
Abstract
Objective
To perform a systematic review and meta-analysis of the epidemiology, precipitants, phenotype, comorbidities, pathophysiology, treatment, and prognosis of primary new daily persistent headache.
Methods
We searched PubMed/Medline, EMBASE, Cochrane, and clinicaltrials.gov until 31 December 2022. We included original research studies with any design with at least five participants with new daily persistent headache. We assessed risk of bias using National Institutes of Health Quality Assessment Tools. We used random-effects meta-analysis where suitable to calculate pooled estimates of proportions. The Preferred Reporting Items for Systematic Reviews and Meta-Analysis compliant study is registered with PROSPERO (registration number CRD42022383561).
Results
Forty-six studies met inclusion criteria, predominantly case series, including 2155 patients. In 67% (95% CI 57–77) of cases new daily persistent headache has a chronic migraine phenotype, however new daily persistent headache has been found to be less likely than chronic migraine to be associated with a family history of headache, have fewer associated migrainous symptoms, be less vulnerable to medication overuse, and respond less well to injectable and neuromodulatory treatments.
Conclusions
New daily persistent headache is a well described, recognisable disorder, which requires further research into its pathophysiology and treatment. There is a lack of high-quality evidence and, until this exists, we recommend continuing to consider new daily persistent headache a distinct disorder.
Introduction
A new daily persistent headache (NDPH) is a headache which begins suddenly and then persists without any remission periods for at least three months, with the affected person often able to remember the exact time and circumstances of the onset (1). The syndrome of NDPH has a variety of secondary causes which are important to recognise as the underlying cause is usually treatable, and if untreated can lead to other forms of neurological disability. NDPH can also occur as a primary headache disorder, where it usually has a similar phenotype to either chronic migraine (CM) or chronic tension-type headache (CTTH) which have transformed from an episodic headache disorder.
The term “new daily persistent headache” was first used by Vanast (2) in 1986 to describe a series of 45 patients who had no history of headache until they suddenly developed chronic daily headaches, often preceded by a viral illness. Vanast followed up this group of patients with NDPH and in the majority the headaches had largely stopped, causing him to describe it as a benign self-limiting form of primary headache (2). This contrasts with more recent evidence and the opinion of many headache experts, who consider primary NDPH to be the most treatment refractory primary headache disorder (3–5).
A systematic review of NDPH (without meta-analysis) was published in 2019, at which point published studies of NDPH were limited to fewer than 100 patients (6). Since 2020, several large series of patients with primary NDPH have been published in both children/adolescents and adults, that have included between 155 and 328 patients, respectively (7–10). Studies have also begun to interrogate its relationship and differentiation from CM and/or CTTH (8,9,11,12). Several studies have also recently been published using functional or structural neuroimaging, which may help to illuminate its pathophysiology (13–15).
Objectives
To perform a systematic review of the existing literature on primary NDPH including its epidemiology, precipitants, phenotype, comorbidities, pathophysiology, treatment, and prognosis.
Methods
We performed a systematic review of the published literature on primary NDPH. The study is compliant with the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) reporting guidelines (16), and is registered with PROSPERO (registration number CRD42022383561). The protocol was not pre-published.
Search strategy
We searched four electronic databases (PubMed/Medline, EMBASE, Cochrane, and clinicaltrials.gov) with the search terms “new daily persistent headache”, “new onset persistent headache” and “daily persistent headaches”, from inception until 31 December 2022. Duplicates and non-English language articles were removed before screening. Reference lists of previous review publications were also reviewed for additional relevant references, although no additional references which met the inclusion criteria were identified using this method.
Selection criteria
Titles and abstracts were screened and assessed for eligibility against the inclusion criteria by two investigators independently (SC and DM), followed by discussion to reach consensus on any discordant records, including a third investigator (MSM) where there was disagreement. We included original research studies with any study design, which included NDPH by the International Classification of Headache Disorders 2nd or 3rd Editions (ICHD-2 and ICHD-3) (1,17) or the modified ICHD-2 criteria proposed by Kung et al. (18). For analysis of migraine symptoms and the proportion of patients with symptoms meeting criteria for CM and CTTH, studies using solely ICHD-2 criteria were excluded, as this by definition excludes those with migraine symptoms. Case reports and case series including less than five patients with NDPH were excluded, other than for epidemiological studies where there was no minimum number of patients with NDPH required for inclusion. Reports of treatment response where the total number of patients who received a treatment was not reported were not included when assessing treatment responses. Studies which included patients with NDPH but that did not report results for NDPH separately from other patients with chronic daily headache were excluded. Conference abstracts were excluded as methodological quality could not be assessed. Studies which included adults or children/adolescents were included but results were reported separately.
