
Abstract
Objective
This study aimed to identify the potential subgroups of migraines based on the patterns of migraine associated symptoms, vestibular and auditory symptoms using latent class analysis and to explore their characteristics.
Method
A total of 555 patients with migraine participated in the study. Symptoms such as nausea, vomiting, photophobia, phonophobia, osmophobia, visual symptoms, vestibular symptoms (dizziness, vertigo), and auditory symptoms (tinnitus, hearing loss, aural fullness) were assessed. Latent class analysis was performed to identify subgroups of migraines. Covariates such as gender, age of migraine onset, frequency of migraine attacks per month, and family history were also considered.
Results
The analysis revealed four latent classes: the Prominent Vestibular; Prominent Nausea; Presenting Symptoms but not prominent or dominant; and Sensory Hypersensitivity groups. Various covariates, such as gender, age of migraine onset, and frequency of migraine attacks, demonstrated significant differences among the four groups. The Sensory Hypersensitivity group showed the presence of multiple sensory symptoms, earlier age of migraine onset, and higher proportion of females. The Prominent Vestibular group had the highest probability of dizziness or vertigo but lacked the presence of auditory symptoms. The Prominent Nausea group exhibited prominent nausea. The Presenting Symptoms but not prominent or dominant group comprised individuals with the highest migraine attacks per month and proportion of chronic migraine.
Conclusion
This study identifies four subgroups of migraines based on the patterns of symptoms. The findings suggest potential different but overlapped mechanisms behind the vestibular and auditory symptoms of migraine. Considering the different patterns of migraine-related symptoms may provide deeper insights for patients’ prognosis and clinical decision-making.
Introduction
Migraine is a prevalent neurological disorder that affects approximately 14–15% of the world's population (1), characterized as a recurrent, throbbing and often severe headache. It is now understood to be a disorder that affects multiple sensory processes (2). Individuals with migraine commonly experience altered sensory input thresholds (3). These changes can result in hypersensitivity in response to various stimuli, such as light or sound, and lead to symptoms such as photophobia (sensitivity to light) and phonophobia (sensitivity to sound).These thresholds may vary between different stages of migraine and subgroups, such as chronic and episodic migraine (4).
Another aspect of migraine lies in its heterogeneity, which allows for subcategories such as migraine with aura and migraine without aura. Vestibular migraine, outlined in the appendix of the International Classification of Headache Disorders, 3rd edition (ICHD-3), is characterized by the presence of vestibular symptoms in association with migraine (5). Recent studies suggest that vestibular migraine may have a polygenic nature, as evidenced by the identification of multiple genetic loci associated with the condition, despite the absence of pathogenic mutations in single candidate gene analyses (6). However, associated symptoms of vestibular migraine, such as auditory manifestations, have been underrecognized (7). In addition to vestibular disturbances, there are reports linking migraine with various auditory symptoms, such as tinnitus, hearing loss and aural fullness (8). Previous studies have shown a close relationship between vestibular and auditory symptoms, with the prevalence of auditory symptoms in patients with vestibular migraine varying from 38% (9) to 61.5% (10). Yet, these auditory symptoms have not been incorporated into the diagnostic criteria for vestibular migraine as they are considered non-specific and common in other vestibular disorders (11). Auditory symptoms have also been observed without the presence of vestibular symptoms, leading to the proposed entity of cochlear migraine (12). Suggestions have emerged advocating for the investigation of the effects of modulating the trigemino-vascular system (TVS), potentially through the inhibition of Calcitonin Gene-Related Peptide (CGRP) in the inner ear and evaluating the subsequent impact on the neuroepithelium in both the auditory and vestibular systems, which may shed light on the pathophysiology of vestibular migraine (7). Overall, the etiology of vestibular-auditory symptoms associated with migraines remains unclear, and it is still uncertain whether these symptoms originate from distinct entities. However, studies have shown a tendency for certain symptoms to occur together in specific conditions. For example, photophobia (13) and tinnitus (14) have been frequently reported in vestibular migraine patients. In theory, if the occurrence of symptoms is entirely random, any possible combination of these symptoms could be observed. We postulate that this phenomenon can be attributed to the diverse characteristics exhibited by individuals with migraine, where the symptoms serve as external manifestations of these characteristics.
