
Abstract
Background Accumulating evidence suggests various specific triggers may lead to new daily persistent headache (NDPH)-like presentations, suggesting that new daily persistent headache is a heterogenous syndrome, and challenging the concept that new daily persistent headache is a primary headache disorder.
Method We searched the PubMed database up to August 2022 for keywords including persistent daily headache with both primary and secondary etiologies. We summarized the literature and provided a narrative review of the clinical presentation, diagnostic work-ups, possible pathophysiology, treatment response, and clinical outcomes.
Results and conclusion New daily persistent headache is a controversial but clinically important topic. New daily persistent headache is likely not a single entity but a syndrome with different etiologies. The issue with past studies of new daily persistent headache is that patients with different etiologies/subtypes were pooled together. Different studies may investigate distinct subsets of patients, which renders the inter-study comparison, both positive and negative results, difficult. The identification (and removal) of a specific trigger might provide the opportunity for clinical improvement in certain patients, even when the disease has lasted for months or years. Nonetheless, if there is a specific trigger, it remains unknown or unidentified for a great proportion of the patients. We need to continue to study this unique headache population to better understand underlying pathogenesis and, most importantly, to establish effective treatment strategies that hopefully resolve the continuous cycle of pain.
History and evolution of the disease entity
New Daily Persistent Headache (NDPH) was first described by Dr Walter Vanast, in 1986, as a benign form of persistent headache after the onset (1). The diagnostic entity was not yet included in the first version of the International Classification of Headache Disorders (ICHD-1) in 1988 (2) but was first recognized in the “Silberstein-Lipton” (S-L) criteria for chronic daily headache (CDH) published in 1994 (3). The lack of a common classification system has led to a miscellany of diverse patients with various triggers and etiologies in early NDPH series, including those with secondary, usually infectious etiologies (4,5).
The clinical description of NDPH has also evolved over the years. Apart from the initial report by Vanast (1), NDPH, according to the S-L criteria, is not necessarily daily or persistent, while “daily” was defined as ≥15 days/month and “persistent” was defined as ≥4 hours/day (3). The pathognomonic features of daily and persistent were reinstated in the second version of ICHD (ICHD-2), published in 2004 (6). Additionally, for the first time, the clinical features were defined as exclusively tension-type headache (TTH)-like only, and migrainous features were not allowed, presumably in order to delineate NDPH from the most common type of CDH – chronic migraine. Notably, ICHD-2 clearly categorized NDPH under primary headache disorders, headache attributed to secondary etiologies must be excluded and can only be diagnosed as secondary headaches regardless of the clinical presentations (6).
After the introduction of ICHD-2, several large NDPH cohort studies demonstrated that headache features, being TTH-like or migrainous, do not differ greatly in the disease-associated disability, quality of life, treatment responses, or prognosis (7,8). Therefore, headache features are no longer restricted in the 3rd version of ICHD (ICHD-3) published in 2018 (9). Moreover, in this revision, the onset of NDPH was defined as pain becoming continuous and unremitting within 24 hours since onset, contrasting 72 hours in ICHD-2, reciprocating the fact that most patients can clearly pinpoint the date of onset (6,9). Secondary headaches must also be ruled out, like in the ICHD-2, reflecting the concept that NDPH is a primary headache disorder. Whether it is reasonable to categorize NDPH as a primary headache will be further discussed in this review.
Epidemiology
Population-based studies of NDPH are rare. Castillo et al. (10) identified two cases of NDPH using S-L criteria among 1883 subjects from the general population, corresponding to a one-year prevalence of 0.1%. Grande et al. (11) reported a one-year prevalence of NDPH of 0.03% in 30,000 persons aged 30–44 years. Notably, this study used the most restrictive ICHD-2 criteria – only patients with TTH features were allowed. The prevalence is expected to be two to three times higher when including those with migrainous features. Both studies suggest that the prevalence of NDPH in the general population is low.