Data extraction
To avoid bias due to duplication only the largest case series per research group was included for analysis of each research question. Articles were assessed for information relating to the following research questions, for which data was extracted by a single author:
Epidemiology
What is the prevalence of NDPH? What is the incidence of NDPH? What proportion of patients with chronic daily headache have NDPH? What proportion of patients with NDPH have a family history of headache?
Precipitants
What proportion of patients with NDPH have a precipitant? What proportion are precipitated by each of the following: infection, stressful life event, extracranial surgery?
Phenotype
What proportion of patients with NDPH had an episodic headache disorder prior to the onset of NDPH? What proportion of patients with NDPH have each of the following characteristics typically used in headache classification: unilateral pain location, throbbing pain quality, moderate to severe pain intensity, nausea, vomiting, photophobia, phonophobia, motion sensitivity, cranial autonomic symptoms? What proportion of patients with NDPH meet criteria for CM and CTTH?
Comorbidities
What proportion of patients with NDPH have medication overuse? What proportion of patients with NDPH have depression, anxiety, or any other comorbidity which has been studied?
Pathophysiology/biomarkers
Are there any biomarkers (e.g., serological markers or imaging features) which can distinguish NDPH from other headache disorders or non-headache controls? What is the pathophysiology of NDPH?
Treatment
What proportion of patients with NDPH respond to non-pharmacological interventions? What proportion of patients with NDPH respond to acute analgesics or triptans? What proportion of patients with NDPH respond to preventive medications typically used in migraine or tension-type headache? What proportion of patients with NDPH respond to injectable or neuromodulatory treatments?
Prognosis
What proportion of patients with NDPH become pain free over time, either treated or untreated?
Risk of bias assessment
Included articles were assessed for risk of bias by two authors independently (SC and DM), using the National Institutes of Health Quality Assessment Tools for cross-sectional studies, case-control studies, or case series studies, depending on the study type. Retrospective cohort studies were assessed using the tool for case series studies.
Statistical analysis
For several of the research questions, the pooled estimates of proportions (with 95% CI) were synthesised using random-effects meta-analysis, using the command metaprop of the software Stata Version 17.0. For meta-analysis of headache phenotype variables only studies which included at least 20 patients with NDPH were included. For all meta-analyses performed, forest plots were generated (shown in the online supplementary material), and the I2 measure was calculated to assess heterogeneity. For research questions where meta-analysis was not possible due to heterogeneity of studies and lack of standardised outcome measures, descriptive data is presented.
Results
The search resulted in 521 unique records, of which 46 met inclusion criteria and included a total of 2155 patients diagnosed with NDPH. PRISMA flowchart of study identification is shown in Figure 1. Of the 46 included reports, 33 related to adults and 13 to children and/or adolescents. The majority (33) were case series or retrospective cohort studies, 10 were case control studies, and three were cross-sectional studies.

PRISMA flow diagram of study identification and inclusion.
No prospective cohort studies or randomised controlled trials were identified. Data on the individual studies, including quality (risk of bias) assessment, is shown in the online supplementary material.
Epidemiology
Primary NDPH is relatively rare, with the only adult study meeting inclusion criteria finding a prevalence of 0.03% (19), and the only paediatric study meeting inclusion criteria finding no cases in a population of 7900 (20). Both studies used ICHD-2 diagnostic criteria for NDPH and estimates using the newer ICHD-3 criteria which includes those with migraine symptoms are likely to be higher. The only epidemiological study which has reported incidence of NDPH after a particular trigger found that 3/450 (0.67%) cases of dengue fever went on to develop NDPH (21). Although still less common than chronic migraine, NDPH appears to make up a larger proportion of chronic daily headache in children and adolescents than adults (22). The exact proportion varies depending on the population studied and diagnostic criteria used, with an estimated pooled proportion of 18% (95%CI 8–27) of children/adolescents and 4% (95%CI 3–6) of adults with chronic daily headache meeting criteria for NDPH (see Table 1 and online Supplementary Figure 1).
