
Abstract
Background
The clinical profile of cluster headache may differ among different regions of the world, warranting interest in the data obtained from the initial Chinese Cluster Headache Register Individual Study (CHRIS) for better understanding.
Methods
We conducted a multicenter, prospective, longitudinal cohort study on cluster headache across all 31 provinces of China, aiming to gather clinical characteristics, treatment approaches, imaging, electrophysiological and biological samples.
Results
In total 816 patients were enrolled with a male-to-female ratio of 4.33:1. The mean age at consultation was 34.98 ± 9.91 years, and 24.89 ± 9.77 years at onset. Only 2.33% were diagnosed with chronic cluster headache, and 6.99% had a family history of the condition. The most common bout was one to two times per year (45.96%), lasting two weeks to one month (44.00%), and occurring frequently in spring (76.23%) and winter (73.04%). Of these, 68.50% experienced one to two attacks per day, with the majority lasting one to two hours (45.59%). The most common time for attacks was between 9 am and 12 pm (75.86%), followed by 1 am and 3 am (43.48%). Lacrimation (78.80%) was the most predominant autonomic symptom reported. Furthermore, 39.22% of patients experienced a delay of 10 years or more in receiving a correct diagnosis. Only 35.67% and 24.26% of patients received common acute and preventive treatments, respectively.
Conclusion
Due to differences in ethnicity, genetics and lifestyle conditions, CHRIS has provided valuable baseline data from China. By establishing a dynamic cohort with comprehensive multidimensional data, it aims to advance the management system for cluster headache in China.
Introduction
Cluster headache (CH) is a severe headache and the most common form of trigeminal autonomic cephalalgias (TACs), with a lifetime prevalence of 124/100,000 (1). The characteristic features of CH include strictly unilateral, periodic headaches of intense severity, often accompanied by autonomic symptoms such as conjunctival injection, lacrimation, nasal congestion, and rhinorrhea (2). The high frequency and intensity of these attacks, coupled with comorbidities such as anxiety and depression, significantly reduce the patients’ quality of life and productivity (3). Moreover, the diagnostic challenges and limited efficacy of current treatments highlight the need for a better understanding of CH (3). Therefore, a comprehensive investigation of the clinical characteristics, pathogenesis, and treatment options for CH is essential to optimize the clinical management and alleviate the social and economic burden associated with this condition.
Due to variations in ethnicity, genetics, and lifestyle conditions, the data pertaining to CH, including its clinical characteristics, imaging, electrophysiology, and biospecimens, may differ across different regions of the world. Although certain aspects of CH have been previously investigated, there is a need for further research that expands on sample sizes and includes a more diverse geographic representation. Furthermore, there is a relative dearth of recent data on CH from the Chinese mainland (4–7). Additionally, there is a scarcity of large-scale longitudinal cohort studies aimed at optimizing the management of CH, both within China and globally (8,9). Consequently, we have initiated the first CH registry study in China, establishing a prospective, longitudinal, multicenter cohort to gain a more comprehensive understanding of CH’s clinical phenotype, pathogenesis, and potential for optimizing treatment regimens. In this article, we present the study design of Chinese Cluster Headache Register Individual Study (CHRIS), the methodology used for data collection at baseline, and report the Phase I baseline data. These findings served as the foundation for subsequent analysis of follow-up data and multimodal data, including biospecimen, imaging, and electrophysiology data.
Methods
Study design and setting of CHRIS
This prospective longitudinal cohort study, formally named the Chinese Cluster Headache Register Individual Study (CHRIS), was initiated in January 2019 and officially established in August 2022. The study was conducted in a multicenter format, encompassing 31 provinces or cities across China (Online Supplementary Table S1). Various levels of healthcare centers, ranging from primary to tertiary care, were included as registry centers to ensure the representativeness of the enrolled patients. Pilot recruitment commenced at headache centers in January 2019 and will continue recruiting for the next few years, with the aim of establishing a prospective and representative longitudinal cohort. All patients provided written informed consent to participate in the study.
