
Abstract
Objective
To assess the association of neurologist ambulatory care with healthcare
Methods
This was a longitudinal cohort study from two-year duration panel data, pooled from 2002–2013, of adult respondents identified with diagnostic codes for headache in the Medical Expenditure Panel Survey. Those with a neurologist ambulatory care visit in year one of panel participation were compared with those who did not for the change in annual aggregate direct headache-related health care costs from year one to year two of panel participation, inflated to 2015 US dollars. Results were adjusted via multiple linear regression for demographic and clinical variables, utilizing survey variables for accurate estimates and standard errors.
Results
Eight hundred and eighty-seven respondents were included, with 23.3% (207/887) seeing a neurologist in year one. The neurologist group had higher year-one mean headache-related expenditures ($3032 vs. $1636), but nearly equal mean year-two expenditures compared to controls ($1900 vs. $1929). Adjusted association between neurologist care and difference in mean annual expenditures from year two to year one was −$1579 (95% CI −$2468, −$690, p < 0.001).
Conclusion
Among headache sufferers, particularly those with higher headache-related healthcare expenditures, neurologist care is associated with a significant reduction in costs over two years.
Headache is among the most common medical conditions, characterized by episodes of disabling pain that may require escalating doses of medication, imaging studies, and specialist care. The ubiquity of headache underlies the range of severity, with the vast majority requiring no treatment or only over-the counter analgesics to abort the headache episode. However, in nationally representative data, up to 22.7% of persons in the United States have severe headaches in any given 90 days (1). Headache is among the top 20 reasons for outpatient medical visits, representing 12 million office visits in 2009, and ranks in the top five diagnoses seen in emergency department visits (1). Although the majority of ambulatory care visits for headache are to primary care physicians, nearly one fourth of patients are seen by specialists (2). Persons with severe headache may be best managed by a comprehensive strategy addressing acute and chronic components of headache, lifestyle modification, appropriate use of neuroimaging, and preventative and abortive medications. In primary headache disorders, the goals of care should include avoidance of unplanned healthcare utilization and unnecessary radiological studies (3,4).
Healthcare costs associated with headache can be substantial, reflecting headache chronicity and severity. Approximately three percent of patients with episodic migraine may develop chronic migraine, increasing to almost seven percent in the setting of poor acute treatment efficacy (5). Chronic migraine sufferers in the United States are estimated to average over $4000 annually in attributable direct healthcare expenditures, while annual costs for episodic migraine care are 60% less (6). When specialists are involved in care, expenditures are often greater, in part due to the severity of the condition (7,8). Cost analyses evaluating the impact of the neurologist, as the specialist most commonly involved with headache care, can be challenging. Administrative claims datasets, on which cost analyses are often based, have the advantage of large sample sizes, but may lack clinical data (9,10). Cross-sectional analyses may fail to account for the severity of the condition, relationship of comorbid disorders, and the circumstances leading to neurologist involvement with care (e.g. neuroimaging may have prompted neurologist care, or occurred because of it). Furthermore, neurologists providing state of the art, high quality care for chronic, severe headache sufferers of necessity must do so at some cost (11). The effect of these measures on patient health may take time to become manifest.
Given these issues, we investigated how neurologist involvement in year one affected healthcare expenditures and utilization in the subsequent year in a nationally representative multiyear dataset. We hypothesize that neurologist care is associated with reductions in headache-related expenditures over time.
Methods
Data source
We used the Medical Expenditure Panel Survey (MEPS), a dataset compiled and maintained by the Agency for Healthcare Research and Quality (AHRQ) that is publicly available for healthcare researchers. MEPS consists of approximately 30,000 annual respondents who participate in the survey for two years, representing the non-institutionalized population of the United States in each year. Both year one and year two data are available for cross-sectional analysis, or both years can be examined in a panel format (12). Respondents complete detailed queries about their medical conditions and healthcare utilization, which are coded and logged by qualified technicians and verified with medical records and claims review whenever possible (13). MEPS has annual full-year and component event files, as well as linkage files and annual and longitudinal pooled survey files for creation of accurate national-level estimates and variances. MEPS further assigns diagnostic coding to each incident of healthcare utilization, allowing for the creation of condition-linked aggregate expenditures (14,15). We utilized the available data for panels 7–17, which includes the years 2002–2013.
Standard protocol approvals, registrations, and patient consents
The Human Subjects Division of the Institutional Review Board of the University of Washington has determined that MEPS is a dataset that does not require associated research projects to be reviewed for exemption or approval. The data contained in MEPs are neither identifiable nor private and do not meet the federal definition of “human subjects research”.
