
Abstract
The objective of this study was to measure the self-reported effect of acute migraine and its treatment on paid work and productivity loss. Patients self-administered a questionnaire in which the impact of a recent migraine on paid work and productivity activities was assessed. We included the questionnaire in a randomized, double-blind, placebo-controlled, crossover, out-patient study designed to examine the safety and efficacy of rizatriptan (5-HT1B/1D receptor agonist) 10 mg p.o. in patients treating four separate migraine attacks. A total of 407 patients, aged 18–65 years, suffering from moderate to severe migrainous headaches was studied. Patients receiving rizatriptan compared with placebo reported 0.7 fewer hours (P < 0.01) of paid worked missed due to absenteeism, 0.4 fewer hours (P < 0.05) of productive time lost on the job, and 1.1 fewer total hours (P < 0.01) of work loss per migraine attack. Rizatriptan compared with placebo significantly reduced migraine-related work loss associated with absenteeism and decreased effectiveness on the job.
Introduction
Migraine is a neurologic disorder that presents as attacks of severe, unilateral, pulsating headache associated with nausea, vomiting, photophobia and phonophobia. These negative health effects are often disabling to the migraineur, resulting in decreased productivity while at work and/or absenteeism from work (1, 2). Migraine-related work loss accounts for the majority of the economic burden of migraine on society (3). This economic burden has been estimated to range from $5 billion to $17 billion a year in the USA (4–6).
To reduce or eliminate the pain and discomfort associated with migraine, abortive pharmacologic therapy has been shown to be effective in migraineurs (7, 8). Abortive pharmacologic therapy has also been suggested to be effective in reducing migraine-related work and productivity loss (1). In this study we present data on work and productivity loss which was collected as part of a randomized, double-blind clinical trial comparing rizatriptan 10 mg, a new 5-HT1B/1D agonist, with placebo in the acute treatment of multiple migraine attacks.
The clinical results of that trial have been previously published (9). In summary, rizatriptan 10 mg was shown to be highly effective in the treatment of acute migraine with onset of action as early as 30 min (9). Additionally, the efficacy of rizatriptan 10 mg was maintained when used to treat multiple discrete migraine attacks. Finally, this trial demonstrated that rizatriptan 10 mg reduced functional disability. We extend these findings here by examining the effect of migraine and its treatment on paid work and productivity loss.
Patients and methods
The clinical trial
Work and productivity loss data were collected in a randomized, double-blind, multicentre clinical trial designed to assess the efficacy of rizatriptan 10 mg vs. placebo in the treatment of migraine. The objectives of the trial were: (i) to confirm the efficacy of rizatriptan 10 mg in the treatment of a first migraine attack, and (ii) to examine the safety and tolerability of rizatriptan after treatment of multiple migraine attacks. Men and women between 18 and 65 years of age with a 6-month history (1–8 attacks per month) of suffering from acute moderate (grade 2) or severe (grade 3) migraine with or without aura based on International Headache Society (IHS) criteria were enrolled in the study. All patients gave written informed consent before entering the study and the protocol was approved by local investigational boards of the 23 investigative sites that participated in the study. These 23 sites were located across the USA and comprised both academic centres and private practices with research experience. Patients were randomly assigned to one of five treatment sequences as shown in Table 1. Patients who received initial treatment of rizatriptan 10 mg for any given attack received rizatriptan for treatment of first and second headache recurrences within 24 h. Patients who received initial treatment of placebo for any given attack were given placebo for treatment of first and second headache recurrences within 24 h. Escape analgesia/antiemetics were permitted in non-responders (i.e. patients not achieving pain relief) beginning 2 h after the initial dose.
Sequences of treatments in each group in the study

P, Placebo; R, rizatriptan 10 mg.
