
Abstract
Background
The distinction between a pre-existing primary headache and a secondary headache at the onset of a disorder is important and has not been taken into account in the International Classification of Headache Disorders-3. This study aimed to improve the general diagnostic criteria for secondary headaches using results of our previous studies.
Materials and methods
We analyzed characteristics of headaches including their changes in intensity, duration, frequency, localization and side, development of new accompanying symptoms, and therapeutic response at the onset of transient ischemic attacks (TIA) (n = 120, mean age 56.1, 55% females) and ischemic stroke (n = 550, mean age 63.1, 56% females) compared to the control group (n = 192, mean age 58.7, 64% females).
Results
Headache of a new type occurred in 8.4% of ischemic stroke patients and 5% of TIA patients on the day of admission but did not occur at all in the control group. Pre-existing headache with a change of at least one characteristic occurred significantly more often in stroke (5.4%) and TIA (7.5%) than in the control group (1%) (p = 0.01 and p = 0.003 respectively).
Conclusion
The presence of a new type of headache and a pre-existing headache with altered characteristics in close temporal relation to a disorder indicates causality. Based on these data we propose revised general diagnostic criteria for secondary headaches.
Keywords
Introduction
The distinction between primary headaches, which are independent diseases, and secondary headaches, which are caused by another disease, trauma or substance was not clear in the International Classification of Headache Disorders (ICHD), first edition (1). It became explicit in the two successive editions. According to the first two editions, a secondary headache could be diagnosed only after treatment or remission of its cause had led to the reduction or abolishment of the headache (1,2). This was highly impractical as doctors often need to diagnose headaches before their treatment or remission. This problem was solved in ICHD-3 in which the diagnostic criteria allowed the diagnosis of a secondary headache at the first patient encounter because the new general diagnostic criteria included criteria for causation (2). They gave a basic scheme that could be modified for each different kind of headache. When a new headache occurs for the first time in close temporal relation to another disorder that is known to cause headache, or fulfils other criteria for causation by that disorder, the new headache is coded as a secondary headache attributed to the causative disorder (2). This remains true even when the headache has the characteristics of a primary headache (migraine, tension-type headache, cluster headache or one of the other trigeminal autonomic cephalalgias). When a pre-existing primary headache becomes chronic or is made significantly worse (usually meaning a two-fold or greater increase in frequency and/or severity) in close temporal relation to such a causative disorder, both the primary and the secondary headache diagnoses should be given, provided that there is good evidence that the disorder can cause headache (2).
The majority of the population has a pre-existing headache before they are affected by the secondary cause of the headache. Tension-type headache alone has a one-year prevalence of 75% and migraine has a one-year prevalence of 10-15% (3). The one-year prevalence of having no headaches at all is not known but the lifetime prevalence of never having had a headache is less than 5% (4). Therefore, a distinction between a pre-existing primary headache that just happens in close temporal relation to a secondary cause and a headache caused by the secondary cause is important. This issue was taken into account in ICHD-3 but in the introductory text to the secondary headaches and not in the diagnostic criteria. In our studies of headaches attributed to transient ischemic attacks (TIA) and headaches attributed to ischemic stroke this problem of pre-existing headaches was dealt with for the first time from a scientific point of view. We compared headaches at the onset of TIA and ischemic stroke to headaches in a control group studied at their admission to the hospital for another disorder not affecting the brain. A new kind of headache was found only in the group of stroke/TIA patients and a usual headache with altered characteristics occurred significantly more often in stroke/TIA patients than in the control group and was therefore caused by stroke/TIA.
The present study aimed to analyze typical changes in clinical characteristics of headache at the onset of a disorder using results of our previous studies and on that basis to further develop the general diagnostic criteria for secondary headaches.
Material and methods
This study is based on materials used in several previous publications (5–8). The methodology was described in detail in those studies. Here we give an abbreviated description. Study populations included patients with transient ischemic attacks (n = 120, mean age 56.1, 55% females), patients with first-ever ischemic stroke (n = 550, mean age = 63.1, 56% females) and 192 control patients admitted acutely for another disorder not affecting the brain (mean age = 58.7, 64% females). The most prevalent diagnoses of controls were “lumbago” and “lumbar spine osteochondrosis”. All data were collected prospectively, using a standardized case report form during face-to-face interviews by a neurologist on admission to the emergency room in all groups of patients. Extensive semi-structured interview forms included information about the patients and controls, clinical characteristics of all previous headaches within the past year, the exact day and the hour of onset of TIA and stroke, all clinical characteristics of headaches at onset of stroke or TIA and 24 h after this, headaches in the control group that arose during admission to hospital and 24 h afterwards. The diagnoses of previous and present headaches were made according to the explicit diagnostic criteria of the ICHD-3 (2). Migraine and tension-type headache fulfilling ICHD-3 diagnostic criteria were the predominant previous headache. They were compared to the headaches at the onset of stroke/TIA again according to the diagnostic criteria of the ICHD-3.