Selection of cohort of interest
We began with the annual condition files in MEPS for the years 2002–2013 to identify patients with headache using the Condition Classification Software (CCS) variables in MEPS condition files. CCS is a publicly available software diagnostic grouper from the AHRQ (16) that uses International Classification of Disease, version 9, Clinical Modification (ICD9-CM). CCS codes in the sample timeframe are durable from year to year, and therefore allow for pooling of patients with similar conditions over different years and panels.
Inclusion criteria
Included respondents had the CCS code for headache (CCS = 84). Respondents had to report headache for both year one and year two of participation in the panel. Only adult respondents (aged 18 or older) reported in MEPS panels 7–17 beginning on 1 January 2002 and ending on 31 December 2013, having non-zero headache-related expenditures in both years of participation, were included.
Data extraction
Extracted data variables were determined by Andersen and Newman criteria of enabling, predisposing, and need factors for healthcare utilization (17). Respondent age, gender, race, years of education, income, insurance status, and geographic region for year one of the panel were abstracted. For each condition, we totaled annual aggregated healthcare expenditures in year one and year two of panel participation. We calculated a headache-specific annual expenditures variable that aggregated costs for condition-linked events including emergency, inpatient, outpatient and office-based medical care, and prescriptions, linked to headache through the events in which they were prescribed. We constructed variables for annual totals of components of headache-related healthcare utilization including ambulatory visits, Emergency Room (ER) visits, inpatient visits, prescriptions, inpatient days, triptan prescriptions, MRI/CT scan usage (from ambulatory care, excluding emergency and inpatient imaging). We also included a compiled Charlson Comorbidity Index (18) for year one for each member of the cohort based on the annual conditions file. Survey design variables, including longitudinal sample weights, pooled primary sampling unit and stratification data, were included for each respondent.
Exposure of interest
We determined the exposure of neurologist involvement with care by examining condition-linked ambulatory care visits identifying specialty of physician seen in year one only. Neurologist involvement was coded as a categorical variable (0/1) based on absence or presence of any neurologist visits.
Statistical analysis
Analyses utilized the MEPS complex sample design (probability weights, stratification, and clustering) for accurate national-level estimates. Descriptive demographic characteristics were determined as a mean (for continuous data) or proportion (for categorical data). All costs were inflated to 2015 US dollars using the Consumer Price Index for medical inflation (19). We further described mean year one and year two headache-related costs stratified across neurologist involvement (total, emergency, ambulatory care and pharmacy) and unadjusted mean differences between the two. We also examined year over year mean differences in constructed healthcare utilization variables (headache-linked ambulatory visits, ER visits, inpatient visits, prescriptions, inpatient days, triptan prescriptions, MRI/CT scan usage) for persons with and without neurologist care in year one.
For our inferential analysis, we performed a multiple (ordinary least squares [OLS]) regression analysis with the outcome of year over year dollar change in expenditures from year one to year two, adjusted for demographic and clinical variables per above. As a sensitivity analysis, we constructed a difference-in-difference linear regression model without survey adjustment using a random effects maximum likelihood estimator for the full year one and year two panel data, with time and treatment indicators and their interaction as the difference-in-difference estimator for comparison to the results of the OLS model. Significance level was set at p = 0.05. The p-values for hypothesis tests for cost and utilization are presented without adjustment for multiplicity. All analyses were performed in Stata 13.0 (StataCorp, College Park, TX).
Subgroup analysis
To evaluate the effect of neurologist care on higher cost patients, we repeated the inferential and descriptive outcomes analysis limited to headache sufferers with greater than median year-one headache related costs. We examined mean differences in healthcare expenditures between year one and year two over the exposure, both unadjusted and adjusted for demographic and clinical variables via multiple OLS regression.
Results
Demographics
A total of 887 patients with headache were extracted from the MEPS data, including 76.7% of (680/887) patients who had headache but no neurologist involvement, and 23.3% (207/887) patients who had a neurologist involved in their care in year one of panel participation (Figure 1). No respondents were excluded due to missing data. Characteristics of the population are summarized in Table 1. The populations were demographically similar, apart from a trend towards low income and public insurance in the no neurologist group and higher income with private insurance in the neurologist group.
Selection design for study, with sample sizes at each stage. MEPS: Medical Expenditure Panel Survey; CCS: Clinical Classification Software. MEPS population demographics. Stratified by neurologist ambulatory care in year one. Estimates are survey adjusted with weighting, clustering, and stratification effects unless otherwise stated.