NDPH is a subtype of CDH. CDH affects 4% of the general population (10,12), but CDH and its various subtypes present substantial management challenges in headache clinics. In tertiary headache centers (13), NDPH accounts for up to 35% of CDH in pediatric population (14,15) and 2.5–10.8% in the adult population (8,16). Some suspect, therefore, that the prevalence of NDPH among all CDH may be higher in pediatric populations. For NDPH, sex predisposition in women may not be as prominent as that seen with migraine and might differ in various populations. In European and North-American studies, the F:M ratio ranged from 1.79–2.57 (7,17–20). In Asian studies, the F:M ratio is lower (0.75–1.35) and studies from India and Japan even showed a slight male predominance (8,21,22). NDPH affects all age groups, and the age of onset varies greatly among studies and may also differ based on sex and trigger (7,8,23)
Triggers of NDPH
Patients with NDPH (20% to 88%) may recall specific triggers before the onset of headache, but the inter-study variance is high (7,17,18,20–22,24). Common triggers include infectious episodes or stressful life events (7,8). Besides, the onset of pediatric NDPH is concentrated in specific months or seasons, supporting a possible link between infectious episodes and the onset of NDPH (20,25); however, school related stressors may also be connected. Some triggers may provide hints to disease mechanisms and are worth further exploration; however, triggers, in general, are easily misattributed and may be affected by recall bias.
The earliest record of NDPH-like headache after an infectious episode can be traced back to 1890 after the Russian/Asiatic flu. Headache was a complaint in 75–83% of the patients during the acute stage, and some of the patients (the exact number unknown) developed a long time subsequent headache that mimics NDPH (26). Infectious episodes as triggers, such as Epstein-Barr virus or Salmonella/E. Coli infection has been mentioned in the early NDPH series before the introduction of the S-L Criteria when both primary and secondary causes were not differentiated (4,5). The infectious triggers are not restricted to specific pathogens. Bordini and Valença (27) reported three possible cases of NDPH in 450 patients with Dengue fever. More recently, approximately half of the patients infected with COVID-19 developed headaches during the acute stage (28). Some patients developed persistent headaches after the resolution of the acute episodes, (29,30), among which some fulfilled the ICHD-3 diagnostic criteria of NDPH (29). In most reported cases with an infectious episode as a trigger of NDPH, the infection is usually systemic and not localized. Some patients may also fulfill the diagnostic criteria of §9.2 – Headache attributed to systemic infection according to the ICHD-3 when the headache started during the acute stage of the infection (9). The demarcation of primary vs secondary headaches in the case of an infectious trigger sometimes can be blurred.
The second most reported trigger is stressful life events, up to 26% in some series (8). However, stress is even more often reported as a trigger for migraine attacks (31) and is highly unspecific and easily falsely attributed. On the contrary, some NDPH triggers are not common but highly specific and remain rarely reported in other headache disorders. These triggers suggest a possible link to the mechanism that triggers persistent headache. In a large NDPH-series (n = 97), Rozen (18) reported nine patients with NDPH-like headaches after surgical interventions that required intubation. Cervical spine joint hypermobility was reported in 11 of 12 NDPH patients in another earlier report (32). Both combined suggest a possible cervicogenic etiology in a subset of NDPH patients. Valsalva event as a trigger has been reported in another seven NDPH patients. None of them had papilledema, and four had a normal weight. Therefore, idiopathic intracranial hypertension is less likely, but idiopathic intracranial hypertension without papilledema can only be excluded with a proper cerebrospinal fluid (CSF) pressure monitor, while a single spinal tap may fall in the normal range (<25 cm CSF) in 40% of these patients (33). Typical treatment options for intracranial hypertension, such as acetazolamide, reduced the headache frequency by more than 90% in five of seven patients (34), suggesting an abnormal distribution or equilibrium of CSF may also link to typical NDPH phenotypes. All the distinct triggers, each accounting for a small proportion of NDPH patients, suggest that NDPH is probably a syndrome with various mechanisms, instead of a homogenous disease (see below).
