
Abstract
Background
Preschool age (i.e. children under six years of age) represents a red flag for requiring neuroimaging to exclude secondary potentially urgent intracranial conditions (PUIC) in patients with acute headache. We investigated the clinical characteristics of preschoolers with headache to identify the features associated with a greater risk of secondary “dangerous” headache.
Methods
We performed a multicenter exploratory retrospective study in Italy from January 2017 to December 2018. Preschoolers with new-onset non-traumatic headache admitted to emergency department were included and were subsequently divided into two groups: hospitalized and discharged. Among hospitalized patients, we investigated the characteristics linked to potentially urgent intracranial conditions.
Results
We included 1455 preschoolers with acute headache. Vomiting, ocular motility disorders, ataxia, presence of neurological symptoms and signs, torticollis and nocturnal awakening were significantly associated to hospitalization. Among the 95 hospitalized patients, 34 (2.3%) had potentially urgent intracranial conditions and more frequently they had neurological symptoms and signs, papilledema, ataxia, cranial nerves paralysis, nocturnal awakening and vomiting. Nevertheless, on multivariable logistic regression analysis, we found that only ataxia and vomiting were associated with potentially urgent intracranial conditions.
Conclusion
Our study identified clinical features that should be carefully evaluated in the emergency department in order to obtain a prompt diagnosis and treatment of potentially urgent intracranial conditions. The prevalence of potentially urgent intracranial conditions was low in the emergency department, which may suggest that age under six should not be considered an important risk factor for malignant causes as previously thought.
Keywords
Introduction
Headache is common in children with a variable incidence according to age (3–8% at three years of age, 19.5% at five years, and 37–51.5% at seven years) (1–3), representing one of the main neurological causes of admission in the pediatric Emergency Departments (ED) (4). Non-traumatic headache accounts for 0.6–2.6% of ED visits per year (5–15), with a hospitalization rate of 8–29% (16), showing a heterogeneous etiology, clinical presentation, age of onset and comorbidities. Aged under six years (i.e. preschool-age) makes diagnosis challenging and is generally considered a “red flag” that requires more in-depth investigations (such as neuroimaging) to exclude secondary life threatening (LT) conditions (16–21). The younger the child is, the more difficult the diagnosis is, considering the reduced ability to describe the characteristics of headache (i.e. intensity, quality, location, and associated symptoms). The main concern is headache due to LT or disabling conditions, such as brain tumors, meningitis, venous sinus thrombosis, subarachnoid hemorrhage and other diseases that require early and appropriate diagnosis and management. However, it is well known that the prevalence of benign secondary causes of headache is much higher (32.9–72.3%) compared to the “dangerous” secondary ones (1.3–15.3%) (16,17) and that children under six years of age may have primary headache (16,18–21). To our knowledge, there is only one study focusing on acute headache in preschool children evaluated in ED that showed a low diagnostic yield of computed tomography (CT) if no worrying history and a normal neurological examination were present, not justifying the risks associated with ionizing radiation exposure (10). Therefore, it is important to identify preschool children who should undergo brain CT in the emergency setting. The aim of this study was to investigate clinical characteristics of headache in preschool age in the emergency setting in order to find features associated with secondary “dangerous” headaches that should require brain CT (Table 1). We also evaluated the etiology of headache to estimate the prevalence of LT conditions.
Warning symptoms/signs (red flags) in children with headache.

Modified by 16,17,23,26,30.