Expenditures
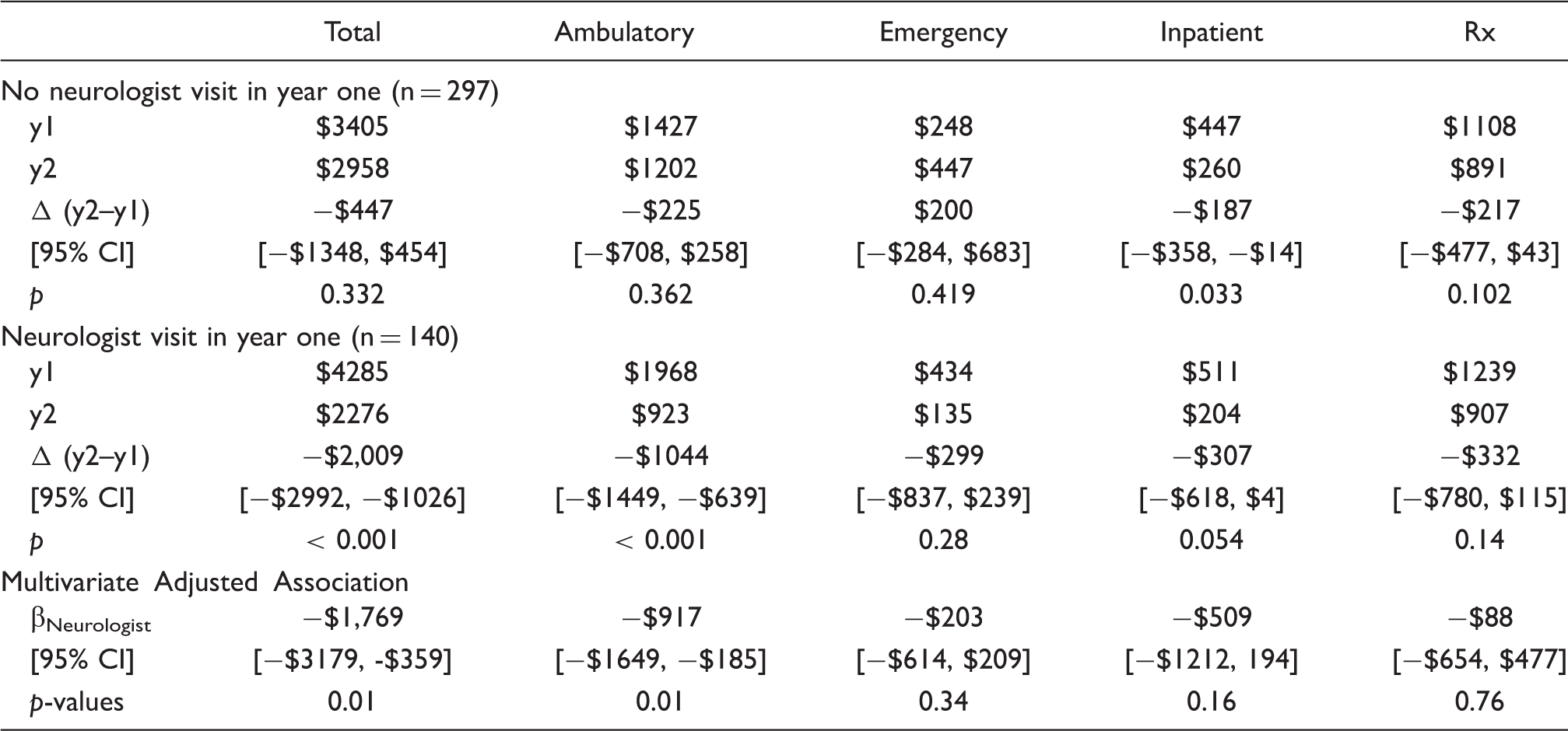
Total expenditures in year one of care demonstrated a higher average cost for respondents seeing a neurologist (Figure 2). When assessing average unadjusted headache-related annual costs over the second year, seeing a neurologist in year one was associated with aggregate cost savings of $1151 (95% CI $449, $1855, p = 0.001). Additionally, in the no neurologist group, headache-related costs rose (save emergency room expenditures) in year two compared with those who saw a neurologist, but not significantly so. In the adjusted analysis, aggregate (−$1579, 95% CI −$2468, −$690, p < 0.001) and ambulatory (−$753, 95% CI −$1160, −$345, p < 0.001) headache-related cost reductions occurred in year two associated with year one neurologist care. Non-significant trends in downward cost reduction were identified in the neurologist group for the emergency room, inpatient stays, and drug treatment variables (Table 2). Sensitivity analysis results for aggregate adjusted costs were largely unchanged in a difference-in-difference model that did not adjust for survey design (difference-in-difference estimator: −$1576, 95% CI −$2411, −$741, p < 0.001.)