Participants
Patients who were receiving treatment or seeking treatment at any of the participating headache centers, who were ≥13 years old, and had been diagnosed with either episodic or chronic CH according to the International Classification of Headache Disorders 3rd edition (ICHD-3) (2) were considered eligible for enrollment in the study. The diagnosis was established by one neurologist with expertise in primary headache disorders and was verified by another headache specialist by reviewing relevant medical records. Patients with secondary causes of headaches or those who were unable to differentiate their CH attacks from other types of headaches were excluded from the study.
Data collection
The electronic structured questionnaires were conducted in the consultation room after the consultation, under the guidance of physicians, nurses, or research staff. In this study, we primarily elaborated on the methodology for baseline data collection in CHRIS (Online Supplemental Table 3).
Demographics: sex, age, height, weight, educational background, occupation, long-term residence, smoking, and drinking habits; Headache-related information: age at onset, course of disease (the duration in years between the first incidence of CH and the initial visit to the headache center of CHRIS), years of misdiagnosis, previous history of other types of headaches, and family histories of other headaches; Clinical characteristics: diagnosis, onset date of bout, frequency of bouts and attacks, duration of bouts and attacks, peak time of attacks, laterality (right- side only, left- side only, side-alternating within between attacks or between bouts), locations (retro-orbital, temporal, forehead, parietal, occipital, teeth, cheek, ear), pain intensity (visual analog scale rating from 0 to 10), circadian rhythm of attacks, seasonality of bouts, accompanying cranial autonomic symptoms (CAS) (i.e., lacrimation, conjunctival injection, rhinorrhea, nasal congestion, facial sweating, ptosis/miosis, eyelid oedema) and additional symptoms (i.e., nausea, vomiting, photophobia, phonophobia, osmophobia, allodynia), pre-episode symptoms (PES) that begin days to weeks before the commencement of cluster episodes (6), pre-attack symptoms (PAS) that begin minutes before the pain in individual attacks (6), triggers, and comorbidities (including anxiety, depression, and insufficient sleep); Previous treatment and response: previous medication options for acute and preventive treatment and effects. We defined conventional acute treatment as nasal spray zolmitriptan, oral zolmitriptan, oxygen, oral rizatriptan, lidocaine nasal drop and oral sumatriptan. We defined the option of acute or preventive treatment (“Taken”) as the proportion of the total number of patients who had received the corresponding treatment. We define effectiveness (“Effective”: <30%, 30%- 50%, >50% reduction in attack frequency) as the proportion of patients who had the corresponding effect for a treatment to the number of patients who received this treatment.
Analysis of baseline data
For this present baseline analysis, the study encompassed all patients admitted to the headache centers in CHRIS from January 2019 to May 2023. The data analysis solely focused on the information obtained during the patients’ initial visits. Descriptive statistics were used to analyze the study cohort’s observed characteristics. Statistical analyses were conducted using SPSS (version 23.0; SPSS, Chicago, IL, USA). Measurement data were presented as means ± standard deviation (SD) or as medians with the interquartile range. Count data were presented as numbers (percentage). A χ2 test was used to compare the baseline characteristics of CH cohorts (men and women) for categorical variables, while Student’s t-test was employed for continuous variables, depending on the distribution. A two-sided p-value less than 0.05 was considered statistically significant.
Results
Demographics
A total of 816 patients diagnosed with CH were enrolled in the CHRIS study, among whom 663 (81.25%) were male and 153 (18.75%) were female, with a male-to-female ratio of 4.33:1. Among them, 19 patients (2.33%) were diagnosed with chronic cluster headache (cCH). The average age at consultation was 34.98 ± 9.91 years, with males having a mean age of 35.16 ± 9.90 years and females having a mean age of 34.07 ± 10.03 years (p = 0.155). The mean age of onset was 24.89 ± 9.77 years, with males having a significantly higher mean age of 25.31 ± 9.71 years compared to females, who had a mean age of 23.09 ± 9.86 years (p = 0.011). A total of 57 patients (6.99%) reported a family history of CH (p = 0.026). Among the patients, 338 (41.42%) reported a history of smoking, and 190 (23.28%) reported a history of alcohol consumption (Table 1).