All headaches at the time of stroke or TIA or at the time of admission to the hospital in controls (meaning within 24 hours) were compared with headaches during the previous year. If patients had had headaches previously, they were asked if the present headache was different from usual headaches. Those patients, who felt that it was different were then asked about reasons for the difference. They included seven parameters: change in intensity, duration, frequency, localization and side of headache, development of new accompanying symptoms, and therapeutic response. A few patients spontaneously indicated another reason for the difference (for example, vertigo), but this was not recorded. In the present paper, we analyze each of the seven clinical characteristics separately to see if one or more are needed to define “altered characteristics”.
Headaches attributed to stroke/TIA were subdivided into three types: a new type of headache, headache with altered characteristics and headache without altered characteristics. We defined a new type of headache as a headache that developed for the first time within 24 hours after the onset of stroke/TIA. A headache with altered characteristics was defined as a preexisting headache but with changes in characteristics at stroke/TIA onset. If a new type of headache or headache with altered characteristics had a phenotype of migraine or tension-type headache, we called it migraine-like and tension-type-like headache (7). If a preexisting headache occurred unaltered, the diagnosis was headache without altered characteristics (migraine or tension-type headache). We included in modified criteria for headache attributed to stroke not only a new type of headache but also a headache with altered characteristics since they both had significant differences in prevalence in patients with stroke compared to control group (8).
Persistent poststroke headaches were defined according to ICHD-3 as a headache attributed to ischemic stroke (a new type of headache and a headache with altered characteristics) and persisting for more than three months after the stroke has stabilized.
Finally, we develop revised general diagnostic criteria for secondary headaches.
Statistical analysis
Statistical analyses were performed with Stata (v14.0) and Microsoft Excel (2014). The basic comparisons were between patients with ischemic stroke/TIA and controls, and between clinical characteristics of headaches. Univariate analyses were performed to calculate crude odds ratios (ORs) with 95% confidence intervals (CIs). We used χ 2 to compare distributions of categorical variables between groups. When quantitative indicators were evaluated for compliance with a normal distribution, we used the Shapiro–Wilk test (when the number studied was less than 50) or the Kolmogorov– Smirnov test (when the number investigated was more than 50). In the χ2 calculation, if the expected number in at least one cell was less than 10, we calculated the χ2 with Yates correction.
Standard protocol approvals, registrations, and ethical considerations
The study was conducted in accordance with the Helsinki Declaration. The Medical Ethics Committee of the Ural State Medical University approved this study. All respondents were informed of the purpose of the study. Written informed consent was obtained from all participants.
Results
A summary of the results underlying the analysis of the diagnostic criteria is presented in Table 1.
Types of headaches and their characteristics in patients at the onset of stroke and TIA compared to the control group.

The percentage was calculated using the number of patients with changed characteristics in each group.
Headache of a new type did not occur in the control group on the day of admission, but it occurred in 8.4% of ischemic stroke patients and 5% of TIA patients. The difference in the occurrence of these headaches in stroke and TIA patients compared to controls was significant (p < 0.001). Thus, a new type of headache is causally related to TIA or stroke. In contrast, pre-existing headaches (migraine or tension-type headache) without altered characteristics were not more prevalent in stroke/TIA but occurred more frequently in control (4.6%) than in stroke patients (1.1%, p = 0,02) and without significant difference in patients with TIA (6.6.%) and controls (4.6%, p = 0.5) illustrating no etiological relationship.
A pre-existing headache with changes of characteristics occurred significantly more often in association with ischemic stroke (5.4%) and TIA (7.5%) than in the control group where only 1% had such headache (p = 0.01 and p = 0.003 respectively). We systematically recorded seven aspects of these characteristics in TIA/stroke patients and found that only a change in localization and a change of laterality of headache occurred in the control group (Table 2). It occurred in 1% of cases but was found in 40% and 20% of stroke patients. In most cases, stroke/TIA patients encountered a change in more than one of these seven parameters (Table 3).