NDPH as a proportion of chronic daily headache.

ICHD-2, International Classification of Headache Disorders 2nd Edition; M-ICHD-2, Modified ICHD-2 criteria including patients with migraine features; ICHD-3β, ICHD 3rd edition beta version.
Forest plots of meta-analyses used to calculate pooled estimates of proportions are shown in the online supplementary material.
In most studies NDPH is about twice as common in females (9,10,23). In studies of children in the northern hemisphere, the onset of NDPH is most common either in early-autumn or January, but there does not appear to be a seasonal pattern in adults (8,10,12,24).
Onset and precipitants
The onset of primary NDPH is typically clearly remembered by the affected patient. In an estimated proportion of 40% of patients the onset of NDPH is linked to a precipitating illness or event, most commonly a systemic infection (usually a flu-like illness), stressful life event, or extracranial surgery (see Table 2 and online Supplementary Figures 2–5).
Precipitating events for NDPH.

≥ used to indicate that total number may be higher as only specific precipitants or infections were mentioned in the manuscript.
ICHD-2, International Classification of Headache Disorders 2nd Edition; M-ICHD-2, Modified ICHD-2 criteria including patients with migraine features; ICHD-3β, ICHD 3rd edition beta version.
Forest plots of meta-analyses used to calculate pooled estimates of proportions are shown in the online supplementary material.
Phenotype and classification
Several iterations of diagnostic criteria have been proposed for primary NDPH. In the ICHD-2 classification, to be diagnosed as primary NDPH the headache should have minimal or no other associated symptoms (17). In contrast, according to current ICHD-3 diagnostic criteria, the diagnosis of primary NDPH is made based on the abrupt onset and persistency of the headache, rather than any of its characteristics or associated symptoms (see Table 3) (1).
ICHD-3 criteria for primary new daily persistent headache.

Notes: 1. 4.10 New daily persistent headache is unique in that headache is daily from onset, and very soon unremitting, typically occurring in individuals without a prior headache history. Patients with this disorder invariably recall and can accurately describe such an onset; if they cannot do so, another diagnosis should be made. Nevertheless, patients with prior headache (1. Migraine or 2. Tension-type headache) are not excluded from this diagnosis, but they should not describe increasing headache frequency prior to its onset. Similarly, patients with prior headache should not describe exacerbation associated with or followed by medication overuse.2. 4.10 New daily persistent headache may have features suggestive of either 1. Migraine or 2. Tension-type headache. Even though criteria for 1.3 Chronic migraine and/or 2.3 Chronic tension-type headache may also be fulfilled, the default diagnosis is 4.10 New daily persistent headache whenever the criteria for this disorder are met. In contrast, when the criteria for both 4.10 New daily persistent headache and 3.4 Hemicrania continua are met, then the latter is the default diagnosis.3. Abortive drug use may exceed the limits defined as causative of 8.2 Medication-overuse headache. In such cases, the diagnosis of 4.10 New daily persistent headache cannot be made unless the onset of daily headache clearly predates the medication overuse. When this is so, both diagnoses, 4.10 New daily persistent headache and 8.2 Medication-overuse headache, should be given.4. In all cases, other secondary headaches such as 5.1 Acute headache attributed to traumatic injury to the head, 7.1 Headache attributed to increased cerebrospinal fluid pressure and 7.2 Headache attributed to low cerebrospinal fluid pressure should be ruled out by appropriate investigations.ICHD-3, International Classification of Headache Disorders 3rd edition.
We found that that migrainous symptoms are present in a large proportion of patients with NDPH. Nausea or vomiting, photophobia, phonophobia, motion sensitivity and throbbing pain quality were each present in approximately half of the patients with NDPH, and unilateral pain location was present in 27% (95% CI 15–39%) (see Table 4 and online Supplementary Figures 6–13).
Previous case series describing phenotype of NDPH.

Dashes used to indicate data not available.
Only studies including at least 20 patients which reported the proportion of patients who experienced individual symptoms are included.
ICHD-3, International Classification of Headache Disorders 3rd Edition; M-ICHD-2, Modified ICHD-2 criteria including patients with migraine features.
Forest plots of meta-analyses used to calculate pooled estimates of proportions are shown in the online supplementary material.
