
Abstract
Objective
To investigate whether levcromakalim (a KATP channel opener) induces migraine-like headache in people with persistent post-traumatic headache who had no known history of migraine.
Methods
In a randomized, double-blind, placebo-controlled, 2-way crossover trial, participants were randomly assigned to receive a 20-minute continuous intravenous infusion of levcromakalim (50 µg/mL) or placebo (isotonic saline) on two separate experimental days with a 1-week wash-out period in between. The primary endpoint was the difference in incidence of migraine-like headache between levcromakalim and placebo during a 12-hour observational period after infusion start. The secondary endpoint was the difference in area under the curve for baseline-corrected median headache intensity scores between levcromakalim and placebo during the 12-hour observational period.
Results
A total of 21 participants with persistent post-traumatic headache were randomized and completed the trial. During the 12-hour observational period, 12 (57%) of 21 participants reported experiencing migraine-like headache following the levcromakalim infusion, compared with three after placebo (P = 0.013). Moreover, the baseline-corrected median headache intensity scores were higher following the levcromakalim infusion than after placebo (P = 0.003).
Conclusion
Our findings suggest that KATP channels play an important role in the pathogenesis of migraine-like headache in people with persistent post-traumatic headache. This implies that KATP channel blockers might represent a promising avenue for drug development. Further research is warranted to explore the potential therapeutic benefits of KATP channel blockers in managing post-traumatic headache.
Introduction
Post-traumatic headache (PTH) is a disabling neurological disorder that has received increased attention in recent years (1,2). It impacts millions of persons worldwide and is often attributed to mild traumatic brain injury (TBI) (1,2). In some individuals, PTH can persist for years and is associated with considerable disability, as no evidence-based treatments are available (3). The need for drug discovery is thus a priority, and one possible drug target is the ATP-sensitive potassium (KATP) channels.
A growing body of evidence support the involvement of KATP channels in the pathogenesis of cephalic pain and, in particular, migraine (4–7). This merits emphasis since the clinical presentation of PTH often resembles migraine (8), and recent data indicate the presence of a shared pathophysiological substrate between the two disorders (9–11). In fact, human experimental studies have demonstrated that the signaling molecules calcitonin gene-related peptide (CGRP) and pituitary adenylate cyclase-activating polypeptide-38 (PACAP-38) are implicated in both PTH and migraine (9–11). These observations are intriguing, as binding of CGRP and PACAP-38 to their G protein-coupled receptors is known to result in KATP channel opening on the vascular smooth muscle cells (VSMCs) within the walls of the meningeal arteries (12–16). This causes vasodilation and outflow of potassium ions (6), which is hypothesized to serve as mechanical and chemical stimuli in the activation and sensitization of perivascular meningeal nociceptors (4). However, it remains unknown whether KATP channel opening has a role in the genesis of migraine-like headache in PTH.
Here, we present the findings of a randomized, double-blind, placebo-controlled, 2-way crossover trial assessing the incidence of migraine-like headache after intravenous infusion of the KATP channel opener levcromakalim in persons with persistent PTH who had no history of migraine.
Materials
The relevant ethics committee approved the study protocol, and all participants provided informed consent prior to undergoing any study-related assessments or procedures. The study was registered on ClinicalTrials.gov (identifier: NCT05243953) and conducted in adherence with the principles of the Declaration of Helsinki. Potential participants were identified and enrolled from the outpatient clinic of a tertiary referral hospital.
The data's accuracy and completeness are affirmed by all authors, with the first and senior authors having unrestricted access to the data and being responsible for the initial draft of the manuscript. All authors reviewed and revised the manuscript.