The Latent Class Analysis (LCA) is a probabilistic modeling algorithm used to identify diverse subgroups or subtypes within multivariate categorical data. This method assumes the existence of finite unobserved classes within a population, which typically have shared external characteristics (15). Latent class analysis (LCA) had been utilized in migraine research, demonstrating its potential to identify distinct subgroups in numerous studies. In a 2008 study, LCA was employed to discern the potential differentiation between migraine with aura and migraine without aura using clinical and genetic data (16). By 2018, LCA was utilized to identify subgroups of migraine based on comorbidity (17). Most recently, in 2021, LCA was employed to classify migraine subtypes using clinical data from a nationwide population-based study in Korea (18). However, migraine symptom analysis in LCA has been restricted to diagnostic criteria such as nausea, vomiting, photophobia, and phonophobia. Additionally, these symptoms were analyzed alongside other clinical features in a singular analytic way.
The evolution of LCA methodology has led to significant improvements over the one-step covariate analysis – an approach that included covariates directly in the model during analysis but may have resulted in flawed models and has since been replaced with newer approaches, including a novel three-step approach (15). Briefly, the three-step approach involves conducting a standard LCA using only the latent class indicators in the initial step. Subsequently, the most likely class variable is derived from the posterior distribution of the LCA in the first step, along with the calculation of classification uncertainty rates. In the final step, the most likely class variable is treated as a latent class indicator variable with prefixed uncertainty rates and included with the auxiliary variable. Further details on this methodology can be found in the article by Bakk and colleagues (19).
This study aims to utilize the updated methodology of LCA and the sensory threshold understanding of migraine symptoms by applying latent class analysis to vestibular-auditory associated symptoms in migraine patients. The objective is to identify potential subgroups of migraines and calculate the probability of symptoms in each subgroup, which can be understood as sensory thresholds. The findings are expected to offer valuable insights into the underlying pathophysiological mechanisms.
Method
Participants
This cross-sectional study was conducted at the Headache Clinic of the First Affiliated Hospital of Chongqing Medical University from June 2019 to June 2023, involving participants who voluntarily sought medical diagnosis or treatment at the hospital and were informed about their participation. A total of 573 patients were included in the study, meeting the following inclusion criteria: 1) fulfillment of diagnostic criteria for migraine or probable migraine according to the International Classification of Headache Disorders, Third Edition (ICHD-3) (20); 2) aged between 18 and 65 years at the time of enrollment; 3) no known history of otologic, severe neurological or psychiatric disorders. The exclusion criteria consisted of: 1) 14 participants with less than one year of migraine duration; 2) four participants with a migraine frequency of less than once per month. Ultimately, a total of 555 eligible patients were included in this study.
Indicators
The symptoms analyzed for latent class analysis were as follows. Nausea, vomiting, photophobia, and phonophobia, which were selected due to their frequent occurrence and recognition as diagnostic criteria for migraines according to ICHD-3. Vestibular symptoms, as defined by the International Classification of Vestibular Disorders (ICVD), included two commonly reported symptoms: dizziness and vertigo. Additionally, visual symptoms such as blurring or flashing lights were incorporated in the analysis as it is a diagnostic criterion for definite vestibular migraine defined by the Bárány Society and the International Headache Society (21). Moreover, tinnitus, hearing loss, and aural fullness were included based on their close association with migraines as auditory symptoms (22). Finally, osmophobia was included in the analysis due to its established links with both migraine (23) and vestibular migraine (24). Notably, allodynia was not included in this study as it has been found to be associated with symptoms such as nausea and vomiting during migraine attacks, as well as phono-photophobia and osmophobia (25,26), which would introduce collinearity and possibly lead to invalid result.
Covariates
The covariates selected for this study are gender, age of migraine onset, frequency of migraine attacks, and family history of headache and dizziness. Literature suggests that female patients are more frequently affected by vestibular migraine (27). However, regarding auditory symptoms, two large cross-sectional studies have found no gender difference (28,29). Hence, gender has been included as a covariate to investigate its influence on vestibular auditory symptoms. An additional covariate to be incorporated is the age of migraine onset, as previous research has revealed that vestibular symptoms vary with the age of onset (30). Furthermore, family history is an important factor to consider in relation to age of onset, as previous studies have linked it to both sex and onset age (31), as well as the frequency of migraines (32) and vestibular symptoms (33). Therefore, this study will consider all these covariates.