Clinical characteristics
The most typical presentation of NDPH is the acute onset headache on a specific day which becomes persistent within 24 hours. Most NDPH patients can recall the day when their headaches started (7,17,24). Hence, in the latest version of the ICHD, clearly remembering the onset is listed as a diagnostic criterion (9). Headache features are not restricted, and migrainous features may be more common than TTH features (7,8,22,25,35), reflecting the evolution of the diagnostic criteria. Notably, despite the prominent migrainous features, most patients presented with bilateral headache that is commonly pressing/tightening (7,21,22,24). Previous headache disorders may exist in up to 29% of the patients with NDPH (7,8,17,22,24), but a chronification of preexisting headache disorders or de novo NDPH must be carefully differentiated based on the headache features changes, if any, and pre-NDPH headache frequency. Even though the headache features are not restricted in NDPH, patients with migrainous features, compared to those with TTH features, may have higher psychiatric co-morbidities, disability, and possibly worse clinical outcomes (8,22).
Traditionally, NDPH has been considered refractory to most treatment options. Robbins et al. identified a subset of patients (24%) who may have remitting/relapsing disease course, instead of persisting headaches in long-term follow-up (7). Two studies suggested early (within six or 12 months after disease onset, respectively) treatment with migraine prophylactic treatment may be associated with better clinical outcome (8,25), and the headache may still remit in more than 50% of the patients (25). Therefore, those with early treatment may be more likely to have a relapsing/remitting disease course compared to those with years of persistent headache. Whether the disease course may be modified with early treatment can only be answered in placebo-controlled studies with long-term follow-up. Such studies are difficult to conduct, especially considering the low prevalence of NDPH.
Psychiatric comorbidities are prevalent in patients with CDH and are associated with decreased quality of life or worse treatment response (36). Comorbid depression affects approximately half of the NDPH patients, and patients with prominent migrainous features were more commonly affected (7,8). A recent study from India used established psychiatric batteries to evaluate the psychiatric comorbidities in patients with NDPH, those with chronic back pain, and healthy controls. In this study, up to 85.5% of NDPH patients had psychiatric comorbidities, and the proportion is significantly higher than those with low back pain or healthy controls (37). Again, the presence of migrainous features was associated with an even higher depression score and pain catastrophizing behavior (37). Disease-associated disability and disease burden remain high in patients with NDPH (8) and not distinguishable from those with chronic migraine (38).
Diagnostic work-up and the 3Ts model of NDPH
All patients who present with a daily headache from onset require neuroimaging. At baseline, a brain MRI with and without gadolinium and an MR venogram are required. This will rule out the majority of secondary mimics of NDPH, including intracranial hypotension, mass lesion, sphenoid sinusitis, hydrocephalus, and cerebral vein thrombosis. If there is any question of arterial issues, such as a daily headache with stroke-like spells or thunderclap-like headache, arterial imaging of both the intracranial and extracranial circulations is needed. In most instances, however, these imaging studies will be normal. Thus, the etiology of the patient’s daily headache from onset remains a mystery. One of the authors (TDR) has established the 3Ts model to help define NDPH subtypes, which then can lead to more distinct treatment options (39). The full model is presented elsewhere, but in essence, looks at: i) Triggering events with specific questions; ii) the response of the headache to the Trendelenburg position; iii) defining the temporal profile of the original headache (Thunderclap or non-thunderclap).
Secondary headaches that mimic NDPH
Certain secondary headaches may present with typical NDPH features but cannot be diagnosed as NDPH following the current ICHD-3 diagnostic system. Possible secondary causes that led to an NDPH-like headache involve different pathologies, both intracranial and extracranial (Table 1). Following are some reported examples:
Headache disorders that mimic new daily persistent headache.

CM, chronic migraine; CSF, cerebrospinal fluid; CTTH, chronic tension-type headache; NDPH, new daily persistent headache.
