2; often: 3; always: 4) in the negative response variables and (never: 4; sometimes: 3; often: 2; always: 1) in the positive response variables; a score of 12–30 corresponded to a good quality of life and a score of 31–48 corresponded to a poor quality of life. The HARDSHIP score was administered by the children themselves.
To assess pain, we used the visual analogue scale (VAS), which measures pain intensity on a scale from 0 to 10: VAS between 1 and 3: pain of mild intensity, VAS between 3 and 5: pain of moderate intensity, VAS between 5 and 7: intense pain, VAS greater than 7: very intense pain.
We explained each statement to all the children in simple terms and each of them could interrupt us if they had a term or question or they did not understand. Each statement took between 1 and 3 minutes before we moved on to the next one.
Data collection procedure
The students were contacted through the headmaster of the school and head teachers of the classes. After request for a 30-minute break in lessons by the administrative authority, we started the distribution of anonymous survey forms to students. The instructions for filling in the forms were carefully explained to the children. The study was conducted in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines (13).
Statistical analysis
The data were entered using CSPro, version 7.3 (US Census Bureau, Washington, DC, USA) and then analysed using SPSS, version 23.0 (IBM Corp., Armonk, NY, USA). Categorical variables were presented as frequency and percentage. Continuous variables were given as the mean ± SD and/or median. Comparisons between variables were made using a chi-squared test, Student’s t-test or analysis of variance. Quality of life variables were coded as poor or good according to the above description on the methodology session. Factors associated with poor quality of life in students with headaches were determined by logistic regression analysis. p < 0.05 was considered statistically significant.
Ethical statement
Approval for the study was obtained from the institutional ethics committee of the University of Douala N° 3003 CEI-UDo/04/2022/T and administrative authorization of the Ministry of Basic Education was obtained through the Littoral regional representation. Consent forms were filled-in in advance by the students’ parents. The survey forms were anonymous and refusal to participate at any stage of the study was considered.
Results
In total, 2515 students were registered in 65 classes but 419 were not included because they were over the age of 12 years or did not provide parental consent. Forty children were excluded because they could not read or write. The final number of students available for analysis was 2056 (Figure 1). In private schools (n = 31), we included 1252 students and 804 were recruited in government schools. More than half of the study population was female (n = 1150; 55.9%). The most common age was 11 years (n = 757; 36.8%) with a median age (interquartile range) = 11 (10–11).

Study population flowchart.
Prevalence and characteristics of headaches
Among this school-age population, 85.7% (95% confidence interval (CI) = 83.1–87.8) had experienced headaches within the 12 months preceding the interview. Some 66.8% (95% CI = 64.2–68.5) of students reported headaches within the previous four weeks (Table 1). Migraineurs accounted for 26.1% (95% CI = 24.2–27.9), whereas 15.1% (95% CI = 13.5–16.7) of students experienced TTH. Other headaches represented 44.6% (95% CI = 42.5–46.7) of cases (Table 2). As shown in Table 3, 60.6% (n = 325) of migraineurs had a headache lasting more than four hours and, for 47.2% of them, the intensity of headache was severe. Some 43.4% of students suffering from TTH described a headache lasting less than one hour, and severe intensity was reported by 57.6% of them (Table 4).
Prevalence of headaches according to the periods considered in the questionnaire.

CI = confidence interval.
Types of headaches (prevalence over the last 12 months).

Other headaches: headache type that do not fullfill diagnostic criteria for migraine or tension-type headache.
CI = confidence interval.
Clinical characteristics of migraine in the study population.

Clinical characteristics of tension-type headache in the study population.

Duration of headaches
Migraineurs described an average headache duration of 1.56 ± 1.63 days, which was significantly higher than a duration of 1.09 ± 1.39 days (p < 0.001) reported by TTH sufferers. In the four weeks preceding the interview, the average duration of headache was significantly higher in migraineurs (3.7 ± 3.2 days) compared to students suffering from TTH (2.6 ± 2.7 days) (p < 0.001).
Duration of medication taken
In the week preceding the interview, the average duration of headaches medication was significantly higher in migraineurs (1.23 ± 1.43 days) compared to TTH cases (0.87 ± 1.22 days) (p < 0.001). Similar findings were described in the four weeks preceding the interview (Table 5).
Distribution of students by headache type and duration of medication.

