
Abstract
Migraine headaches are among the leading causes of disability in the world. The burden of migraines is highest in women of reproductive age. This cross-sectional study characterized the prevalence, symptoms and correlates of migrainous headaches in 154 pregnant women attending a prenatal care clinic in Lima, Peru. Lifetime prevalence of migraine defined by modified IHS criteria was 9.1± (95± CI 4.6–13.6). When probable migraines were included, the lifetime prevalence of migraine in this population was 29.2± (95± CI 22.0–36.4). Migraine headaches were associated with a maternal history of headache, childhood carsickness, a diagnosis of allergies, and a high frequency of fatigue. Although headache-related disability was low in terms of missed work and recreation, high rates of headache pain and medicinal use reflect the true impact on this population.
Introduction
Migraine is a common chronic-episodic disorder of idiopathic origin, ranked among the world's top 20 causes of years lived with disability by the World Health Organization (1). Numerous population-based epidemiological studies in developed countries have reported the lifetime prevalence of migraine in women to be between 11 and 32% (2–10), and the 1-year prevalence in women to be between 9 and 22% (2–4,7,8,11–18). These surveys have demonstrated that women are approximately three times as likely as men to suffer from migraine, and the prevalence in women peaks during the reproductive years.
A recent multinational survey of migraines in Latin America showed comparable 1-year prevalence rates (19). These investigators confirmed that reproductive-aged women bear the largest burden of migraine, and they also noted that the rates of medical consultation and diagnosis of migraine were lower in Latin America than in developed countries.
Several studies have shown that migraines are a risk factor for ischaemic stroke in young women; other studies suggest that a history of migraine headaches may be associated with hypertension in pregnancy and subsequent vascular disorders (20–25). As the burden of disease in Peru shifts from infectious communicable outcomes to chronic illnesses, it is essential to characterize the risk factors and outcomes for vascular disorders in this population, with an emphasis on women of reproductive age.
To this end, we conducted a pilot cross-sectional study in the pregnant patient population at Dos de Mayo Hospital in Lima, Peru, with the principal aim of assessing the prevalence, symptoms and risk factors of migraine in an unstudied population. The information from the pilot will provide a basis for future studies of migraine disorders and related disorders of pregnancy and chronic disease in Peru.
Methods
Data collection
Subjects were recruited from the prenatal care clinic at Dos de Mayo Hospital in Lima, Peru, from July to September 2004. Eligible subjects were between the ages of 18 and 45 years with a pregnancy of less than 37 weeks of gestational age. Hospital personnel approached eligible subjects as they checked in for their prenatal consultations, and referred them to a team of trained interviewers from Peru and the USA to hear more about the study. Sampling was conducted continuously according to the availability of study interviewers. When more potential subjects were available for interview than there were interviewers, subjects were approached in a random fashion.
The interviewers presented the study consent forms to potential participants to read, and then answered any residual questions. Upon consent and enrolment into the study, subjects were interviewed in Spanish according to a structured migraine assessment questionnaire (adapted from the deCODE Genetics migraine questionnaire) (26). The interview included questions regarding medical history, pre-pregnancy weight and general health, pregnancy-related symptoms and headache characteristics, as well as an assessment of the disability associated with headaches experienced before and during pregnancy. Height and blood pressure on the day of the interview were collected from the subjects’ prenatal record files.
All participants were asked if they had ever experienced headache episodes. Headache classification was determined using modified criteria established by the International Headache Society (27). ‘Strict migraine’ (IHS category 1.1 or 1.2) was defined by at least five lifetime headache attacks lasting 4–72 h, with at least two of the qualifying pain characteristics (unilateral location, pulsating quality, moderate or severe pain intensity, aggravation by routine physical exertion), at least one of the associated symptoms (nausea and/or vomiting, photo/phonophobia), and not readily attributable to another central nervous system disorder or head trauma (according to subject self-report). ‘Probable migraine’ (IHS category 1.6) was designated if all but one of the strict migraine criteria were fulfilled, excluding headaches attributable to another disorder.