The primary endpoint was pain relief (change in headache severity from 2 or 3 to 0 or 1) at 2 h during the first migraine attack period. Patients rated headache severity on a four-point scale (0 = no headache, 1=mild pain, 2=moderate pain, 3=severe pain), functional ability on a four-point scale (0=normal, 1=mildly impaired, 2=severely impaired, 3=unable to do activities, 4=requires bed rest), and presence of vomiting, nausea, phonophobia, and/or photophobia (0 = no, 1 = yes) immediately before initial dose and at 0.5, 1, 1.5, 2, 3, and 4 h thereafter for each attack. Work and productivity loss data were collected by questionnaire 24 h after onset of treatment or when the headache ended (10). Specifically, only patients who worked for pay or planned to work for pay during the headache completed the following questions:
How many total hours of paid work did you miss because of your most recent migraine headache or migraine headache treatment?
During your most recent migraine headache, how many hours altogether did you work while you had symptoms due to the headache or its treatment?
How would you rate your effectiveness on the job during the period you had the migraine headache? (100% means you are at your best and 0% means you are at your worst)
In addition, patients were asked to describe how much difficulty they had:
doing things that required their body (e.g. walking, bending, reaching);
concentrating on their work (e.g. not being distracted);
controlling irritability toward the people they worked with (e.g. co-workers);
doing their work carefully (e.g. without making mistakes), and finishing all their work (e.g. not taking unfinished work home).
Patients were asked to respond on a scale of 0–5, where 0 represented none and 5 not done—can't do at all. Finally, patients were asked how much of the time they had difficulty performing daily activities on a scale of 1–6, where 1 represented all the time and 6 none of the time.
Statistical analysis
Work loss due to absenteeism was measured as the self-reported estimates provided by the patient. Work loss attributable to lower productivity on the job was estimated by multiplying the number of hours worked with a migraine by one minus the percent effectiveness (divided by 100) during work. These methods were based on work loss constructs utilized in previous migraine studies (11–14). Work and productivity loss data were analysed from all completed questionnaires. A linear mixed effects model using S-PLUS 4.5 was estimated with patient as a random effect, headache, treatment, and carryover as fixed effects. In addition, we included as covariates all baseline migraine symptoms (i.e. severity, functional ability, nausea, vomiting, photophobia, and phonophobia) as well as age, gender, and time of initial treatment. A backwards elimination procedure was used to evaluate fixed effects prior to the assessment of treatment differences. Given the non-normality of the response variables, 95% confidence intervals were constructed using a bootstrap resampling methodology (15) utilizing S-PLUS 4.5.
Results
A total of 407 patients treated 1365 headaches across all four periods of the study. Of these patients 63% (257/407) reported working for pay or planning to work for pay when treating a headache. Twenty percent (81/407) of these patients treated only a single headache when they worked for pay or planned to work for pay, while 19% (77/407), 14% (55/407), and 11% (44/407) treated two, three, and four headaches, respectively, when they worked for pay or planned to work for pay. Eighty-one percent of these patients were female and the mean age was 41 years.
Collectively, patients reported working for pay or planning to work for pay during 42% (576/1365) of the headaches treated. This was consistent across all four periods of the study: 43% (174/407) in period 1, 41% (150/367) in period 2, 38% (127/335) in period 3, and 40% (125/313) in period 4. Table 2 summarizes baseline migraine symptoms by treatment group averaging across all headaches where patients worked for pay or planned to work for pay. The effect of these covariates on work loss was evaluated prior to the assessing the effect of treatment on work loss. Baseline functional ability was found to have the greatest influence on work loss. Specifically, patients who had less functional ability at baseline experienced greater work loss. In addition, we found that the presence of vomiting, the time of the initial treatment, and gender influenced work loss. Patients who were vomiting at baseline and females experienced greater work loss than those who were not vomiting and males, respectively. Moreover, patients who treated their headache earlier in the day tended to have greater work loss.