Impact of headaches on school and -school activities
Four weeks before the interview, the average number of days of school absence was significantly higher in migraineurs (0.77 ± 1.4 days) compared to TTH cases (0.52 ± 1.1 days) (p = 0.003). Some 57.6% of migraineurs stopped their activities (leisure, household chores, school) because of headaches compared to 47.3% of students with TTH. In addition, 31.2% of migraineurs parents/guardians lost days of work as a result of a child's headache (Table 6).
Impact of headaches on school and extra-school activities over the last four weeks.

Impact of headaches on quality of life
Quality of life was poor in 33.4% of migraineurs, and they were 2.84 times more likely to have a poor quality of life than students without headaches. Children with TTHs were 1.67 times more likely to have a poor quality of life than students without headaches (Table 7). Some 7.1% of headache cases said they were “always” afraid of having a headache and 13.8% of them “always” wanted to notify their headaches (Figure 2(a)). Some 19% of students with headache “never” had access to leisure activities. In addition, 24% of headaches sufferers were “never” able to manage their headaches well (Figure 2(b)).

(a) Psychological impact of headaches over the last four weeks. (b) Psychological impact of headaches over the last four weeks.
Impact of headaches on quality of life.
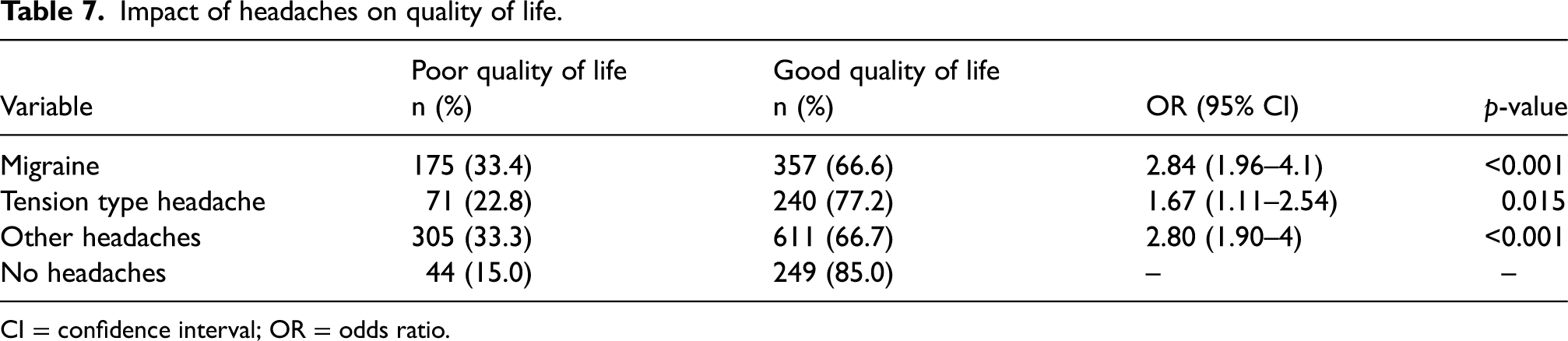
CI = confidence interval; OR = odds ratio.
Factors associated with poor quality of life in students with headaches
After a multivariate analysis using logistic regression, factors associated with poor quality of life among students were factors associated with headaches (nausea, vomiting, avoidance of walking), school and extra-school impact data (parents stopping their activities in the last four weeks) (Table 8).
Factors associated with poor quality of life in students with headaches.