Demographics of patients with CH (N = 816).

*p < 0.05; CH: cluster headache.
Laterality and location of attacks
A majority of the patients (n = 767, 94.00%) in the study exhibited strictly unilateral attacks, while a smaller proportion of patients (n = 49, 6.00%) reported experiencing side-alternating (p = 0.090), with 30 (3.68%) patients within different bouts and 19 (2.33%) patients within between episodes. The retro-orbital (75.98%, p = 0.431) and temporal (74.39%, p = 0.044) were the most commonly affected locations during attacks, followed by the forehead (38.11%, p = 0.899), parietal (28.92%, p = 0.882), and occipital (26.96%, p = 0.117). Less frequently reported locations included the teeth (12.50%, p < 0.0001), cheek (11.64%, p = 0.011), and ear (5.16%, p = 0.001) (Table 2).
Clinical characteristics of CH patients (N = 816).

*p < 0.05; CH: cluster headache.
Periodicity of bouts and attacks
In the study, 45.96% of the enrolled patients reported experiencing one to two bouts of CH per year, while 40.1% had less than one bout per year, and only 9.56% reported more than two bouts per year (p = 0.147). The duration of these bouts varied, with the majority of patients reporting bouts lasting from two weeks to one month (44.00%), followed by one to two months (21.94%), less than two weeks (18.26%), and more than two months (11.27%) (p = 0.539) (Table 2). Bouts were found to occur most frequently in the spring (March to May, 76.23%) and winter (December to February, 73.04%), while they were least common in the summer (June to August, 47.79%) (Figure 1). During the cluster period, the majority of patients (68.50%) experienced one to two attacks per day, with a smaller proportion reporting more than two attacks (18.26%) or less than one (13.48%) per day (p = 0.956). Among those experiencing attacks, 45.59% reported each attack lasting one to two hours, while 32.23% reported attacks lasting less than one hour (p = 0.962) (Table 2). Additionally, 698 patients (85.54%) reported a circadian rhythm to their attacks, with the most common times of day being from 9 am to 12 pm (75.86%) and from 1 am to 3 am (43.48%) (Figure 1).