Cranial pathologies
Aguiar de Sousa et al. (40) reported a young female patient with a typical NDPH clinical presentation. Brain MRI revealed multiple white matter hyperintensities without gadolinium enhancement, involving the corpus callosum, juxtacortical and periventricular. A repeated MRI two years later revealed new gadolinium-enhanced lesions in the subcortical white matter, and multiple sclerosis was subsequently diagnosed. Treatment with interferon-beta-1a improved the headache intensity, but the headache remained persistent (40). There have been several reports of NDPH-like headaches with thunderclap headache onset (41–43). Brain MR angiography during the acute stage revealed typical features seen in those with reversible vasoconstriction syndrome (RCVS) – multifocal arterial vasoconstriction, and the patient responded well to nimodipine, the standard treatment for RCVS (41,43). These cases suggest a possible arterial origin of the daily persistent headache. Infection or inflammation in the cranial structure may also present with a typical NDPH headache. Lee et al. (44) reported two pediatric cases with sphenoid sinusitis with minimal nasal symptoms but typical NDPH presentations. Skull base metastasis may also mimic NDPH. In this patient, following radiosurgery, the intensity of pain improved greatly (10 to 2, 0–10 scale), but the headache remained daily and persistent (45).
Extracranial pathologies
Carotid and vertebral artery compression secondary to goiter may also present with typical NDPH symptoms, and the headache completely resolved after thyroidectomy (46). Low-pressure headache due to CSF-venous fistula may resemble typical NDPH presentations, and surgical ligation completely resolved the headache in this case (47). Even more rarely, two independent groups reported daily-persistent headaches secondary to nutcracker syndrome – aortomesenteric compression of the left renal vein (48,49). One patient had nearly complete resolution of headache symptoms after aortomesenteric decompression (48), and six out of eight patients had immediate pain resolution after CSF volume removal (49). Notably, none of these eight patients had elevated intracranial pressure at baseline. The authors suggest that renal vein compression may lead to retrograde flow through the lumbar vein, which subsequently perturbs the CSF pressure balance and causes headaches. (49). The miscellaneous mimics of NDPH suggest more than one mechanism may be involved in the generation of persistent headaches. Proper identification of potential mimics provides the opportunity for an accurate treatment and possibly headache resolution.
Pathogenesis
At present, there is no defined pathogenesis for NDPH. If we take the stance that NDPH is not a single entity, there cannot be a unified pathogenesis theory but multiple potential underlying causes. If, however, we group patients into specific subtypes, we may be able to define unique underlying pathogenesis for each subgroup. Patients within a distinct NDPH subgroup will probably have the same underlying etiology, but those between subgroups not. Some patients who fit into more than one subgroup may have mixed etiologies (18,39). For example, post-infectious NDPH patients who worsen in the Trendelenburg position may have both a headache caused by a pro-inflammatory response to a virus plus elevated CSF pressure possibly caused by the virus itself and/or the location they were infected (vacationing at a higher altitude) and/or from the inflammatory cascade to the infection. Alternatively, some triggers remain a universal experience to nearly all human beings, e.g., headaches associated with an acute infection. Another argument for the pathogenesis would be a failed off-switch to cease the headache (50). This hypothesis requires further exploration.
The author (T. Rozen) and colleagues have defined a unique subtype of NDPH caused by nutcracker physiology with secondary spinal lumbar vein dilation and subsequent spinal epidural venous congestion (49). This would be one of the first NDPH subtypes with a definable underlying etiology that can be specifically treated with the resolution of head pain. There have recently been published studies trying to define structural brain alterations which may be unique to the NDPH population. This is a substantial leap forward in studying this condition. So far in adults, no structural imaging changes have been noted; however, in a pediatric population with NDPH, there were unique alterations compared to age-matched controls, including a reduction in thickness in the left superior frontal gyrus, cortical thinning in the temporal and middle frontal gyrus, and altered functional connectivity between certain brain regions (51,52). The issue with these studies, however, is that they regard NDPH as a single homogenous entity which it is not; so, the study results have to be interpreted with some caution. It is like studying the functional imaging of headache patients and not teasing out who has migraine, cluster headache, TTH, etc. The results would be uninterpretable outside of denoting the functional imaging of head pain. It would be very instructive to repeat the anatomical and functional connectivity studies by NDPH subtypes. This could provide very useful information.