CI = confidence interval; OR = odds ratio.
Discussion
The present study aimed to provide features of primary headaches among students in the city of Douala. The study was conducted in 52 primary schools randomly selected from five districts in the city of Douala. The diagnosis of primary headache was made according to the ICHD-3 criteria and the paediatric version of the HARDSHIP questionnaire used for recruitment. The prevalence of primary headache was high: in the preceding year, 85.7% of children reported headache, and 66.8% reported headaches within the previous four weeks with migraine the most common type (26.1%), followed by TTH (15.1%) and other headaches in 44.6% of cases. The impact of these primary headaches was notable: 32.8% of migraineurs reported absenteeism from school compared to 22.5% of students with TTH and 57.6% of migraineurs had a break in their activities compared to 47.3% of students with TTH.
More than half of the participants were female. The most recent population data of the National Statistics Institute of Cameroon showed female predominance in 2019 (14). The majority of students were enrolled in the level III classes not only to reflect the age range considered in the methodology, but also to reduce recall bias linked to the intellectual and memorization skills required to fill in the survey form (8). The median age of our population was 11 years (interquartile range= 10–11), which is a result similar to that obtained by Zewde et al. (8) in Ethiopia (12 years); Luvsanonnov et al. (15) in Mongolia (11 years); and Genc et al. (16) in Lithuania (11 years).
Prevalence of primary headaches
In this study, the one-year prevalence of headaches was 85.7%. Migraine was found in more than one-quarter of students suffering from primary headache. This predominance of migraine over TTH in children was also reported by Zewde et al. (8) in Ethiopia in 2018 (38% vs. 19.9%); Luvsaronnov et al. (15) in Mongolia (27.1% vs. 16.1%); and Wöber et al. (17) in Turkey in 2018 (26.7% vs. 12.9%). However, Genc et al. (16) in Lithuania found a higher prevalence of TTH, which was higher than the migraine prevalence (21.4% vs. 25.6%) (16). This difference, although isolated for studies using the ICHD-3 criteria, could be explained by the influence of race and environment in the development of headache in general and migraine attacks in particular (7). The lower migraine prevalence of 10.1% in children and adolescents in Kuwait was associated with reported cultural, genetic and geographical reasons by Al-Hashel et al. (18). Asian populations are less likely to develop a migraine attack than black subjects and much less likely than Caucasian subjects (18,19).
Description of the clinical characteristics of primary headaches
More than one-third of migraineurs reported an attack duration of two to four hours. Wöber et al. (17) in Turkey found an attack duration of two to four hours in 19.4% of migraineurs. The duration of migraine attacks has been reported to be shorter in children compared to adults.
Among these students, 43.5% and 47.2% of migraineurs described their pain as severe and very severe, respectively. For Wöber et al. (17), 55.4% and 16.1% of migraineurs experienced severe and very severe pain. In Norway, Krogh et al. (20) reported incidences of 51.4% and 41.9% for severe and very severe intensity cases of migraine attacks. The intensity of migraine attacks experienced by children is severe regardless of race (African or Caucasian).
In more than two-third of migraineurs, the location of the headache was bilateral. Wöber et al. (17) and Maiga et al. (21) found bilateral pain location in migraineurs in 53.2% and 44.8% of cases, respectively. This discrepancy could be explained by the difference in age groups. Wöber et al. (17) and Maiga et al. (21) included adolescents (15–18 years and 12–17 years). Migraine attacks are most often bilateral in children compared to the unilateral location reported by adolescents and adults (22,23).
Approximately one-third of migraineurs reported pressing character of pain. Some 21.6% of migraineurs described a similar pattern in the study by Wöber et al. (17). The atypical features of migraine attacks in children were wrongly attributed to sinusitis or refraction and ocular convergence (24). More than half of migraine sufferers reported vomiting during their attacks and more than two-thirds experienced nausea. Similar findings were reported by Zewde et al. (8) in Ethiopia, which highlights the diagnostic challenge of migraine in sub-Saharan Africa, where a headache associated with nausea and vomiting is often wrongly treated as malaria. This should raise the attention of parents and physicians.
The pulsatile character described by the majority of TTH cases may be explained by a memory bias of these younger population. Age-related differences in symptom description may have influence this result. Also, the undifferenciated headache (UdH) reported by Wöber et al. (17) represents those headaches that are in a shifting state between migraine and TTH before maturing by adulthood into one or the other. It may be possible that some patients with suspected TTH really had migraine. By contrast, Genizi et al. (2) reported a pressing-like pain in more than half of students suffering from TTH. The study by Genizi et al. (2) included children and adolescents seen in a specialized neurology clinic with more accurate clinical investigation. In the present study, TTH was worsened by walking and/or was responsible for avoidance of walking in more than half of children.