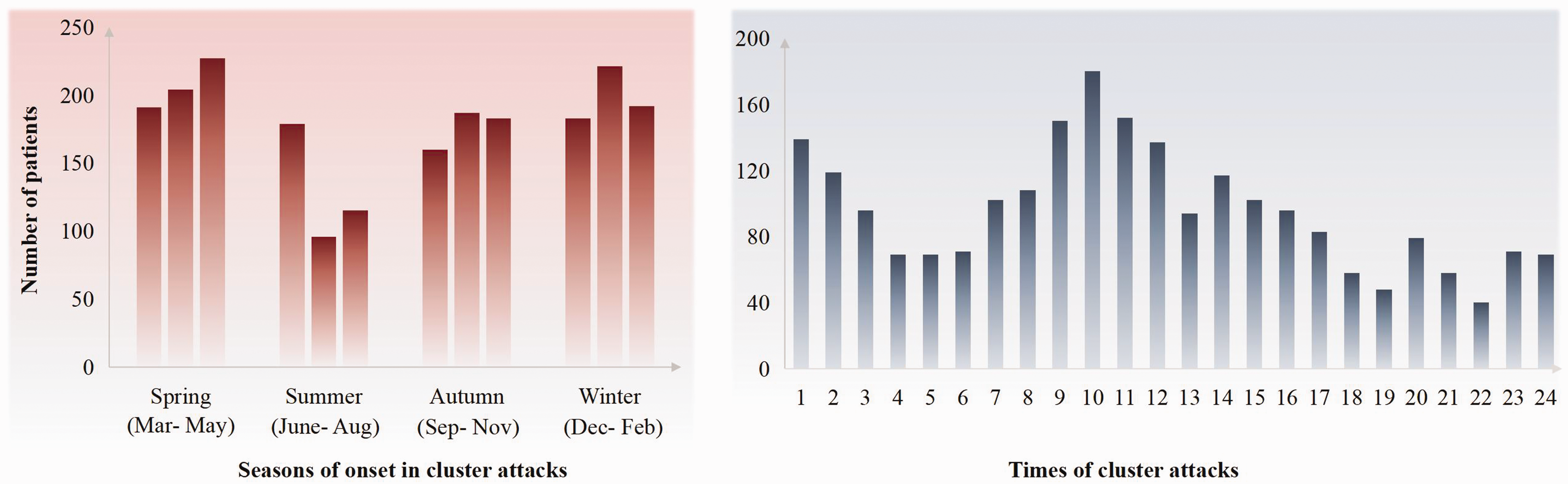
Seasons and times of cluster attacks. Bouts occurred most frequently in spring (March to May) and winter (December to February), and least commonly in summer (June to August). Attacks most commonly occurred from 9 am to 12 pm and from 1 am to 3 am.
Possible triggers for attacks
Among the enrolled patients, 401 (49.14%) patients reported insufficient sleep as a trigger for attacks. There were 297 (36.40%) patients that experienced attacks after temperature changes, and 276 (33.82%) that experienced attacks after emotional fluctuation. Fatigue was reported in 241 (29.53%) patients as a trigger. Only 19 (12.33%) females experienced attacks during menstruation. Of the “drinking” patients, 78 of 190 patients (41.05%) reported attacks after alcohol consumption; of the “smoking” patients, 47 of 338 patients (13.91%) reported attacks after smoking. A total of 20.71% of patients experienced spontaneous attacks without an identified trigger.
Cranial autonomic and additional features
A total of 514 (62.98%) patients reported experiencing PAS (p = 0.023), while 157 (19.19%) displayed PES (p = 0.091) (Table 2). The most prevalent autonomic symptom during the attacks was lacrimation (78.80%), followed by conjunctival injection (53.19%), nasal congestion (49.63%), and rhinorrhea (38.97%). Less frequently observed autonomic symptoms included facial sweating (35.05%), ptosis/miosis (34.80%), and eyelid edema (14.46%). Nausea was reported by 57.48% of the patients, and 32.11% presented with vomiting. Photophobia (55.02%) and phonophobia (53.55%) were more commonly reported, while allodynia (16.30%) and osmophobia (16.05%) were less common. Over half of the patients reported restlessness or agitation during the attacks (55.88%), and only 14.46% experienced exacerbation of symptoms through physical activity. Notably, certain autonomic symptoms, such as conjunctival injection (p = 0.002), rhinorrhea (p = 0.012), ptosis/miosis (p = 0.034), eyelid edema (p = 0.024), as well as additional symptoms, such as osmophobia (p = 0.039) and aggravation by physical activities (p = 0.006), displayed significant sex-based differences (Figure 2).