Depending on the presence or absence of migrainous symptoms, NDPH is sometimes sub-classified as a chronic migraine variant (NDPH-CM), or tension-type variant (NDPH-CTTH). An estimated 67% (95% CI 57–77) have a CM phenotype and 33% (95% CI 23–43) have a CTTH phenotype (see online Supplementary Figures 17 and 18), although this estimate is limited by the fact that the included studies did not all use the same diagnostic criteria.
In some patients (between 3.6% and 14.8% in the largest published series) NDPH begins following a thunderclap headache (9,10).
An estimated 78% (95%CI 67–89) of children/adolescents, and 49% (95%CI 32–67) of adults with NDPH had an episodic headache disorder prior to the onset of NDPH (see online Supplementary Figure 14). An estimated 40% (95% CI 29–52%) of adults with NDPH have a family history of headache (see online Supplementary Figure 15) suggesting patients who develop NDPH may have an inherited susceptibility to headache disorders.
Given its overlap in symptoms with CM and CTTH, whether primary NDPH deserves a diagnostic category of its own is debated. A recent article has proposed that primary NDPH should not be a separate diagnostic category, but it did not include a comparison group of patients with CM and/or CTTH (9). A paediatric study has compared children with NDPH to those with CM and found that the phenotype was similar, other than a lower prevalence of photophobia in the NDPH group (8). An adult study has compared those with NDPH-CM to those with CM, and found that the NDPH-CM group were less likely to have a family history of headache, had fewer associated migraine symptoms, less osmophobia, nausea and vomiting, and shorter duration of premonitory and postdromal symptoms (11).
Comorbidities
Medication overuse occurs in NDPH in an estimated 19% (95% CI 4-33) of children/adolescents and 31% (95% CI 20-42) of adults (see online Supplementary Figure 16). However, it appears to be less common in NDPH than CM – 22% vs. 34% in a childhood comparison study and 33% vs. 51% in an adult comparison study (8,11).
Depression and anxiety, assessed either by patient self-report or validated questionnaires, are common in NDPH. One study of 55 patients with NDPH found that 93% had high Generalized Anxiety Disorder Scale–7 (GAD-7) scores, and 89% had high Patient Health Questionnaire-9 (PHQ-9) depression scores; and both were higher in NDPH than patients with chronic lower back pain who had a similar pain severity (25). Another study comparing 92 patients with NDPH to 92 patients with migraine and tension-type headache found that anxiety and depression were more common in NDPH than migraine. Sleep disturbance was also common in NDPH and was correlated with depression (26).
Anecdotally, NDPH appears to be associated with joint hypermobility syndromes. In a small exploratory study of 12 patients with primary NDPH assessed by a physical therapist, 11 were found to have cervical joint hypermobility, and 10 were found to have widespread peripheral joint hypermobility using the Beighton score (27).
Biomarkers
Immunological markers
A small study measuring tumour necrosis factor alpha (TNFα) in the serum and cerebrospinal fluid (CSF) found that CSF TNFα levels were elevated in 19/20 patients with NDPH, but they were also elevated in 16/16 with CM, and 2/2 patients with post-traumatic headache (28).
Neuroimaging
Patients with NDPH typically have magnetic resonance imaging (MRI) of the brain performed to exclude a secondary cause. In NDPH, no macroscopic brain changes are seen, in keeping with it being a primary headache disorder. In a study of clinically performed MRI in 97 NDPH cases, 13% had white matter lesions on MRI, which only occurred in patients with vascular risk factors (29).
Several recent MRI studies have sought to discover structural or functional brain signatures of NDPH. A study using voxel-based and surface-based morphometry in 23 adults with NDPH did not find any grey matter differences in NDPH compared to non-headache controls (14). In contrast, a study of only 13 adolescents with NDPH found reduced cortical thickness in bilateral superior temporal gyri, left superior and middle frontal gyrus areas compared to non-headache controls (15). Resting-state functional MRI was also used in this study, and showed differences in functional connectivity between NDPH and controls (15).
A study using cerebral perfusion MRI imaging in 15 patients with NDPH found decreased cerebral blood flow measures in several regions of the right hemisphere in patients with NDPH compared to healthy controls and/or patients with chronic migraine, although the clinical significance of these measures is uncertain (13).