Participants were asked to report days of work, school housework and social activities missed due to headaches during the 3 months before the index pregnancy, and since becoming pregnant. Grading of pre-pregnancy responses was performed according to the Migraine Disability Assessment Score, which categorizes the number of days disrupted by headaches during a 3-month period into groups of minimal, mild, moderate and severe disability. Participants were also asked to report the number of days they experienced headache and to rate the severity of their headache pain on a scale of 0–10 (where 0 is no pain, and 10 is the most severe pain) before and during pregnancy (28).
Statistical analysis
Data were entered and managed in Microsoft Excel and analysed using SPSS and EpiInfo. Characteristics associated with strict and probable migraine headaches were determined using χ2 and Mann–Whitney U-tests. Logistic regression analysis was used to find adjusted odds ratios (OR) and 95% confidence intervals (CI). All reported P-values are two-tailed.
This study was approved by the institutional review boards of Dos de Mayo Hospital and the University of Washington. Participants signed a consent form in order to be included in the study.
Results
During the study period, 161 women were approached and 154 (96%) agreed to participate. A total of 14 subjects met the IHS criteria for strict migraine, and 31 additional subjects met the criteria for probable migraine. Among the remaining subjects, 50 women reported headache episodes that did not fit the migrainous criteria. Lifetime prevalence of strict migraine was calculated to be 9.1% (95% CI 4.6–13.6), and lifetime prevalence of any migrainous headache (strict or probable) was 29.2% (95% CI 22.0–36.4). Characteristics of the three groups are presented in Table 1.
Characteristics of study participants according to migraine classification, Dos de Mayo Hospital, Lima, Peru, 2004

N (%) unless otherwise noted; S.E. = standard error.
Some respondent information unknown; subjects with missing values not included in variable-specific calculations.
A comparison of headache characteristics among all study participants reporting headache episodes is presented in Table 2. The most influential criteria that distinguished strict and probable migraines were the typical length of episodes and associated nausea and/or vomiting. The most influential criteria that distinguished probable migraines from other types of headache were the lifetime number of episodes, the typical length, the pulsating quality of pain, aggravation by physical exertion, and identification of a central nervous system cause.
Distribution of headache characteristics used to classify migraine status among participants who reported headache episodes, Dos de Mayo Hospital, Lima, Peru, 2004