Treatment
NDPH has been considered refractory to treatment, and up to date, there has been no well-designed or controlled study evaluating the clinical response of specific medication in NDPH. Treatment strategy usually follows the established protocols in other CDHs. For example, patients with prominent migrainous features are treated with chronic migraine prophylactic treatment. The standard treatment regimen of CDH has been reviewed elsewhere (53). Notably, medication overuse headache (MOH), which develops after NDPH, is not a rare complication (35). A standard treatment regimen against MOH should be considered in these patients. Nonetheless, patients with NDPH were less likely to develop MOH than those with other CDH (54). The exact reason remains unknown, but the initial inefficacy of acute medication and the type of acute medication used may contribute to the relatively lower prevalence synergically. Besides the common treatment for CDHs, some specific treatment regimens for NDPH have been investigated in small-scaled open-label studies, as discussed below.
Nerve Block/Stimulation
Great occipital nerve block improved headaches in 33% of pediatric NDPH patients in a retrospective study (55). Nerve blocks remain a favorable option in treating pediatric patients because of the tolerable side effect profiles, even though the efficacy has not been well established (56). The long-term outcomes of occipital nerve stimulation have been recently investigated. After eight years of follow-up, only 11% of the patients still had favorable responses (57). The evidence to support the general use of nerve block/stimulation in the treatment of NDPH is low, even though some patients might still benefit from the treatment.
Anti-Tumor Necrosis Factor-alpha (TNF-α) treatment
Exclusive intrathecal elevation of TNF-α levels has been reported in patients with NDPH and chronic migraine, suggestive of a role of CNS inflammation in CDH, including NDPH (58). Doxycycline reduces the expression of TNF-α (59), and in an open-label trial, four out of four NDPH patients with high TNF-α levels in the CSF reported ≥50% improvement of headache after three months of doxycycline treatment, among which two patients reported complete relief of pain (60). Venlafaxine, a serotonin-norepinephrine reuptake inhibitor, may inhibit the upregulation of TNF-α (61). In one case report, an NDPH patient who had not responded to more than 20 different medical treatments, had a remarkable reduction in headache intensity (from 9 to 3, 0–10 scale) after three months of treatment. The headache recurred after discontinuation of venlafaxine but remitted again after treatment resumed (62).
Intravenous ketamine
In a retrospective study, 14 patients with refractory NDPH were treated with a subanesthetic dosage of ketamine, and eight of them (57.1%) had a reduction in headache intensity (≥1.5, 0–10 scale) (63). Ketamine is an N-methyl-D-aspartic acid (NMDA) receptor antagonist, and the role of NMDA in NDPH may be worth further investigation.
OnabotulinumtoxinA (BTX)
In a meeting abstract, Ali et al. treated 12 patients with NDPH with BTX following the PREEMPT protocol used in the treatment of chronic migraine (64,65). Six out of the 12 patients (50%) had a reduction in headache frequency after two sessions (six months) of BTX therapy, and the response rate increased to 63.6% after four sessions of BTX therapy (65). Other case reports of the clinical efficacy of BTX in the treatment of NDPH exist (66,67). The efficacy of BTX in NDPH has not been examined in controlled studies.
Calcitonin gene-related peptide (CGRP) antibodies
Antibodies against CGRP or its receptor are emerging treatment options in migraine (68). Their roles in NDPH remain unknown. A recent cohort study reported some benefits of CGRP antibodies in 112 adolescent patients with refractory CDH, two-thirds of whom had continuous headaches. Among them, 12 were diagnosed with NDPH, but no breakdown data on NDPH were provided (69). A clinical trial has been conducted but was early terminated due to COVID-19 (ClinicalTrials.gov Identifier: NCT04260087). No results have been published yet.
3Ts model-specific treatment
A more effective way to treat NDPH is by defining subtypes and then utilizing distinct treatments for each subtype based on the theorized underlying pathogenesis. These specific treatment options are summarized in Table 2. There is evidence from small case series that the treatment effect is more substantial when this is done.
New daily persistent headache with specific triggers and their corresponding treatment options.