Participants
The study enrolled participants aged 18 to 65 years with persistent PTH due to mild TBI in accordance with the International Classification of Headache Disorders, 3rd edition (ICHD-3) (17). Participants had to report an average of ≥4 headache days per month in the three months prior to enrolment. Exclusion criteria included a history of primary or secondary headache disorders, except for infrequent episodic tension-type headache, prior to the mild TBI. Other exclusion criteria were multiple mild TBIs, moderate-to-severe TBI, whiplash injury, craniotomy, and recent initiation, discontinuation, or change in dosing of preventive headache medication within two months of study enrolment. Eligibility was further confirmed through a review of electronic medical records. The complete list of eligibility criteria can be found in the Online Supplementary Tables 1–2.
Design
The study had a randomized, double-blind, placebo-controlled, 2-way crossover design and was conducted at single center. The allocation concealment, randomization, and drug preparation were performed by independent pharmacy staff.
Participants were allocated to either receive a continuous 20-minute infusion of 20 mL levcromakalim (50 µg/mL) or 20 mL placebo (isotonic saline) in the antecubital fossa on two separate study days. To ensure accurate drug administration, a time- and volume-controlled infusion pump was used. The two study days were separated by a ≥1 week washout period, and the dose of levcromakalim administered was the same as that used in previous human experimental studies (6,7).
Participants who reported taking acute headache medications within 48 hours of the planned infusion start, had a baseline headache intensity of >3 on 11-point numerical rating scale, or had migraine-like headache at infusion start were rescheduled for another study day.
Procedures
When participants arrived on the first study day, trained personnel collected demographic and clinical data. Participants then underwent a physical and neurological examination, during which they were informed that levcromakalim might cause a headache, without disclosing any information about its possible onset, duration, or features. The same procedures were then carried out on both study days. Participants were placed in a supine position, and intravenous access was established through peripheral cannulation of the antecubital fossa. Trained personnel used a 12-hour headache diary to record outcome data, adverse events, and hemodynamic variables at the time of infusion start (i.e., baseline). This process was repeated every 10 minutes until 1 hour after the infusion started, following which participants were discharged and instructed to complete the headache diary hourly until 12 hours post-infusion start.
Statistical analysis
All statistical analyses were carried out using Microsoft Excel (version 2102) and R (version 4.1.0). Characteristics of the study population are reported with means ± standard deviations (SD), medians and interquartile ranges (IQR), or absolute numbers and percentages. Visual inspection and the Shapiro-Wilk test was applied to examine the normal distribution of data, as appropriate. All randomized participants were included in the outcome analyses based on the intention-to-treat principle.
The primary endpoint was the difference in incidence of migraine-like headache between levcromakalim and placebo during the 12-hour observational period post-infusion start. McNemar’s test was used to analyze the results for the primary endpoint and to perform sample size calculations. Twenty-one participants were required to achieve 80% power at a significance level of 5%. This assumed that 50% of participants experience migraine-like headache only after levcromakalim, while 10% would do so only after placebo. The criteria for experimentally-induced migraine-like headache is shown in Figure 1.

Criteria for migraine-like headache.
The secondary endpoint was the difference in area under the curve (AUC) for median headache intensity scores between levcromakalim and placebo during the 12-hour observational period post-infusion start. Baseline correction was applied to the AUC values, which were used as a summary measure in accordance with the trapezium rule (18). This was done to mitigate the potential influence of different headache intensity scores at baseline between the two study days. The Wilcoxon signed-rank test was used to analyze the results for the secondary endpoint. Furthermore, paired t-tests were applied to compare AUC values for the percentage change in respectively mean arterial blood pressure and heart rate between levcromakalim and placebo. Moreover, Fisher’s exact test was used to examine whether there was a carryover effect of levcromakalim compared to placebo on the first study day.
Results
Participants
Of 49 individuals screened for eligibility, 21 were enrolled and completed both experimental days (Figure 2). The most common causes of mild TBI were falls (n = 7) followed by sports-related trauma (n = 5), and traffic accident (n = 4) (Online Supplementary Table 3). The remaining mild TBIs (n = 5) had varied causes, such other unintentional traumas and assault. The participants had a mean age of 40.2 years ± 10.9, and most were women (n = 17) and had a migraine-like phenotype (n = 19). The median duration since the mild TBI was 11.6 (IQR, 4.7 to 11.0) years, and the mean number of monthly headache days were 30.0 ± 9.5. In addition, nine (42%) of 21 participants reported current use of preventive headache medications, and about half (n = 11) had a family history of migraine with or without aura. A more detailed summary of the participants’ demographic and clinical characteristics can be found in Table 1.