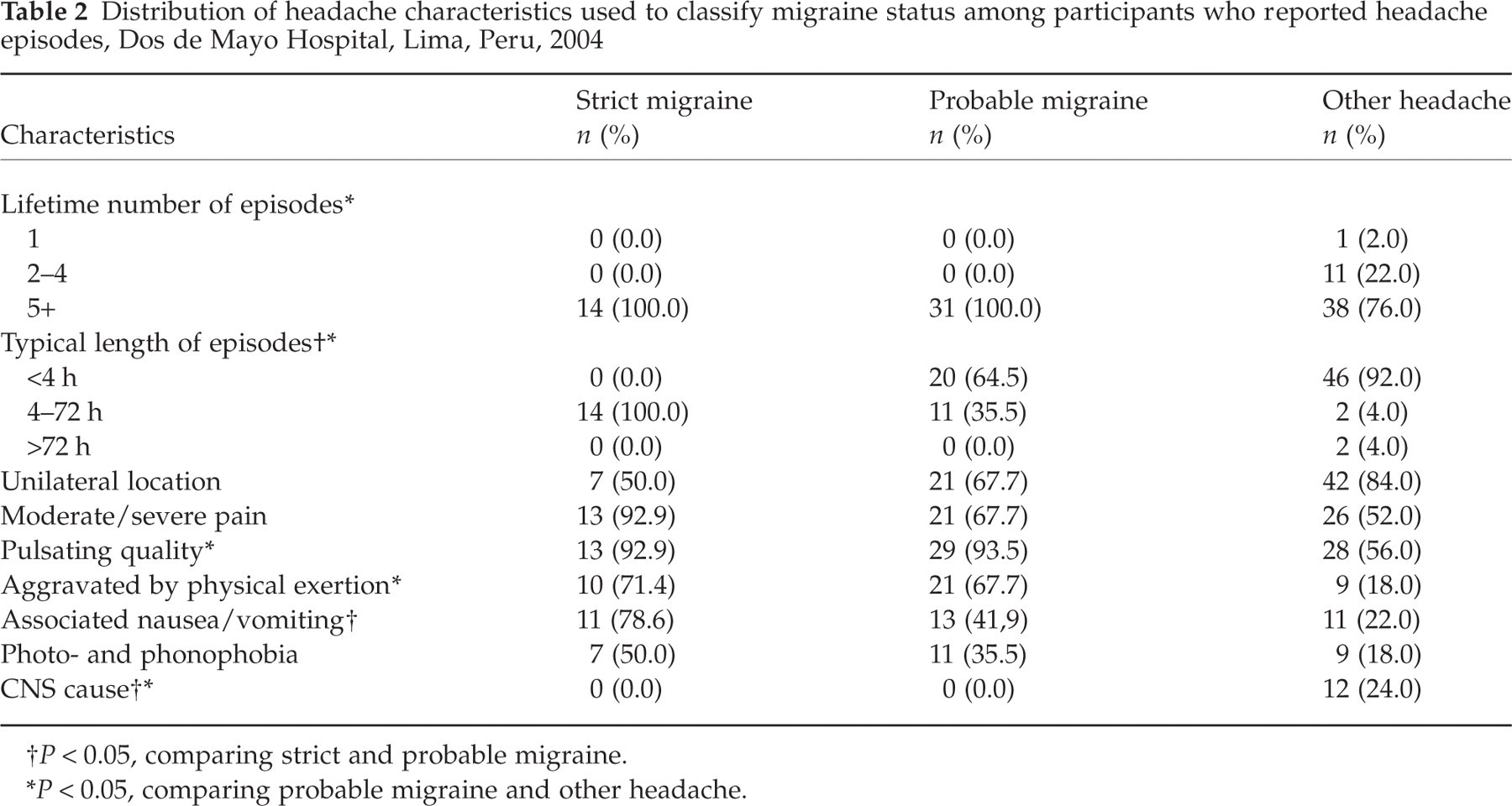
P < 0.05, comparing strict and probable migraine.
P < 0.05, comparing probable migraine and other headache.
Table 3 shows the distribution of headache characteristics not used for the classification of migraine among participants reporting headache episodes. Strict and probable migraine cases were combined to represent all migrainous subjects. Compared with participants with other kinds of headaches, participants with migrainous headaches reported a significantly higher prevalence of aura-like symptoms (any focal, sensory or speech alterations preceding the onset of headache) and were significantly more likely to use pharmaceutical treatment for headache relief. All participants with any type of headache attack were equally likely to report associated neck and shoulder pain, nutritional triggers, association with the menstrual cycle, having had clinical testing (e.g. MRI, X-ray, blood testing), and the use of alternative treatments (e.g. massage, compresses).
Distribution of headache characteristics not used to classify migraine status among participants who reported headache episodes, Dos de Mayo Hospital, Lima, Peru, 2004

Includes strict and probable migraines.
Some respondent information unknown.
P < 0.001.
P < 0.05.
Table 4 shows that the distribution of disrupted days due to headache appeared to vary according to headache type (P = 0.08). However, only four migrainous subjects and two non-migrainous subjects reported enough headache-related disruption before pregnancy to be categorized as at least mild headache-related disability. Subjects with migraine reported a higher frequency of headache days (P < 0.05) and a higher severity of pain in the 3 months before pregnancy compared with subjects with non-migrainous headache (P < 0.05).
Headache-related disability∗ in the 3 months before pregnancy among participants reporting lifetime headache episodes, Dos de Mayo Hospital, Lima, Peru, 2004

N (%) unless otherwise noted; S.E. = standard error.
Some participant responses unknown.
Strict and probable migraines.
P < 0.05 for Mann–Whitney U-test.
Assessments of headache-related disability could not be performed according to the MIDAS grading system for the period since pregnancy, because of the varying gestational ages and changes in employment status since pregnancy. However, a comparison of the self-scored headache pain scales is shown in Table 5. Again, subjects with migraine reported a higher severity of pain during pregnancy compared with subjects with non-migrainous headache (P < 0.05). Comparing intrapatient qualitative changes in self-scored pain before and during pregnancy, it appears that patients with migrainous and non-migrainous headaches were equally likely to experience headache relief during pregnancy (P = 0.7).