Material and methods
This multicenter exploratory retrospective cohort study was carried out in the ED of 14 Italian pediatric hospitals throughout the national territory (southern, central and northern), from 1 January 2017 to 31 December 2018. Preschool-age patients with new-onset non-traumatic headache were included from both urban and rural areas. The Institutional Ethical Committee (IEC) of the Bambino Gesù Children’s Hospital approved the study protocol. At the time of admission, parents or legal guardians gave their informed consent to the use of anonymized and aggregated data for research purposes in all clinical centers involved in this study. No specific consent form was required for this study given its retrospective nature. Patients were selected from electronic databases using the keyword “headache” in the fields “history”, “clinical examination” and “diagnosis”. We excluded patients with chronic headache or already known pathology considering medical history. We obtained demographic data, clinical history, neurological examination, investigations performed and hospital admission. Comorbidities were psychiatric disorders, sleep disorders, atopic disorders and cardio-vascular diseases. Priority of consultation at ED was based on a four-color triage coding scale according to Italian Health System Guidelines (22) and was assigned by a trained triage nurse. For the purposes of this study, the triage codes were grouped into two classes: High/Intermediate priority for patients classified “Red code” (critical medical state) and “Yellow code” (serious state, risk of evolution into critical conditions); Low/Non urgent priority for patients classified “Green code” (fair state, stable vital signs) or “White code” (good state, non-urgent consultation). The etiology of headache was based on the diagnosis made at the end of the diagnostic work-up. LT intracranial conditions, such as neoplastic, cerebrovascular, inflammatory or infectious, intracranial hypertension and malformative central nervous system (CNS) lesions were named potentially urgent intracranial conditions (PUIC), pointing out that a diagnostic and treatment delay could increase morbidity or mortality.
Statistical analysis
Clinical and demographic features were described. A statistical analysis was performed using the software STATA/IC 14.2 version 2017. We tested the normality by Skewness/Kurtosis test. Data were reported as median values with an interquartile range (IQR), and direct comparisons were made with Mann-Whitney rank-sum tests. Percentages were used to describe categorical outcomes, and distributions of categorical data were compared with either a Pearson's χ2 test or a Fisher's exact test, as appropriate. No sample size calculations were done a priori.
Patients were divided in two subgroups, hospitalized and discharged, and were compared in the bivariate analysis, to identify symptoms and signs associated to admission. Logistic regression analysis model was performed to detect variables associated with a higher risk of hospitalization. Clinical features with statistically significant differences at bivariate analysis were selected as independent variables. Sex and age were included a priori to adjust the effect of each independent variable for the demographic characteristics of the cohort. Variables with extremely unbalanced distribution in the two groups (frequency 0% in one group) were excluded. Adjusted odds ratios (OR) and 95% confidence intervals (CI 95%) were used as measures of effect. Hospitalized patients were further divided in two subgroups – patients with and without PUIC- and were compared to detect predictive variables associated with a higher risk of PUIC. Subsequently, a logistic regression analysis model was performed. The statistical significance was set at p < 0.05.
Results
This study included 1455 patients referring to ED with acute headache. Eight hundred forty-six were males and the median age was 55 months (IQR 45–65). Demographic and clinical characteristics were reported in Table 2, with a comparison between discharged and hospitalized patients. Three hundred twenty-five patients (22.3%) had comorbidities and 375 (25.8%) reported a family history of headache. The median time from symptoms onset to ED admission was one day (IQR: 1–2) and 681 children (46.8%) took pain relief therapy before or during their stay in the ED. Five hundred and sixty-two (38.6%) children had acute headache associated with fever, 487 (33.5%) with vomiting and 128 (8.8%) patients showed at least one neurological symptom or sign, as papilledema, ocular motility disorders, nystagmus, ataxia and dizziness. One hundred and twenty-three (8.50%) children reported pain in the occipital region and many patients presented multiple associated symptoms. A high/intermediate priority code was given to 149 patients (10.2%) and low/non-urgent to 1360 (89.8%). Specialist consultations were requested for 323 children (22.2%), mainly neurological (196) and ophthalmological (193). Neuroimaging studies were performed in 187 patients (13.3%): 169 (11.6%) CT scan, 16 (1.1%) brain magnetic resonance imaging (MRI) and 2 (0.1%) both CT and MRI (Table 2).
Baseline characteristics, symptoms/signs and clinical management of children presenting headache in Emergency Department.