Data collection
All participants underwent face-to-face interviews conducted by experienced headache clinicians. A semi-structured questionnaire was used to collect information on participants’ age, gender, headache characteristics, symptoms experienced during the ictal phase of most attacks, presence of medication overuse, family history of migraine and dizziness. Headache characteristics included the age of headache onset, duration of migraine history, and the frequency and severity of headache attacks. The symptoms were assessed using the closed-ended question for higher sensitivity (34): “Do you experience any of the following symptoms during the ictal phase in most of your migraine attacks: nausea, vomiting, sensitivity or avoidance to light, sensitivity or avoidance to sound, sensitivity or avoidance to odor, dizziness, vertigo, ringing in the ears, hearing loss, feeling of fullness in the ears, or visual disturbances such as blurred vision?” In addition to differentiating between dizziness and vertigo, participants were encouraged to provide a detailed description of their vestibular symptoms. Specifically, regarding dizziness, participants were asked about if they experienced a disturbed spatial orientation without a false or distorted sense of motion, with question like “When you feel dizzy, do you also have a sense that you or your environment is moving or spinning, or is it more like off-balance?”. With vertigo, we check for an internal feeling of self-motion when no motion is present or a distorted sense of movement during normal movement, with questions like “Would you describe the sensation more as feeling unsteady on your feet or as if you are moving when you are not?” Each symptom was coded as either 1 (present) or 0 (absent). The final diagnosis of migraine subtypes was determined according to the ICHD-3 and ICVD classifications and was reviewed by an experienced senior headache specialist.
Latent class analysis
We employed Mplus version 8.3 to construct the latent class model. Initially, the latent class models were fitted using only the indicators, which in this study are the symptoms. The selection of the optimal number of classes was based on the Akaike Information Criterion (AIC), Bayesian Information Criterion (BIC), sample-size adjusted BIC (SABIC), and Vuong-Lo-Mendell-Rubin likelihood ratio test (VLMR-LRT). The AIC and BIC serve as measures of model fit and complexity, while SABIC is a modification of BIC that accounts for sample size to ensure the selection of a model that not only fits the data well but also generalizes to a broader population. Generally, lower values of AIC, BIC, and SABIC are preferred, indicating better fit. The VLMR-LRT is a statistical test used in LCA to assess whether adding an extra latent class significantly improves the model fit compared to a model with one fewer class; a value above 0.05 indicates no significant difference. The model progression initially starts with one latent class, then proceeds to two latent classes, and continues until the point where the AIC, BIC, and SABIC reach their lowest values, or the VLMR-LRT is insignificant (15,35). After determining the optimal number of latent classes, we calculated the probabilities of each symptom for each class, as well as the class probabilities for each participant. Next, we assigned each participant to a class based on their highest class probability. The covariates are analyzed using the 3-step method, as previously described, utilizing the built-in function ‘R3STEP’ in the Mplus software (36). This involves creating the most likely class variable using the latent class posterior distribution obtained during the first step, and subsequently regressing the most likely class on the covariates, while considering the misclassification in the second step. Figure 1 provides a summary of the study's design.

Overview of the study.
Results
Selection of optimal number of latent classes
We fitted six different latent class models ranging from one class to six classes. Table 1 summarizes the values of AIC, BIC, SABIC, VLMR-LRT of each model, as well as the count and size of the smallest class. Based on the p-value from VLMR-LRT, we found no statistical differences between subsequent models and the previous one starting from the five-class model (p = 0.061), meaning that there is no significant improvement after the four-class model. Comparing the AIC, BIC, and SABIC values of the remaining four models, we found that the four-class model is superior, with the lowest AIC and SABIC values, while the BIC value ranks second lowest and it did not have a class that is extremely small. Considering all the aforementioned factors, we selected the four-classification model as the optimal number of latent classes.
Model fit statistics of latent class analysis.

AIC = Akaike information criterion; BIC = Bayesian information criterion; SABIC = sample-size adjusted BIC; VLMR-LRT = Vuong-Lo-Mendell-Rubin likelihood ratio test.