Study flow diagram.
Demographic and clinical characteristics of the study population.
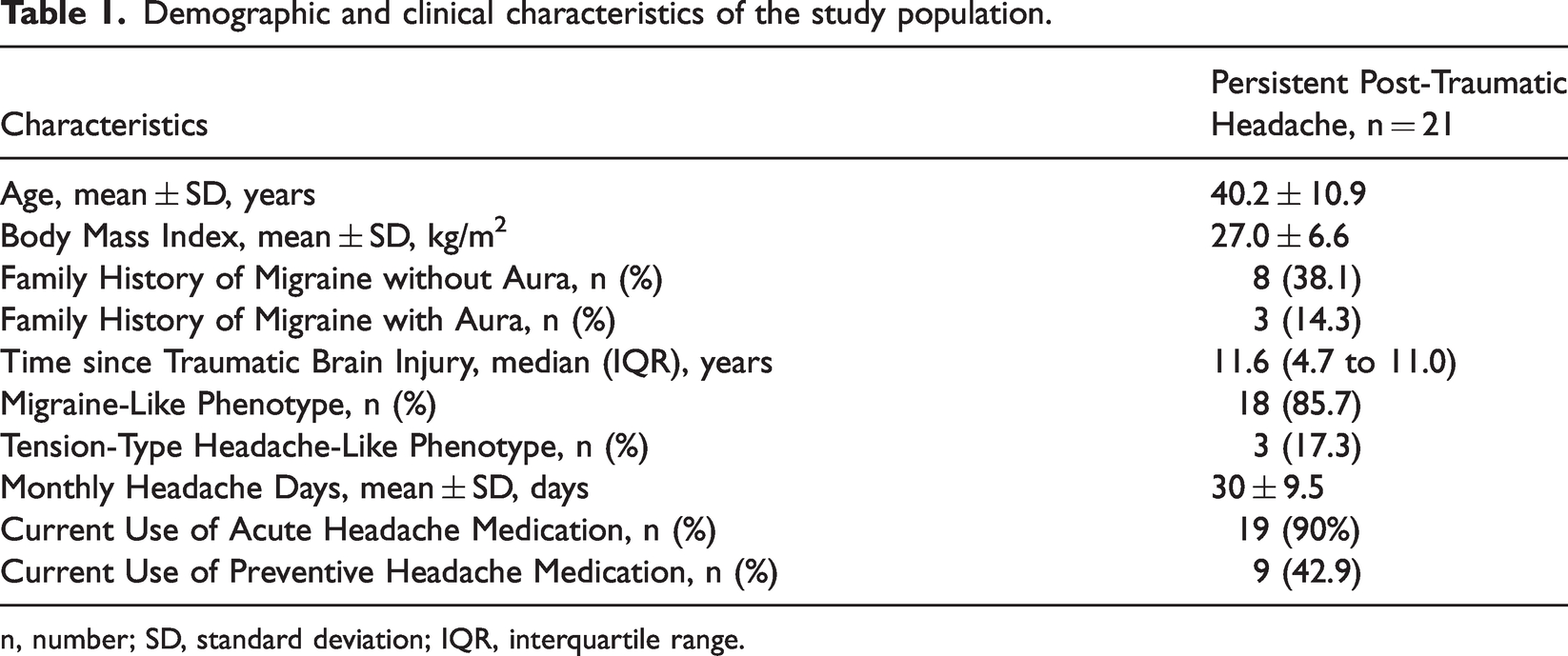
n, number; SD, standard deviation; IQR, interquartile range.