Baseline migraine symptoms by treatment group across all headaches where patients worked for pay or planned to work for pay

Analyses of the effect of treatment on work and productivity loss were performed averaging across all four attacks given that, after adjustment for covariates and treatment, no differences were detected across attacks for any response variable. The results of these analyses adjusting for baseline characteristics are shown in Table 3. For headaches treated with placebo, the average number of hours of work loss due to absenteeism was 2.2 h per migraine attack. Rizatriptan, however, significantly reduced the average number of hours of work loss due to absenteeism by 0.7 h per migraine attack. Patients taking rizatriptan compared with placebo reported working 4.2 h vs. 4.7 h with symptoms. However, effectiveness on the job was 4.5% greater among patients taking rizatriptan. This increase in effectiveness on the job combined with the reduction in number of hours worked with migraine resulted in 0.4 fewer hours of productive time lost per migraine attack, favouring rizatriptan. Altogether, rizatriptan significantly decreased the total number of hours of work loss by 1.1 h per migraine attack treated compared with placebo. Figure 1 depicts a summary of the work loss results.

Paid work and productivity loss due to migraine by treatment group 95% confidence intervals. All treatment differences are statistically significant (see Table 3). ∗Hours worked with migraine multiplied by one minus percent effective in paid work performance. †Work hours missed plus hours worked with migraine multiplied by one minus percent effective in paid work performance. •, Rizatriptan; ▪, placebo.
Paid work and productivity loss due to migraine
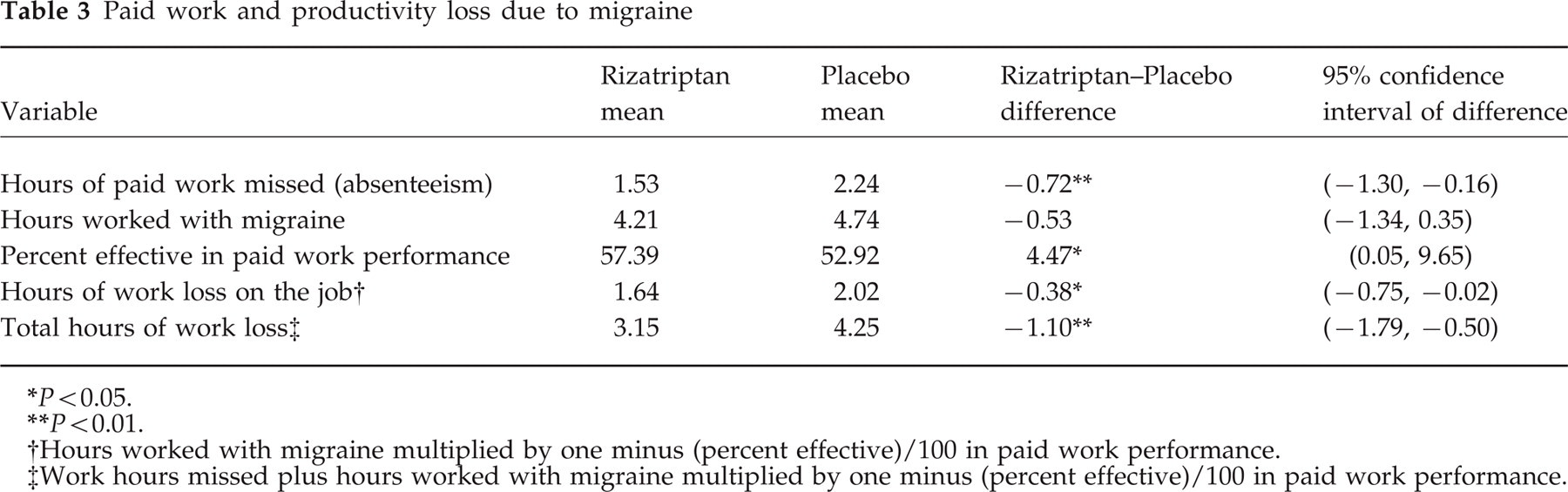
P < 0.05.
P < 0.01.
Hours worked with migraine multiplied by one minus (percent effective)/100 in paid work performance.