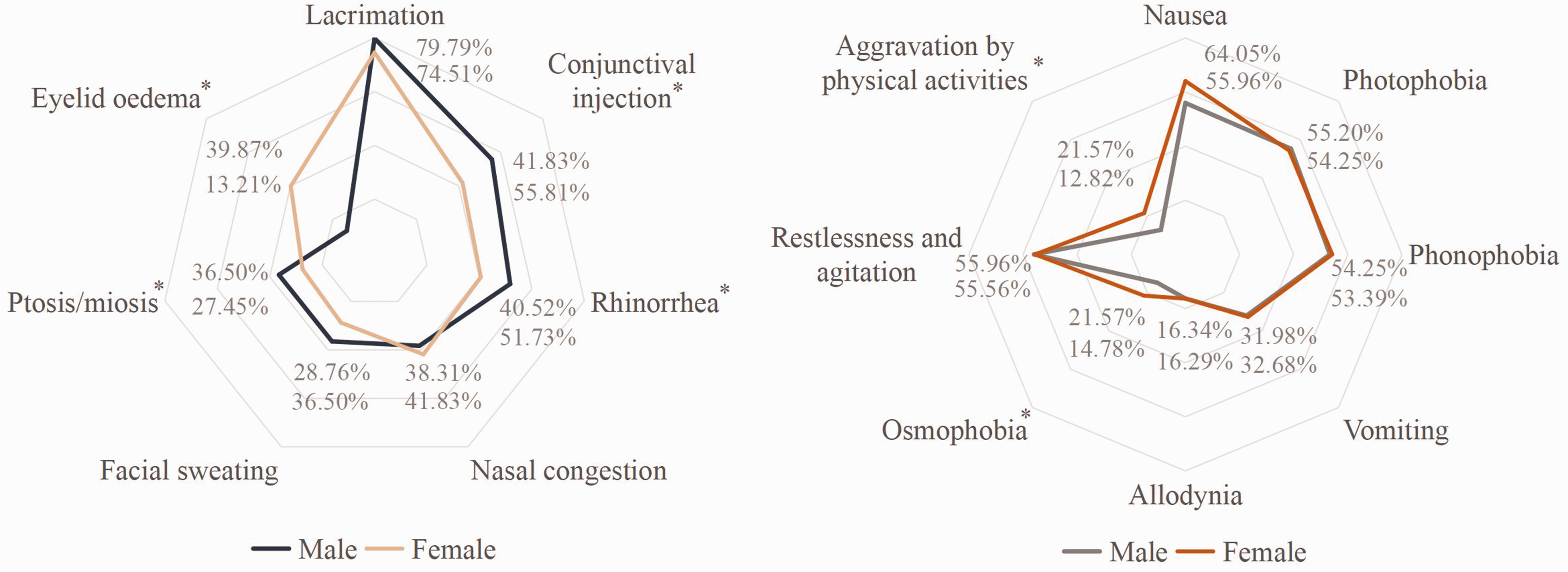
Autonomic and additional symptoms of CH patients (N = 816). Lacrimation was the most commonly experienced autonomic symptom during the attacks. Nausea, photophobia, phonophobia, and restlessness or agitation during the attacks were more common. Conjunctival injection, rhinorrhea, ptosis/miosis, eyelid oedema as well as osmophobia, and aggravation by physical activities, demonstrated significant sex-based differences. *p < 0.05.
Time delay for correct diagnosis
Only a small proportion of patients (n = 97, 11.89%) received a correct diagnosis of CH at the time of initial presentation. Nearly half of the patients (39.22%) encountered a considerable delay of 10 years or more in receiving the accurate diagnosis (Figure 3).

Time delay for correct diagnosis of CH (N = 816).