At the time of infusion start, 14 participants experienced a mild headache on levcromakalim day and 12 did so on placebo day. The rest of the participants, at this point, were headache-free prior to receiving their respective infusions. The baseline headache intensity scores and the accompanying symptoms at the time of infusion start on both experimental days are shown in Online Supplementary Table 4.
Migraine-like headache and headache intensity scores
Twelve (57%) of 21 participants experienced migraine-like headache during the 12-hour observational period after levcromakalim infusion, whereas only three participants did so after placebo (P = 0.013; Table 2). In addition, nine of 21 participants experienced migraine-like headache only after receiving levcromakalim, of which three participants did so on both levcromakalim and placebo day. Of note, no participants reported migraine-like headache exclusively after placebo. During the 1-hour in-hospital period, seven of 21 participants experienced migraine-like headache after levcromakalim, whereas only one participant did so following placebo.
Characteristics of migraine-like headache after levcromakalim and placebo.

No, number; TTH, tension-type headache; Bilat, bilateral; Throb, throbbing; Unilat, unilateral; Pres, pressing: NA, not applicable; Comb, combined throbbing and pressing quality of headache.
aLocalization (unilateral, bilateral)/pain intensity (11-point numeric rating scale, with 0 indicating no headache and 10 indicating the worst headache imaginable)/quality of headache (throbbing, pressing, combined throbbing and pressing)/aggravation of headache by routine physical activity (plus denotes presence, minus denotes absence).
bThe participant is asked to determine whether the headache following levcromakalim or placebo infusion resembles his/her, if applicable, usual migraine-like headache.
cMigraine-like headache is defined by the criteria outlined in Table 1.
Associated symptoms are nausea, photophobia, and phonophobia. Worsening is defined as an increase in the severity of these symptoms at the onset of migraine-like headache compared with baseline (i.e., time of infusion start), as rated on a 4-point Likert scale (0 = none, 1 = mild, 2 = moderate, 3 = severe).
The baseline-corrected AUC for median headache intensity scores was higher after levcromakalim than placebo (P = 0.003; Figure 3A). Notably, levcromakalim infusion resulted in a median peak headache intensity of 6 (IQR, 4 to 7), with the median time to reach this peak intensity occurring 240 minutes (IQR, 120 to 360) post-infusion.

(A). Baseline-corrected median headache intensity scores after levcromakalim and placebo. The median headache intensity scores, adjusted for baseline values, after levcromakalim and placebo infusion over the 12-hour observational period. The data is represented with median headache intensity scores after levcromakalim (red line) and placebo infusion (black line). (B). Baseline-corrected mean arterial blood pressures after levcromakalim and placebo. The mean arterial blood pressure values, adjusted for baseline values, after levcromakalim and placebo infusion over the 60-min in-hospital observational period. The data is represented with mean arterial blood pressure after levcromakalim (red line) and placebo infusion (black line) and (C). Baseline-Corrected Mean Heart Rates after Levcromakalim and Placebo. The mean heart rate values, adjusted for baseline values, after levcromakalim and placebo infusion over the 60-min in-hospital observational period. The data is represented with mean heart rate after levcromakalim (red line) and placebo infusion (black line).
The peak headache following levcromakalim infusion was primarily characterized by its bilateral location (n = 19), a pressing sensation (n = 16), and a pain intensity that was graded as moderate to severe (n = 19). Furthermore, 12 participants reported aggravation of head pain in response to routine physical activity. Concomitant symptoms manifested as photophobia (n = 13), phonophobia (n = 7), and nausea or vomiting (n = 7).
Adverse events, use of rescue medication and hemodynamic variables
The adverse events observed included palpitations, flushing, and warm sensations, which occurred more frequently after levcromakalim than placebo (P < 0.05 for all). Furthermore, 11 of 21 participants reported use of rescue medication to treat their headache, whereas two did so after placebo. In terms of hemodynamic variables, the baseline-corrected AUC for mean arterial blood pressure did not differ after levcromakalim than placebo (P = 0.103; Figure 3B), while the baseline-corrected AUC for mean heart rate was lower after levcromakalim than placebo (P = 0.05; Figure 3C).