Characteristics of four classes
After determining that a four-class classification was optimal, we further plotted the radar graphs for symptoms probabilities of each class, as shown in Figure 2. After classifying each participant according to their class probabilities, we examine the intergroup differences within the classes, as summarized Table 2. The significant results were further plotted in Figure 3.
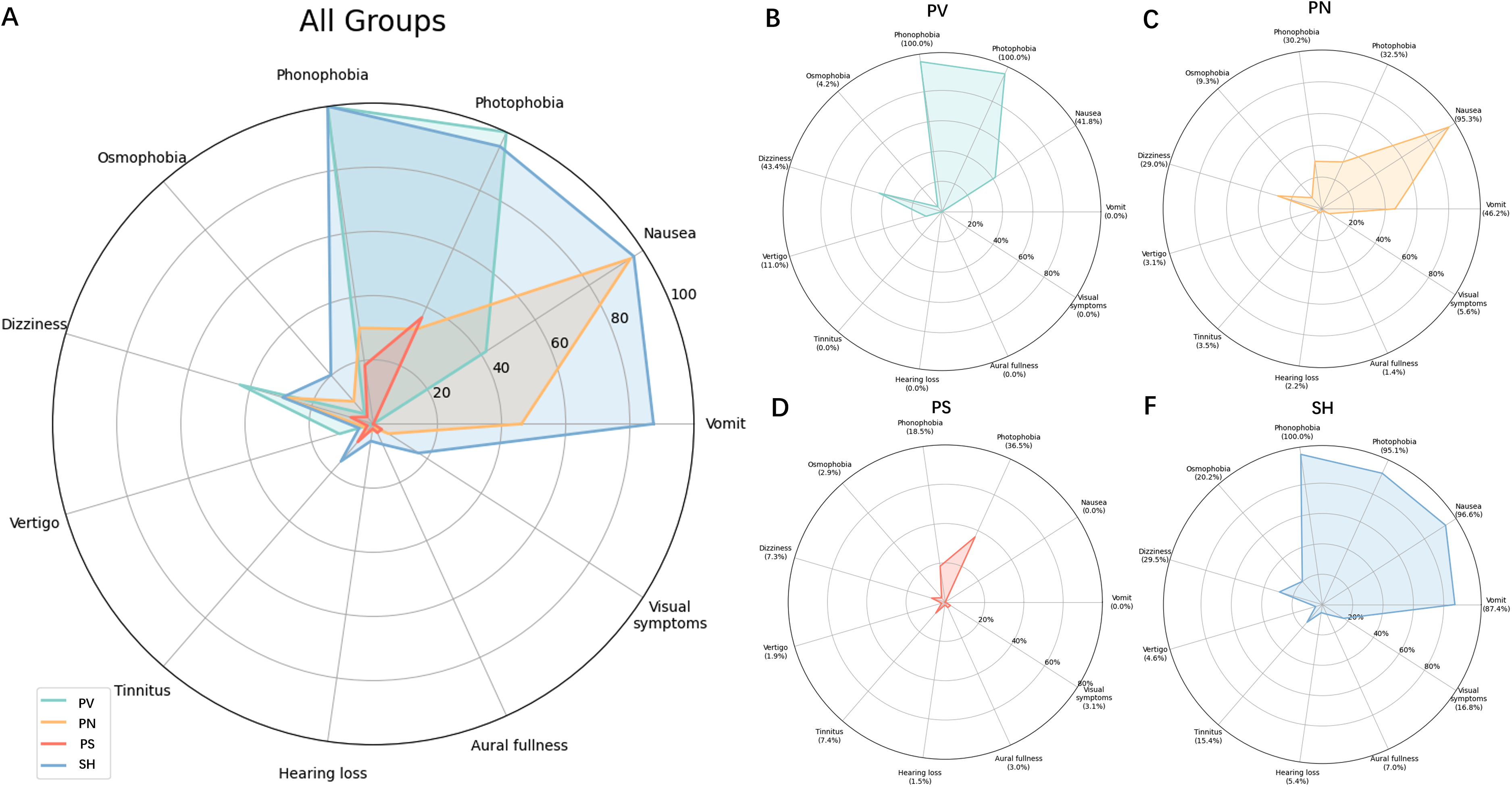
Radar plot symptoms probability in all groups and in separate. PV = prominent vestibular group; PN = prominent nausea group; PS = presenting symptoms but not prominent or dominant group; SH = sensory hypersensitive group.