Treatment status
A total of 291/816 (35.67%) patients received conventional acute treatment (including nasal spray zolmitriptan, oral zolmitriptan, oxygen, oral rizatriptan, lidocaine nasal drop and oral sumatriptan (10)), while 256/816 (31.37%) patients utilized other analgesics or non-pharmacological treatments such as NSAIDS, compounded analgesics, or acupuncture. Additionally, 269/816 (32.97%) patients reported that they did not receive any treatment. Of the common treatments, oxygen was the most frequently received option (45.36%, N = 132/291), followed by oral zolmitriptan (43.30%, N = 126/291), nasal spray zolmitriptan (28.52%, N = 83/291), oral rizatriptan (12.71%, N = 37/291), lidocaine nasal drop (11.34%, N = 33/291), and oral sumatriptan (1.37%, N = 4/291) (Figure 4a). None of the patients attempted neurostimulation techniques such as pterygopalatine ganglion stimulation or non-invasive vagus nerve stimulation for acute treatment. In terms of effectiveness, oral sumatriptan was found to be the most effective, followed by oral rizatriptan, oxygen, oral zolmitriptan, nasal spray zolmitriptan, and lidocaine nasal drop (Figure 5a). Only 198/816 (24.26%) patients had used conventional transitional or preventive treatments, including oral glucocorticoid (45.96%, N = 91/198), verapamil (21.73%, N = 43/198), nerve block (18.18%, N = 36/198), pregabalin (15.15%, N = 30/198), topiramate (13.14%, N = 26/198), sodium valproate (4.55%, N = 9/198), gabapentin (2.53%, N = 5/198), lithium (2.02%, N = 4/198), and calcitonin gene-related peptide monoclonal antibodies (CGRP-mAb) (2.02%, N = 4/198) (Figure 4b). Among these treatments, CGRP-mAb was found to be the most effective, followed by oral glucocorticoid, topiramate, gabapentin, verapamil, sodium valproate, nerve block, pregabalin, and lithium (Figure 5b).

The ratio of patients with CH receiving the medication. (a) Acute treatment and (b) Transitional or preventive treatment.

The ratio of medication “efficacy”. (a) Acute treatment and (b) Transitional or preventive treatment. “Effective”: <30%, 30%–50%, or >50% reduction in attack frequency, which was the proportion of patients who had the corresponding effect for a treatment to the number of people who received this treatment.
Discussion
CHRIS is the first registry study of CH conducted in China, aiming to establish a representative, prospective longitudinal cohort by enrolling consecutive CH patients. The comprehensive and extensive dataset that has been collected thus far provides valuable insights into the demographics, clinical characteristics, diagnosis, and treatment status of CH patients in China. Moving forward, CHRIS endeavors to continue data collection, encompassing clinical characteristics, imaging, electrophysiology, and biological samples, as well as ensuring complete follow-up to establish a dynamic cohort that complements previous studies. The ultimate goal of this study is to enhance the management system for CH in China and to serve as an important reference for CH research worldwide.
This study adheres to the principles of multicenter, multidimensional and multi-node research design. This study spreads across 31 provinces and cities with hospitals of different levels across China, providing a comprehensive representation of geographic breadth in the data. Moreover, previous studies have revealed that CH has East-West differences (4,11,12) in its clinical characteristics, such as stronger male dominance, fewer aura, lower rate of restlessness, and more rare chronic subtypes, suggesting possible variations in CH pathogenesis. Therefore, we conducted in-depth studies from multiple-dimension (such as imaging, biomics) and multiple-node (at visit and follow-up). Our baseline data already reveal some differences between men and women, and between East and West.
Regarding the Western and Eastern differences in CH, the current study found some clinical characteristics to be consistent with those reported North America and Europe (13–15), such as male dominance, retro-orbital and temporal areas as common locations of attack, one to two hours as common duration, lacrimation being a common autonomic symptom, high rates of photophobia and phonophobia, and seasonal tendencies in spring and winter. However, some differences were observed and were relatively consistent with our previous studies (4,6). In our study, there was a decreased trend in male predominance compared to the study in 2013 (4), which could be partly attributed to lifestyle changes (16) or improved rates of correct diagnosis allowing more female CH patients to avoid being misdiagnosed with migraine (4). Nonetheless, male predominance remains stronger in China than North America and Europe (17,18), possibly due to ethnic and genetic differences responsible for a more pronounced male predominance in China than in North America and Europe. Furthermore, some studies have reported that the proportion of cCH in Eastern countries varied between 0–7.5% (12), and our study found that only 2.33% of patients were diagnosed with cCH, which is lower than the proportion reported in North America and Europe (15,19). This prominent difference could be attributed to ethnic or cultural differences, and the larger sample in our study makes the results more reliable. Family history plays an essential role in the pathogenesis of CH, and the ratio of 6.99% in our study is relatively close to the previous estimates of family history of CH (6.27%) (20). We found the circadian pattern from 9 am to 12 pm, and from 1 am to 3 am, which is consistent with a study in Korea (21), but slightly different from the midnight peak found in North America and Europe (22). Differences in circadian rhythms may be ascribed to East-West racial variations, an area of investigation deserving additional examination.