Mean healthcare expenditures for headache by category, year one (circle) and year two (arrowhead), by neurologist ambulatory care status (neuro = neurologist ambulatory care in year one (grey), control = no neurologist ambulatory care visits in year one (black)). Adjusted inferential analysis – difference in year two and year one expenditures, association with neurologist visit in year one (βNeurologist).

High cost subgroup − survey adjusted mean year one and year two expenditures in 2015 US dollars, stratified by presence of neurologist year one visit, with adjusted inferential analysis assessing neurologist association with cost changes (βNeurologist).
Utilization
Mean headache-linked utilization difference in year-one (y1) vs. year two (y2) by neurologist visit in year one.

Discussion
We demonstrate the association of neurologist care with headache-related healthcare expenditures and utilization over time using publicly available US data. While headache expenditures for respondents seeing neurologists were substantially higher in year one, expenditures fell dramatically in year two. Headache-related expenditures in the group not exposed to neurologist care remained similar in both years. These findings were echoed in reduced healthcare utilization in the year after neurologist care for MRI/CT and ambulatory care.
Our findings confirm and expand upon previous efforts to detail the involvement of neurologists in the care of headache patients. In a large commercial claims dataset, only 27% of patients with migraine headaches had seen a neurologist in the ambulatory care setting in the same calendar year (11). In a survey of US headache patients, only 15% of respondents diagnosed with chronic migraine had seen a neurologist in the preceding three months (6). In our study of nationally representative data with adult respondents having had at least some headache-related healthcare expenditure for each of two years, neurologists were seen in outpatient and office-based medical visits only 23% of the time in the first year. In each of these studies, only a minority of headache patients visit neurologists in ambulatory care.
Costs attributable to headache have only recently attempted to quantify the effects of specialists on care, instead differentiating between chronic and episodic headaches by expenditures. Analyses utilizing this dichotomy generally note the greater usage of neurologists in chronic migraine as compared to episodic migraine, with costs of chronic migraine care being substantially greater. In a web-based survey of over 3000 persons (International Burden of Migraine Study), chronic migraineurs in the US were four times more likely to see neurologists than episodic migraine sufferers, with three times greater direct health care expenditures (20). In a general population survey in France, chronic headache sufferers were six times more likely to see a neurologist, and direct healthcare costs were 10–50 times greater for chronic than episodic headache (21,22). As part of the assessment of the effect on neurologists in a cross-sectional analysis of 10 million commercially insured persons, average annual claims in migraine patients were 66% greater ($834 vs. $502) when a neurologist was involved (11).
Combining cost and specialist utilization analyses indicates that patients seen by a neurologist may have greater headache severity, with more chronic migraine, consuming more headache-related healthcare and generating greater costs. The question is whether neurologist care can improve clinical outcomes while reducing the cost burden over time. In our year-one data, the group who had seen a neurologist had substantially higher direct healthcare costs attributable to their headache, consistent with prior analyses. They also had a higher number of headache-related ambulatory care visits, more prescriptions, and more imaging.
In considering care trajectories of patients with headache, and especially those with chronic migraine, looking at a period longer than one year is necessary to more fully appreciate the effects of neurologist care on headache-related expenditures and utilization. The reduction from the first to second year headache-related costs was substantial, with annual expenditures achieving parity with controls. We see substantial reductions in ambulatory care visits and less emergency care, prescriptions, and neuroimaging in year two after neurologist care. Our work confirms prior longitudinal analyses of appropriate care in headaches. In a retrospective analysis of 3700 US service members, initiation of daily migraine prophylaxis resulted in prominent reductions in ambulatory care expenditures, emergency room expenditures, and definite migraine-related prescription expenditures totaling greater than $500 in savings over a 180-day period compared to a matched cohort (23). An examination of analgesic overuse headache sufferers in a Danish Headache Center showed that detoxification led to reductions in medication costs of 24% on average and 43% in triptan overusers (24). These latter two studies further suggest mechanisms where neurologists may reduce costs in more severe headache patients, and may explain our findings that patients under the care of neurologists had less ambulatory care and ER visits and lower use of prescription medications and triptans in year two compared to year one.
One criticism of our analysis of costs is that we are witnessing regression to the mean rather than any association of neurologist care. However, we note that the magnitude of the adjusted association with year one care is greatest among patients with higher year one expenditures. In this subset, respondents in the control group had a much smaller reduction in expenditures compared to the group seeing a neurologist in year one ($445 vs. $1977). This led to substantially lower mean year two costs in the neurologist group despite much larger year one costs. While we do not discount that some year over year change may be related to regression to the mean, we assert that neurologist care is independently associated with cost savings.