Variables with significant differences among four group. PV = prominent vestibular group; PN = prominent nausea group; PS = presenting symptoms but not prominent or dominant group; SH = sensory hypersensitive group.Turkey's honest significant difference (Tukey's HSD) method was utilized for conducting post-hoc analysis of numeric variables. The Family-wise error rate was set at 0.05 to account for multiple comparisons. The significance levels of the adjusted p-values were denoted by varying numbers of *.*:<0.05;**:<0.01;***:<0.001;****:<0.0001.
Demographics and ictal phase symptoms of total participants and four latent classes.
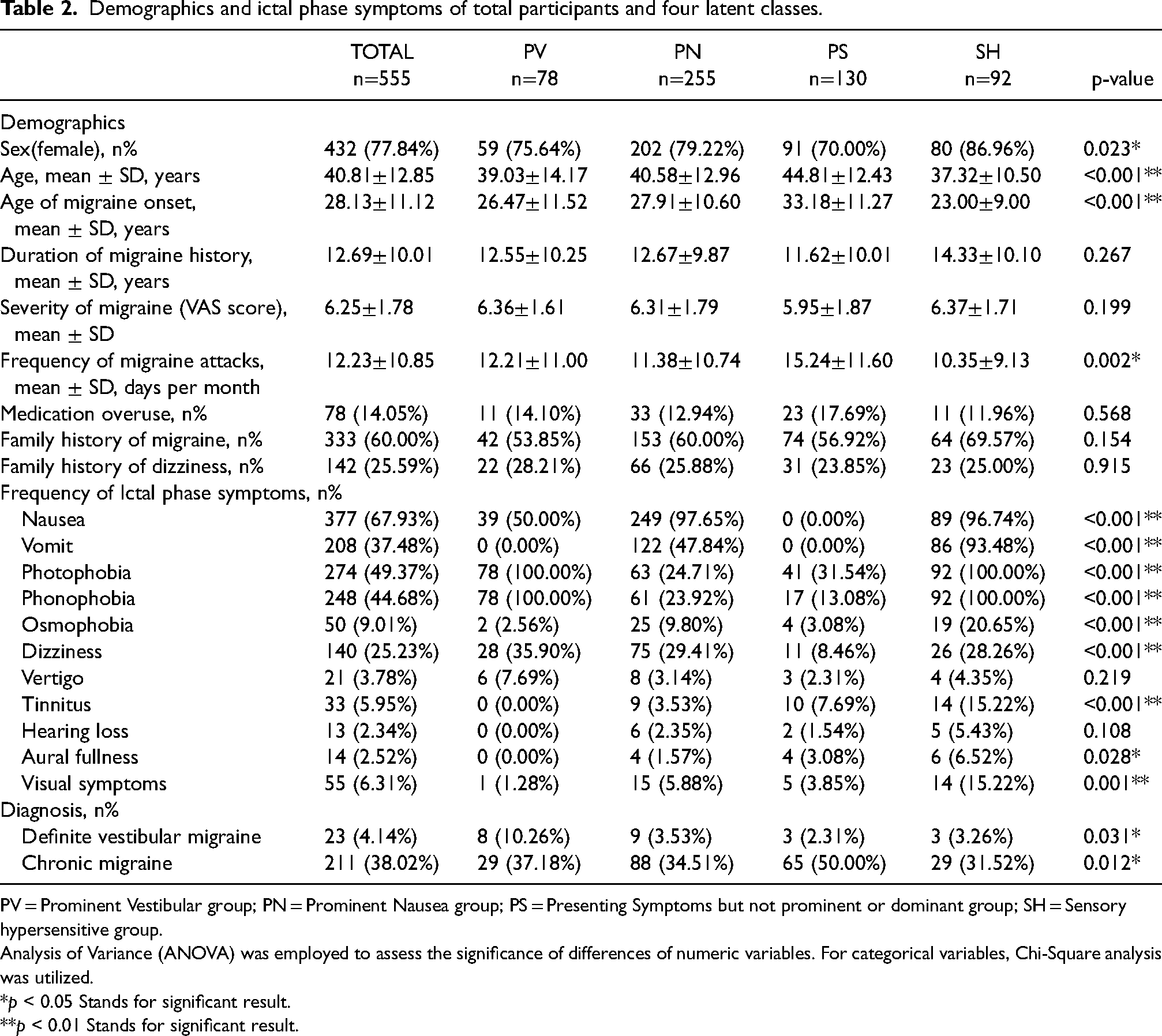
PV = Prominent Vestibular group; PN = Prominent Nausea group; PS = Presenting Symptoms but not prominent or dominant group; SH = Sensory hypersensitive group.