Discussion
The present randomized, placebo-controlled trial showed that the KATP channel opener levcromakalim induces migraine-like headache in people with persistent PTH who had no known history of migraine. In addition, the provoked migraine-like headache resembled the participants' usual spontaneous episodes of migraine-like headache, suggesting that the underlying disease mechanisms are shared between the two. The implications are then that KATP channel opening facilitates the genesis of cephalic pain and more importantly migraine-like headache in people with persistent PTH. This, in turn, raises the prospect of addressing unmet treatment needs in PTH by developing KATP channel blockers.
KATP channel involvement in headache disorders
In recent years, there has been growing interest in the role of KATP channels in the disease mechanisms underlying headache disorders (6,7,19–22). Past research indicates that levcromakalim induces a specific headache phenotype corresponding to the diagnosed headache disorder of participants within various study populations. More precisely, people with migraine develop migraine attacks (6,7), while those with cluster headache report cluster headache attacks (23). In contrast to this, levcromakalim elicits mild or no headache in healthy volunteers (24).
Magnetic resonance angiography has further deepened our understanding of KATP channel involvement in headache disorders. A randomized controlled trial reported that intravenous infusion of levcromakalim elicited a more pronounced dilation of the middle meningeal artery (MMA) in healthy individuals, compared with placebo (24). Importantly, this dilation was found to be more marked during the presence of a headache. In contrast, no significant changes in diameter were observed for the middle cerebral artery (MCA) (24). This indicates that intravenous levcromakalim infusion dilates extracerebral intracranial arteries, such as the MMA, while leaving intracerebral arteries like the MCA unaffected.
Possible sites and mechanisms of action
Levcromakalim is the third inducer of migraine-like headache to be identified in people with persistent PTH (10,11). The first one is CGRP, which elicited a 70% induction rate of migraine-like headache, compared with only 20% after placebo (10). A critical question is then: what is the relative contribution of KATP channel opening and CGRP to the pathogenesis of spontaneous episodes with migraine-like headache? The answer remains unknown and is an area ripe for novel scientific discoveries.
Another important question pertains to the site(s) and mechanism(s) of action by which KATP channel opening causes migraine-like headache. One possible site of action is the meningeal vasculature. It is known that levcromakalim dilates the MMA in healthy individuals (24,25), and ex vivo rodent data supports that this dilation is mediated by opening of KATP channels (26). The efflux of positively charged potassium ions from VSMCs and accompanying vasodilation is posited to activate and sensitize perivascular nociceptors, ultimately resulting in the perception of migraine-like headache (Figure 4) (4,5). This hypothesis aligns well with experimental data showing that intravenous infusion of CGRP can induce migraine-like headache in people with persistent PTH (10). Here, it merits emphasis that CGRP is a potent dilator of the MMA (27,28), and this dilation is mediated via opening of KATP channels (6,7,19). Further research is, nonetheless, needed to ascertain whether the effects of KATP channel opening on the meningeal vasculature and its perivascular nociceptors contributes to migraine-like headache in PTH and other headache disorders.

Possible mechanism and site of action of KATP channel opening in the pathogenesis of migraine-like headache in people with persistent PTH. The figure illustrates a hypothesized mechanism and site of KATP channel opening in the development of migraine-like headache in people with persistent PTH. It highlights the involvement of the signaling molecules CGRP and PACAP, both of which bind to G protein-coupled receptors on VSMCs of meningeal arteries, activating cAMP-dependent pathways and opening KATP channels. The resulting potassium efflux and the accompanying vasodilation serve to activate and sensitize the perivascular meningeal nociceptors, a process facilitated by both chemical and mechanical stimulation. PTH = post-traumatic headache, CGRP = calcitonin gene-related peptide, PACAP-38 = pituitary adenylate cyclase-activating polypeptide-38; VSMCs = vascular smooth muscle cells; AC = adenylate cyclase; ATP = adenosine triphosphate; cAMP = cyclic adenosine monophosphate; KATP channels = ATP-sensitive potassium channels.