Regarding sex differences in CH, our study has identified some clinically significant characteristics. Women with CH had a significantly higher positive family history when compared to men, and this finding is consistent with previous studies that reported a higher family history in female patients (4,17,20). Moreover, migraine-like symptoms, such as vomiting, nausea and aggravation by physical activities, were more common in women with CH, which is consistent with some of the previous studies and may be due to the fact that migraine comorbidity occurs more often in women (23,24).
The baseline data from this study offer a preliminary overview of the current status of CH diagnosis and treatment in China. The correct initial diagnosis rate of CH patients was found to be 11.89%, similar to 10.8% in 2013 (4), suggesting the need to continue to promoting measures to optimize diagnosis and treatment, as well as the reason why we conducted CHRIS. What is more, the current diagnosis rate still falls short compared to that reported in foreign studies (25,26), and almost 50% of patients experienced a delay exceeding 10 years before being correctly diagnosed. Therefore, it is critical to improve the understanding of CH and enhance the accuracy of diagnosis through various studies, including the proposed CHRIS. The results also showed that a meager 35.67% of patients received common acute treatment, and only 24.26% received common “long-term” treatment for CH, which, it should be noted, does not exactly represent standardized CH care. Specifically, 45.36% of patients received oxygen, 28.52% received nasal zolmitriptan as an acute treatment; 45.96% received oral glucocorticoid as a transitional treatment; and 21.73% received verapamil as a preventive treatment. Such a low percentage of use of these drugs, which are classified as Level A recommended in the guideline of CH (10), may, we speculate, be due to the irregularity of the treatment modalities or the poor availability of the drugs in hospitals or even in China (i.e., verapamil, sumatriptan, CGRP-mAb). Specifically, most hospital pharmacies are not routinely stocked with verapamil which patients need to purchase themselves at the pharmacy. Most physicians’ knowledge of lithium agents also limits their dosing options. Notably, the effectiveness of the medication deviated from previous reports, e.g. only 34.85% of patients using oxygen saw more than 50% reduction in headaches, which could be due to irregularities in medication use and inadequate physician education, such as low oxygen inhalation flow. Thus, the CHRIS study aims to significantly enhance CH diagnosis and treatment in China by standardizing treatment protocol and improving physician education in the management of CH.
CHRIS has some strengths. Firstly, it is the first registry study on CH in China, providing the world with more comprehensive and updated data from China. Secondly, we collect multidimensional information based on the cohort to explore the pathogenesis and treatment options for CH, including clinical characteristics, imaging, electrophysiology and biological sample. Our primary focus is to establish a dynamic follow-up cohort and combine time and data spans to explore CH continuously. Despite these strengths, our study has some limitations. Firstly, although our study sites cover 31 provinces and cities throughout China, may not be sufficient to represent the population size comprehensively. We aim to address this shortfall by enhancing the CH map systematically.
Conclusion
As the inaugural registry study on patients with CH in China, CHRIS has successfully established a comprehensive and prospective longitudinal cohort. This study collects a wide range of cohort data, including clinical features, imaging, electrophysiology, biological samples, and complete follow-up. By employing such an approach, the study effectively tackles previous research limitations. It is our belief that long-term follow-up and multidimensional data are indispensable for the development and optimization of patient-specific treatment systems in China. In addition, the findings from this study will contribute significantly to research of CH on a global scale.