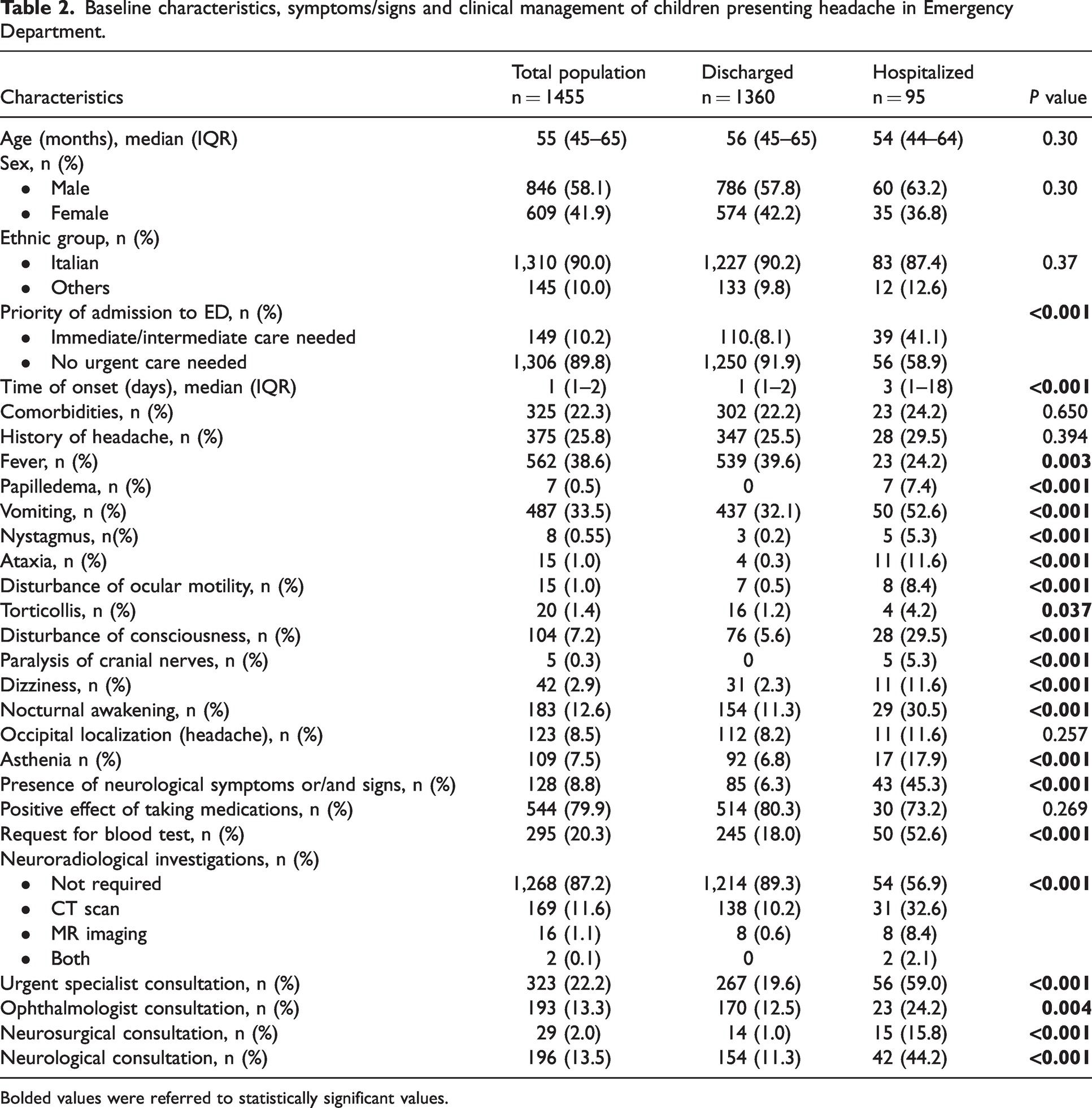
Bolded values were referred to statistically significant values.