Pathophysiology
The underlying biology of primary NDPH is poorly understood. There are a variety of explanations proposed to explain the pathophysiology in all or a subset of patients with NDPH, driven by clinical findings.
Immunological
An infectious illness, most commonly a flu-like illness, is the most common precipitant for NDPH in most series (see Table 2). One study found evidence of recent herpes simplex virus in 42% and cytomegalovirus in 11% (30). NDPH may also be associated with higher than expected rates of immune-mediated illnesses (31). Vanast, who originally described NDPH and found high rates of EBV positivity in his patients, proposed an immunological basis of the condition via a viral-induced immune response (32,33). This hypothesis may be supported by the observation of high rates of CSF TNFα, although this finding was not specific to NDPH and may be a non-specific reaction to chronic pain or another confounder (28).
The suspected immune basis of NDPH has led some clinicians to treat patients with recent-onset post-infectious headache with corticosteroids, with a good effect in a small series of patients (34). In another small series, patients with post-infectious NDPH with high IgG viral titres were treated with antiviral medication, with an improvement in five out of six patients (35).
Psychological
Stressful life events are another common precipitant of NDPH. The combination of the treatment refractory nature, association with depression and anxiety, and onset after a stressful event in some patients could suggest that NDPH is similar to other psychogenic or functional neurological disorders, where the headache is one manifestation of a vulnerability to central sensitivity and altered interoception (36,37).
This may be supported by the observation of anxiety and pain catastrophisation being more common in NDPH than chronic back pain, and “somatic symptoms” being more common in NDPH than CM and CTTH (25,37). However, there is subjectivity to the assessment of somatic symptoms and this study did not state whether the assessment was performed blinded to the diagnosis of the patient.
A case series has described nine patients who were diagnosed with both NDPH and panic disorder. All had no prior history onset of headache, and the panic attacks began within the same week as NDPH. Most had a good response to a combination of topiramate and selective serotonin-reuptake inhibitors (38).
Cervicogenic
Cervical hypermobility is proposed to be a predisposing factor to the development of NDPH possibly due to upper cervical spine facet joint irritation (35). However, the only study which assessed this included a small number of cases and did not have a control group (27). Chronic pain of many forms, including migraine, is common in those with hypermobility (39,40), and therefore an association may not be specific to NDPH. The mechanism of headache and other neurological symptoms in joint hypermobility disorders is poorly understood, likely has multiple causes, and could also be explained by immunological abnormalities or anxiety disorders in hypermobile patients (41).
If cervical hypermobility does play a strong role in the development of NDPH then physical therapy targeted at neck muscle strengthening may be expected to improve headache.
Nutcracker physiology
A subset of patients with NDPH where it was triggered by a single Valsalva event and associated with subtle features of raised intracranial pressure has been described (42). Cases have since been published suggesting that some of these patients may have vascular compression of the left renal vein (termed Nutcracker syndrome) and subsequent spinal epidural venous congestion, which may be amenable to treatment, for example with lumbar vein embolisation (43–45).
Treatment
There are a growing number of effective treatments for CM, and to a lesser extent CTTH, which have been proven in randomised placebo-controlled trials. There is very limited evidence on the treatment of NDPH, which is limited to case reports, small open-label case series, and expert opinion. In headache trials there is commonly a placebo group response of around 30% meaning it is plausible that any described responses to treatment in primary NDPH are not due to a true treatment effect. Prospective studies, particularly randomised blinded placebo-controlled trials are lacking, but are limited by the rarity of the condition. Currently, expert opinion generally recommends treating as per the headache phenotype i.e., CM if symptoms of migraine are present and CTTH if they are not (4,46). However, it is recognised that patients with NDPH often do not respond to these treatments and many headache experts consider primary NDPH to be the most treatment refractory primary headache disorder (3–5).
Non-pharmacological treatments
No studies were identified which assessed the efficacy of non-pharmacological interventions in NDPH, and where outcome data was reported separately for patients with NDPH to other headache diagnoses.
Acute treatments
Given the continuous nature of the headache in NDPH, acute treatments are not used in NDPH to abort attacks but to reduce pain severity during exacerbations. Triptans have been reported to improve pain severity in 11/34 (32%) of patients, and are possibly more effective in NDPH-CM than NDPH-CTTH (47).
Preventive medications
Although they are often used in clinical practice, few studies report the proportion of patients who respond to migraine preventive medications.