Headache-related disability∗ during pregnancy among participants reporting lifetime headache episodes, Dos de Mayo Hospital, Lima, Peru, 2004
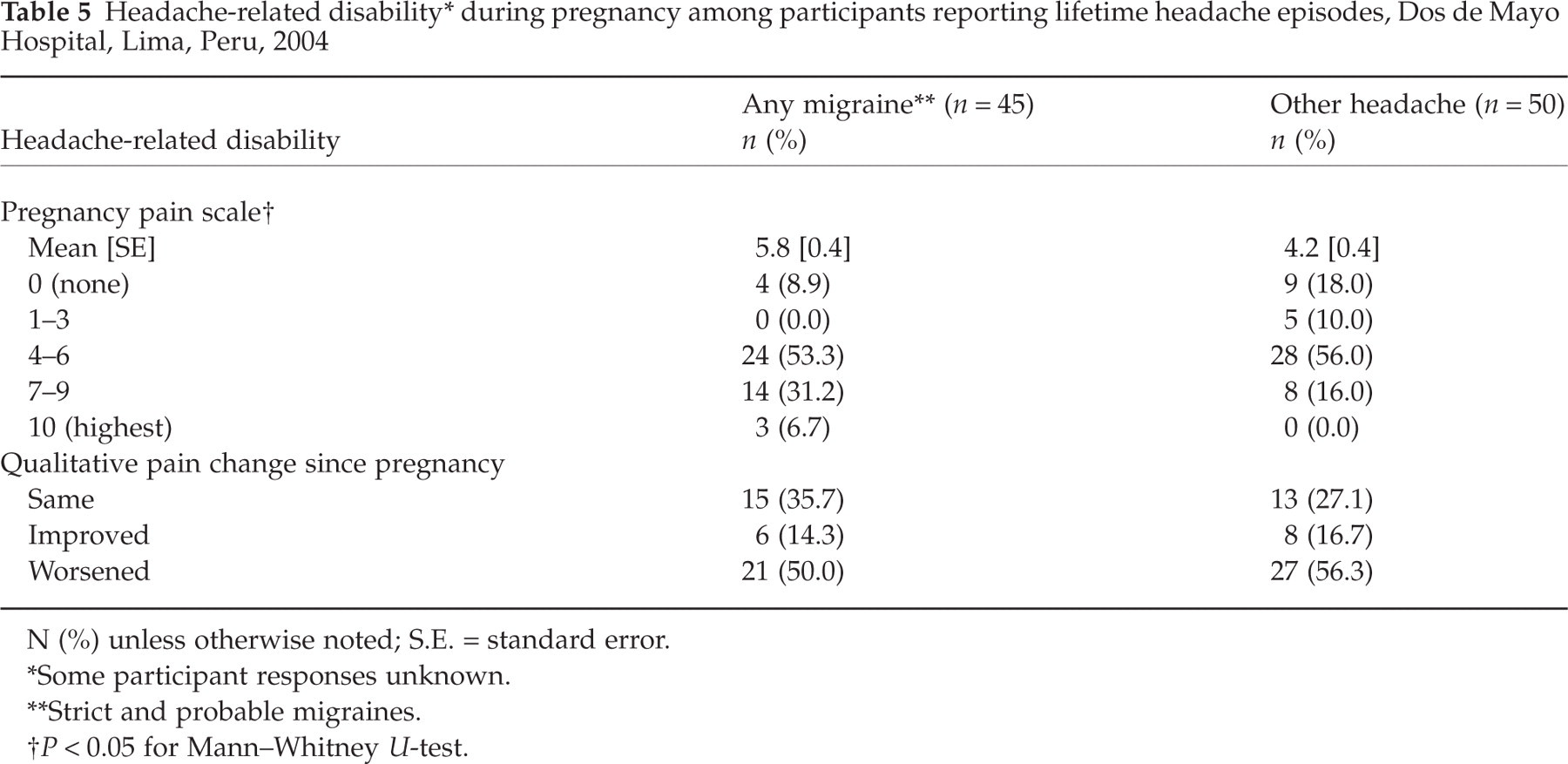
N (%) unless otherwise noted; S.E. = standard error.