Ninety-five patients (6.5%) were hospitalized and clinical characteristics were compared to those discharged. Sex, age, medication intake and comorbidities did not differ between the two groups, while the median time of symptoms onset was significantly higher in the hospitalized subgroup (p < 0.001) and fever was more often present in discharged patients (p = 0.003) (Table 2). No children with papilledema or cranial nerve palsy were discharged and hospitalized subgroup more frequently had vomiting, asthenia, nocturnal awakening (p < 0.001), torticollis (p = 0.037) and neurological symptoms and signs (Table 2). In particular, ataxia, dizziness, disturbances of consciousness, ocular motility disorders (i.e. strabismus, mydriasis, ptosis) and nystagmus showed an increased frequency in hospitalized patients (p < 0.001). Subsequently, a logistic regression analysis was performed and we found that ocular motility disorders (OR:5.76; 95%CI:1.36–24.36; p = 0.02), ataxia (OR:5.46; 95%CI:1.37–21.83; p = 0.02), presence of neurological symptoms and signs (OR: 5.22; 95%CI:1.76–15.44; p = 0.003), torticollis (OR: 5.98; 95%CI: 1.69–21.19; p = 0.006), nocturnal awakening (OR:2.37; 95%CI: 1.33–4.24; p = 0.003) and vomiting (OR:1.80; 95%CI: 1.08–3.01; p = 0.02), were independent variable associated to hospitalization (Table 3). Conversely, sex, age, fever, asthenia, dizziness and disturbance of consciousness were not linked to hospitalization (Table 3). The etiology of headache is reported in Table 4.
Multivariable logistic regression model exploring the factors associated with hospitalization in children presenting headache in Emergency Department.

Bolded values were referred to statistically significant values.
OR: Odds Ratio; Std. Err.: standard errors.
The distribution of the final diagnosis in children presenting headache in Emergency Department.

Among the hospitalized patients where PUIC were assessed, 34 (2.3%) had PUIC, such as brain tumors, cerebral vascular diseases, intracranial hypertension, CNS inflammatory disorders and malformation. The associated symptoms are reported in online Supplementary Tables S1–S6. Therefore, the 95 hospitalized children were divided into two groups – patients with PUIC and without PUIC – and were compared in order to identify features associated to potentially life-threatening disease. The presence of neurological symptoms and signs, papilledema, ataxia, cranial nerves paralysis, nocturnal awakening and vomiting were significantly associated with PUIC (Table 5). Nevertheless, on multivariable logistic regression analysis, we found that only ataxia and vomiting were associated with PUIC (OR: 19.03; 95% CI: 1.97–183.4; p = 0.01 and OR: 3.41; 95%CI: 1.02–11.36; p = 0.05, respectively) while the comorbidities were inverse associated with PUIC (OR: 0.19; 95% CI: 0.04–0.87; p = 0.01) (Table 6). Importantly, we have highlighted that all children with brain tumor had acute headache and at least one neurological sign or symptom and/or vomiting (online Supplementary Table S2). As regards headache etiology in ED, a comparison between our cohort and previous studies was performed and is reported in Table 7. In these studies, children aged 0–18 years were included and the frequency of secondary LT diseases was variable, from 1.3 to 15.3% (5–15). In most of our patients, the headache was due to a benign cause, while only 2.3% was related to LT diseases (1.0% brain tumors, 0.2% cerebral vascular disease, 0.6% CNS inflammatory disorders, 0.3% intracranial hypertension, and cerebral malformations in 0.1%) (Table 4). Patients with undefined headache were reevaluated and PUIC were excluded. Regarding the final diagnosis of cerebral vascular disease (online Supplementary Table S3), the associated symptoms were vomiting, dizziness, and drowsiness or nocturnal awakening; so, among these children, none presented headache as the only symptom. In the nine children with inflammatory disorders, associated symptoms were mainly characterized by fever, vomiting and/or neurological signs and symptoms (online Supplementary Table S4). Papilledema was present in three out of five children with intracranial hypertension and the remaining two showed other associated symptoms (online Supplementary Table S5).