Description of changes in clinical characteristics of headache in patients with TIA and stroke compared to controls.

Number of changed clinical characteristics in patients with stroke and TIA compared to controls.

Discussion
The main finding in the present study is that a headache that occurs in close temporal relation to an ischemic stroke or transient ischemic attack and fulfills the diagnostic criteria of a previous headache is causally related to the stroke/TIA if the patient feels it is different and if there is a change in one or more of seven clinical characteristics. We show this by comparing patients to an extensive control material and defended this headache as a headache with altered characteristics.
Therefore, new criteria for secondary headaches should include both types of headache: a new type of headache and a headache with altered characteristics. It is important to know the distinctive features of these types of headaches. A new type of headache is a headache which arose for the first time in close temporal relation to a disorder (stroke/TIA or other disorder), therefore it can be attributed to this disorder and represents a secondary headache. A headache with altered characteristics which arose for the first time in close temporal relation to a disorder (stroke/TIA or other disorder) is a previous headache triggered by an underlying disorder which provokes changes in its initial characteristics. Serrano et al. (9) showed that the characteristics of a primary headache can vary over time. In stroke or TIA, the causative event is acute and changes of headache characteristics in such a short time are extremely unlikely. This was also seen in our study as a headache with altered characteristics was very rarely seen in the hospital control group which was studied in parallel with stroke/TIA patients (7). It is interesting to note that headaches with changes of characteristics prevailed in stroke/TIA patients and a new type of headache did not occur at all in controls (5,7). Using this new information, we suggest future revision of the general diagnostic criteria for secondary headaches.
Critique of existing general diagnostic criteria for secondary headaches of the ICHD-3
The main limitation of the existing general diagnostic criteria for the secondary headaches of ICHD-3 is the absence in the criteria of a comparison of clinical characteristics of the presumed secondary headache with a pre-existing headache (Figure 1). This is a problem because migraine has a one-year prevalence of 10–15% and tension-type headache (TTH) at least 75% (4). The prevalence of migraine during one year before stroke was 13.3% and the prevalence of TTH was 62.5% (7).
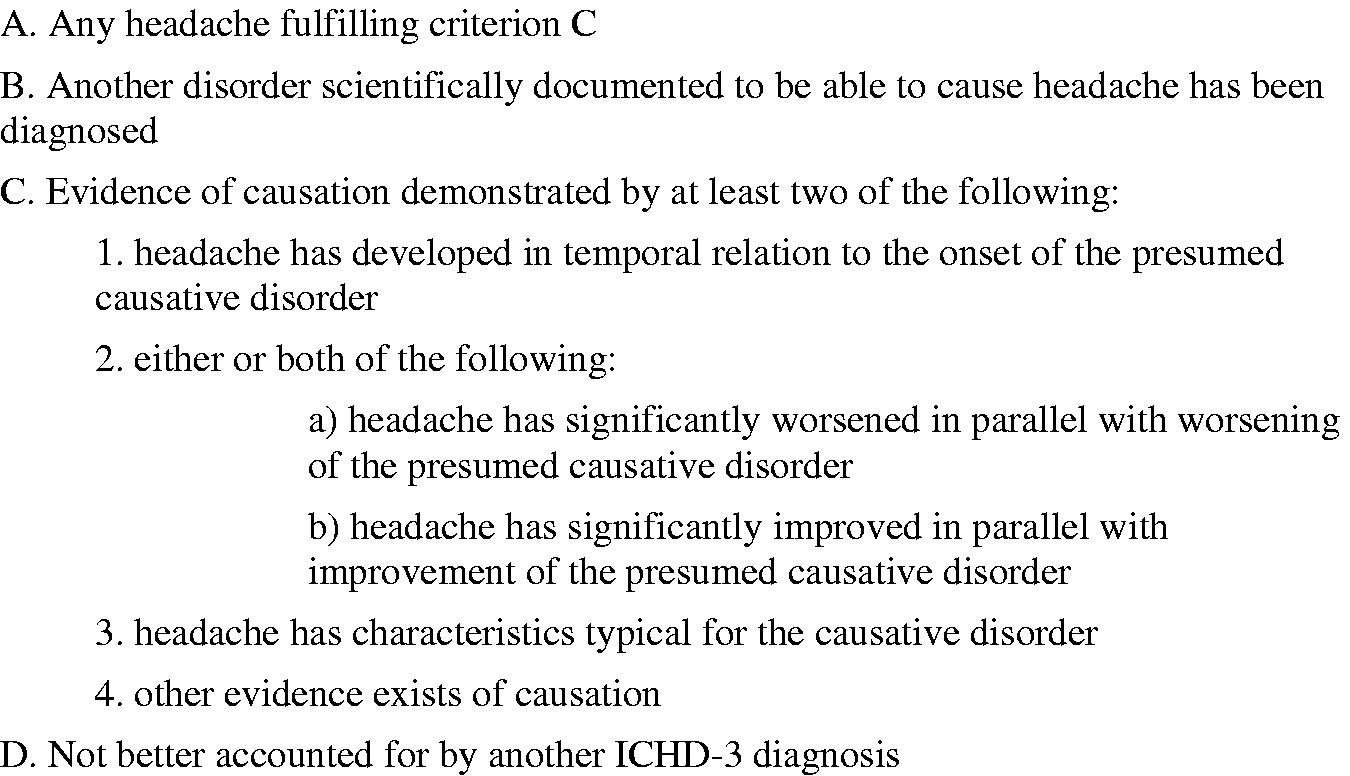
General diagnostic criteria for secondary headaches of the ICHD-3.