Analysis of Variance (ANOVA) was employed to assess the significance of differences of numeric variables. For categorical variables, Chi-Square analysis was utilized.
*p < 0.05 Stands for significant result. **p < 0.01 Stands for significant result.
Patients assigned to latent class one (14%, n = 78, Figure 2(b)) exhibit a high probability of photophobia and phonophobia, accompanied by the highest probability of dizziness, vertigo, and the lowest probability of auditory symptoms. Latent class two (45%, n = 255, Figure 2(c)) shows the second highest probability of nausea, but other symptoms are less notable. Latent class three (24%, n = 130, Figure 2(d)) exhibits a low probability of all symptoms, with no symptoms exceeding a 40% probability. Latent class four (17%, n = 92, Figure 2(f)) has the highest probability of nausea, vomiting, phonophobia, osmophobia, auditory symptoms and visual symptoms, along with the second highest probability of dizziness vertigo, and photophobia. Based on these findings, we have renamed the classes as follows: PV (Prominent Vestibular) group to refer to latent class one, PN (Prominent Nausea) group to refer to latent class two, PS (Presenting Symptoms but not prominent or dominant) group to refer to latent class three, and SH (Sensory Hypersensitive) group to refer to latent class four.
The intergroup differences revealed significant variations among the four groups in terms of gender, age, onset age of migraine, frequency of migraine attacks per month, and the diagnosis of definite vestibular migraine and chronic migraine. Post-hoc analysis indicated that the PS group had the highest mean age, onset age of migraine, most frequent migraine attacks per month, and higher proportion of patients with chronic migraine. In contrast, the SH group exhibited the youngest mean age and onset age of migraine, as well as a higher percentage of females. Additionally, the PV group exhibited a higher percentage of individuals diagnosed with definite vestibular migraine. There were no significant differences observed among duration of migraine history, severity of migraine attacks, medication overuse, and the family history of both migraine and dizziness.
Incorporating covariate with three-step approach
We analyzed the impact of covariates on latent class analysis using a three-step approach. The results of the multinomial logistic regression can be found in Online Supplemental Table 1. We virtualized the covariates impact on class probability in Figure 4. It was found that a later onset of migraine increased the probability of belonging to the PS group in comparison to the other three groups, which is depicted in Figure 4(d). The odds ratios were 2.298(95 CI [1.067:4.943], p = 0.008), 1.622(95 CI [1.161:2.267], p < 0.001), and 2.880(95 CI [1.796:3.964], p < 0.001) with the PV, PN and SH group as the reference respectively. In contrast, later onset of migraine decreased the probability of belonging to the SH group, with an odds ratio of 0.564(95 CI [0.382:0.746], p = 0.008) and 0.347(95 CI [0.216:0.478], p < 0.001) with the PN and PS group as the reference respectively. Furthermore, a higher frequency of migraine attacks increased the risk of belonging to the PS group, as indicated in Figure 4(e), with odds ratios of 1.343(95 CI [1.065:1.693], p = 0.011) and 1.464(95 CI [1.201:1.785], p = 0.019) with the PN and SH group as the reference respectively. Gender, the family history of both migraine and dizziness did not demonstrate significant results in four classes. However, a notable tendency is observed in Figure 4(a): being male correlates with a decreased probability of being in the SH group. Additionally, Figure 4(b) presents an elevated probability of being in the PV group for individuals with a family history of dizziness. Lastly, Figure 4(c) shows that a positive family history of headache increases the likelihood of an SH group classification.

Effects of covariates on group probabilities in multinomial logistic regression. PV = prominent vestibular group; PN = prominent nausea group; PS = presenting symptoms but not prominent or dominant group; SH = sensory hypersensitive group.