In a retrospective case series of 18 NDPH patients, of whom 16 had tried amitriptyline and seven had tried sodium valproate, none had a beneficial response to either (30). In a sequential treatment regime of muscle relaxants, followed by tricyclic antidepressants, then selective serotonin reuptake inhibitors and finally antiepileptic drugs, only 30% of patients had at least a moderate response to one of the treatments (48).
In a recent series of 162 patients with NDPH, there was a response to amitriptyline in 17/89 (19%), dosulepin in 1/3 (33%), flunarizine in 2/20 (10%), gabapentin in 7/37 (19%), methysergide in 2/7 (28%), propranolol in 12/53 (23%), pizotifen in 2/26 (8%), topiramate in 18/76 (24%), and sodium valproate in 2/35 (6%) (9).
Injectable and neuromodulatory treatments
Greater occipital nerve (GON) block injections have been reported as effective in 33–63% of patients with NDPH, similar to efficacy rates in CM (49–51). In one series, cranial nerve blocks targeted to the pain were reported to be effective in 61% of patients with NDPH (47), but in another series of patients treated with multiple cranial nerve block injections, only 10% of patients with NDPH responded, compared to 49% of those with CM (52).
In a series of 11 patients treated with intravenous dihydroergotamine only two (18%) patients with NDPH had a mild benefit, compared to a beneficial effect in 84/113 (74%) patients with migraine (53). In another study of 51 patients with NDPH, intravenous dihydroergotamine led to at least a moderate improvement in 19 (37%) of cases, compared to 80/130 (62%) of patients with migraine (54).
In a series of five patients with NDPH treated with intravenous sodium valproate no patients had an improvement in headache days, and only one patient had a marginal improvement in headache severity (55).
A case series of 16 patients with NDPH treated with onabotulinumtoxinA injections reported that eight (50%) had an improvement in headache frequency after six months (56). In another study of onabotulinumtoxinA, which included nine patients with NDPH, two patients had an improvement of Headache Impact Test-6 score (57). Unfortunately, a previous open-label clinical trial of onabotulinumtoxinA for NDPH was terminated due to difficulty with enrolment (58).
In a case series of nine patients with NDPH treated with invasive occipital nerve stimulation only one patient (11.1%) had a positive response (59). This compares to a 45.3% response rate in CM in the same unit, suggesting than even invasive surgical treatments may be less effective in NDPH than CM (60).
Prognosis
Prospective natural history studies of NDPH have not been conducted, but many experts consider NDPH to usually be persistent and highly resistant to treatment (3,4,48). Other authors have suggested that there are subforms of NDPH, with a group of patients who have a self-limiting form and others who have a long-lasting treatment-refractory form (47). In the largest previous series, 93% of patients were classed as having the persistent refractory form (10). The disparity between these findings and the original description by Vanast of NDPH being a self-limiting headache may be partly due to referral bias. The groups that report that NDPH is refractory to treatment are generally tertiary referral centres where patients with self-limiting NDPH are unlikely to be referred.
Studies that have assessed prognosis of NDPH (either treated or untreated) are shown in Table 5.
Prognosis of NDPH.