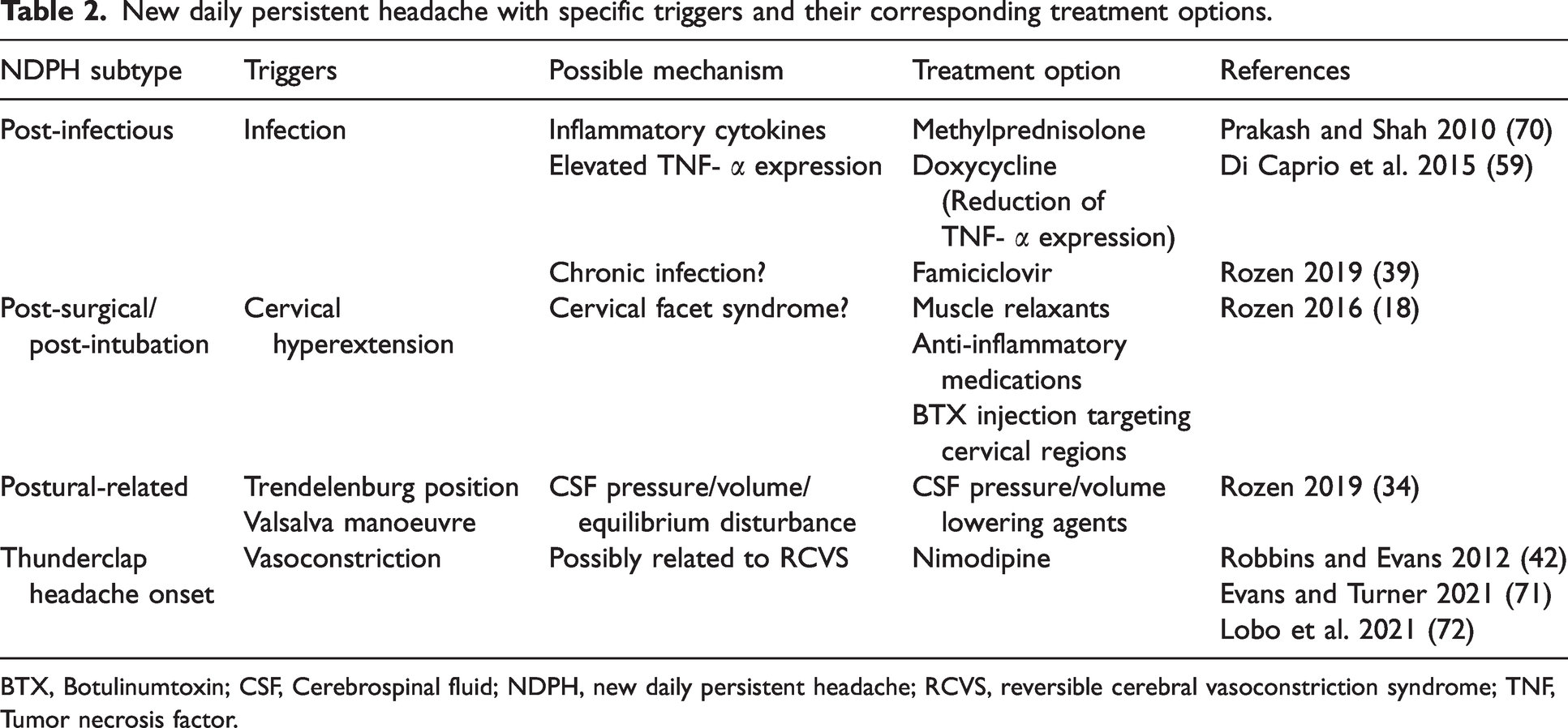
BTX, Botulinumtoxin; CSF, Cerebrospinal fluid; NDPH, new daily persistent headache; RCVS, reversible cerebral vasoconstriction syndrome; TNF, Tumor necrosis factor.