Baseline and clinical characteristics in 95 hospitalized children presenting headache with potentially urgent intracranial conditions in comparison with not-potentially urgent intracranial conditions.

Bolded values were referred to statistically significant values.
Multivariable logistic regression model exploring the factors associated with potentially urgent, underlying conditions related to headache.

Bolded values were referred to statistically significant values.
OR: Odds Ratio; Std. Err.: standard errors.
Etiology of headache in Emergency Department: comparison with the various published studies.

aOnly patients with focal neurological signs at admission to ED; *In grey the study only focused on preschool children; °value referred at the percentage of all access in ED, independent of age.
ED: Emergency department; ne: not expressed.
Discussion
Headache is a common symptom in children, even in preschoolers and represents one of the main neurological causes of access to the ED. Headache in children under six years of age is still considered a diagnostic challenge often requiring neuroimaging to exclude malignant causes (15,16,23–28). To date, there are few studies focused on this age group. In fact, only one study examined 364 children (aged two to five years) with acute headache in ED showing that the diagnostic yield of CT scan is low for children with no history of concern and a normal neurological examination (10). Our study investigated a large preschooler cohort admitted to ED for headache, taking into account the epidemiological, clinical and etiological characteristics. We identified clinical features associated with an increased risk of secondary LT headache, which should lead to further investigation (i.e. brain CT) and admission rather than discharge. There was a higher frequency of male patients (817 males vs 585 females) similar to other studies (29), although sex did not correlate with hospitalization or PUIC (Tables 2, 3, 5, 6). A longer duration of headache before ED admission was associated with hospitalization (Table 2), while fever correlates better with discharge, in line with the higher frequency of benign secondary diseases (mainly airway infection) that did not require further investigation. Vomiting, torticollis, ocular motility disorders, ataxia, vertigo and drowsiness were more frequent in hospitalized children and were also reported in PUIC. In particular, the presence of neurological symptoms and signs, papilledema, ataxia, cranial nerves paralysis, nocturnal awakening and vomiting were significantly associated with PUIC, even if only ataxia and vomiting resulted associated variables at multivariable logistic regression analysis. Comorbidities showed an inverse association with PUIC. We also noted that headache due to PUIC was always associated with other symptoms and signs, mainly neurological. For example, patients with cerebrovascular disease (online Supplementary Table S3) also had vomiting, dizziness, drowsiness or nocturnal awakening; so, among these children, none presented headache as the only symptom. Nine children had inflammatory disorders of CNS and associated symptoms were mainly fever, vomiting and neurological signs or symptoms (online Supplementary Table S4). Most patients with intracranial hypertension had papilledema (online Supplementary Table S5). Accordingly, associated symptoms and signs should be carefully evaluated in order to obtain a prompt diagnosis and treatment of PUIC.
In our study, although all patients with PUIC were hospitalized, we can state that if a child with absence of comorbidities but with ataxia and vomiting presents to the emergency department there is a high chance of having a PUIC and the patient must be hospitalized quickly.
As regards headache etiology, 97.7% of the patients received a diagnosis of primary or benign secondary (i.e. related to airway or other extracerebral infections), while 34 children (2.3%) had PUIC (1.0% brain tumor, 0.2% vascular pathologies, 0.6% inflammatory disorders of CNS, 0.3% intracranial hypertension and cerebral malformations in 0.1%) (Table 4). Therefore, we confirmed that benign conditions are the most frequent causes of headache evaluated in the ED. The prevalence of PUIC was low, which may suggest that an age of under six should not be considered an important risk factor for malignant causes as previously thought. In addition, the occipital localization was not linked to PUIC, and this is also supported by a study that reported no different headache etiology when there was an occipital localization (30). To our knowledge, this is the largest preschool population evaluated in the ED for headache. We confirmed that benign secondary disorders represent the first cause of headache access in the ED in preschool age, while PUIC are rare. The lower LT diseases reported compared to Lateef et al. (10) (2.3% versus 7.2%), could be explained by different inclusion criteria, as we excluded post-traumatic headache and patients with known intracranial pathologies. In our study, the use of neuroimaging (12.9%) was less frequent than reported in literature (20.6%) (10), and this could be related to the continuous improvement of the knowledge of headache in children.