Some participant responses unknown.
Strict and probable migraines.
P < 0.05 for Mann–Whitney U-test.
Stepwise logistic regression analysis was performed to identify risk factors and comorbidities of migrainous headaches (Table 6). Subjects with migraine headaches were more likely to report a history of headache in their mothers (adjusted OR 4.17; 95% CI 1.62–10.8), a personal history of carsickness in childhood (aOR 2.95; 95% CI 1.11–7.86), and a high frequency of pre-pregnancy episodes of fatigue (aOR 7.07; 95% CI 2.04–24.5). An indication of an association was also found for multiparity and a diagnosis of allergies.
Odds ratios (OR) and 95% confidence intervals (CI) for selected factors associated with any migraine∗, Dos de Mayo Hospital, Lima, Peru, 2004

Strict and probable migraine.
Each variable adjusted for all other variables in the table.
Discussion
The burden of migraine headaches in women is well characterized in North America and Europe, but few studies have reported the prevalence of migraines in Latin America. To our knowledge, this is the first report attempting to characterize migraine headaches in Peruvian women of reproductive age. The results of this pilot and feasibility study suggest that the prevalence of the migraine syndrome in this population is comparable with the prevalence in similar populations in developed countries.
The results also suggest that the burden of migraine is significantly higher in comparison with non-migrainous headaches in terms of pain severity, frequency of attacks, and use of pharmaceutical treatment. This differential was not shown in the standard MIDAS rankings; the almost uniformly low MIDAS results may simply reflect the inability of this low-income population to miss activities due to headache attacks. Similarly, physician diagnosis of migraine was rare; only four migrainous subjects (8.9%) reported receiving clinical testing for headaches, and only three migrainous subjects (6.7%) had received a physician diagnosis of migraine.
The majority of migraine sufferers reported headache onset after age 13 years, and approximately half reported an association with menstruation. This is consistent with estimates of menstrual migraine in developed countries (29). Approximately half of all headache sufferers reported some degree of pain relief since becoming pregnant; this finding is also consistent with reports of migraine in pregnancy in developed countries (30).
Limitations to interpretation of this study include the cross-sectional study design and the potential influence of language and cultural differences between some of the interviewers and participants. Misclassification of headache type is possible, as indicated by the presence of ‘aura-like’ symptoms and one physician diagnosis of migraine among the non-migrainous participants. The questionnaire also did not ask women to describe multiple headache types, and it is presumed that subjects described the headache episodes most burdensome to them. Underreporting of less severe forms of headache is possible, and must be considered when interpreting the comparison of migrainous with non-migrainous headaches (Tables 2–5). Additionally, our results are limited by the ability of women to accurately recall headaches occurring before the index pregnancy, which may also be influenced by the severity of the headache.
The questionnaire was not validated in the study population. It is possible that the IHS criteria for headache classification are not as accurate in pregnant women; this hypothesis must be tested. This hospital-based pilot study was conducted in an urban population of generally low socioeconomic status, and it would be inadvisable to generalize the findings to the entire Peruvian population. However, information generated by this pilot study will be used to guide the development of future studies of migraine among Peruvians. Future studies ought to include a larger sample and validation of the International Headache Society classification criteria in this population.
In summary, our results suggest that migraine headaches affect a substantial proportion of reproductive-aged women in Peru. Moreover, our results suggest that the population seeking prenatal care in urban, low-income hospitals is under-diagnosed and under-treated in terms of headache disorders. In accordance with ‘Lifting the Burden’, the global campaign against headache, additional studies in this population are necessary to identify the underlying causes of health-care gaps and opportunities for targeted education and treatment (31).
Acknowledgements
The authors wish to acknowledge the contributions of Ms Elena Sanchez Calderon and Ms Miriam Zanabria Roman. This research was supported by awards from the Multidisciplinary International Research Training Program (Fogarty International Center, National Institutes of Health, T37-TW00049) and the Amauta Public Health Practica Program (Puget Sound Partners for Global Health, Bill and Melinda Gates Foundation).