Work hours missed plus hours worked with migraine multiplied by one minus (percent effective)/100 in paid work performance.
To gain a better understanding of how migraine headaches affected the patient's ability to work, we asked patients to describe the difficulties encountered while working with a migraine. In general, patients reported less difficulty working with a migraine when the headache was treated with rizatriptan. These results are shown in Table 4. Finally, patients taking rizatriptan reported less time having difficulty performing regular daily activities (P = 0.004) than patients taking placebo.
Migraine work difficulty

Response scale: 0, none; 1, slight amount; 2, some; 3, quite a bit; 4, a great deal; 5, can't do at all.
Discussion
Given the debilitating effects of migraine headaches, effective treatment that relieves the pain and associated symptoms should also be effective in reducing work loss among those experiencing a migraine while at work or prior to going to work. The results of this study indicate that rizatriptan 10 mg compared with placebo significantly reduced migraine-related work loss by a little over 1 h per migraine attack. This finding was consistent across all four attacks and was supported by other qualitative productivity measures. For instance, patients taking rizatriptan reported less difficulty doing things that required the use of their body (e.g. walking, bending, reaching and lifting). While other studies have suggested that abortive oral pharmacologic therapy can reduce work loss (16), none of these studies was randomized, double-blind, or placebo-controlled. Nonetheless, the reductions in work loss (0.5–2.4 h) observed in these studies were similar to the reductions observed in this study.
One of the challenges of this finding is translating an observed reduction in work loss into economic terms (i.e. costs). Clearly this translation depends on the economic perspective one adopts in the evaluation. The Panel on Cost-Effectiveness in Health and Medicine has recommended the use of a targeted average age–gender-specific wage rate for the societal perspective (17). Alternatively, the Panel has suggested using a more equitable average market wage rate. Adopting this latter approach and based on an average hourly wage pay of an employee in the USA as reported by the Bureau of Labor Statistics (18), we found that the cost associated with the observed reduction in work loss would be approximately $16 per migraine attack. What is not clear, however, is how meaningful this reduction is in terms of costs for other economic perspectives such as those of an employer. The magnitude will depend on the type of job and how migraine leads to absenteeism and decreased production on the job. For some jobs, absenteeism can be cost additive to the employer. For example, absenteeism for a hospital nurse can cost a hospital more as a float or agency nurse is brought in as a temporary replacement. In contrast, a manager may miss work because of a migraine but make up the missed work the following day or the work may be made up by another worker covering for the manager in his or her absence.
A unique feature of this analysis was the examination of the effect of baseline migraine symptoms and characteristics on work loss. Our analyses indicated that functional ability had the greatest influence on work loss. For instance, patients who were disabled at baseline (e.g. required bed rest) or were vomiting because of their migraine tended to experience greater work loss than those were not disabled or vomiting. Similar results were found for those who treated their headache earlier in the day or were female. One implication of these findings is that future studies that examine the effect of treatment on work loss should account for the effect of these variables in both the design of the study and the analysis.
A potential limitation of this study as well as all the other studies that examined the effect of abortive migraine therapy on work loss is that work loss is a self-reported measure. The validity of self-reported work loss in terms of concordance with actual work records and output, however, is difficult to ascertain. This can only be done by conducting studies of work loss and absenteeism in collaboration with employers. Although there is precedent for conducting a study with employers (13), collecting actual work loss records can be challenging due to management and employee concerns, union rules, accuracy, and how or whether work loss records are captured by employers. Given the recall period in this study was 24 h, we believe the amount of bias due to recall of work loss due to absenteeism may not be significant.
In conclusion, rizatriptan compared with placebo not only offers clinical benefits in terms of pain relief and decreased functional disability but may also offer significant economic benefits. In particular, rizatriptan compared with placebo significantly reduced migraine-related work loss associated with absenteeism and decreased effectiveness on the job among patients who worked or planned to work during their migraine.
Footnotes
Acknowledgement
This study was funded by Merck Research Laboratories.