Our work has implications at multiple levels of healthcare. For insurers intent on developing episodes of care encompassing treatment for chronic conditions in a defined period (25), consideration should be made in ensuring that the longitudinal effects of care are captured on a wider timeframe. Third party payers, both commercial and public, should ensure that risk adjustment algorithms are accurate and predictive for patients with severe and chronic headache, otherwise neurologists may be disincentivized from taking higher severity patients (26). Alternative payment models (27,28) focusing on headache care and the role of neurologists as headache specialists should be encouraged.
There are limitations to our analysis. First, we pooled multiple years of data to increase the sample size, utilizing the longitudinal weighting and pooled variance and stratification variables. Although we include year in the inferential analysis, we did not specifically test for trends in each year as annual data did not have adequate sample sizes to permit such testing. Second, we confined our analysis only to respondents who had at least some headache-related expenditures in both years of the panel, reducing the generalizability of our study to persons who engage healthcare for their headaches, compared to persons that may have headaches but do not seek medical care. Such patients may have less severe headaches, have less of a need to see providers for evaluation and management of their headaches, and hence, not appreciably contribute to the direct cost of headache care. Third, we focus on headache-linked expenses, and do not account for those costs that are not attributable to headache. In this, we are reliant on the structure of MEPS for condition-linked events. Therefore, we suspect that we underestimate cost reductions in total healthcare when factoring in utilization of services that are not directly headache-related. Fourth, we are assessing only the association of any year one exposure to a neurologist on expenditures and utilization in the following year. We do not assess the effect of subsequent years, nor do we assess a dose-dependent effect for multiple visits to a neurologist, or proximity of a neurologist visit to subsequent headache-related healthcare use. MEPS data is de-identified, preventing any linkage prior to or subsequent to inclusion, so we do not know about headache care before or after the study period. Fifth, we utilize the broadest definition of headache in administrative claims data to capture patients seeking headache care rather than parsing migraine versus non-migraine headache care. Most severe primary headaches prompting healthcare use are migraine (29), but our analysis does not exclusively pertain to migraine. Sixth, we acknowledge that our model can only be adjusted for observed variation, and there is very likely unobserved variation between headache patients seen by a neurologist and not seen, including but not limited to sleep, diet, exercise, and other lifestyle effects not captured by MEPS. Lastly, we only analyze direct healthcare costs, and do not include indirect costs such as caretaker burden, lost wages and benefits, absenteeism and reduced productivity (presenteeism), which can be quite substantial among patients with poorly controlled headache pain (20).
In short, our work demonstrates that neurologist involvement with headache care, despite having higher mean expenditures in year one, is associated with substantive reductions in healthcare expenditures and utilization in the subsequent year. We look forward to confirmation of our results in longitudinal analysis of large administrative claims datasets as well as prospective data gathered from registries and elsewhere. Ultimately, these findings should aid in decisions involving reimbursement and access to care within health systems among third party payers, and for policymakers to improve the lives and health of headache sufferers.
Public health relevance
Patients who see a neurologist for headache have higher initial headache-related expenditures. Patients who saw a neurologist have similar headache-related expenditures in the year following the initial neurologist visit to patients who did not see a neurologist. For headache patients with greater than average initial costs, those who saw a neurologist in the first year had lower costs in the subsequent year.
Footnotes
Acknowledgements
John Ney takes full responsibility for the data, the analyses and interpretation, and the conduct of the research; John Ney had full access to all of the data, and has the right to publish the results of this research.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: John Ney and Jason Sico are employees of the United States Government. This manuscript was not a term of their employment, nor did they receive any compensation for the manuscript. John Ney has been a consultant for AxelaCare, a home intravenous infusion company, SpecialtyCare, a surgical services company, and Ceribell, an EEG device company. Jason Sico served on the Medical Advisory Board for Acorda Therapeutics and receives grant funding from the Veterans Affairs administration (CDA 11-262, PPO 15-404). Brian Callaghan receives grant funding from NINDS (K23 grant [NS079417]). He performs medical consultations for Advance Medical, consults for a PCORI grant, and performs medical legal consultations. Brandon Magliocco is an employee of the AAN. Brad Klein reports speaking honoraria for Allergan, Avanir, Depomed, Pernix, Teva, US Worldmeds, and the American Academy of Neurology; research grants for Alder, Allergan, and Eli Lilly and Company; and a shareholder stake in Appsbydocs. Greg Esper reports no disclosures.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.