Discussion
In this study, we conducted latent class analysis on the common symptoms associated with migraines, as well as the vestibular and auditory symptoms. Our analysis revealed the presence of four latent classes, the PS, PV, PN and SH group. The PN group appeared to be a less severe version of SH groups, exhibiting reduced probability of symptoms compared to SH group besides nausea. Given the intricate etiology of chronic migraine (37), which accounts for a substantial proportion (50%) of the PS group, and the minimal probability of vestibular-auditory symptoms within, we have opted not to delve into the PS group in this study. As a result, the focus of our discussion will primarily be on the SH and PV groups, where the most pronounced characteristics were observed.
The SH group had a higher proportion of female patients. Female migraine patients are more susceptible to accompanying symptoms of migraine such as vomiting, nausea, photophobia and phonophobia (38). A recent genome-wide association study (GWAS) revealed that rs146094041 in the Estrogen Related Receptor Gamma (ESRRG) gene is associated with the early onset of migraine in the Chinese Han population (39). The ESRRG gene belongs to the estrogen receptor-related receptor (ESRR) family and has been found to participate in several brain activities, such as regulating energy homeostasis, social behaviors, and memory and learning abilities (40). Additionally, ESRRG has been found to be closely related to hearing loss in both mice and humans, particularly in females (41), which may explain that vestibular migraine patients with auditory symptoms tend to have younger onset age of migraine than those without (42). Furthermore, there is a case report of an individual with both hearing loss and developmental delay due to ESRRG disruption (43), indicating the crucial role of ESRRG in auditory system and brain development.
The SH group also featured the highest probability of osmophobia, nausea and vomiting. Migraine patients with osmophobia have a younger age of migraine onset (44) and a higher proportion of females compared to males (23), which aligns with the SH group traits. The cooccurrence of osmophobia, nausea, vomiting has been documented in several studies. A nosographic analysis of 1934 headache patients found that osmophobia is highly paralleled with nausea in migraine patients but not in tension-type headache patient (45). Another study focusing on pediatric migraineurs demonstrated a significant association between osmophobia and vomiting (46). Interestingly, a study focus on the dopamine symptoms (DAs) of migraine patients, including yawning, somnolence, nausea, vomiting, mood changes, fatigue, and diuresis, found an independent association between osmophobia and DAs, both pre-synaptic and post-synaptic (47), suggesting the potential role of dopamine in this phenomenon.
The mechanism behind the occurrence of multiple symptoms in the SH group is currently unknown. However, it is possible that hormones, hormone-related receptors genes, and dopamine play a role in it. In a prior latent class analysis (LCA) of migraine conducted in Korea (18), researchers identified three classes, one of which was termed “photophobia and phonophobia.” This class demonstrated the highest frequencies of both photophobia and phonophobia, as well as a notably high rate of osmophobia. This finding aligns with the SH group in our study, which similarly exhibited sensory hypersensitivity. We have discovered that this phenomenon of sensory hypersensitivity is not confined to photophobia, phonophobia, and osmophobia but can also extend to additional senses, including vestibular and auditory symptoms.
The PV (Prominent Vestibular) group in our study exhibits the highest occurrence of dizziness, vertigo onset and definite vestibular migraine cases based on current diagnostic criteria. It is also characterized by the highest probability of photophobia and phonophobia, with the lowest prevalence of auditory symptoms among the four groups. It is noteworthy that in the PV group, a phenomenon is observed where the frequency of dizziness shows significant differences across the four groups, while the differences in vertigo are not significant. However, the frequency and the probability of vertigo predicted by LCA in the PV group remain the highest compared to other groups, which aligns with dizziness. We believe this may be attributed to the relatively small sample size of vertigo rather than a discrepancy between dizziness and vertigo. Future studies that incorporate a larger cohort of vertigo patients may further substantiate this point.