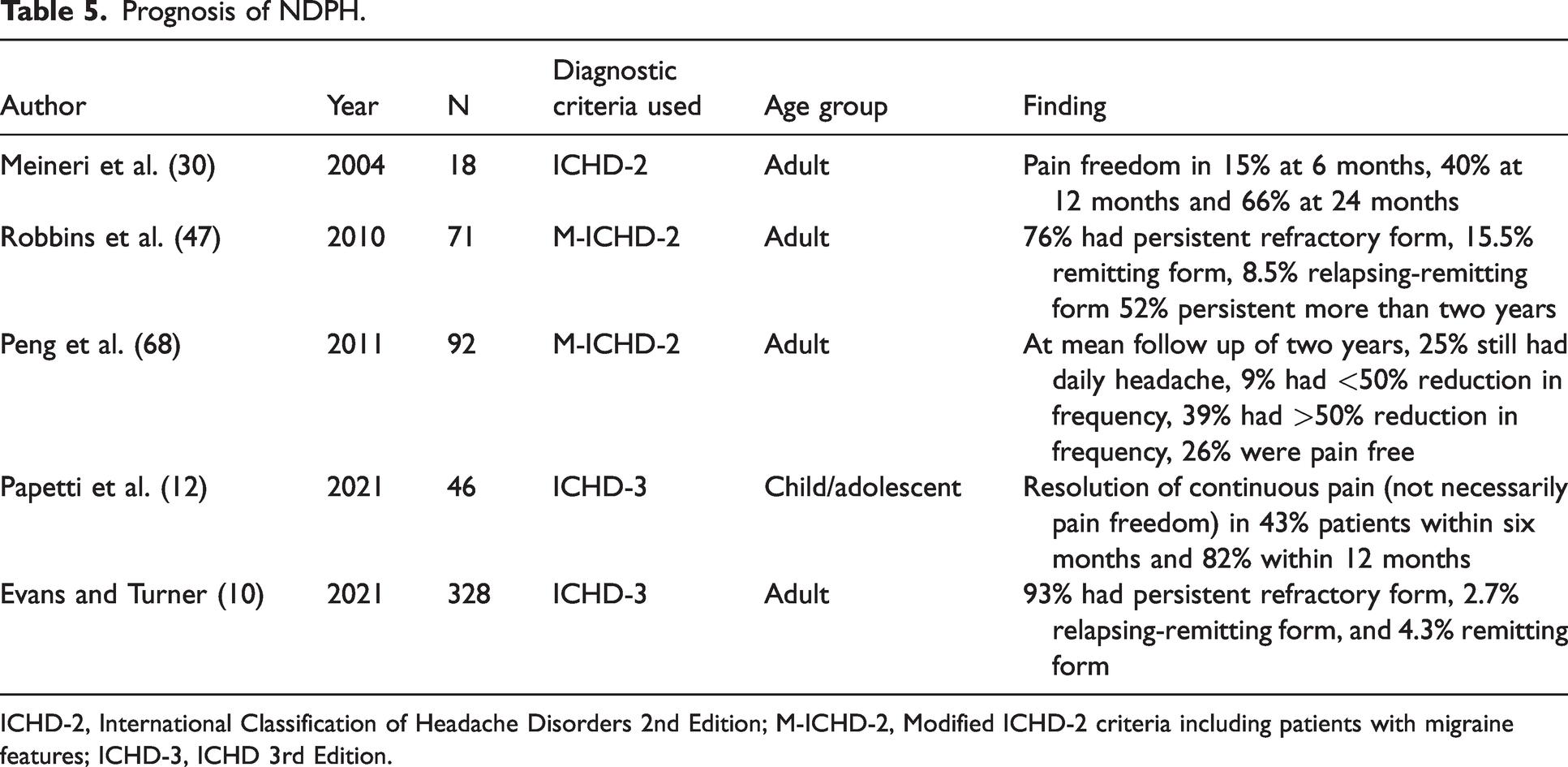
ICHD-2, International Classification of Headache Disorders 2nd Edition; M-ICHD-2, Modified ICHD-2 criteria including patients with migraine features; ICHD-3, ICHD 3rd Edition.
Discussion
While the clinical syndrome of NDPH is easy to recognise and its phenotype has been well described, its pathophysiology and optimal treatment is poorly understood.
We found NDPH to be overrepresented in children and adolescents compared to adults, as a proportion of chronic daily headache. This fact has been recognised by previous narrative reviews, but remains unexplained. If the inflammatory pathophysiological hypothesis is correct then it could relate to increased frequency of viral infections or less developed immune system in children compared to adults.
We have found that in approximately two thirds of cases, NDPH has the phenotype of CM, with most of the remaining having a CTTH phenotype. It is currently unknown whether NDPH deserves a dedicated diagnostic category, however the similarity in phenotype to CM or CTTH does not necessarily mean similarity in pathophysiology. Several studies comparing the phenotype, comorbidities, or treatment response of NDPH to CM and/or CTTH have identified differences between NDPH and CM and/or CTTH. Although most migrainous symptoms are common in NDPH patients, pain is typically unilateral in migraine whereas we estimated NDPH to be unilateral in only 27% of cases. NDPH appears to be less vulnerable to medication overuse than CM, which may be because acute treatments are less effective in NDPH, whereas in CM these treatments often will have been helpful in the past while experiencing episodic migraine (EM). Medication overuse is also a common cause of transformation from EM to CM, whereas the onset of NDPH is unrelated to medication use. NDPH also appears to respond less well to injectable and neuromodulatory treatments than CM. These differences in phenotype and treatment response suggest that NDPH is a distinct syndrome from CM and CTTH.