Almost all students experienced phonophobia during a headache episode. This was consistent with the findings of Wöber et al. (17). Episodes of TTH could have a deleterious impact on daily life activities.
Impact of headaches
In the present study, the impact of primary headaches was assessed in terms of school absenteeism, loss of leisure time, loss of parental working time, children's emotional state during attacks and their quality of life.
The headaches disrupted school and social activities of the students. Over the last four weeks, about one-third of migraineurs reported school absenteeism from school. The majority of them experienced a break in their activities (leisure and household chores). The proportions of school absenteeism and break in activities were higher in migraineurs compared to students with TTH. Philip et al. found absenteeism in 20.5% of migraineurs compared to 11.3% of students with TTH, and cessation of activities in 57.3% of migraineurs compared to 34.5% of students with TTH. This difference in terms of impact could be a result of the clinical expression of migraine, which is typically more severe, worsened by walking and accompanied by nausea, vomiting or photophobia, being less frequently reported in TTH. Other studies conducted in Sub-Saharan Africa found an impact on the quality of life in 63.8–76.8% of students, with migraine described as an inability to attend outdoor activities, to carry out household chores, and school absence (7,21).
Parents’ professional activities were also disrupted. As a result of an attack, almost one-third of parents of student migraineurs were absent from their workplace for at least one day. A lower percentage was found in the parents of students with TTH. Wöber et al. (17) found a loss of working time in 14.5% and 7.8% of parents of children and adolescents with migraine and TTH, respectively. Headaches also had an impact on the students’ emotional state. Almost three-quarters of students were afraid (to varying degrees) of having an attack, and one-quarter systematically had attention deficit during attacks. Al-Hashel et al. (18) found systematic attention deficit during headache in 26% of students. This may contribute to poor school performance.
In Douala, students with headaches were more likely to have a poor quality of life than students without headaches (odds ratio = 2.6). Migraine had the highest burden in term of poor quality of life. This was also reported in other studies (7,17). The quality of life of children suffering from primary headache is reduced compared to healthy children, particularly in the areas of mental health, parental impact time and family cohesion (25). The presence in our urban context of numerous triggers such as sensory stimulation, noise, heat, light, air pollution, hypoglycaemia and stress could contribute to the burden of primary headache in school-age children of Douala.
Because the students in the present study are in an exam year and a transition year from primary to secondary education, they are subject to greater academic pressure, with more subjects, more teaching hours, and even more continuous assessments and exams. Other studies have established the link between school stress and the onset of headache attacks, which have a detrimental impact on the quality of life (26,27).
This study provides, for the first time, data on the high frequency and the burden of primary headache in school-age children in Cameroon. However, these data are more representative of urban areas and are dependent on the recall of participants and the accuracy of the information reported (memory or recall bias). In Cameroon, a Central African country, headache is an ubiquitous presenting symptom of various pathologies such as malaria and flu that affect large numbers of people and it can sometimes be difficult to differentiate primary from secondary headaches disorders.
Conclusions
Primary headaches are common in primary school students. Migraine was the leading cause. Headaches were responsible for school absenteeism, and for the cessation of activities such as leisure and domestic activities. Primary headache had an impact on the children such as school absence and attention deficit, and on parents’ activities. Students with headaches are more likely to have poor quality of life, and migraine is more disabling than tension type headache.
Clinical implications
The prevalence of primary headache was high: in the preceding year, 85.7% of children reported headache, and 66.8% reported headaches within the previous four weeks with migraine the most common type (26.1%), followed by TTH (15.1%) and other headaches in 44.6% of cases.
The impact of these primary headaches was notable: 32.8% of migraineurs reported absenteeism from school compared to 22.5% of students with TTH and 57.6% of migraineurs had a break in their activities compared to 47.3% of students with TTH.
Footnotes
Acknowledgements
We thank Dr David Garcia-Azorin for proofreading the manuscript. We also thank all of the students and teachers for their help and collaboration.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical statement
Approval was obtained from the institutional ethics committee of the University of Douala N° 3003 CEI-UDo/04/2022/T, and administrative authorization of the Ministry of Basic Education was obtained through the Littoral regional representation. Consent forms were completed in advance by the students’ parents.
Funding
No financial support was received for the research, authorship and/or publication of this article.