Our study has some limitations. Given the retrospective nature of the study we cannot exclude that there is a group of patients who were not included in the electronic medical records because they had relevant missing data on clinical history and neurological examination. We assume that this group is very small considering the basic level of clinical information included in this study. Bonferroni correction to the alpha value considered statistically significant has not been applied to safeguard the exploratory significance of our study. We restricted the study to Italian hospitals so our results are not generalizable.
In conclusion, our study identified clinical features that should be carefully evaluated in the emergency department in order to obtain a prompt diagnosis and treatment of PUIC. If they are present, they could represent an indication to perform brain CT, considering the limitation in the detection of posterior fossa alteration, and the patient must be hospitalized. Our study may suggest that age under six should not be considered an important risk factor as previously thought, but this needs to be confirmed in future studies (that compare the prevalence of dangerous etiologies in patients under six years of age versus over six years old).
Clinical implications
The prevalence of PUIC was low, which may suggest that an age of under six should not be considered an important risk factor for malignant causes as previously thought. Most children with life threatening pathology had at least one neurological symptom/sign besides headache. If a child with absence of comorbidities but with ataxia and vomiting presents to the emergency department there is a high chance of having a PUIC and they must be hospitalized quickly. The occipital localization of headache did not show any significant correlation with PUIC.
Supplemental Material
sj-pdf-1-cep-10.1177_03331024231164361 - Supplemental material for Children under 6 years with acute headache in Pediatric Emergency Departments. A 2-year retrospective exploratory multicenter Italian study
Supplemental material, sj-pdf-1-cep-10.1177_03331024231164361 for Children under 6 years with acute headache in Pediatric Emergency Departments. A 2-year retrospective exploratory multicenter Italian study by Umberto Raucci, Pasquale Parisi, Valentina Ferro, Erika Margani, Nicola Vanacore, Vincenzo Raieli, Claudia Bondone, Lucia Calistri, Agnese Suppiej, Antonella Palmieri, Duccio Maria Cordelli, Salvatore Savasta, Amanda Papa, Alberto Verrotti, Alessandro Orsini, Renato D’Alonzo, Piero Pavone, Raffaele Falsaperla, Mario Velardita, Raffaella Nacca, Laura Papetti, Roberta Rossi, Daniela Gioè, Cristina Malaventura, Flavia Drago, Cristina Morreale, Lucia Rossi, Thomas Foiadelli, Sonia Monticone, Chiara Mazzocchetti, Alice Bonuccelli, Filippo Greco, Silvia Marino, Gabriele Monte, Antonella Versace, Stefano Masi, Giovanni Di Nardo, Antonino Reale, Alberto Villani and Massimiliano Valeriani in Cephalalgia
Footnotes
Acknowledgments
The project was carried out as part of the initiatives of the study group of Italian Neurological Pediatric Urgency-Emergency Research Group of the Italian Society of Pediatric Neurology and associated Network (INPUERGOSINP).
Authors’ contributions
UR conceptualized and designed the study, designed the data collection instruments, coordinated and supervised data collection, directed all stages of data analyses, and drafted the initial manuscript; PP undertook the conception and design of the study, the interpretation of the data, and drafting the initial manuscript; VF, NV contributed to the design of the study, undertook the analysis of the data, and critically revised the manuscript for important intellectual content; MV, VR, LP contributed to the design of the study, and critically revised the manuscript for important intellectual content; all other authors contributed to the design of the study and interpretation of the data and critically revised the manuscript for important intellectual content; and all authors reviewed, and approve the final manuscript as submitted, and agree to be accountable for all aspects of the work.
Data availability statement
De-identified datasheets are available for other researchers upon reasonable request to the corresponding author.
Declaration of conflicting interests
The authors declare no conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported also by the Italian Ministry of Health with “Current Research funds”
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.