Therefore, the great majority of patients who have a headache in close temporal relation to a secondary disorder have a previous primary headache. There is no requirement for a headache attributed to a secondary disorder to be of a new type and there is limited guidance about a headache that phenomenologically fulfils the diagnostic criteria of a pre-existing headache. The comments about this are not in the diagnostic criteria nor dealt with in a footnote. However, in the introductory text to part 2 of ICHD-3, it is specified that if a pre-existing headache is made significantly worse, normally meaning a doubling in frequency, then both the primary headache diagnosis and the secondary headache diagnosis should be given. This is not sufficient for several reasons. First, such an important distinction should not be made in the introductory text because it would often be overlooked. Second, in the acute stage of a disease like ischemic stroke or TIA, it is impossible to diagnose a doubling in the frequency of headaches until a patient has been followed up for a long period. Third, the present study makes it clear that increased frequency is only one changed characteristic that proves the etiological relationship between the ischemic event and headache. In our data, there are seven other changes in the clinical characteristics of headaches, and each of them supports an etiological relationship. For these reasons, it is crucially important to improve the general diagnostic criteria for secondary headaches of the ICHD-3.
Proposal for revised general criteria for secondary headaches
We suggest revised criteria for secondary headaches which distinguish between a new type of headache, a headache of a previous type with altered characteristics and a headache of a previous type without changes in clinical characteristics (Figure 2). The characteristics are outlined in the proposed footnote to criterion C. These characteristics were recorded in patients who had first said yes to the question: Do you feel that this headache is different from your usual headache? Those who said yes were questioned about seven parameters of change and one was enough to establish causality. It must be pointed out that this has been shown only in stroke and TIA. Therefore, it is recommended for other secondary causes of headaches to just rely on patients´ indication that the headache is different and then if needed specify the difference.
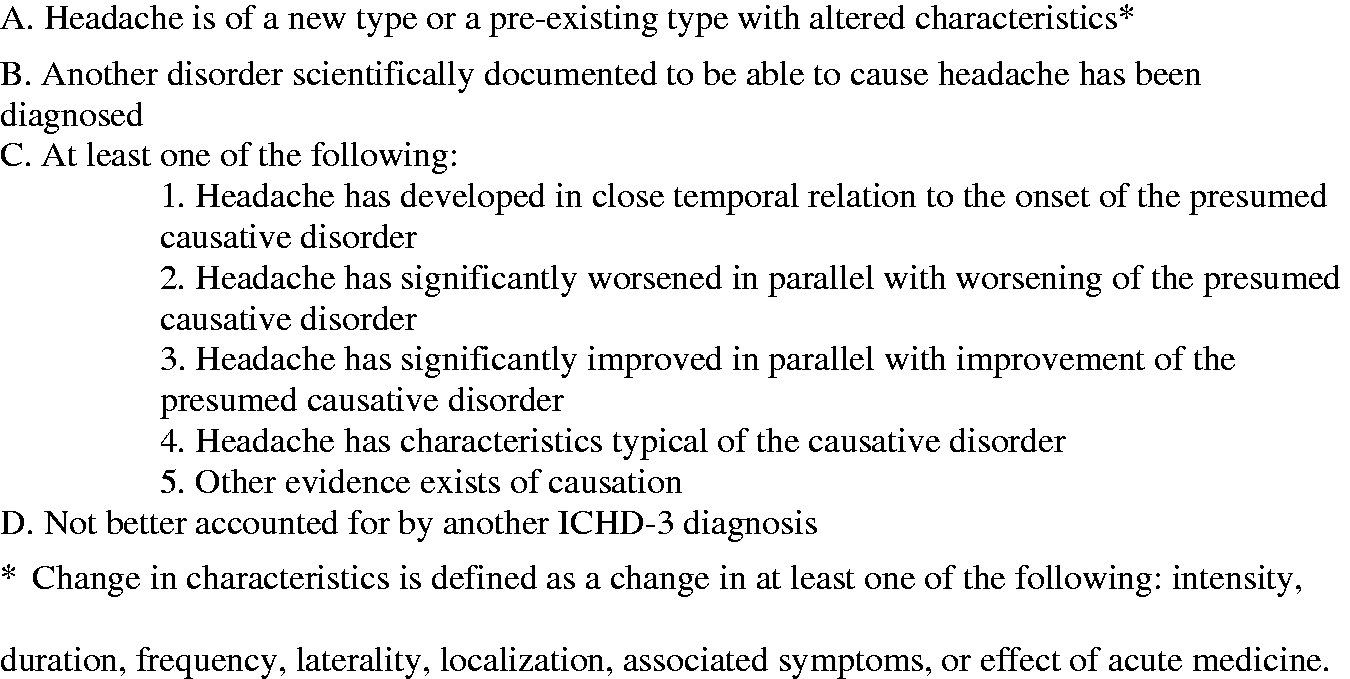
Proposed general diagnostic criteria for secondary headaches.
It might be argued that primary headaches change over time as shown by Serrano et al. (9). In our study of very acute disorders, this was not a problem, but in other types of secondary headaches with more protracted or less known onset, it should be considered.