A less probable site of action is the primary afferents of the trigeminal ganglion and upper cervical ganglia, which provide nociceptive innervation to meninges and its vasculature (29). The opening of KATP channels leads to the efflux of positively charged potassium ions, resulting in hyperpolarization of the primary afferents (4,6). This suggests an anti-nociceptive effect of KATP channel openers (e.g., levcromakalim) (30), and there were previous speculations about their potential to treat headaches (31). This notion has now been debunked, but it might be asserted that hyperpolarization mediated by KATP channel opening results in the activation of hyperpolarization-activated cyclic nucleotide-gated (HCN) channels on the primary afferents (32). Upon activation, HCN channels lead to depolarization and generation of action potentials (32–34). This would then translate into a pro-nociceptive effect and explain how opening of KATP channels on the primary afferents can elicit migraine-like headache. However, the forehead is also innervated by primary afferents of the trigeminal ganglion, but neither intradermal nor intramuscular administration of levcromakalim to the forehead elicited pain in healthy individuals (35). Thus, the concept of HCN channel involvement remains speculative, and studies are needed to test whether pre-treatment with a HCN channel blocker can prevent migraine-like headache induced by KATP channel openers, such as levcromakalim.
KATP channel opening in PTH versus migraine
A notable aspect of our results is the observed 57% induction rate of migraine-like headache in people with persistent PTH. This contrasts previous studies that reported a 100% induction rate of migraine attacks in people with migraine without aura, and 82% for those with migraine with aura (6,7). Considering the identical dose and infusion duration across these studies, the observed differences indicate a less pronounced role of KATP channel opening in the pathogenesis of PTH than in migraine. Moreover, it is plausible that the molecular and cellular underpinnings of PTH differ somewhat from those of migraine, resulting in varied responses to levcromakalim. Further investigations are thus needed to refine our understanding on the role of KATP channels in the pathogenesis of different headache disorders.
Targeting KATP channels in PTH
Our findings highlight the promising avenue of drug development that targets KATP channels in people with PTH. A potential strategy is to design drugs blocking the KATP channels. This approach might inhibit the intracranial vasodilation and subsequent activation of the trigeminovascular system, processes believed to be central to the genesis of cephalic pain (4,5). However, it is important to consider the multifaceted roles of KATP channels in other physiological processes, such as the regulation of insulin secretion and cardiac function (36,37). Therefore, these blockers must be carefully designed to minimize potential side effects. An option might be to develop drugs blocking the Kir6.1-SUR2B subtype of the KATP channels, which is expressed on the VSMCs of the intracranial arteries (38,39).
The timing of intervention with KATP channel blockers in the treatment of PTH is a critical aspect that warrants careful consideration. The initiation of drug administration in the early stages of the disease might lead to the most beneficial therapeutic outcomes. In this context, it is important to take note of the available evidence related to CGRP signaling in concussed rodents (40,41). The downstream vascular effects of CGRP involve opening of KATP channels (4,5). This knowledge is particularly relevant as it provides a mechanistic link between CGRP signaling and the potential therapeutic benefits of KATP channel blockers. Recent findings in concussed rodents have shown that the inhibition of CGRP signaling can prevent cutaneous allodynia (a surrogate marker of headache chronification) in the early stages post-concussion (42). However, this effect does not extend to the later stages after concussion, indicating a time-sensitive window for drug intervention. This discovery might be linked to the role of diffuse noxious inhibitory controls (DNIC), a physiological mechanism important to descending pain modulation (43). A loss of DNIC, observed in concussed rodents (44), results in a diminished capacity of the brain to inhibit ascending pain signals which, in turn, can lead to headache chronification and persistence. Interestingly, it has been found that the inhibition of CGRP signaling can prevent the loss of DNIC in concussed rodents (42). It would thus be insightful to explore whether the administration of a KATP channel blocker can produce similar results in concussed rodents. If such an association is found, it suggests that KATP channel blockers are most effective when administered in the early stages following mild TBI. Despite the promising implications of our results, more experimental research is needed to ascertain the role of KATP channels in the pathogenesis of PTH. This includes the development of effective and safe drugs that target these channels. Further investigations should encompass preclinical studies to explore the effects of KATP channel openers and blockers in animal models of PTH, paving the way for potential clinical trials. It is nonetheless important to acknowledge that the underpinnings of PTH are likely to encompass a plethora of pathophysiological mechanisms. While our results elucidate the potential role of KATP channels, it represents just one piece of the intricate puzzle. Other molecular and cellular pathways are also involved and merit further investigation. Our findings, while shedding light on one avenue, should be interpreted in the broader context of PTH’s diverse pathophysiological landscape.