Article highlights
CHRIS aims to establish a dynamic cohort with comprehensive multidimensional data, providing the world with valuable data in China. Distinct clinical features of CH exhibit variations concerning East-West disparities and sex differences, indicating potential discrepancies in the underlying pathophysiological mechanisms. The limited efficacy of diagnosis and treatment in China, coupled with the low rate of correct diagnosis, highlights the necessity for continual enhancement of the diagnostic and treatment system for cluster headache.
Supplemental Material
sj-pdf-1-cep-10.1177_03331024241235193 - Supplemental material for Profile of Chinese Cluster Headache Register Individual Study (CHRIS): Clinical characteristics, diagnosis and treatment status data of 816 patients in China
Supplemental material, sj-pdf-1-cep-10.1177_03331024241235193 for Profile of Chinese Cluster Headache Register Individual Study (CHRIS): Clinical characteristics, diagnosis and treatment status data of 816 patients in China by Shuhua Zhang, Suiyi Xu, Chunfu Chen, Zhanyou Xue, Yuanrong Yao, Hongru Zhao, Hongling Zhao, Yabin Ji, Dan Wang, Dongmei Hu, Kaiming Liu, Jianjun Chen, Sufen Chen, Xiaoyu Gao, Wei Gui, Zhiliang Fan, Dongjun Wan, Xueqian Yuan, Wensheng Qu, Zheman Xiao, Ming Dong, Hebo Wang, Chunyang Ju, Huifang Xu, Liang Zhang, Xiaolin Wang, Mingjie Zhang, Xun Han, Ye Ran, Zhihua Jia, Hui Su, Yingji Li, Huanxian Liu, Wei Zhao, Zihua Gong, Xiaoxue Lin, Yingyuan Liu, Yin Sun, Siyuan Xie, Deqi Zhai, Ruozhuo Liu, Shengshu Wang, Zhao Dong, Shengyuan Yu and on behalf of the Chinese Cluster Headache Alliance (CCHA) in Cephalalgia
Footnotes
Acknowledgement
Thanks to Zhonglin Liu, Yanhong Wang, Li Li, Zhe Wang, Li Mei, Peng Xu, Haiyan Yu, Yang Liu, Min Chen, Rui Liu, Weiliang He, Jiajun Yang, Ge Tan, Jiasi Li, Dan Zhang, Xianliang Li, Yuhong Man, Lin Li, Yusheng He, Zhanxiu Ren, Xiaojuan Wang, Jie Zhang, Xingkai An, Zhongling Zhang, Jing Zhang, Yonghui Liu, Yi Zhang, Qun Gu, Lijuan Wang, Shi Qiu, Haiyan Cai, Lanyun Yan, Nana Hu, Chun Huang, Mei Yin, Ran Zhang, Juan Yi, Fang Chen, Qiaolin Gao, Yi Wang, Zengqiang Zhang, Yunqing Qin, Yu Hao, Qi Zhang, Yongbin Song, Hui Xue, Peng Feng, Wei Shao, Mingxin Li, Chenmin Huang, Weian Chen, Qiuling Tong as CCHA members for their contribution in providing the cases and the participation of patients with CH in CHRIS.
Authorship contribution statement
SHZ and SYX analyzed the data and results, and drafted the manuscript. SSW analyzed the data. CFC, SHZ, SYX, ZYX, YRY, HRZ, HLZ, YBJ, DW, DMH, KML, JJC, SFC, XYG, WG, ZLF, DJW, XQY, WSQ, ZMX, MD, HBW, CYJ, HFX, LZ, XLW, MJZ, XH, YR, ZHJ, HS, YJL, HXL, WZ, ZHG, XXL, YYL, YS, SYX, DQZ, RZL collected and interpreted the data. ZD proposed the concept and design of the study and revised manuscript for critical intellectual content. SYY proposed the concept and design of the study. All authors read and approved the final manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.