The new criterion A makes the relation to pre-existing headache clear. For acute diseases, sub-criterion C1 will usually be easy to establish. For diseases with a protracted course, for example headaches attributed to arteriovenous malformation or meningioma, the time relation may be difficult to establish. In this situation criteria C2, 3, 4 and 5 will usually be helpful. The original footnotes in ICHD-3 should be preserved. They explain the criteria in more detail and are not shown here. The new aspect is the footnote to criterion A which presents the different changes in characteristics that in the present study were associated with an etiological relation.
Strengths and weaknesses of the present study
It might be regarded as a weakness that this paper is based only on studies of headaches in stroke and TIA. Studying so many patients with first-ever stroke or TIA and controls in the acute phase after admission is, however, a huge task not likely to be repeated.
According to our previous study, only 60% of the headaches at stroke onset fulfilled the diagnostic criteria of ICHD-3 for acute headaches attributed to ischemic stroke (9) while 100% fulfilled our proposed alternative diagnostic criteria. Our proposed revision of the diagnostic criteria for secondary headaches is therefore an improvement, but the details of the proposal, in particular the seven clinical characteristics regarded as important changes, require further study. A similar methodology to ours is recommended for other acute diseases, for example, for headaches attributed to other cranial or cervical vascular disorders and headaches attributed to trauma/injury. Diseases with a protracted course represent a big challenge in this respect. They will be very difficult to study and may need a separate design.
Conclusion
This study shows that the occurrence of a previous headache such as a migraine or tension-type headache without changes of characteristics in close temporal relation to ischemic stroke or transient ischemic attack is not causal. However, the occurrence of a pre-existing headache with altered characteristics according to seven different parameters indicates a high degree of likelihood that the headache is attributed to stroke or TIA. Based on these data, we have proposed revised general diagnostic criteria for secondary headaches. We recommend that they be considered by the headache classification committee for inclusion in the future revision of the International Classification of Headache Disorders.
Article highlights
It is important to take a careful history of the previous headache as well as of the actual headache and analyze changes in their clinical characteristics at the onset of a disorder for exclusion of a secondary headache. Headaches phenomenologically fulfilling the diagnostic criteria for migraine or tension-type headache can be caused by secondary disorder if they have altered clinical characteristic.
Footnotes
Author contributions
Conceptualization: Jes Olesen; Methodology: Jes Olesen and Elena R. Lebedeva; Formal Analysis: Elena R. Lebedeva and Jes Olesen; Investigation: Elena R. Lebedeva; Data Curation: Elena R. Lebedeva: Writing – Original Draft Preparation: Jes Olesen and Elena R. Lebedeva; Writing – Review & Editing: Elena R. Lebedeva and Jes Olesen.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.