Previous literature reports concurrent photophobia and phonophobia in definitive vestibular migraine patients, with a prevalence between 75.8% and 87% (13,48). Existing evidence suggests a potential role for Calcitonin Gene-Related Peptide (CGRP) in this phenomenon. As a neuropeptide, CGRP presumably mediates both visual, auditory and vestibular pathways, inducing these symptoms. This assumption is supported by evidence from multiple researches that CGRP is proven to induce photophobia behavior in mice (49–51). In human volunteers, there are significant photophobia and phonophobia developments after CGRP infusion (52). In the meantime, migraine patients experiencing phonophobia exhibit insufficient auditory pathway suppression compared to healthy controls, implicating CGRP as a likely causative agent due to its neurotransmitter mediating effects in the outer hair cells (53). Moreover, studies have shown a substantial increase in the expression level of CGRP in the vestibular nucleus of motion sickness rat model (54). Furthermore, inhibition of CGRP receptors improve vestibular function in rat models of chronic migraine (55).
In our study, we observed a notable distinction between the Sensory Hypersensitivity (SH) group and the Prominent Vestibular (PV) group. Patients in the PV group aligned more closely with traditional Vestibular Migraine (VM) patients, exhibiting a higher incidence of definite VM diagnosis. Contrary to the common perception that VM typically starts in the 30 to 40 age range (56), patients in the SH group were generally younger and presented a variety of symptoms beyond vestibular ones, such as auditory symptoms. Furthermore, we identified differences in family history between the two groups. A family history of vertigo increases the probability of belonging to the PV group, while patients with a family history of migraine were more likely to be in the SH group. These indications suggest that the SH group might represent a potential independent subclass within vestibular migraine, characterized by a range of associated symptoms including auditory symptoms. These could point to a pathophysiological mechanism that overlaps with, yet is distinct from, that of traditional VM. Current understanding of vestibular migraine associated symptoms is limited, and current diagnostic criteria for vestibular migraine do not encompass these symptoms (7). The significance of these symptoms in categorizing the highly heterogeneous vestibular migraine population requires further investigation.
One limitation of this study is that the participants were all Chinese Asian and recruited from a single hospital, which may limit the generalizability of the findings to other populations or settings. Additionally, the study relied on self-reported symptoms and retrospective data, which may introduce recall bias and potential inaccuracies in symptom reporting. Our study also included patients diagnosed with probable migraine, some of whom did not exhibit symptoms of the ictal phase, suggesting that certain individuals with migraine may experience fewer symptoms as presented in the PSG group. However, including these patients could impact the model's fit and future studies may be needed to validate this finding. Finally, our study did not include all potential symptoms experienced during migraine attacks, aura or interictal phases, nor did we account for all factors that might influence them. This approach may not fully reflect the complexity of migraine and associated symptoms. Future research employing temporal methods, like a latent transition model, could offer valuable insights into the progression patterns of migraine symptoms.
Conclusion
In conclusion, this study utilized latent class analysis to examine the diverse subcategories of migraines based on vestibular and auditory symptoms. The analysis identified four latent classes: the Sensory Hypertensive (SH), Prominent Vestibular (PV), Prominent Nausea (PN), and Presenting Symptoms but not prominent or dominant (PS) groups. The SH group displayed the most pronounced characteristics, including a higher prevalence of multiple sensory symptoms, an earlier age of migraine onset, and a higher proportion of females. The PV group exhibited the highest probability of dizziness, vertigo but without the presence of auditory symptoms. The findings suggest potentially different but overlapped mechanisms behind the vestibular and auditory symptoms of migraine, including genes, neurotransmitters and neuropeptides. Overall, this study provides valuable insights into the heterogeneity of migraines and demonstrates the potential of incorporating different patterns of migraine-related symptom into clinical considerations.
Article highlights
Identified four migraine subgroups with associated vestibular-auditory symptoms using latent class analysis: Prominent Vestibular, Prominent Nausea, Presenting Symptoms but not prominent or dominant, Sensory Hypersensitive.
Findings suggest potential different but overlapped mechanism behind the vestibular and auditory symptoms of migraine and possibly assist with patient prognosis and treatment.
Supplemental Material
sj-docx-1-cep-10.1177_03331024241262488 - Supplemental material for Latent class analysis of migraine associated vestibular-auditory symptoms
Supplemental material, sj-docx-1-cep-10.1177_03331024241262488 for Latent class analysis of migraine associated vestibular-auditory symptoms by Hui Li, Xiaonuo Xu, Rongjiang Xu, Ping Xiao Fan, Jiying Zhou and Liang Dong in Cephalalgia
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.