High-quality evidence regarding NDPH is currently lacking, and the syntheses presented in this review are limited by the heterogeneity of included studies. There are several potential explanations for the heterogeneity. Firstly, NDPH may not be a single disease entity. Several authors have proposed that NDPH is a heterogenous group of conditions with different pathophysiology (61,62). Secondly, there may be cultural or biological reasons why the presentation of NDPH differs by country or region. Thirdly, the changing diagnostic criteria for NDPH mean that the same patient may be included or excluded from the diagnosis depending on which criteria were used in the study.
We limited the diagnostic criteria for inclusion to ICHD-2 and subsequent editions in an attempt to minimise this, but this meant we were not able to include any studies published prior to 2004. Criteria had been proposed prior to this by Silberstein et al. (63) but these were not sufficiently similar to current criteria, as the headache did not have to be daily or continuous and the minimum duration was one month rather than three.
Another limitation of our search strategy is that it is probable that other published studies have included patients with NDPH but have not explicitly described the diagnosis as such. For example, a study has reported persistent headache following psychological stress in the form of a terror attack (64), and studies have also reported persistent headache after Covid-19 (65), but these studies were unable to be included as it was not possible to identify how many of the patients included would meet criteria for NDPH.
Further studies of NDPH are required and should include a control population with CM and/or CTTH. Studies should prioritise investigation of its underlying pathophysiology with biomarkers such as inflammatory mediators or calcitonin gene-related peptide (CGRP), and/or neuroimaging studies with larger sample sizes. Due to its rarity, it is unlikely that randomised controlled trials of treatment in NDPH will be performed, but future research should study treatments which are proven in CM such as onabotulinumtoxinA and CGRP monoclonal antibodies to determine whether NDPH responds and if the response in NDPH differs to CM.
Key findings
NDPH accounts for approximately 18% cases of chronic daily headache in children and 4% in adults. The phenotype of NDPH in two thirds of cases resembles chronic migraine. The pathophysiology of NDPH is poorly understood, but small studies suggest associations with autoimmunity, psychological factors, and joint hypermobility. Evidence for treatment of NDPH is limited to observational studies, but suggests it may respond less well to treatment than chronic migraine.
Supplemental Material
sj-pdf-1-cep-10.1177_03331024231168089 - Supplemental material for New daily persistent headache: A systematic review and meta-analysis
Supplemental material, sj-pdf-1-cep-10.1177_03331024231168089 for New daily persistent headache: A systematic review and meta-analysis by Sanjay Cheema, Dwij Mehta, Jason Charles Ray, Elspeth J Hutton and Manjit Singh Matharu in Cephalalgia
Supplemental Material
sj-pdf-2-cep-10.1177_03331024231168089 - Supplemental material for New daily persistent headache: A systematic review and meta-analysis
Supplemental material, sj-pdf-2-cep-10.1177_03331024231168089 for New daily persistent headache: A systematic review and meta-analysis by Sanjay Cheema, Dwij Mehta, Jason Charles Ray, Elspeth J Hutton and Manjit Singh Matharu in Cephalalgia
Footnotes
Data availability
The extracted data used for the analyses is available upon reasonable request to the corresponding author.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: SC and DM have no competing interests.
JCR has served on advisory boards for Viatris, Lilly and Pfizer and has received compensation for educational presentations supported by Allergan, Novartis and Viatris.
EJH has served on advisory boards for Sanofi-Genzyme, Novartis, Teva, Eli Lilly, Allergan and Lundbeck, been involved in clinical trials sponsored by Novartis,Teva, Xalud, Cerecin, AEON Biopharma and Abbvie and has received payment for educational presentations from Allergan, Teva, Eli Lilly and Novartis.
MSM is chair of the medical advisory board of the CSF Leak Association; has served on advisory boards for Allergan, Autonomic Technologies Inc, Eli Lilly, Novartis, Pfizer, Salvia and TEVA; has received payment for educational presentations from Allergan, electroCore, Eli Lilly, Novartis and TEVA; has received grants from Abbott, Medtronic and electroCore; and has a patent on system and method for diagnosing and treating headaches (WO2018051103A1, issued).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.