Limitations
The present trial has certain limitations that must be acknowledged. One limitation is the in-hospital observational period, which was limited to 1 hour after the infusion started due to feasibility constraints. Consequently, we cannot rule out the possibility that environmental factors (e.g., specific foods, stress) might have influenced the outcome data during the remaining 11 hours of the observational period. However, it is worth noting that most participants who experienced migraine-like headache after levcromakalim reported its onset during the in-hospital period. Another important consideration is the potential impact of preventive headache medication, which was being used by about half of the participants. It is possible that the use of preventive medication reduces the likelihood of inducing migraine-like headache. However, among the 12 participants who reported migraine-like headache after levcromakalim, five were using preventive medication while seven were not. Further investigations are warranted to explore these limitations and their potential influence on the development of migraine-like headache. A third limitation pertains to using the term ‘migraine-like headache’. It is important to note that migraine-like headache can manifest in a plethora of headache disorders (17). Our findings might therefore extend to other headache disorders as well. Hence, it is possible that the disease mechanisms underlying migraine-like headache are shared across headache disorders. Moreover, it is worth noting that the use of migraine-like headache as a primary endpoint does not capture the entire spectrum of headache features and accompanying symptoms unique to each individual with persistent PTH. Yet, it permits some individual variation and captures the phenotype of most patients with persistent PTH in clinical samples. Finally, it also merits mention that our study population represents a subset of people with persistent PTH, who are severely affected. The reason for this is that the participants were referred from a tertiary care unit which skews our population towards people with more severe manifestations of PTH. Future research might benefit from a more diverse sample, including a wider spectrum of people with PTH.
Conclusions
Our results suggest that KATP channels are likely to play a key role in the neurobiological underpinnings of PTH, as demonstrated by the induction of migraine-like headache in people with PTH following administration of levcromakalim. Therefore, KATP channel blockade might represent a potential drug target for PTH. Further research is needed to elucidate the exact mechanism and site of action of KATP channels in disease mechanisms underlying PTH.
Key findings
In this randomized, double-blind, placebo-controlled, 2-way crossover trial, levcromakalim significantly induced a higher incidence of migraine-like headache in people with PTH, compared to placebo. KATP channels are presumed to have a pivotal role in the neurobiological foundations of migraine-like headache in people with persistent PTH. Blockade of KATP channels may constitute a promising pharmacological target for the management of PTH.
Supplemental Material
sj-pdf-1-cep-10.1177_03331024231210930 - Supplemental material for Hypersensitivity to opening of ATP-sensitive potassium channels in post-traumatic headache
Supplemental material, sj-pdf-1-cep-10.1177_03331024231210930 for Hypersensitivity to opening of ATP-sensitive potassium channels in post-traumatic headache by Haidar M. Al-Khazali, Rune H. Christensen, David W. Dodick, Basit Ali Chaudhry, Rami Burstein and Håkan Ashina in Cephalalgia
Footnotes
Author contributions
Study concept and design: HA; Data acquisition and analysis: HMA, RHC, BAC, HA; Drafting of the manuscript: HMA, RHC, HA; Critical revision of the manuscript: HMA, RHC, DWD, BAC, RB, HA; Funding acquisition: HA.