Post-Infectious NDPH
b. Post-surgical/post-procedure NDPH
This is typically an older subgroup of NDPH sufferers. Their headache is speculated to be the result of an exacerbation of an underlying upper cervical facet syndrome induced by the cervical hyperextension occurring during intubation and the neck positioning during surgery. Treatments directed at the high cervical spine irritation including medications (muscle relaxants combined with anti-inflammatories), BTX injections, and pain anesthesia procedures have shown positive efficacy in this patient population (18).
c. Treatment based on the Trendelenburg worsening
An immediate worsening of headache in the Trendelenburg position suggests a state of elevated CSF pressure/volume. The authors have defined subgroups of NDPH with this presentation, and most appear to respond to CSF pressure/volume lowering medications including acetazolamide, spironolactone, and/or indomethacin sustained release (34).
d. Thunderclap onset
There are now 20 plus published cases for this NDPH subtype. It is probably a sub-form of RCVS. In those studies, with treatment data, nimodipine appears very effective. The dose is typically much lower than that utilized in post-subarachnoid hemorrhage vasospasm (42,71,72).
Controversy in the diagnosis and personal opinions from the authors
Is NDPH a primary headache disorder?
The authors suspect that a great proportion of true NDPH, defined as a daily persistent headache lasting for more than three months in a patient who has no personal or family history of headache, may be a secondary headache. In some instances, we can define the underlying secondary etiology; in others, it is yet undefined or unidentified. Something must have happened to that individual to turn on the switch from no headache to a daily persistent intractable headache that is unremitting for months to years. If a triggering event can be denoted, such as post-viral or post-surgical, the patient could be labeled with a distinct established secondary ICHD classification. Nonetheless, the proportion of NDPH patients with identifiable secondary triggers remains unknown. Both primary and secondary NDPH may coexist. In that circumstance, a new ICHD classification should be created for secondary NDPH with subtypes by triggering event, Trendelenburg response, thunderclap onset, and/or current unknown etiology. Clinically, secondary etiologies were sometimes defined and identified years later, and more importantly, the removal of the triggers or treatment options that target the triggers provides rapid clinical improvement (41).
Is NDPH just a quick chronification of migraine or tension-type headache?
In many instances, if we look at the headache phenotype of NDPH patients and disregard the temporal profile of onset, we can diagnose chronic migraine or TTH in the majority. The question arises: can migraine or TTH start daily from the onset, especially if that individual never experienced any prior headaches or had a very minimal personal and family history of headaches? The typical scenario for headache chronification is a slow and steady increase in headache frequency unless there is a secondary lesion (like a brain neoplasm). The judgment for a rapid chronification vs de novo onset depends on the patients’ interpretation of their daily headaches. If they feel it is their prior headache just chronified, most likely they are correct in that assumption, especially if testing for secondary conditions is negative. However, if they feel it is a new distinct entity or their first-ever headache, then in that instance, NDPH should be the diagnosis. The demographics and headache phenotype are somewhat different when comparing chronic migraine to NDPH with a migrainous phenotype (7,73), suggesting that both might be divergent conditions. Treatment responses provide additional clues. As we often see in NDPH, both with and without migraine features, the treatment response rate to typical migraine preventives is quite low, suggesting against this being just an offshoot of the primary headache syndrome.
Conclusion
NDPH is a controversial but clinically important topic. It sometimes is just a quick chronification of an already pre-existent primary headache disorder, rarely a manifestation of an underlying psychiatric disorder, and perhaps frequently secondary to something as the number of documented secondary etiologies of NDPH keeps increasing in the literature. The heterogeneity of NDPH renders interstudy comparison difficult and inconclusive when specific subgroups are not separately studied. What is important is that the patients who develop a daily headache out of the blue in many instances have a life-changing event. We need to continue to study this unique headache population to better understand underlying pathogenesis and, most importantly, to establish effective treatment strategies that hopefully resolve the continuous cycle of pain.
Clinical implications
NDPH is a syndrome that encompasses different etiologies/subtypes. The identification of a specific trigger provides the opportunity for specific treatment options. Accumulating evidence suggests that a least some patients have a secondary etiology, which challenges the current diagnosis of NDPH as a primary headache.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.