Availability of data and materials
Upon reasonable request, the corresponding author will provide the necessary data and materials to interested researchers for the purpose of academic scrutiny, reproducibility, and further scientific investigation.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: DWD. reports the following competing interests. Consulting: Amgen, Atria, CapiThera Ltd., Cerecin, Ceruvia Lifesciences LLC, CoolTech, Ctrl M, Allergan, AbbVie, Biohaven, GlaxoSmithKline, Lundbeck, Eli Lilly, Novartis, Impel, Satsuma, Theranica, WL Gore, Genentech, Nocira, Perfood, Praxis, AYYA Biosciences, Revance, Pfizer. Honoraria: American Academy of Neurology, Headache Cooperative of the Pacific, Canadian Headache Society, MF Med Ed Research, Biopharm Communications, CEA Group Holding Company (Clinical Education Alliance LLC), Teva (speaking), Amgen (speaking), Eli Lilly (speaking), Lundbeck (speaking), Pfizer (speaking), Vector Psychometric Group, Clinical Care Solutions, CME Outfitters, Curry Rockefeller Group, DeepBench, Global Access Meetings, KLJ Associates, Academy for Continued Healthcare Learning, Majallin LLC, Medlogix Communications, Medica Communications LLC, MJH Lifesciences, Miller Medical Communications, WebMD Health/Medscape, Wolters Kluwer, Oxford University Press, Cambridge University Press. Non-profit board membership: American Brain Foundation, American Migraine Foundation, ONE Neurology, Precon Health Foundation, International Headache Society Global Patient Advocacy Coalition, Atria Health Collaborative, Arizona Brain Injury Alliance, Domestic Violence HOPE Foundation/Panfila. Research support: Department of Defense, National Institutes of Health, Henry Jackson Foundation, Sperling Foundation, American Migraine Foundation, Henry Jackson Foundation, Patient Centered Outcomes Research Institute (PCORI). Stock options/shareholder/patents/board of directors: Aural analytics (options), Axon Therapeutics (shares/board), ExSano (options), Palion (options), Man and Science, Healint (options), Theranica (options), Second Opinion/Mobile Health (options), Epien (options), Nocira (options), Matterhorn (shares), Ontologics (shares), King-Devick Technologies (options/board), EigenLyfe (shares), AYYA Biosciences (options), Cephalgia Group (shares/board), Atria Health (options/employee). Patent 17189376.1-1466:vTitle: Onabotulinum Toxin Dosage Regimen for Chronic Migraine Prophylaxis (Non-royalty bearing). Patent application submitted: Synaquell® (Precon Health). In addition, R.B. has received honoraria, acted as a consultant or advisory board member for Alder, Allergan, Amgen, Autonomic Technologies, Avanir, Biohaven, CGRP Diagnostics, Dr. Reddy's Laboratories, ElectroCore, Eli Lilly, GlaxoSmithKline, Merck, Pernix, Teva, and Trigemina. RB also reports receiving CME fees from Healthlogix, Medlogix, and WebMD/Medscape, and holds patents for several products, including (9061025, 11732265.1, 10806890, US2021-0015908, WO21007165, US2021-0128724, WO21005497). RB is a reviewer for the National Institute of Neurological Disorders and Stroke (NINDS) and holds stock options in Allay Lamp and Percept, outside of the submitted work. HA reports personal fees from Teva, outside of the submitted work. HMA reports personal fees from Pfizer, outside of the submitted work. The remaining authors declare no competing interests.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from the research council of Copenhagen University Hospital – Rigshospitalet (E-23831-03 to H.A.), Hartmann Foundation (A37853 to H.A.), and Lundbeck Foundation (R373-2021-1199 to H.A.).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.